Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sample Questions: American Board of Medical MicrobiologyDocument8 pagesSample Questions: American Board of Medical Microbiologyelattar.laila1891No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- GNC SSN Past Paper 18-1Document32 pagesGNC SSN Past Paper 18-1Fan Eli100% (30)
- Global Atlas of Palliative CareDocument111 pagesGlobal Atlas of Palliative CareAlexandra Raluca PepelanNo ratings yet
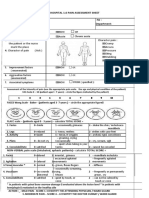
- Fisa Evaluare DurereDocument2 pagesFisa Evaluare DurerecristianNo ratings yet
- Ascend FlexDocument16 pagesAscend FlexBeatrizCuadrosNo ratings yet
- US Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchDocument101 pagesUS Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchGeorgesNo ratings yet
- Saver OneDocument2 pagesSaver OneamicoadrianoNo ratings yet
- Ekg InterpretareDocument25 pagesEkg InterpretareTeodor SlabuNo ratings yet
- Cleft Handout PASAGIDocument4 pagesCleft Handout PASAGIAyessah Nesreen PasagiNo ratings yet
- MARCH 16 2017 Plab 1 Recall PDFDocument27 pagesMARCH 16 2017 Plab 1 Recall PDFSamah KhanNo ratings yet
- Lesson 2-Introduction To The ICD-10-CM ClassificationDocument10 pagesLesson 2-Introduction To The ICD-10-CM ClassificationSwamyNo ratings yet
- (TNHS) : Summary and ExplanationDocument12 pages(TNHS) : Summary and Explanationcass100% (2)
- Field'S Stains A & B: (For in Vitro Diagnostic Use Only)Document2 pagesField'S Stains A & B: (For in Vitro Diagnostic Use Only)SHER AfghanNo ratings yet
- Antibiotic ATB For ExternDocument64 pagesAntibiotic ATB For ExternKarn AuerkarnnNo ratings yet
- Balanti An ES School Contingency Plan FINALDocument54 pagesBalanti An ES School Contingency Plan FINALCathyren Capizonda TevesNo ratings yet
- Quick Guide To Prescribing, Medicine Supplies and Support From Your PharmacyDocument11 pagesQuick Guide To Prescribing, Medicine Supplies and Support From Your Pharmacyminhmap90_635122804No ratings yet
- Guarino 2014Document21 pagesGuarino 2014ChangNo ratings yet
- Drug Abuse and Its Prevention PowerpointDocument15 pagesDrug Abuse and Its Prevention PowerpointChrizel NiloNo ratings yet
- The Autoimmune ProtocolDocument82 pagesThe Autoimmune Protocolsame shitNo ratings yet
- Optima™ CT660: Reference Protocol GuideDocument350 pagesOptima™ CT660: Reference Protocol GuideLizbeth CelaNo ratings yet
- PK PD en Critical IllnessDocument27 pagesPK PD en Critical IllnessDaniela BolivarNo ratings yet
- Table 3 International Consensus Criteria For Behavioural Variant FTDDocument1 pageTable 3 International Consensus Criteria For Behavioural Variant FTDFranco Paolo Maray-GhigliottoNo ratings yet
- Tugas BahasaDocument2 pagesTugas BahasaCitraNo ratings yet
- New India Family Floater Mediclaim Proposal FormDocument5 pagesNew India Family Floater Mediclaim Proposal FormspibluNo ratings yet
- OB C. 15 Study GuideDocument10 pagesOB C. 15 Study GuidePaige Nicole GauthreauxNo ratings yet
- Diltiazem Hydrochloride 2 CreamDocument3 pagesDiltiazem Hydrochloride 2 CreamOmair FarooqNo ratings yet
- International Journal of SurgeryDocument12 pagesInternational Journal of SurgeryNadya PutriNo ratings yet
- Proforma For PH CertificateDocument2 pagesProforma For PH CertificateDivakar MauryaNo ratings yet
- Teacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Document34 pagesTeacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Prakash AppaNo ratings yet
- 06 - Ambulatory Care PDFDocument50 pages06 - Ambulatory Care PDFandirio7486No ratings yet