Download as pdf or txt
You might also like
- Antifungal DrugsDocument35 pagesAntifungal Drugsn4pnjfk6rbNo ratings yet
- Antifungal Agent PPT PresentationDocument38 pagesAntifungal Agent PPT Presentationdinberu tadesseNo ratings yet
- Antifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BDocument23 pagesAntifungal Drugs: Side Effects and Adverse Reactions of Amphotericin BElizabeth IdananNo ratings yet
- Antifungaldrugs 150519204813 Lva1 App6892Document54 pagesAntifungaldrugs 150519204813 Lva1 App6892Jennifer S ZiegenNo ratings yet
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Antifungal Drugs: Anti-Infectives and Anti-Inflammatory: Ncm106 - Pharmacology 2 Semester, AY 2020-2021Document34 pagesAntifungal Drugs: Anti-Infectives and Anti-Inflammatory: Ncm106 - Pharmacology 2 Semester, AY 2020-2021imnas100% (1)
- AntifungalDocument22 pagesAntifungalhenokt129No ratings yet
- Clinical Pharmacy: Antifungal & AntiviralDocument7 pagesClinical Pharmacy: Antifungal & Antiviralوقت بدل ضايعNo ratings yet
- Case PresentationDocument16 pagesCase PresentationGurudatta G SNo ratings yet
- Antimicrobials: Dr. Ahmed Mohammed Elamin PHD of Clinical PharmacolgyDocument44 pagesAntimicrobials: Dr. Ahmed Mohammed Elamin PHD of Clinical PharmacolgyAhmed MawiaNo ratings yet
- PHARMADocument25 pagesPHARMAAtteya Mogote AbdullahNo ratings yet
- Otiflox New Ear DropsDocument9 pagesOtiflox New Ear DropsShreyas ModiNo ratings yet
- Antifungal AgentsDocument42 pagesAntifungal AgentsOluwatobi AyomideNo ratings yet
- Pharmacology AntifungalsDocument24 pagesPharmacology AntifungalsAbdul qadeer100% (1)
- 1.antifungal Drug Derma Presentation .DoneDocument38 pages1.antifungal Drug Derma Presentation .Donesahghanshyam9160No ratings yet
- Antifungals Student'sDocument34 pagesAntifungals Student'sapril jholynna garroNo ratings yet
- Revized 5 - Antifungal Medications - 2021Document28 pagesRevized 5 - Antifungal Medications - 2021احمد علىNo ratings yet
- Antifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Document37 pagesAntifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Hafsat JimetaNo ratings yet
- K100170188 - Nur Fajar Istiqomah - Fitoterapi TuberkulosisDocument21 pagesK100170188 - Nur Fajar Istiqomah - Fitoterapi Tuberkulosis7188Nur Fajar IstiqomahNo ratings yet
- Antifungal Drugs: Activity No. 7Document16 pagesAntifungal Drugs: Activity No. 7Junah SeninaNo ratings yet
- AntifungalDocument41 pagesAntifungalDeribe BekeleNo ratings yet
- Prepared by The: Antibiotic Guidelines 3 Edition 2011Document82 pagesPrepared by The: Antibiotic Guidelines 3 Edition 2011araNo ratings yet
- PRESENTED TO: Sir Zafar Iqbal Presented By: Group-EDocument31 pagesPRESENTED TO: Sir Zafar Iqbal Presented By: Group-EAdia MasooraNo ratings yet
- Anti Fungal 180303181604Document51 pagesAnti Fungal 180303181604Alfredo SarachoNo ratings yet
- Antibiotics Simplified 1st Edition DR - Osama Ma3rofDocument57 pagesAntibiotics Simplified 1st Edition DR - Osama Ma3rofDark AngelNo ratings yet
- Antifungal DrugsDocument43 pagesAntifungal DrugsMohammed WasimNo ratings yet
- Antifungal Agents: Dewi Selvina R & Instiaty Department of Pharmacology FmuiDocument37 pagesAntifungal Agents: Dewi Selvina R & Instiaty Department of Pharmacology Fmuisalsa2506No ratings yet
- Antifungals Agents ReviewerDocument4 pagesAntifungals Agents ReviewerSITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- All PharmcoDocument36 pagesAll PharmcoBridged AgukoNo ratings yet
- Antifungal Drugs 3Document54 pagesAntifungal Drugs 3Mikee MeladNo ratings yet
- Anthelmentics Version 2Document21 pagesAnthelmentics Version 2N Gv FcNo ratings yet
- 8 AntifungalDocument10 pages8 Antifungalnusaiba.alobaidyNo ratings yet
- Antifungal AgentsDocument72 pagesAntifungal AgentsChristine OnyangoNo ratings yet
- SK Suruj, Medicinal Chemistry III, Roll No - 38301921059, 3rd Year 6th Sem..PDF Ca2Document10 pagesSK Suruj, Medicinal Chemistry III, Roll No - 38301921059, 3rd Year 6th Sem..PDF Ca2Sk SurajNo ratings yet
- Drugs Used in Infections (Chemotherapeutic AgentsDocument683 pagesDrugs Used in Infections (Chemotherapeutic AgentsKobby AmoahNo ratings yet
- AntifungalDocument20 pagesAntifungalAliImadAlKhasakiNo ratings yet
- Anti Fungal: Dr. Dr. Nico L Lumbuun, SPFKDocument45 pagesAnti Fungal: Dr. Dr. Nico L Lumbuun, SPFKAudhrey BNo ratings yet
- Hiv & Aids-Related Drugs: Pharma - Semis GutierrezDocument3 pagesHiv & Aids-Related Drugs: Pharma - Semis GutierrezYsabelle GutierrezNo ratings yet
- Drug Use in LeprosyDocument23 pagesDrug Use in LeprosyIrish Nicole DCNo ratings yet
- 14-Antiameobic Antifungal 2021Document22 pages14-Antiameobic Antifungal 2021Amr SalemNo ratings yet
- Antifungal DrugsDocument66 pagesAntifungal DrugsMalueth AnguiNo ratings yet
- Damage To Cell MembraneDocument7 pagesDamage To Cell MembraneEsteph CortesNo ratings yet
- Antifungal Drugs0Document26 pagesAntifungal Drugs0yaya mohaNo ratings yet
- Nursing Management of Anti Fungal DrugsDocument25 pagesNursing Management of Anti Fungal DrugsJennyDaniel100% (1)
- Definition of Antifungal DrugsDocument11 pagesDefinition of Antifungal DrugsShah ZebNo ratings yet
- Pharmacology of Antituberculosis Drugs: DR - Datten Bangun MSC, SPFK Dept - Farmakologi & Terapeutik Fak - Kedokteran UhnDocument45 pagesPharmacology of Antituberculosis Drugs: DR - Datten Bangun MSC, SPFK Dept - Farmakologi & Terapeutik Fak - Kedokteran UhnPutri Rahmi MaharaniNo ratings yet
- Antimicrobial AgentsDocument14 pagesAntimicrobial AgentsMay Chelle ErazoNo ratings yet
- NCM 106 AntibacterialDocument11 pagesNCM 106 AntibacterialBruno, Kurt Andrei V.No ratings yet
- 1.antifungal Drug Derma Presentation .DoneDocument29 pages1.antifungal Drug Derma Presentation .Donesahghanshyam9160No ratings yet
- Post Test - CasesDocument5 pagesPost Test - CasesChristian Angelo LeonorNo ratings yet
- Mycology Group BDocument17 pagesMycology Group BAnge OuedraogoNo ratings yet
- Antimicoticos y AntiviralesDocument5 pagesAntimicoticos y AntiviralesGeraldine Andrade RamirezNo ratings yet
- Aminoglycosides ResearchDocument12 pagesAminoglycosides Researchتارا للطباعة والترجمةNo ratings yet
- 6 QuinolonesDocument15 pages6 Quinolonesnusaiba.alobaidyNo ratings yet
- AntifungalsDocument58 pagesAntifungalsMuhammad Shahid BilalNo ratings yet
- Mucormycosis ManagementDocument3 pagesMucormycosis Managementparteek bajwaNo ratings yet
- Anasthesia & AsthmaDocument30 pagesAnasthesia & AsthmafadhiliNo ratings yet
- 3Document2 pages3Nashat SaadiNo ratings yet
- Ilovepdf MergedDocument351 pagesIlovepdf MergedSwara SawantNo ratings yet
- General Concepts and Principles of Disease and Therapeutics: Environmental Diseases Dr. Horacio Saguil JRDocument38 pagesGeneral Concepts and Principles of Disease and Therapeutics: Environmental Diseases Dr. Horacio Saguil JRSwara SawantNo ratings yet
- Nutritional DiseasesDocument30 pagesNutritional DiseasesSwara SawantNo ratings yet
- Article No 1: Abnormal Psychology and Maladaptive Behaviour Exists Everywhere, Does It Influence Society?Document20 pagesArticle No 1: Abnormal Psychology and Maladaptive Behaviour Exists Everywhere, Does It Influence Society?Swara SawantNo ratings yet
- Kaposi SarcomaDocument11 pagesKaposi Sarcomaedgar mandengNo ratings yet
- Microbiology Test For Examanswer by Assel MaamDocument157 pagesMicrobiology Test For Examanswer by Assel MaamAMAN SINGHNo ratings yet
- The Complement SystemDocument33 pagesThe Complement SystemFarlogyNo ratings yet
- Understanding The Immune SystemDocument8 pagesUnderstanding The Immune Systemmohamed waleedNo ratings yet
- Diphtheria The Strangling AngelDocument4 pagesDiphtheria The Strangling AngelDatu Nur-Jhun Salik, MDNo ratings yet
- Artikel Ilmiah KikiDocument8 pagesArtikel Ilmiah KikiAdinah ZahraNo ratings yet
- UNICEF - 2010 - HandBook For Cold Chain ManagersDocument112 pagesUNICEF - 2010 - HandBook For Cold Chain ManagersasmintehminaNo ratings yet
- Employee Health and Personal Hygiene HandbookDocument45 pagesEmployee Health and Personal Hygiene HandbookAsma OmarNo ratings yet
- Immunodeficiency DiseasesDocument59 pagesImmunodeficiency DiseasesJkgamerzNo ratings yet
- ENTEROBACTERIACEAEDocument40 pagesENTEROBACTERIACEAECharmaine Corpuz GranilNo ratings yet
- MDWF 2060 Skaidre Brown 2Document3 pagesMDWF 2060 Skaidre Brown 2api-354751775No ratings yet
- Hematology Review Notes Dela Cruz TopicDocument22 pagesHematology Review Notes Dela Cruz TopicShienna Rose Ann ManaloNo ratings yet
- CDC China 2008 PDFDocument5 pagesCDC China 2008 PDFEbolite HemorrhagicianNo ratings yet
- Drug Study - DoxycylineDocument3 pagesDrug Study - DoxycylineHaifi Hun100% (1)
- We Should Avoid Oily Food . Be Healthy. A. Finally C. Consequently B. in Order To D. So ThatDocument1 pageWe Should Avoid Oily Food . Be Healthy. A. Finally C. Consequently B. in Order To D. So ThathendriNo ratings yet
- Hem QuizDocument38 pagesHem QuizRaneem AljuhaniNo ratings yet
- Drugs Acting On The Immune SystemDocument16 pagesDrugs Acting On The Immune SystemRellie Castro0% (2)
- Dapus OrtopedDocument2 pagesDapus OrtopedqathrunnadaNo ratings yet
- Biological Hazards: Health Hazards Associated With Exposure To Biological AgentsDocument42 pagesBiological Hazards: Health Hazards Associated With Exposure To Biological AgentsKate PagalingNo ratings yet
- Hiv-Aids: Gladys Ziregbe (MRS.)Document25 pagesHiv-Aids: Gladys Ziregbe (MRS.)Esther Anabu EzimaNo ratings yet
- Hypersensitivity and AutoimmunityDocument41 pagesHypersensitivity and AutoimmunityDenish Calmax AngolNo ratings yet
- Excuse LetterDocument1 pageExcuse LetterJennifer Sabanal-Bonite100% (1)
- LPL - PSC Sant Nagar (Burari) Maharaja Agrasen Complex, Main Burari Ro Ad, Sant Nagar, Burari Delhi Sharma - Har1 DelhiDocument4 pagesLPL - PSC Sant Nagar (Burari) Maharaja Agrasen Complex, Main Burari Ro Ad, Sant Nagar, Burari Delhi Sharma - Har1 DelhiarpanNo ratings yet
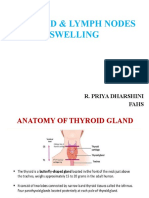
- Thyroid & Lymph NodesDocument44 pagesThyroid & Lymph NodesSarah CornerNo ratings yet
- Nilai Rujukan LaboratoriumDocument4 pagesNilai Rujukan LaboratoriumSila DarmanaNo ratings yet
- Report of Mr. Shivshankar HondeDocument1 pageReport of Mr. Shivshankar HondeShivshankar HondeNo ratings yet
- Modifiable Factors Non Modifiable Factors: Pathophysiology (Theoretical Based) 23Document4 pagesModifiable Factors Non Modifiable Factors: Pathophysiology (Theoretical Based) 23Ara_Ongaco_8894No ratings yet
- BMDM - Bone Marrow-Derived Macrophage ProductionDocument6 pagesBMDM - Bone Marrow-Derived Macrophage ProductionTran Trang AnhNo ratings yet
- Book 1Document6 pagesBook 1Kieth Garcia DariaNo ratings yet
- SarcoidosisDocument7 pagesSarcoidosisJohn SmithNo ratings yet