
The Endocrine System
The Endocrine System
You might also like
- Topic 10Document17 pagesTopic 10Lorraine RiegoNo ratings yet
- Johanna Jane H. Macasero - Endocrine System TranscriptDocument13 pagesJohanna Jane H. Macasero - Endocrine System TranscriptJohanna MacaseroNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemSuzette MalibagoNo ratings yet
- EndocrineDocument12 pagesEndocrinejamille consingNo ratings yet
- EndocrineDocument2 pagesEndocrineHoney Mie MorenoNo ratings yet
- UntitledDocument12 pagesUntitledDerrick kinyaNo ratings yet
- The Endocrine System Consists of Hormones Secreted by Glands Traveling Through The Blood To Target TissuesDocument16 pagesThe Endocrine System Consists of Hormones Secreted by Glands Traveling Through The Blood To Target TissuesAljon AniesNo ratings yet
- UntitledDocument2 pagesUntitledJhannyt Jyn BasaloNo ratings yet
- Clinton Hackney Anatomy & Physiology II BctcsDocument65 pagesClinton Hackney Anatomy & Physiology II BctcsJack HolthouseNo ratings yet
- Mcqs of Endocrine SystemDocument25 pagesMcqs of Endocrine SystemkajuNo ratings yet
- Sheena Khan: Biochemistry Generiic Bs NursingDocument22 pagesSheena Khan: Biochemistry Generiic Bs NursingsharmeenNo ratings yet
- Chapter 9Document8 pagesChapter 9Bea SeloterioNo ratings yet
- Endocrine Anatomy and PhysiologyDocument10 pagesEndocrine Anatomy and PhysiologyJojo JustoNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Bio ReportDocument4 pagesBio ReportKate MabanagNo ratings yet
- EndokrinDocument70 pagesEndokrinNur Hadi PrayitnoNo ratings yet
- The Endocrine SystemDocument12 pagesThe Endocrine Systemmagma_pt9888No ratings yet
- Endocrine System: EndocrinologyDocument10 pagesEndocrine System: EndocrinologyAnya IgnacioNo ratings yet
- Chapter - 17 PhysiologyDocument49 pagesChapter - 17 PhysiologyAhsanullah PathanNo ratings yet
- ENDOCRINE SYSTEM - Anatomy and PhysiologyDocument10 pagesENDOCRINE SYSTEM - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- Endocine System Physiology 20-4-2020Document61 pagesEndocine System Physiology 20-4-2020Farah AljayyousiNo ratings yet
- Care of Clients With Problem On EndocrineDocument48 pagesCare of Clients With Problem On EndocrineAngel CauilanNo ratings yet
- Endocrine System HandoutsDocument5 pagesEndocrine System HandoutsBeatriz IcayNo ratings yet
- Chapter 16 - The Endocrine SystemDocument73 pagesChapter 16 - The Endocrine SystemAbdullah AlghamdiNo ratings yet
- Endocrine System: DR - Entissar Mansour 2O16-2017Document162 pagesEndocrine System: DR - Entissar Mansour 2O16-2017Zainab Alshamary100% (1)
- Human Anatomy & Physiology: Autonomic Nervous SystemDocument8 pagesHuman Anatomy & Physiology: Autonomic Nervous SystemBeth EchavezNo ratings yet
- Chap 3 Reproductive Hormones of Female AnimalsDocument80 pagesChap 3 Reproductive Hormones of Female Animalsyabsiradaniel930No ratings yet
- The Endocrine System: An OverviewDocument12 pagesThe Endocrine System: An Overviewlovelyc95No ratings yet
- Endocrine SystemDocument95 pagesEndocrine SystemUmar Ilyasu JibrilNo ratings yet
- Endocrinology IntroductionDocument43 pagesEndocrinology IntroductionDICKSONNo ratings yet
- LMS Endocrine SystemDocument23 pagesLMS Endocrine Systemhakdog hakdogNo ratings yet
- Anfis Endokrin S2 (Compatibility Mode) .CompressedDocument66 pagesAnfis Endokrin S2 (Compatibility Mode) .CompressedAmiliya EmilNo ratings yet
- Endocrine System: Hypophysis Sella Turcica Pituitary HypophysialDocument2 pagesEndocrine System: Hypophysis Sella Turcica Pituitary HypophysialMikaela MosqueraNo ratings yet
- Introduction To EndocrinologyDocument12 pagesIntroduction To EndocrinologyBunny OzuNo ratings yet
- Chapter 34 - Introduction To The Endocrine SystemDocument3 pagesChapter 34 - Introduction To The Endocrine Systemkdayeon018No ratings yet
- Advanced_Physiology_and_Pathophysiology_Essentials..._----_(Hypothalamus_and_Pituitary_Gland)Document1 pageAdvanced_Physiology_and_Pathophysiology_Essentials..._----_(Hypothalamus_and_Pituitary_Gland)Ann MariletteNo ratings yet
- Hormones, ClassificationDocument10 pagesHormones, ClassificationMenoNo ratings yet
- Forelæsning 3Document8 pagesForelæsning 3natashathelinNo ratings yet
- Suplemen Materi HormonDocument16 pagesSuplemen Materi Hormonnali fazaNo ratings yet
- Endocrine System: A & P-Ii Unit VDocument25 pagesEndocrine System: A & P-Ii Unit VAsad KHANNo ratings yet
- The Endocrine System - PMCDocument20 pagesThe Endocrine System - PMCStephanie TeddNo ratings yet
- Topic 1 Endocrine SystemDocument140 pagesTopic 1 Endocrine SystemmasdfgNo ratings yet
- Endocrine ReviewerDocument5 pagesEndocrine ReviewerAshley MalolotNo ratings yet
- PHR 121 Anatomy & Physiology: Diploma in PharmacyDocument51 pagesPHR 121 Anatomy & Physiology: Diploma in PharmacyAzmi ArifinNo ratings yet
- Adrenocorticotropic Hormone (ACTH) From The Anterior Pituitary Gland Specifically StimulatesDocument2 pagesAdrenocorticotropic Hormone (ACTH) From The Anterior Pituitary Gland Specifically StimulatesStjepan ErženNo ratings yet
- Endocrine PhysiologyDocument79 pagesEndocrine PhysiologyCHALIE MEQUNo ratings yet
- Anatomy and Physiology-Endocrine SystemDocument5 pagesAnatomy and Physiology-Endocrine SystemEixid Enna YeLik100% (1)
- Endocrine System Endocrine System: "The Body Regulator"Document31 pagesEndocrine System Endocrine System: "The Body Regulator"angelus008No ratings yet
- Endocrine ReviewerDocument5 pagesEndocrine ReviewerAshley MalolotNo ratings yet
- ENDOCRINE SYSTEMDocument3 pagesENDOCRINE SYSTEMveraabalossarahmaeNo ratings yet
- Endocrinology Apllied ScienceDocument44 pagesEndocrinology Apllied ScienceAdam PrabowoNo ratings yet
- Chemistry of HormonesDocument10 pagesChemistry of HormonesRuqayya ImranNo ratings yet
- ANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIDocument9 pagesANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIAmoroso, Marian Corneth D.No ratings yet
- Hormones:: Signaling MoleculesDocument20 pagesHormones:: Signaling MoleculesSangeeta DwivediNo ratings yet
- Lec.12 Introd To Hormones 2018Document29 pagesLec.12 Introd To Hormones 2018sofiaNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
- Coordination of Body Functions by Chemical MessengerDocument6 pagesCoordination of Body Functions by Chemical MessengerHorain FatimaNo ratings yet
- Introduction To EndocrinologyDocument15 pagesIntroduction To Endocrinologykazim786ahmedNo ratings yet
- Endocrine System: A Tutorial Study GuideFrom EverandEndocrine System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (1)
- Lesson 7Document42 pagesLesson 7속강대No ratings yet
- Specific PathoDocument3 pagesSpecific Patho속강대No ratings yet
- Geriang Ina NCP UliDocument12 pagesGeriang Ina NCP Uli속강대No ratings yet
- NCP Ms Case PresDocument9 pagesNCP Ms Case Pres속강대No ratings yet
- When A Child Has A Cardiovascular Disorder: Nursing Care of A FamilyDocument152 pagesWhen A Child Has A Cardiovascular Disorder: Nursing Care of A Family속강대No ratings yet
- Review Notes in Plane Trigonometry Functions of A Right Triangle (SOH-CAH-TOA)Document7 pagesReview Notes in Plane Trigonometry Functions of A Right Triangle (SOH-CAH-TOA)속강대No ratings yet
- Hemodialysis PDFDocument880 pagesHemodialysis PDFmmm777maribel100% (2)
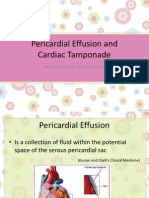
- Pericardial Effusion and Cardiac TamponadeDocument18 pagesPericardial Effusion and Cardiac TamponadeSiti Hamidah Abd Aziz100% (1)
- Periocarditis: A) Acute PericarditisDocument4 pagesPeriocarditis: A) Acute Pericarditisssuhass243No ratings yet
- National NORCET-3 - FinalDocument90 pagesNational NORCET-3 - FinalSHIVANIINo ratings yet
- Antiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Document1 pageAntiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Ponpimol Odee BongkeawNo ratings yet
- What Are The Health Benefits of ExerciseDocument2 pagesWhat Are The Health Benefits of ExerciseJoycs PintoNo ratings yet
- DR Syed Sadakathulla Bakhtiari Baqavi: 46. Asbabe Waba Ko Ibn Sina Ne Btaya Hai Jo Four HainDocument22 pagesDR Syed Sadakathulla Bakhtiari Baqavi: 46. Asbabe Waba Ko Ibn Sina Ne Btaya Hai Jo Four HainMd QasimNo ratings yet
- Algorithms - Paediatric Advanced Life Support PDFDocument1 pageAlgorithms - Paediatric Advanced Life Support PDFLenox BlackNo ratings yet
- Chronic HK NewInsightDocument107 pagesChronic HK NewInsightKHALID NAAMNo ratings yet
- Congestive Heart FailureDocument64 pagesCongestive Heart FailureBentoys StreetNo ratings yet
- Sledai-2K: Data Collection Sheet: Total ScoreDocument1 pageSledai-2K: Data Collection Sheet: Total ScoreSuryadi Limardi0% (1)
- CARDIOresp AssesmentDocument11 pagesCARDIOresp AssesmentshivaniNo ratings yet
- Heart Valve SelectionDocument16 pagesHeart Valve Selectionfelixsafar3243No ratings yet
- Drug Study Template 1Document2 pagesDrug Study Template 1Karylle Joy WacguisanNo ratings yet
- Pharmacist MCQ Review 2019Document316 pagesPharmacist MCQ Review 2019Ali Adnan Afridi100% (3)
- Initial Management Chest Pain1Document12 pagesInitial Management Chest Pain1Mohd Faizal SimonNo ratings yet
- Anatomy SBA MCQ eMRCSDocument81 pagesAnatomy SBA MCQ eMRCSTowhid HasanNo ratings yet
- Anatomy of Urinary Tract-Netter PDFDocument64 pagesAnatomy of Urinary Tract-Netter PDFJanu Arman100% (1)
- Interstitial Diffuse Lung Disease Patient QuestionnaireDocument4 pagesInterstitial Diffuse Lung Disease Patient QuestionnaireJamban08No ratings yet
- 5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THDocument6 pages5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THRomeo AragonNo ratings yet
- HMS - Women's Health (MCQ & Notes)Document44 pagesHMS - Women's Health (MCQ & Notes)marouf elgoulNo ratings yet
- Urine Formation and Routine TestDocument22 pagesUrine Formation and Routine Testabigail lausNo ratings yet
- ICD 11 ExercisesDocument30 pagesICD 11 Exerciseszawiyah GhaniNo ratings yet
- Case Study: Hyponatremia: Bicol University College of NursingDocument34 pagesCase Study: Hyponatremia: Bicol University College of NursingDaniel Angelo ArangoNo ratings yet
- CCHD Screening - MohDocument6 pagesCCHD Screening - MohAhmed Mohammed100% (1)
- SINGKATANDocument26 pagesSINGKATANOkto FanesaNo ratings yet
- Hypertension in Geriatrics 2010Document51 pagesHypertension in Geriatrics 2010Andre HawkNo ratings yet
- Blood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseDocument14 pagesBlood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseNorries Jonell CaballarNo ratings yet
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- 1 PredDocument7 pages1 PredandreaNo ratings yet






























































































Download as pdf or txt
You might also like
- Topic 10Document17 pagesTopic 10Lorraine RiegoNo ratings yet
- Johanna Jane H. Macasero - Endocrine System TranscriptDocument13 pagesJohanna Jane H. Macasero - Endocrine System TranscriptJohanna MacaseroNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemSuzette MalibagoNo ratings yet
- EndocrineDocument12 pagesEndocrinejamille consingNo ratings yet
- EndocrineDocument2 pagesEndocrineHoney Mie MorenoNo ratings yet
- UntitledDocument12 pagesUntitledDerrick kinyaNo ratings yet
- The Endocrine System Consists of Hormones Secreted by Glands Traveling Through The Blood To Target TissuesDocument16 pagesThe Endocrine System Consists of Hormones Secreted by Glands Traveling Through The Blood To Target TissuesAljon AniesNo ratings yet
- UntitledDocument2 pagesUntitledJhannyt Jyn BasaloNo ratings yet
- Clinton Hackney Anatomy & Physiology II BctcsDocument65 pagesClinton Hackney Anatomy & Physiology II BctcsJack HolthouseNo ratings yet
- Mcqs of Endocrine SystemDocument25 pagesMcqs of Endocrine SystemkajuNo ratings yet
- Sheena Khan: Biochemistry Generiic Bs NursingDocument22 pagesSheena Khan: Biochemistry Generiic Bs NursingsharmeenNo ratings yet
- Chapter 9Document8 pagesChapter 9Bea SeloterioNo ratings yet
- Endocrine Anatomy and PhysiologyDocument10 pagesEndocrine Anatomy and PhysiologyJojo JustoNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Bio ReportDocument4 pagesBio ReportKate MabanagNo ratings yet
- EndokrinDocument70 pagesEndokrinNur Hadi PrayitnoNo ratings yet
- The Endocrine SystemDocument12 pagesThe Endocrine Systemmagma_pt9888No ratings yet
- Endocrine System: EndocrinologyDocument10 pagesEndocrine System: EndocrinologyAnya IgnacioNo ratings yet
- Chapter - 17 PhysiologyDocument49 pagesChapter - 17 PhysiologyAhsanullah PathanNo ratings yet
- ENDOCRINE SYSTEM - Anatomy and PhysiologyDocument10 pagesENDOCRINE SYSTEM - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- Endocine System Physiology 20-4-2020Document61 pagesEndocine System Physiology 20-4-2020Farah AljayyousiNo ratings yet
- Care of Clients With Problem On EndocrineDocument48 pagesCare of Clients With Problem On EndocrineAngel CauilanNo ratings yet
- Endocrine System HandoutsDocument5 pagesEndocrine System HandoutsBeatriz IcayNo ratings yet
- Chapter 16 - The Endocrine SystemDocument73 pagesChapter 16 - The Endocrine SystemAbdullah AlghamdiNo ratings yet
- Endocrine System: DR - Entissar Mansour 2O16-2017Document162 pagesEndocrine System: DR - Entissar Mansour 2O16-2017Zainab Alshamary100% (1)
- Human Anatomy & Physiology: Autonomic Nervous SystemDocument8 pagesHuman Anatomy & Physiology: Autonomic Nervous SystemBeth EchavezNo ratings yet
- Chap 3 Reproductive Hormones of Female AnimalsDocument80 pagesChap 3 Reproductive Hormones of Female Animalsyabsiradaniel930No ratings yet
- The Endocrine System: An OverviewDocument12 pagesThe Endocrine System: An Overviewlovelyc95No ratings yet
- Endocrine SystemDocument95 pagesEndocrine SystemUmar Ilyasu JibrilNo ratings yet
- Endocrinology IntroductionDocument43 pagesEndocrinology IntroductionDICKSONNo ratings yet
- LMS Endocrine SystemDocument23 pagesLMS Endocrine Systemhakdog hakdogNo ratings yet
- Anfis Endokrin S2 (Compatibility Mode) .CompressedDocument66 pagesAnfis Endokrin S2 (Compatibility Mode) .CompressedAmiliya EmilNo ratings yet
- Endocrine System: Hypophysis Sella Turcica Pituitary HypophysialDocument2 pagesEndocrine System: Hypophysis Sella Turcica Pituitary HypophysialMikaela MosqueraNo ratings yet
- Introduction To EndocrinologyDocument12 pagesIntroduction To EndocrinologyBunny OzuNo ratings yet
- Chapter 34 - Introduction To The Endocrine SystemDocument3 pagesChapter 34 - Introduction To The Endocrine Systemkdayeon018No ratings yet
- Advanced_Physiology_and_Pathophysiology_Essentials..._----_(Hypothalamus_and_Pituitary_Gland)Document1 pageAdvanced_Physiology_and_Pathophysiology_Essentials..._----_(Hypothalamus_and_Pituitary_Gland)Ann MariletteNo ratings yet
- Hormones, ClassificationDocument10 pagesHormones, ClassificationMenoNo ratings yet
- Forelæsning 3Document8 pagesForelæsning 3natashathelinNo ratings yet
- Suplemen Materi HormonDocument16 pagesSuplemen Materi Hormonnali fazaNo ratings yet
- Endocrine System: A & P-Ii Unit VDocument25 pagesEndocrine System: A & P-Ii Unit VAsad KHANNo ratings yet
- The Endocrine System - PMCDocument20 pagesThe Endocrine System - PMCStephanie TeddNo ratings yet
- Topic 1 Endocrine SystemDocument140 pagesTopic 1 Endocrine SystemmasdfgNo ratings yet
- Endocrine ReviewerDocument5 pagesEndocrine ReviewerAshley MalolotNo ratings yet
- PHR 121 Anatomy & Physiology: Diploma in PharmacyDocument51 pagesPHR 121 Anatomy & Physiology: Diploma in PharmacyAzmi ArifinNo ratings yet
- Adrenocorticotropic Hormone (ACTH) From The Anterior Pituitary Gland Specifically StimulatesDocument2 pagesAdrenocorticotropic Hormone (ACTH) From The Anterior Pituitary Gland Specifically StimulatesStjepan ErženNo ratings yet
- Endocrine PhysiologyDocument79 pagesEndocrine PhysiologyCHALIE MEQUNo ratings yet
- Anatomy and Physiology-Endocrine SystemDocument5 pagesAnatomy and Physiology-Endocrine SystemEixid Enna YeLik100% (1)
- Endocrine System Endocrine System: "The Body Regulator"Document31 pagesEndocrine System Endocrine System: "The Body Regulator"angelus008No ratings yet
- Endocrine ReviewerDocument5 pagesEndocrine ReviewerAshley MalolotNo ratings yet
- ENDOCRINE SYSTEMDocument3 pagesENDOCRINE SYSTEMveraabalossarahmaeNo ratings yet
- Endocrinology Apllied ScienceDocument44 pagesEndocrinology Apllied ScienceAdam PrabowoNo ratings yet
- Chemistry of HormonesDocument10 pagesChemistry of HormonesRuqayya ImranNo ratings yet
- ANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIDocument9 pagesANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIAmoroso, Marian Corneth D.No ratings yet
- Hormones:: Signaling MoleculesDocument20 pagesHormones:: Signaling MoleculesSangeeta DwivediNo ratings yet
- Lec.12 Introd To Hormones 2018Document29 pagesLec.12 Introd To Hormones 2018sofiaNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
- Coordination of Body Functions by Chemical MessengerDocument6 pagesCoordination of Body Functions by Chemical MessengerHorain FatimaNo ratings yet
- Introduction To EndocrinologyDocument15 pagesIntroduction To Endocrinologykazim786ahmedNo ratings yet
- Endocrine System: A Tutorial Study GuideFrom EverandEndocrine System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (1)
- Lesson 7Document42 pagesLesson 7속강대No ratings yet
- Specific PathoDocument3 pagesSpecific Patho속강대No ratings yet
- Geriang Ina NCP UliDocument12 pagesGeriang Ina NCP Uli속강대No ratings yet
- NCP Ms Case PresDocument9 pagesNCP Ms Case Pres속강대No ratings yet
- When A Child Has A Cardiovascular Disorder: Nursing Care of A FamilyDocument152 pagesWhen A Child Has A Cardiovascular Disorder: Nursing Care of A Family속강대No ratings yet
- Review Notes in Plane Trigonometry Functions of A Right Triangle (SOH-CAH-TOA)Document7 pagesReview Notes in Plane Trigonometry Functions of A Right Triangle (SOH-CAH-TOA)속강대No ratings yet
- Hemodialysis PDFDocument880 pagesHemodialysis PDFmmm777maribel100% (2)
- Pericardial Effusion and Cardiac TamponadeDocument18 pagesPericardial Effusion and Cardiac TamponadeSiti Hamidah Abd Aziz100% (1)
- Periocarditis: A) Acute PericarditisDocument4 pagesPeriocarditis: A) Acute Pericarditisssuhass243No ratings yet
- National NORCET-3 - FinalDocument90 pagesNational NORCET-3 - FinalSHIVANIINo ratings yet
- Antiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Document1 pageAntiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Ponpimol Odee BongkeawNo ratings yet
- What Are The Health Benefits of ExerciseDocument2 pagesWhat Are The Health Benefits of ExerciseJoycs PintoNo ratings yet
- DR Syed Sadakathulla Bakhtiari Baqavi: 46. Asbabe Waba Ko Ibn Sina Ne Btaya Hai Jo Four HainDocument22 pagesDR Syed Sadakathulla Bakhtiari Baqavi: 46. Asbabe Waba Ko Ibn Sina Ne Btaya Hai Jo Four HainMd QasimNo ratings yet
- Algorithms - Paediatric Advanced Life Support PDFDocument1 pageAlgorithms - Paediatric Advanced Life Support PDFLenox BlackNo ratings yet
- Chronic HK NewInsightDocument107 pagesChronic HK NewInsightKHALID NAAMNo ratings yet
- Congestive Heart FailureDocument64 pagesCongestive Heart FailureBentoys StreetNo ratings yet
- Sledai-2K: Data Collection Sheet: Total ScoreDocument1 pageSledai-2K: Data Collection Sheet: Total ScoreSuryadi Limardi0% (1)
- CARDIOresp AssesmentDocument11 pagesCARDIOresp AssesmentshivaniNo ratings yet
- Heart Valve SelectionDocument16 pagesHeart Valve Selectionfelixsafar3243No ratings yet
- Drug Study Template 1Document2 pagesDrug Study Template 1Karylle Joy WacguisanNo ratings yet
- Pharmacist MCQ Review 2019Document316 pagesPharmacist MCQ Review 2019Ali Adnan Afridi100% (3)
- Initial Management Chest Pain1Document12 pagesInitial Management Chest Pain1Mohd Faizal SimonNo ratings yet
- Anatomy SBA MCQ eMRCSDocument81 pagesAnatomy SBA MCQ eMRCSTowhid HasanNo ratings yet
- Anatomy of Urinary Tract-Netter PDFDocument64 pagesAnatomy of Urinary Tract-Netter PDFJanu Arman100% (1)
- Interstitial Diffuse Lung Disease Patient QuestionnaireDocument4 pagesInterstitial Diffuse Lung Disease Patient QuestionnaireJamban08No ratings yet
- 5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THDocument6 pages5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THRomeo AragonNo ratings yet
- HMS - Women's Health (MCQ & Notes)Document44 pagesHMS - Women's Health (MCQ & Notes)marouf elgoulNo ratings yet
- Urine Formation and Routine TestDocument22 pagesUrine Formation and Routine Testabigail lausNo ratings yet
- ICD 11 ExercisesDocument30 pagesICD 11 Exerciseszawiyah GhaniNo ratings yet
- Case Study: Hyponatremia: Bicol University College of NursingDocument34 pagesCase Study: Hyponatremia: Bicol University College of NursingDaniel Angelo ArangoNo ratings yet
- CCHD Screening - MohDocument6 pagesCCHD Screening - MohAhmed Mohammed100% (1)
- SINGKATANDocument26 pagesSINGKATANOkto FanesaNo ratings yet
- Hypertension in Geriatrics 2010Document51 pagesHypertension in Geriatrics 2010Andre HawkNo ratings yet
- Blood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseDocument14 pagesBlood Sugar Lowering Effect of Zinc and Multi Vitamin/ Mineral Supplementation Is Dependent On Initial Fasting Blood GlucoseNorries Jonell CaballarNo ratings yet
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- 1 PredDocument7 pages1 PredandreaNo ratings yet