
Aversion Therapy
Aversion Therapy
You might also like
- Ybocs Ii 2Document21 pagesYbocs Ii 2Ali MatheisNo ratings yet
- IB Psychology, Health Psychology, Learning OutcomesDocument5 pagesIB Psychology, Health Psychology, Learning OutcomesBruce BybeeNo ratings yet
- Undoing Lyme Disease: How to Make Your Mitochondria Fight Lyme Borreliosis by Surfing Oxygen WavesFrom EverandUndoing Lyme Disease: How to Make Your Mitochondria Fight Lyme Borreliosis by Surfing Oxygen WavesNo ratings yet
- Case Study-HR Planning at The City HotelDocument5 pagesCase Study-HR Planning at The City Hotelfahad rustam100% (2)
- 1999 Aversion Therapy-BEDocument6 pages1999 Aversion Therapy-BEprabhaNo ratings yet
- Aversion TherapyDocument11 pagesAversion Therapyayyappan.ashok6713100% (2)
- Principles of Behavior Therapy and Behavior Modification (Chapter PDFDocument23 pagesPrinciples of Behavior Therapy and Behavior Modification (Chapter PDFRashi Sharma100% (1)
- Behaviour TherapyDocument16 pagesBehaviour TherapyANA MAE PABLO83% (6)
- Aversive ConditioningDocument4 pagesAversive Conditioningiulia9gavrisNo ratings yet
- Behavioral TherapyDocument3 pagesBehavioral TherapymoumukhNo ratings yet
- BehaviourismDocument9 pagesBehaviourismVijeyachandhar DorairajNo ratings yet
- Aversion TherapyDocument3 pagesAversion Therapyden777No ratings yet
- Techniques PrintedDocument14 pagesTechniques PrintedAzizNo ratings yet
- Behavior Therapy Techniques:: Areej Fatima Roll NO: 379Document7 pagesBehavior Therapy Techniques:: Areej Fatima Roll NO: 379jehanzebNo ratings yet
- Supportive TherapyDocument64 pagesSupportive TherapyRibhav GuptaNo ratings yet
- Abnormal Psychology Comer 8th Edition Test BankDocument56 pagesAbnormal Psychology Comer 8th Edition Test BankJeffery Davis100% (36)
- Literature Review On Classical ConditioningDocument5 pagesLiterature Review On Classical Conditioningafmzslnxmqrjom100% (1)
- Health PsychologyDocument51 pagesHealth PsychologyShakeel Ahmed100% (3)
- Aversion TherapyDocument4 pagesAversion Therapyamagra993023100% (1)
- Abnormal Psychology Comer 8th Edition Test BankDocument56 pagesAbnormal Psychology Comer 8th Edition Test BankbenjaminwagnerjtpoarxcfyNo ratings yet
- Covert Extinction TherapyDocument6 pagesCovert Extinction TherapyAnet Augustine AnetNo ratings yet
- Behaviour TherPYDocument11 pagesBehaviour TherPYrupali kharabeNo ratings yet
- Fundamentals of Abnormal Psychology 8th Edition Comer Test BankDocument56 pagesFundamentals of Abnormal Psychology 8th Edition Comer Test BankIrene Peterson100% (39)
- Behavior Therapy Short Ver.Document21 pagesBehavior Therapy Short Ver.AngelNo ratings yet
- Abnormal Psychology Comer 8th Edition Test BankDocument31 pagesAbnormal Psychology Comer 8th Edition Test Bankwydcirri.818y4100% (48)
- Behavioural Excess Is An Undesirable Target Behaviour The Person Wants To Decrease in FrequencyDocument10 pagesBehavioural Excess Is An Undesirable Target Behaviour The Person Wants To Decrease in FrequencyGodwin EzekielNo ratings yet
- Behavior TherapyDocument52 pagesBehavior TherapySajal SahooNo ratings yet
- Behavioral TherapyDocument4 pagesBehavioral TherapyseemabNo ratings yet
- Placebo Effect Literature ReviewDocument5 pagesPlacebo Effect Literature Reviewukefbfvkg100% (1)
- SW 142 ReportingDocument10 pagesSW 142 ReportingKrishian Erl AndogNo ratings yet
- Prevention and Treatments For Alcohol Abuse and Addiction WorksheetsDocument5 pagesPrevention and Treatments For Alcohol Abuse and Addiction WorksheetsHan Thai Pham (Hannah)No ratings yet
- Behavioural TherapyDocument6 pagesBehavioural TherapyBiswas AruNo ratings yet
- Canjpsychiatryreview PDFDocument11 pagesCanjpsychiatryreview PDFnovywardanaNo ratings yet
- Essay On Placebo Effect With Thesis StatementDocument8 pagesEssay On Placebo Effect With Thesis Statementafcmtzlda100% (2)
- Aversion TherapyDocument47 pagesAversion TherapyJohn Rey MagsicoNo ratings yet
- Learn MedDocument6 pagesLearn Medapi-3699361No ratings yet
- Behavior Science & Clinical Psycology 2 (Mrinmoy Roy)Document16 pagesBehavior Science & Clinical Psycology 2 (Mrinmoy Roy)Dr. MrinmoyNo ratings yet
- Abramowitz 2007Document10 pagesAbramowitz 2007PalomaNo ratings yet
- Introduction To Behavioral SciencesDocument38 pagesIntroduction To Behavioral Sciencesmahrabfatima316No ratings yet
- Scientific Method in PsychologyDocument22 pagesScientific Method in PsychologyEvon GohNo ratings yet
- Psychotherapeutic Treatment To DisordersDocument9 pagesPsychotherapeutic Treatment To DisordersFahad BhayoNo ratings yet
- A Seminar On Behavioral Therapy: M.O.S.C. College of Nursing Kolenchery Mental Health NursingDocument10 pagesA Seminar On Behavioral Therapy: M.O.S.C. College of Nursing Kolenchery Mental Health NursingCHANDNI C VNo ratings yet
- CH 2Document15 pagesCH 28f6nss6kvzNo ratings yet
- Inspiration Powerpoint NoteDocument13 pagesInspiration Powerpoint Noteapi-201676767No ratings yet
- Gillihan Et Al. 2012 Common Pitfalls EX RP For OCDDocument7 pagesGillihan Et Al. 2012 Common Pitfalls EX RP For OCDFaris Aziz PridiantoNo ratings yet
- Article 54Document11 pagesArticle 54Tufail KhanNo ratings yet
- Aversion John ReyDocument7 pagesAversion John ReyJohn Rey MagsicoNo ratings yet
- Effectiveness of Cognitive Behavioural Therapy (CBT) and Pharmacotherapy For The Treatment of Obsessive-Compulsive DisorderDocument13 pagesEffectiveness of Cognitive Behavioural Therapy (CBT) and Pharmacotherapy For The Treatment of Obsessive-Compulsive DisorderDipto Kumer SarkerNo ratings yet
- CBT KaddenDocument28 pagesCBT KaddenAbhik SahaNo ratings yet
- Borrie and Suedfeld - (1995) - Draft - Health and Clinical ApplicationsDocument23 pagesBorrie and Suedfeld - (1995) - Draft - Health and Clinical Applicationsfriend717No ratings yet
- Behavioral Psychology and CounsellingDocument13 pagesBehavioral Psychology and Counsellingsuhail iqbal sipra100% (1)
- The Behaviourist Appr.Document2 pagesThe Behaviourist Appr.swerlg87ezNo ratings yet
- Mental Health TheoriesDocument6 pagesMental Health TheoriesRodzel Oñate BañagaNo ratings yet
- Bad Behavior (Non-Punctuality)Document23 pagesBad Behavior (Non-Punctuality)Ali ZulfiqarNo ratings yet
- Behaviorism by Red LightDocument5 pagesBehaviorism by Red LightRedMoonLightNo ratings yet
- Anxiety TherapyDocument14 pagesAnxiety TherapyToolika WNo ratings yet
- Systems Plus College Foundation Balibago, Angeles City, Pampanga College of NursingDocument8 pagesSystems Plus College Foundation Balibago, Angeles City, Pampanga College of NursingAly PinpinNo ratings yet
- Somatization ThesisDocument5 pagesSomatization Thesisxlyexqvff100% (3)
- Health Psychology AssignmentDocument12 pagesHealth Psychology AssignmentAnvesha ChoukseyNo ratings yet
- Understanding Hard to Maintain Behaviour Change: A Dual Process ApproachFrom EverandUnderstanding Hard to Maintain Behaviour Change: A Dual Process ApproachNo ratings yet
- Abdul Aziz AssignmentDocument5 pagesAbdul Aziz Assignmentfahad rustamNo ratings yet
- Antipsychotics 1Document41 pagesAntipsychotics 1fahad rustam100% (1)
- Assessment and Treatment of Individuals at High RiDocument8 pagesAssessment and Treatment of Individuals at High Rifahad rustamNo ratings yet
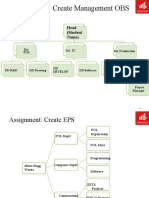
- Assignment 2 Making OBS & EPSDocument3 pagesAssignment 2 Making OBS & EPSfahad rustamNo ratings yet
- EME AttendanceDocument2 pagesEME Attendancefahad rustam100% (1)
- Human Resources (1) NewDocument12 pagesHuman Resources (1) Newfahad rustamNo ratings yet
- Jogging Line Application-1Document1 pageJogging Line Application-1fahad rustam100% (1)
- PQM Assignment 3: Deadline 9-5-2020Document7 pagesPQM Assignment 3: Deadline 9-5-2020fahad rustamNo ratings yet
- Conduct of Academic Audit FinalDocument3 pagesConduct of Academic Audit Finalfahad rustamNo ratings yet
- Competitive Profile MatrixDocument10 pagesCompetitive Profile Matrixfahad rustamNo ratings yet




































































Download as pdf or txt
You might also like
- Ybocs Ii 2Document21 pagesYbocs Ii 2Ali MatheisNo ratings yet
- IB Psychology, Health Psychology, Learning OutcomesDocument5 pagesIB Psychology, Health Psychology, Learning OutcomesBruce BybeeNo ratings yet
- Undoing Lyme Disease: How to Make Your Mitochondria Fight Lyme Borreliosis by Surfing Oxygen WavesFrom EverandUndoing Lyme Disease: How to Make Your Mitochondria Fight Lyme Borreliosis by Surfing Oxygen WavesNo ratings yet
- Case Study-HR Planning at The City HotelDocument5 pagesCase Study-HR Planning at The City Hotelfahad rustam100% (2)
- 1999 Aversion Therapy-BEDocument6 pages1999 Aversion Therapy-BEprabhaNo ratings yet
- Aversion TherapyDocument11 pagesAversion Therapyayyappan.ashok6713100% (2)
- Principles of Behavior Therapy and Behavior Modification (Chapter PDFDocument23 pagesPrinciples of Behavior Therapy and Behavior Modification (Chapter PDFRashi Sharma100% (1)
- Behaviour TherapyDocument16 pagesBehaviour TherapyANA MAE PABLO83% (6)
- Aversive ConditioningDocument4 pagesAversive Conditioningiulia9gavrisNo ratings yet
- Behavioral TherapyDocument3 pagesBehavioral TherapymoumukhNo ratings yet
- BehaviourismDocument9 pagesBehaviourismVijeyachandhar DorairajNo ratings yet
- Aversion TherapyDocument3 pagesAversion Therapyden777No ratings yet
- Techniques PrintedDocument14 pagesTechniques PrintedAzizNo ratings yet
- Behavior Therapy Techniques:: Areej Fatima Roll NO: 379Document7 pagesBehavior Therapy Techniques:: Areej Fatima Roll NO: 379jehanzebNo ratings yet
- Supportive TherapyDocument64 pagesSupportive TherapyRibhav GuptaNo ratings yet
- Abnormal Psychology Comer 8th Edition Test BankDocument56 pagesAbnormal Psychology Comer 8th Edition Test BankJeffery Davis100% (36)
- Literature Review On Classical ConditioningDocument5 pagesLiterature Review On Classical Conditioningafmzslnxmqrjom100% (1)
- Health PsychologyDocument51 pagesHealth PsychologyShakeel Ahmed100% (3)
- Aversion TherapyDocument4 pagesAversion Therapyamagra993023100% (1)
- Abnormal Psychology Comer 8th Edition Test BankDocument56 pagesAbnormal Psychology Comer 8th Edition Test BankbenjaminwagnerjtpoarxcfyNo ratings yet
- Covert Extinction TherapyDocument6 pagesCovert Extinction TherapyAnet Augustine AnetNo ratings yet
- Behaviour TherPYDocument11 pagesBehaviour TherPYrupali kharabeNo ratings yet
- Fundamentals of Abnormal Psychology 8th Edition Comer Test BankDocument56 pagesFundamentals of Abnormal Psychology 8th Edition Comer Test BankIrene Peterson100% (39)
- Behavior Therapy Short Ver.Document21 pagesBehavior Therapy Short Ver.AngelNo ratings yet
- Abnormal Psychology Comer 8th Edition Test BankDocument31 pagesAbnormal Psychology Comer 8th Edition Test Bankwydcirri.818y4100% (48)
- Behavioural Excess Is An Undesirable Target Behaviour The Person Wants To Decrease in FrequencyDocument10 pagesBehavioural Excess Is An Undesirable Target Behaviour The Person Wants To Decrease in FrequencyGodwin EzekielNo ratings yet
- Behavior TherapyDocument52 pagesBehavior TherapySajal SahooNo ratings yet
- Behavioral TherapyDocument4 pagesBehavioral TherapyseemabNo ratings yet
- Placebo Effect Literature ReviewDocument5 pagesPlacebo Effect Literature Reviewukefbfvkg100% (1)
- SW 142 ReportingDocument10 pagesSW 142 ReportingKrishian Erl AndogNo ratings yet
- Prevention and Treatments For Alcohol Abuse and Addiction WorksheetsDocument5 pagesPrevention and Treatments For Alcohol Abuse and Addiction WorksheetsHan Thai Pham (Hannah)No ratings yet
- Behavioural TherapyDocument6 pagesBehavioural TherapyBiswas AruNo ratings yet
- Canjpsychiatryreview PDFDocument11 pagesCanjpsychiatryreview PDFnovywardanaNo ratings yet
- Essay On Placebo Effect With Thesis StatementDocument8 pagesEssay On Placebo Effect With Thesis Statementafcmtzlda100% (2)
- Aversion TherapyDocument47 pagesAversion TherapyJohn Rey MagsicoNo ratings yet
- Learn MedDocument6 pagesLearn Medapi-3699361No ratings yet
- Behavior Science & Clinical Psycology 2 (Mrinmoy Roy)Document16 pagesBehavior Science & Clinical Psycology 2 (Mrinmoy Roy)Dr. MrinmoyNo ratings yet
- Abramowitz 2007Document10 pagesAbramowitz 2007PalomaNo ratings yet
- Introduction To Behavioral SciencesDocument38 pagesIntroduction To Behavioral Sciencesmahrabfatima316No ratings yet
- Scientific Method in PsychologyDocument22 pagesScientific Method in PsychologyEvon GohNo ratings yet
- Psychotherapeutic Treatment To DisordersDocument9 pagesPsychotherapeutic Treatment To DisordersFahad BhayoNo ratings yet
- A Seminar On Behavioral Therapy: M.O.S.C. College of Nursing Kolenchery Mental Health NursingDocument10 pagesA Seminar On Behavioral Therapy: M.O.S.C. College of Nursing Kolenchery Mental Health NursingCHANDNI C VNo ratings yet
- CH 2Document15 pagesCH 28f6nss6kvzNo ratings yet
- Inspiration Powerpoint NoteDocument13 pagesInspiration Powerpoint Noteapi-201676767No ratings yet
- Gillihan Et Al. 2012 Common Pitfalls EX RP For OCDDocument7 pagesGillihan Et Al. 2012 Common Pitfalls EX RP For OCDFaris Aziz PridiantoNo ratings yet
- Article 54Document11 pagesArticle 54Tufail KhanNo ratings yet
- Aversion John ReyDocument7 pagesAversion John ReyJohn Rey MagsicoNo ratings yet
- Effectiveness of Cognitive Behavioural Therapy (CBT) and Pharmacotherapy For The Treatment of Obsessive-Compulsive DisorderDocument13 pagesEffectiveness of Cognitive Behavioural Therapy (CBT) and Pharmacotherapy For The Treatment of Obsessive-Compulsive DisorderDipto Kumer SarkerNo ratings yet
- CBT KaddenDocument28 pagesCBT KaddenAbhik SahaNo ratings yet
- Borrie and Suedfeld - (1995) - Draft - Health and Clinical ApplicationsDocument23 pagesBorrie and Suedfeld - (1995) - Draft - Health and Clinical Applicationsfriend717No ratings yet
- Behavioral Psychology and CounsellingDocument13 pagesBehavioral Psychology and Counsellingsuhail iqbal sipra100% (1)
- The Behaviourist Appr.Document2 pagesThe Behaviourist Appr.swerlg87ezNo ratings yet
- Mental Health TheoriesDocument6 pagesMental Health TheoriesRodzel Oñate BañagaNo ratings yet
- Bad Behavior (Non-Punctuality)Document23 pagesBad Behavior (Non-Punctuality)Ali ZulfiqarNo ratings yet
- Behaviorism by Red LightDocument5 pagesBehaviorism by Red LightRedMoonLightNo ratings yet
- Anxiety TherapyDocument14 pagesAnxiety TherapyToolika WNo ratings yet
- Systems Plus College Foundation Balibago, Angeles City, Pampanga College of NursingDocument8 pagesSystems Plus College Foundation Balibago, Angeles City, Pampanga College of NursingAly PinpinNo ratings yet
- Somatization ThesisDocument5 pagesSomatization Thesisxlyexqvff100% (3)
- Health Psychology AssignmentDocument12 pagesHealth Psychology AssignmentAnvesha ChoukseyNo ratings yet
- Understanding Hard to Maintain Behaviour Change: A Dual Process ApproachFrom EverandUnderstanding Hard to Maintain Behaviour Change: A Dual Process ApproachNo ratings yet
- Abdul Aziz AssignmentDocument5 pagesAbdul Aziz Assignmentfahad rustamNo ratings yet
- Antipsychotics 1Document41 pagesAntipsychotics 1fahad rustam100% (1)
- Assessment and Treatment of Individuals at High RiDocument8 pagesAssessment and Treatment of Individuals at High Rifahad rustamNo ratings yet
- Assignment 2 Making OBS & EPSDocument3 pagesAssignment 2 Making OBS & EPSfahad rustamNo ratings yet
- EME AttendanceDocument2 pagesEME Attendancefahad rustam100% (1)
- Human Resources (1) NewDocument12 pagesHuman Resources (1) Newfahad rustamNo ratings yet
- Jogging Line Application-1Document1 pageJogging Line Application-1fahad rustam100% (1)
- PQM Assignment 3: Deadline 9-5-2020Document7 pagesPQM Assignment 3: Deadline 9-5-2020fahad rustamNo ratings yet
- Conduct of Academic Audit FinalDocument3 pagesConduct of Academic Audit Finalfahad rustamNo ratings yet
- Competitive Profile MatrixDocument10 pagesCompetitive Profile Matrixfahad rustamNo ratings yet