
Management of Normal Labor and Delivery - UpToDate
Management of Normal Labor and Delivery - UpToDate
You might also like
- Wits Obstetrics 2008Document134 pagesWits Obstetrics 2008Muvenn Kannan100% (1)
- Arora PLAB 2 90 Day Planner - MinDocument12 pagesArora PLAB 2 90 Day Planner - Minmalmegrim100% (1)
- Mks Notes in Obgyn eDocument134 pagesMks Notes in Obgyn eإسراء محمود100% (3)
- Wa0022Document19 pagesWa0022Fan Eli50% (2)
- Management of Normal Labor and Delivery - UpToDateDocument46 pagesManagement of Normal Labor and Delivery - UpToDateTrần Ngọc BíchNo ratings yet
- Management of Normal Labor and DeliveryDocument46 pagesManagement of Normal Labor and DeliveryCIARA SOFIA SANDOVAL GARCIANo ratings yet
- Atención Al PartoDocument24 pagesAtención Al Partolusia nasdetNo ratings yet
- Management of Normal Labor and DeliveryDocument40 pagesManagement of Normal Labor and Deliveryrendyprimananda840No ratings yet
- Labor and Delivery Management of The Normal First StageDocument56 pagesLabor and Delivery Management of The Normal First Stagearrecis59No ratings yet
- Preterm LaborDocument18 pagesPreterm LaborJezreel NicolasNo ratings yet
- Labor - Overview of Normal and Abnormal Progression - UpToDateDocument29 pagesLabor - Overview of Normal and Abnormal Progression - UpToDateDiana LeverdaNo ratings yet
- Labor Dystocia Research ProtocolDocument27 pagesLabor Dystocia Research ProtocolMilaNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument37 pagesInduction of Labor With Oxytocin - UpToDateMerjem DautiNo ratings yet
- Module 5 Induction and Augmentation of LaborDocument17 pagesModule 5 Induction and Augmentation of LaborZyrene RiveraNo ratings yet
- Labor - Overview of Normal and Abnormal Progression - UpToDateDocument32 pagesLabor - Overview of Normal and Abnormal Progression - UpToDateThương ThươngNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument54 pagesInduction of Labor With Oxytocin - UpToDateJhoseline CamposNo ratings yet
- Postterm Pregnancy - UpToDateDocument16 pagesPostterm Pregnancy - UpToDateCarlos Jeiner Díaz SilvaNo ratings yet
- Obstetrics 2Document6 pagesObstetrics 2najmulNo ratings yet
- UpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitDocument31 pagesUpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitH. FoeNo ratings yet
- Cesarean Delivery Pre OpDocument17 pagesCesarean Delivery Pre OpAncuta CalimentNo ratings yet
- Labor Induction: Citations VerifyDocument8 pagesLabor Induction: Citations VerifyjiniabrahamNo ratings yet
- VacumDocument16 pagesVacumGkpmi Ekklesia JayapuraNo ratings yet
- Diagnosis of Preterm Labor and Overview of Preterm BirthDocument15 pagesDiagnosis of Preterm Labor and Overview of Preterm BirthKenny IncsNo ratings yet
- Labor Overview of Normal and Abnormal ProgressionDocument29 pagesLabor Overview of Normal and Abnormal Progressionarrecis59No ratings yet
- Prevention of The FirstDocument4 pagesPrevention of The FirstJEFFERSON MUÑOZNo ratings yet
- Maternal Nursing Care - CHPT 12 The Process of Labor and BirthDocument45 pagesMaternal Nursing Care - CHPT 12 The Process of Labor and Birththubtendrolma100% (6)
- Breech - Management Of: 1. PurposeDocument15 pagesBreech - Management Of: 1. PurposeMuathNo ratings yet
- The Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyDocument3 pagesThe Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyKyla VillafrancaNo ratings yet
- Operative Vaginal DeliveryDocument26 pagesOperative Vaginal DeliveryZurya UdayanaNo ratings yet
- Educational Topic 32: Obstetric Procedures: U 2: O S C: PDocument4 pagesEducational Topic 32: Obstetric Procedures: U 2: O S C: PStetho LoveNo ratings yet
- TC11Document4 pagesTC11FrancisNo ratings yet
- Pregnancy Loss (Miscarriage) - Clinical Presentations, Diagnosis, and Initial Evaluation - UpToDateDocument21 pagesPregnancy Loss (Miscarriage) - Clinical Presentations, Diagnosis, and Initial Evaluation - UpToDateDiana LeverdaNo ratings yet
- Factors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaDocument8 pagesFactors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaIllona SaharaNo ratings yet
- Vaginal Birth After Cesarean Delivery - StatPearls - NCBI BookshelfDocument5 pagesVaginal Birth After Cesarean Delivery - StatPearls - NCBI BookshelfSantiago Tomas QuinterosNo ratings yet
- Trail of LaborDocument5 pagesTrail of LaborNithiya NadesanNo ratings yet
- Prognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesDocument5 pagesPrognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesTriponiaNo ratings yet
- Screening of High-Risk Pregnancy, Newer Modalities of DiagnosisDocument12 pagesScreening of High-Risk Pregnancy, Newer Modalities of DiagnosisSanthosh.S.U100% (10)
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument10 pagesBest Practice & Research Clinical Obstetrics and GynaecologyMBMNo ratings yet
- The Gynecologic Examination: Pamela Charney, MDDocument22 pagesThe Gynecologic Examination: Pamela Charney, MDTiara AnggrainiNo ratings yet
- Ectopic Pregnancy Term PaperDocument7 pagesEctopic Pregnancy Term Paperauhavmpif100% (1)
- 1471 2393 13 31 PDFDocument6 pages1471 2393 13 31 PDFTriponiaNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Gestational AgeDocument34 pagesGestational AgeAaliyaan KhanNo ratings yet
- Safe Prevention of The Primary Cesarean Delivery - ACOGDocument16 pagesSafe Prevention of The Primary Cesarean Delivery - ACOGAryaNo ratings yet
- Women's Health Care Physicians: Tubal Ectopic PregnancyDocument25 pagesWomen's Health Care Physicians: Tubal Ectopic PregnancyIsidore TompeenNo ratings yet
- Thesis Related To Ectopic PregnancyDocument8 pagesThesis Related To Ectopic Pregnancydnnsgccc100% (2)
- Literature Review Placenta PreviaDocument7 pagesLiterature Review Placenta Previaeygyabvkg100% (2)
- Clinical Evaluation of Labor: An Evidence-And Experience-Based ApproachDocument13 pagesClinical Evaluation of Labor: An Evidence-And Experience-Based ApproachAlejandro Abarca VargasNo ratings yet
- Indications For Outpatient Antenatal Fetal Surveillance ACOGDocument62 pagesIndications For Outpatient Antenatal Fetal Surveillance ACOGagraisabelaNo ratings yet
- Reference ResearchDocument8 pagesReference Research9. NOORSHAHIDA MOHAMADNo ratings yet
- DR Case Presentation FinalDocument35 pagesDR Case Presentation FinalLord Allen B. GomezNo ratings yet
- Nadt15i1p33 PDFDocument12 pagesNadt15i1p33 PDFNuke YolandaNo ratings yet
- Management Placenta PreviaDocument24 pagesManagement Placenta PreviaMuhammad RifaldiNo ratings yet
- Nasterea in Prezentatie PelvinaDocument14 pagesNasterea in Prezentatie PelvinaIrina AdrianaNo ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument9 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfKatherine DavilaNo ratings yet
- OB - Reporting CPDDocument7 pagesOB - Reporting CPDD A M N E R ANo ratings yet
- Module 2 Activity 2 Group 2Document23 pagesModule 2 Activity 2 Group 2Allyza Montaño Santander GomezNo ratings yet
- Bahan Utk VCDocument58 pagesBahan Utk VCTias DiahNo ratings yet
- Research Paper On Labor and Delivery NursingDocument4 pagesResearch Paper On Labor and Delivery Nursingniisexgkf100% (1)
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfLaura valentina ramos mezaNo ratings yet
- By: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyDocument54 pagesBy: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyBharat ThapaNo ratings yet
- Case Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniDocument15 pagesCase Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniAnto SaragihNo ratings yet
- Female Infertility in The U.a.EDocument88 pagesFemale Infertility in The U.a.EOhmed KhiljiNo ratings yet
- HypogonadismDocument10 pagesHypogonadismJaya SantikaNo ratings yet
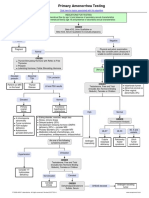
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Antepartum Haemorrhage: Women's & Children's ServicesDocument4 pagesAntepartum Haemorrhage: Women's & Children's ServicesYwagar YwagarNo ratings yet
- Nbns1104 Transculture in NursingDocument8 pagesNbns1104 Transculture in Nursingdicky chongNo ratings yet
- Anatomical Changes in PregnancyDocument13 pagesAnatomical Changes in PregnancyAnyaNo ratings yet
- Osce EmergenciesjDocument31 pagesOsce EmergenciesjTess WilliamsNo ratings yet
- Estrous Cycle 2018-VA-177Document16 pagesEstrous Cycle 2018-VA-177Syed Mohsin NisarNo ratings yet
- Penurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiDocument5 pagesPenurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiadiNo ratings yet
- Operational Guidelines For Establishing Sentinel Stillbirth Surveillance SystemDocument40 pagesOperational Guidelines For Establishing Sentinel Stillbirth Surveillance Systemraval anil.uNo ratings yet
- Акушерство Фукс англ 2019Document875 pagesАкушерство Фукс англ 2019ȜLaa AsHrafNo ratings yet
- Ob Part 2Document7 pagesOb Part 2gmik02No ratings yet
- Session #45 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document6 pagesSession #45 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- E-Poster Rcog 2018Document1 pageE-Poster Rcog 2018Ana MarianaNo ratings yet
- PDF Attached: Laboratory Investigation ReportDocument3 pagesPDF Attached: Laboratory Investigation ReportAnkita YadavNo ratings yet
- Determinants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalDocument14 pagesDeterminants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Hormonal Contraception Methods (Iter)Document12 pagesHormonal Contraception Methods (Iter)Lady JNo ratings yet
- Acute Inversion of The UterusDocument10 pagesAcute Inversion of The UterusNurlina SetiadiNo ratings yet
- Euthenics ModuleDocument4 pagesEuthenics ModuleHanna AsmadNo ratings yet
- Chect List and Activities Breast and LymphaticDocument9 pagesChect List and Activities Breast and LymphaticJessoliver GalvezNo ratings yet
- Mayer-Rokitansky-K Uster-Hauser Syndrome: Diagnosis and ManagementDocument7 pagesMayer-Rokitansky-K Uster-Hauser Syndrome: Diagnosis and ManagementRavi SinghNo ratings yet
- Vaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesDocument6 pagesVaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesCristinaCaprosNo ratings yet
- Form 2D Health Plan Implementation Pregnancy Prenatal CareDocument2 pagesForm 2D Health Plan Implementation Pregnancy Prenatal CareLora CarpioNo ratings yet
- Contoh Abstract Yang Systematic Review a Systematic Review and Network Meta-Analysis Comparing the Use of Foley Catheters, Misoprostol, And Dinoprostone for Cervical Ripening in the Indu... - PubMed - NCBIDocument2 pagesContoh Abstract Yang Systematic Review a Systematic Review and Network Meta-Analysis Comparing the Use of Foley Catheters, Misoprostol, And Dinoprostone for Cervical Ripening in the Indu... - PubMed - NCBIWienda GeraldineNo ratings yet
- DR NR EvalDocument4 pagesDR NR EvalNaomi RebongNo ratings yet
- The Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterDocument5 pagesThe Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterBob IrsanNo ratings yet
























































































Download as pdf or txt
You might also like
- Wits Obstetrics 2008Document134 pagesWits Obstetrics 2008Muvenn Kannan100% (1)
- Arora PLAB 2 90 Day Planner - MinDocument12 pagesArora PLAB 2 90 Day Planner - Minmalmegrim100% (1)
- Mks Notes in Obgyn eDocument134 pagesMks Notes in Obgyn eإسراء محمود100% (3)
- Wa0022Document19 pagesWa0022Fan Eli50% (2)
- Management of Normal Labor and Delivery - UpToDateDocument46 pagesManagement of Normal Labor and Delivery - UpToDateTrần Ngọc BíchNo ratings yet
- Management of Normal Labor and DeliveryDocument46 pagesManagement of Normal Labor and DeliveryCIARA SOFIA SANDOVAL GARCIANo ratings yet
- Atención Al PartoDocument24 pagesAtención Al Partolusia nasdetNo ratings yet
- Management of Normal Labor and DeliveryDocument40 pagesManagement of Normal Labor and Deliveryrendyprimananda840No ratings yet
- Labor and Delivery Management of The Normal First StageDocument56 pagesLabor and Delivery Management of The Normal First Stagearrecis59No ratings yet
- Preterm LaborDocument18 pagesPreterm LaborJezreel NicolasNo ratings yet
- Labor - Overview of Normal and Abnormal Progression - UpToDateDocument29 pagesLabor - Overview of Normal and Abnormal Progression - UpToDateDiana LeverdaNo ratings yet
- Labor Dystocia Research ProtocolDocument27 pagesLabor Dystocia Research ProtocolMilaNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument37 pagesInduction of Labor With Oxytocin - UpToDateMerjem DautiNo ratings yet
- Module 5 Induction and Augmentation of LaborDocument17 pagesModule 5 Induction and Augmentation of LaborZyrene RiveraNo ratings yet
- Labor - Overview of Normal and Abnormal Progression - UpToDateDocument32 pagesLabor - Overview of Normal and Abnormal Progression - UpToDateThương ThươngNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument54 pagesInduction of Labor With Oxytocin - UpToDateJhoseline CamposNo ratings yet
- Postterm Pregnancy - UpToDateDocument16 pagesPostterm Pregnancy - UpToDateCarlos Jeiner Díaz SilvaNo ratings yet
- Obstetrics 2Document6 pagesObstetrics 2najmulNo ratings yet
- UpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitDocument31 pagesUpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitH. FoeNo ratings yet
- Cesarean Delivery Pre OpDocument17 pagesCesarean Delivery Pre OpAncuta CalimentNo ratings yet
- Labor Induction: Citations VerifyDocument8 pagesLabor Induction: Citations VerifyjiniabrahamNo ratings yet
- VacumDocument16 pagesVacumGkpmi Ekklesia JayapuraNo ratings yet
- Diagnosis of Preterm Labor and Overview of Preterm BirthDocument15 pagesDiagnosis of Preterm Labor and Overview of Preterm BirthKenny IncsNo ratings yet
- Labor Overview of Normal and Abnormal ProgressionDocument29 pagesLabor Overview of Normal and Abnormal Progressionarrecis59No ratings yet
- Prevention of The FirstDocument4 pagesPrevention of The FirstJEFFERSON MUÑOZNo ratings yet
- Maternal Nursing Care - CHPT 12 The Process of Labor and BirthDocument45 pagesMaternal Nursing Care - CHPT 12 The Process of Labor and Birththubtendrolma100% (6)
- Breech - Management Of: 1. PurposeDocument15 pagesBreech - Management Of: 1. PurposeMuathNo ratings yet
- The Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyDocument3 pagesThe Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyKyla VillafrancaNo ratings yet
- Operative Vaginal DeliveryDocument26 pagesOperative Vaginal DeliveryZurya UdayanaNo ratings yet
- Educational Topic 32: Obstetric Procedures: U 2: O S C: PDocument4 pagesEducational Topic 32: Obstetric Procedures: U 2: O S C: PStetho LoveNo ratings yet
- TC11Document4 pagesTC11FrancisNo ratings yet
- Pregnancy Loss (Miscarriage) - Clinical Presentations, Diagnosis, and Initial Evaluation - UpToDateDocument21 pagesPregnancy Loss (Miscarriage) - Clinical Presentations, Diagnosis, and Initial Evaluation - UpToDateDiana LeverdaNo ratings yet
- Factors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaDocument8 pagesFactors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaIllona SaharaNo ratings yet
- Vaginal Birth After Cesarean Delivery - StatPearls - NCBI BookshelfDocument5 pagesVaginal Birth After Cesarean Delivery - StatPearls - NCBI BookshelfSantiago Tomas QuinterosNo ratings yet
- Trail of LaborDocument5 pagesTrail of LaborNithiya NadesanNo ratings yet
- Prognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesDocument5 pagesPrognostic Factors For Successful Vaginal Birth After Cesarean Section - Analysis of 162 CasesTriponiaNo ratings yet
- Screening of High-Risk Pregnancy, Newer Modalities of DiagnosisDocument12 pagesScreening of High-Risk Pregnancy, Newer Modalities of DiagnosisSanthosh.S.U100% (10)
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument10 pagesBest Practice & Research Clinical Obstetrics and GynaecologyMBMNo ratings yet
- The Gynecologic Examination: Pamela Charney, MDDocument22 pagesThe Gynecologic Examination: Pamela Charney, MDTiara AnggrainiNo ratings yet
- Ectopic Pregnancy Term PaperDocument7 pagesEctopic Pregnancy Term Paperauhavmpif100% (1)
- 1471 2393 13 31 PDFDocument6 pages1471 2393 13 31 PDFTriponiaNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Gestational AgeDocument34 pagesGestational AgeAaliyaan KhanNo ratings yet
- Safe Prevention of The Primary Cesarean Delivery - ACOGDocument16 pagesSafe Prevention of The Primary Cesarean Delivery - ACOGAryaNo ratings yet
- Women's Health Care Physicians: Tubal Ectopic PregnancyDocument25 pagesWomen's Health Care Physicians: Tubal Ectopic PregnancyIsidore TompeenNo ratings yet
- Thesis Related To Ectopic PregnancyDocument8 pagesThesis Related To Ectopic Pregnancydnnsgccc100% (2)
- Literature Review Placenta PreviaDocument7 pagesLiterature Review Placenta Previaeygyabvkg100% (2)
- Clinical Evaluation of Labor: An Evidence-And Experience-Based ApproachDocument13 pagesClinical Evaluation of Labor: An Evidence-And Experience-Based ApproachAlejandro Abarca VargasNo ratings yet
- Indications For Outpatient Antenatal Fetal Surveillance ACOGDocument62 pagesIndications For Outpatient Antenatal Fetal Surveillance ACOGagraisabelaNo ratings yet
- Reference ResearchDocument8 pagesReference Research9. NOORSHAHIDA MOHAMADNo ratings yet
- DR Case Presentation FinalDocument35 pagesDR Case Presentation FinalLord Allen B. GomezNo ratings yet
- Nadt15i1p33 PDFDocument12 pagesNadt15i1p33 PDFNuke YolandaNo ratings yet
- Management Placenta PreviaDocument24 pagesManagement Placenta PreviaMuhammad RifaldiNo ratings yet
- Nasterea in Prezentatie PelvinaDocument14 pagesNasterea in Prezentatie PelvinaIrina AdrianaNo ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument9 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfKatherine DavilaNo ratings yet
- OB - Reporting CPDDocument7 pagesOB - Reporting CPDD A M N E R ANo ratings yet
- Module 2 Activity 2 Group 2Document23 pagesModule 2 Activity 2 Group 2Allyza Montaño Santander GomezNo ratings yet
- Bahan Utk VCDocument58 pagesBahan Utk VCTias DiahNo ratings yet
- Research Paper On Labor and Delivery NursingDocument4 pagesResearch Paper On Labor and Delivery Nursingniisexgkf100% (1)
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfLaura valentina ramos mezaNo ratings yet
- By: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyDocument54 pagesBy: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyBharat ThapaNo ratings yet
- Case Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniDocument15 pagesCase Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniAnto SaragihNo ratings yet
- Female Infertility in The U.a.EDocument88 pagesFemale Infertility in The U.a.EOhmed KhiljiNo ratings yet
- HypogonadismDocument10 pagesHypogonadismJaya SantikaNo ratings yet
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Antepartum Haemorrhage: Women's & Children's ServicesDocument4 pagesAntepartum Haemorrhage: Women's & Children's ServicesYwagar YwagarNo ratings yet
- Nbns1104 Transculture in NursingDocument8 pagesNbns1104 Transculture in Nursingdicky chongNo ratings yet
- Anatomical Changes in PregnancyDocument13 pagesAnatomical Changes in PregnancyAnyaNo ratings yet
- Osce EmergenciesjDocument31 pagesOsce EmergenciesjTess WilliamsNo ratings yet
- Estrous Cycle 2018-VA-177Document16 pagesEstrous Cycle 2018-VA-177Syed Mohsin NisarNo ratings yet
- Penurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiDocument5 pagesPenurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiadiNo ratings yet
- Operational Guidelines For Establishing Sentinel Stillbirth Surveillance SystemDocument40 pagesOperational Guidelines For Establishing Sentinel Stillbirth Surveillance Systemraval anil.uNo ratings yet
- Акушерство Фукс англ 2019Document875 pagesАкушерство Фукс англ 2019ȜLaa AsHrafNo ratings yet
- Ob Part 2Document7 pagesOb Part 2gmik02No ratings yet
- Session #45 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document6 pagesSession #45 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- E-Poster Rcog 2018Document1 pageE-Poster Rcog 2018Ana MarianaNo ratings yet
- PDF Attached: Laboratory Investigation ReportDocument3 pagesPDF Attached: Laboratory Investigation ReportAnkita YadavNo ratings yet
- Determinants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalDocument14 pagesDeterminants of Pre-Eclampsia Incidence Among Pregnant Women in Antenatal Care at Fortportal Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Hormonal Contraception Methods (Iter)Document12 pagesHormonal Contraception Methods (Iter)Lady JNo ratings yet
- Acute Inversion of The UterusDocument10 pagesAcute Inversion of The UterusNurlina SetiadiNo ratings yet
- Euthenics ModuleDocument4 pagesEuthenics ModuleHanna AsmadNo ratings yet
- Chect List and Activities Breast and LymphaticDocument9 pagesChect List and Activities Breast and LymphaticJessoliver GalvezNo ratings yet
- Mayer-Rokitansky-K Uster-Hauser Syndrome: Diagnosis and ManagementDocument7 pagesMayer-Rokitansky-K Uster-Hauser Syndrome: Diagnosis and ManagementRavi SinghNo ratings yet
- Vaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesDocument6 pagesVaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesCristinaCaprosNo ratings yet
- Form 2D Health Plan Implementation Pregnancy Prenatal CareDocument2 pagesForm 2D Health Plan Implementation Pregnancy Prenatal CareLora CarpioNo ratings yet
- Contoh Abstract Yang Systematic Review a Systematic Review and Network Meta-Analysis Comparing the Use of Foley Catheters, Misoprostol, And Dinoprostone for Cervical Ripening in the Indu... - PubMed - NCBIDocument2 pagesContoh Abstract Yang Systematic Review a Systematic Review and Network Meta-Analysis Comparing the Use of Foley Catheters, Misoprostol, And Dinoprostone for Cervical Ripening in the Indu... - PubMed - NCBIWienda GeraldineNo ratings yet
- DR NR EvalDocument4 pagesDR NR EvalNaomi RebongNo ratings yet
- The Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterDocument5 pagesThe Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterBob IrsanNo ratings yet