Download as pdf or txt
You might also like
- John Bird Published by Taylor and FrancisDocument9 pagesJohn Bird Published by Taylor and FrancisromwamaNo ratings yet
- What Is Decarbonization ?: Main Engine Decarb Preparation, Procedure & Commissioning Sumit NarayanDocument3 pagesWhat Is Decarbonization ?: Main Engine Decarb Preparation, Procedure & Commissioning Sumit NarayanManisha100% (1)
- MIPS Simple Pipeline Simulator - Final ReportDocument9 pagesMIPS Simple Pipeline Simulator - Final ReportRawaha Bin KhalidNo ratings yet
- Stardew Valley Community Center ChecklistDocument7 pagesStardew Valley Community Center Checklistpauchanmnl100% (2)
- Coma, Hyperthermia and Bleeding Associated With Massive LSD OverdoseDocument6 pagesComa, Hyperthermia and Bleeding Associated With Massive LSD Overdose0j1u9nmkv534vw9vNo ratings yet
- Module 6.9 TLEDocument115 pagesModule 6.9 TLEroseavy90% (10)
- Materials and MethodsDocument5 pagesMaterials and Methodsike ikeNo ratings yet
- 10.0000@Www - Ncbi.nlm - nih.Gov@Generic 398AABAEB690Document19 pages10.0000@Www - Ncbi.nlm - nih.Gov@Generic 398AABAEB690annyzaukNo ratings yet
- Randomized Trial of Acupuncture To Lower Blood Pressure: HypertensionDocument10 pagesRandomized Trial of Acupuncture To Lower Blood Pressure: HypertensionYoga PermatasariNo ratings yet
- Morning and Evening Blood Pressures Are Associated With Intima-Media Thickness in A General PopulationDocument7 pagesMorning and Evening Blood Pressures Are Associated With Intima-Media Thickness in A General PopulationAgung WistaraNo ratings yet
- Assessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaDocument6 pagesAssessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaprabuNo ratings yet
- Safar ReviewDocument6 pagesSafar ReviewSergio GonzalezNo ratings yet
- Journal EBMDocument12 pagesJournal EBMmairahimadhaniNo ratings yet
- Sex-Related Relationships Between Uric Acid AnDocument8 pagesSex-Related Relationships Between Uric Acid Annguyenthanhluan2801No ratings yet
- The Effects of Verapamil SR and Bisoprolol On Reducing The Sympathetic Nervous System's ActivitDocument4 pagesThe Effects of Verapamil SR and Bisoprolol On Reducing The Sympathetic Nervous System's ActivitDian Sekar LarassatiNo ratings yet
- Effects of Endurance Training On Baroreflex Sensitivity and Blood Pressure in BorderliDocument6 pagesEffects of Endurance Training On Baroreflex Sensitivity and Blood Pressure in BorderliMilenckaVidalConsiglieriNo ratings yet
- Exercise and Weight Loss Reduce Blood Pressure in Men and Women With Mild HypertensionDocument12 pagesExercise and Weight Loss Reduce Blood Pressure in Men and Women With Mild HypertensionAliyah Adek RahmahNo ratings yet
- Proton-Pump Inhibitors Therapy and Blood Pressure ControlDocument6 pagesProton-Pump Inhibitors Therapy and Blood Pressure ControlTeky WidyariniNo ratings yet
- Epidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Document2 pagesEpidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Mirza RisqaNo ratings yet
- Protective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive RatsDocument19 pagesProtective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive Ratsberliana syifaNo ratings yet
- Postexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State CyclingDocument10 pagesPostexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State Cyclingnuttela ismeNo ratings yet
- Nutrition, Metabolism & Cardiovascular DiseasesDocument8 pagesNutrition, Metabolism & Cardiovascular DiseasesDebora AlvesNo ratings yet
- Hypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyDocument7 pagesHypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyIndah SundariNo ratings yet
- Paper Grupo 2Document9 pagesPaper Grupo 2Fiorella LeyvaNo ratings yet
- WongDocument5 pagesWongtalleresccorporal5No ratings yet
- Ali 2018Document1 pageAli 2018cynthia nataliaNo ratings yet
- Chronic Baroreflex Activation Restores Spontaneous Baroreflex Control and Variability of Heart Rate in Obesity-Induced HypertensionDocument10 pagesChronic Baroreflex Activation Restores Spontaneous Baroreflex Control and Variability of Heart Rate in Obesity-Induced HypertensionCaesar Catalin CaratasuNo ratings yet
- 29 493 PDFDocument7 pages29 493 PDFmehrshad Farahpour Gp5No ratings yet
- Global REACH 2018: Volume Regulation in High-Altitude Andeans With and Without Chronic Mountain SicknessDocument9 pagesGlobal REACH 2018: Volume Regulation in High-Altitude Andeans With and Without Chronic Mountain SicknessFiorella LeyvaNo ratings yet
- Dose-Response Association Between Level of Physical Activity and Mortality in Normal, Elevated, and High Blood PressureDocument9 pagesDose-Response Association Between Level of Physical Activity and Mortality in Normal, Elevated, and High Blood PressureChristopher LeNo ratings yet
- Abnormalities of Angiotensin Regulation in PotsDocument14 pagesAbnormalities of Angiotensin Regulation in Potsiri_balNo ratings yet
- BNP in ChagasDocument3 pagesBNP in ChagasJuan Guillermo Pérez CarreñoNo ratings yet
- Non-Invasive Blood Pressure Monitoring Underestimates Hypertensive Response To Exercise in Suspected Heart Failure With Preserved Ejection FractionDocument3 pagesNon-Invasive Blood Pressure Monitoring Underestimates Hypertensive Response To Exercise in Suspected Heart Failure With Preserved Ejection FractionEffendi UChinNo ratings yet
- Cold Pressor Test As A Predictor of HypertensionDocument4 pagesCold Pressor Test As A Predictor of HypertensionBima ZahriNo ratings yet
- HR 2008203Document6 pagesHR 200820322125327No ratings yet
- Experimental Biology and MedicineDocument9 pagesExperimental Biology and Medicineiri_balNo ratings yet
- Effect of BmiDocument5 pagesEffect of BmiSyaiful Putra RanaNo ratings yet
- Hormone Therapy in Postmenopausal WomenDocument8 pagesHormone Therapy in Postmenopausal WomenChyntia Pramita SariNo ratings yet
- Sodium and Potassium Intake in Overweight And.596Document2 pagesSodium and Potassium Intake in Overweight And.596jackie funtanillaNo ratings yet
- Vranish 2016Document7 pagesVranish 2016Jenifer de OliveiraNo ratings yet
- JHH 2013 121Document5 pagesJHH 2013 121adri20121989No ratings yet
- PIH Renal Doppler Pregnancy - CutDocument4 pagesPIH Renal Doppler Pregnancy - CutAnonymous 9QxPDpNo ratings yet
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDocument9 pagesEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNo ratings yet
- 19 03 PDFDocument6 pages19 03 PDFT h o r y n R a m o sNo ratings yet
- Turkish Journal Subclinical HypothyroidismDocument5 pagesTurkish Journal Subclinical HypothyroidismAminaNo ratings yet
- Anggun A. MenawanDocument10 pagesAnggun A. MenawanAisyah MazlanNo ratings yet
- Antihypertensive Drugs: A Perspective On The Value of Improved Blood Pressure Control in The USADocument21 pagesAntihypertensive Drugs: A Perspective On The Value of Improved Blood Pressure Control in The USAjphanindraNo ratings yet
- DIAZ2017 Relation Btween CRF and BP in Young Adult Mediation AnalysisDocument5 pagesDIAZ2017 Relation Btween CRF and BP in Young Adult Mediation AnalysisMumtaz MaulanaNo ratings yet
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDocument6 pagesPostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriNo ratings yet
- En V60n4a06Document5 pagesEn V60n4a06Palwasha MalikNo ratings yet
- Jact 10 I 3 P 190Document5 pagesJact 10 I 3 P 190Chiranjeevi Kumar EndukuruNo ratings yet
- Association of Orthostatic Hypotension WithDocument11 pagesAssociation of Orthostatic Hypotension WithAulia Whiratama PutraNo ratings yet
- Aps 2011118 ADocument6 pagesAps 2011118 ADaniel Lee Eisenberg JacobsNo ratings yet
- The Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineDocument6 pagesThe Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineAnonymous K9tmd7T0PzNo ratings yet
- Pulse Rate Variability Is Not A Surrogate For Heart Rate VariabilityDocument7 pagesPulse Rate Variability Is Not A Surrogate For Heart Rate VariabilityFiras ZakNo ratings yet
- 10 1016@j Medcle 2016 11 016 PDFDocument6 pages10 1016@j Medcle 2016 11 016 PDFlabibah mahmudaNo ratings yet
- Nejmoa 2215025Document11 pagesNejmoa 2215025pharmaNo ratings yet
- Diferent Exercise TrainingDocument9 pagesDiferent Exercise TrainingRenan Carraro RosaNo ratings yet
- CoQ 10 in HypertensionDocument6 pagesCoQ 10 in HypertensionHendri YantoNo ratings yet
- Prehypertensive State, Mild Hypertension, Metabolic Syndrome and Cardiovascular Risk Factors Among Young Adults in Rural MalaysiaDocument8 pagesPrehypertensive State, Mild Hypertension, Metabolic Syndrome and Cardiovascular Risk Factors Among Young Adults in Rural MalaysiaIndah SundariNo ratings yet
- Plasma Adrenomedullin Level and Development of Hypertension: Original ArticleDocument5 pagesPlasma Adrenomedullin Level and Development of Hypertension: Original ArticleCharles KalangiNo ratings yet
- 4 I PDFDocument6 pages4 I PDFDaniel Fernando Mendez CarbajalNo ratings yet
- Phisiological Response Anxiety CardioddDocument13 pagesPhisiological Response Anxiety CardioddCatalina CordonasuNo ratings yet
- JurnalDocument6 pagesJurnaldr.d4No ratings yet
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
- 2005 Prevention of Obesity in MiceDocument9 pages2005 Prevention of Obesity in MiceFerroBemNo ratings yet
- A Novel Function For Fatty Acid Translocase (FAT) CD36 Involvement in Long Chain Fatty Acid TransfDocument7 pagesA Novel Function For Fatty Acid Translocase (FAT) CD36 Involvement in Long Chain Fatty Acid TransfFerroBemNo ratings yet
- 78 Physiological and Metabolic Responses To A Hill WalkDocument9 pages78 Physiological and Metabolic Responses To A Hill WalkFerroBemNo ratings yet
- 55 Waging War On Physical Inactivity Using ModernDocument28 pages55 Waging War On Physical Inactivity Using ModernFerroBemNo ratings yet
- 52 Oral (13C) Glucose Oxidation During Prolonged ExerciseDocument8 pages52 Oral (13C) Glucose Oxidation During Prolonged ExerciseFerroBemNo ratings yet
- 56 Dietary Carbohydrate, Muscle Glycogen Content, andDocument8 pages56 Dietary Carbohydrate, Muscle Glycogen Content, andFerroBemNo ratings yet
- 46 Pyruvate Ingestion For 7 Days Does Not ImproveDocument8 pages46 Pyruvate Ingestion For 7 Days Does Not ImproveFerroBemNo ratings yet
- PAFLU Vs Sec of LaborDocument1 pagePAFLU Vs Sec of LaborMavic Morales100% (1)
- 1700 N Manhattan Ave - Royal Towers - Notice of CondemnationDocument14 pages1700 N Manhattan Ave - Royal Towers - Notice of CondemnationMatthew SelfNo ratings yet
- Opsrey - Acre 1291Document97 pagesOpsrey - Acre 1291Hieronymus Sousa PintoNo ratings yet
- Documents That Need To Be Submitted During TCSDocument4 pagesDocuments That Need To Be Submitted During TCSAnkur AgrawalNo ratings yet
- Topic On CC11Document3 pagesTopic On CC11Free HitNo ratings yet
- 6º Ano Ingles Unit4 Test3Document3 pages6º Ano Ingles Unit4 Test3Paula Lopes100% (1)
- 6 Feasibility Assessment ToolDocument5 pages6 Feasibility Assessment Toolalibaba1888No ratings yet
- CS701 - Theory of Computation Assignment No.1: InstructionsDocument2 pagesCS701 - Theory of Computation Assignment No.1: InstructionsIhsanullah KhanNo ratings yet
- The Brain and Nervous System (Psychology) Unit 14: An Academic ReportDocument7 pagesThe Brain and Nervous System (Psychology) Unit 14: An Academic ReportOlatokunbo SinaayomiNo ratings yet
- BIRD Internet Routing DaemonDocument4 pagesBIRD Internet Routing DaemonAleksandra FeyNo ratings yet
- Asterisk For Dumb MeDocument164 pagesAsterisk For Dumb MeAndy CockroftNo ratings yet
- ISC 2016 Chemistry Paper 2 Practical SolvedDocument12 pagesISC 2016 Chemistry Paper 2 Practical SolvedMritunjay Kumar SharmaNo ratings yet
- Ateneo Philosophy Club: Project ProposalDocument2 pagesAteneo Philosophy Club: Project ProposalArmando MataNo ratings yet
- WPP2019 Pop F01 2 Total Population MaleDocument547 pagesWPP2019 Pop F01 2 Total Population MaleMaria BozhkoNo ratings yet
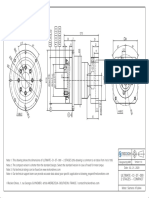
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- Pawan's ResumeDocument1 pagePawan's ResumePAWAN YADAVNo ratings yet
- Money Laundering, Terrorism Financing in NigeriaDocument7 pagesMoney Laundering, Terrorism Financing in NigeriaThe Law Brigade (Journals) PublishersNo ratings yet
- Crane Design Guide 2Document8 pagesCrane Design Guide 2Mesfin Derbew0% (1)
- CadburyDocument24 pagesCadburyDeepti Mangal50% (2)
- Crypt Arithmatic Problem SolutionDocument10 pagesCrypt Arithmatic Problem SolutionHariom Patel100% (4)
- Chapter 9 LectureDocument29 pagesChapter 9 Lectureinam vf100% (6)
- Project On Trigonometry: Designed By:-Shubham Kumar 10 D Roll No: - 6Document36 pagesProject On Trigonometry: Designed By:-Shubham Kumar 10 D Roll No: - 6Surbhi Nagpal AhujaNo ratings yet
- John Hagstrom: Philip BiggsDocument4 pagesJohn Hagstrom: Philip BiggsDarci HallNo ratings yet
- PetretecDocument8 pagesPetretecVenkatesan KrishnachariNo ratings yet
- Sabam Sariaman CVDocument1 pageSabam Sariaman CVsabamsiregarNo ratings yet