Download as pdf or txt
You might also like
- Pesci 12Document5 pagesPesci 12Rumana Ali100% (3)
- History of Miasmic Theory 2007Document6 pagesHistory of Miasmic Theory 2007Elaf AbuzarourNo ratings yet
- Essentials of Fire Fighting-Firefighter PPE PDFDocument81 pagesEssentials of Fire Fighting-Firefighter PPE PDFAbdullah Anar100% (3)
- Dallas Pain QuestionnaireDocument1 pageDallas Pain QuestionnaireAndreea-Alexandra LupuNo ratings yet
- Capítulo Historia de MH. Neuman-Thom. 2011Document21 pagesCapítulo Historia de MH. Neuman-Thom. 2011Carolina CortezNo ratings yet
- John Snow: Inhalation of EtherDocument4 pagesJohn Snow: Inhalation of Etherdr jameer kamateNo ratings yet
- History Pain ReliefDocument4 pagesHistory Pain ReliefPoupae SupattraNo ratings yet
- The Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDocument7 pagesThe Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDiana NiculaeNo ratings yet
- Aair 2 165Document7 pagesAair 2 165HeheebNo ratings yet
- Miller 7th Ed Chapter I HistoryDocument35 pagesMiller 7th Ed Chapter I Historyjbahalkeh7570No ratings yet
- The LDN Book - Chapter 1: The History and Pharmacology of LDNDocument24 pagesThe LDN Book - Chapter 1: The History and Pharmacology of LDNChelsea Green Publishing100% (1)
- From The Department of Physiology, Harvard School of Public Health, Boston, MassDocument16 pagesFrom The Department of Physiology, Harvard School of Public Health, Boston, MasshyperbarichealthNo ratings yet
- hhEF66 HTM PDFDocument354 pageshhEF66 HTM PDFJuan Diego De La Cruz MiñanoNo ratings yet
- SerendipityDocument35 pagesSerendipityDr.Shilpa JohnNo ratings yet
- Arsenic EatersDocument6 pagesArsenic EatersbuttertopparrotNo ratings yet
- Essay 101Document7 pagesEssay 101Angel NettoNo ratings yet
- TB ParuDocument7 pagesTB Parumira fitriNo ratings yet
- The Introduction of Halothane Into Clinical Practice: The Oxford ExperienceDocument6 pagesThe Introduction of Halothane Into Clinical Practice: The Oxford Experiencearyati yayaNo ratings yet
- Dialysis History English PDFDocument20 pagesDialysis History English PDFgimenNo ratings yet
- History of CancerDocument2 pagesHistory of CancerDherick RosasNo ratings yet
- Mnagement Cyanide Smoke InhalationDocument10 pagesMnagement Cyanide Smoke InhalationMerlin PakayaNo ratings yet
- NIV - Past, Present and FutureDocument9 pagesNIV - Past, Present and FutureDejan ŽujovićNo ratings yet
- Historia de La MH Ii2007Document20 pagesHistoria de La MH Ii2007Carolina CortezNo ratings yet
- Historia de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Document12 pagesHistoria de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Luis CruzNo ratings yet
- Nobel Laureates in Physiology or MedicineDocument27 pagesNobel Laureates in Physiology or MedicineBiotech PressNo ratings yet
- A History of Veterinary Anaesthesia Nov011Document9 pagesA History of Veterinary Anaesthesia Nov011Lorena B-iNo ratings yet
- Chloroform For The KingDocument7 pagesChloroform For The Kingapi-184836296No ratings yet
- Lectures On The Whole of Anatomy An Annotated Translation of Prelectiones Anatomiae Universalis William HarveyDocument69 pagesLectures On The Whole of Anatomy An Annotated Translation of Prelectiones Anatomiae Universalis William Harveyjanet.yanes764100% (9)
- Oxford Club Penicilina em InglêsDocument13 pagesOxford Club Penicilina em InglêsDongala Pedro MiguelNo ratings yet
- After Comming HeadDocument1 pageAfter Comming HeadEva TriwidyastutiNo ratings yet
- Hemker-2016-Journal of Thrombosis and HaemostasisDocument10 pagesHemker-2016-Journal of Thrombosis and Haemostasis786smhNo ratings yet
- The Story of OzoneDocument58 pagesThe Story of OzoneTee R Taylor100% (1)
- Test 05 RTIDocument13 pagesTest 05 RTIkhaivinhdoNo ratings yet
- History of PenicillinDocument11 pagesHistory of PenicillinAilsa StephensonNo ratings yet
- Carcinosin A Clinical and Pathogenetic StudyDocument11 pagesCarcinosin A Clinical and Pathogenetic StudySohail LatifNo ratings yet
- Epidemic Cholera RecordDocument7 pagesEpidemic Cholera RecordmaniNo ratings yet
- The History of COPDDocument12 pagesThe History of COPDcarloscano1994No ratings yet
- Medicine Key Words NewDocument5 pagesMedicine Key Words Newmu574f4.al1No ratings yet
- Compression Asphyxia and Other Clinicopathological Findings From The Hillsborough Stadium DisasterDocument5 pagesCompression Asphyxia and Other Clinicopathological Findings From The Hillsborough Stadium Disasterdr. Ayu Nabila Kusuma PradanaNo ratings yet
- Congenital Hypertrophic Pyloric Stenosis With Report of Nine CasDocument40 pagesCongenital Hypertrophic Pyloric Stenosis With Report of Nine CasVașadi Razvan CristianNo ratings yet
- Loeffler SyndromeDocument19 pagesLoeffler SyndromeYama Sirly PutriNo ratings yet
- Introduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Document3 pagesIntroduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Pablo PradoNo ratings yet
- Dr.H.O.GUNEWARDENE (Folder)Document38 pagesDr.H.O.GUNEWARDENE (Folder)Ian GardnerNo ratings yet
- Canmedaj00472 0105Document3 pagesCanmedaj00472 0105Andre Eka Putra PrakosaNo ratings yet
- Penicillin ReportDocument9 pagesPenicillin ReportJean CabigaoNo ratings yet
- The Accidental Scientist: The Role of Chance and Luck in Scientific DiscoveryFrom EverandThe Accidental Scientist: The Role of Chance and Luck in Scientific DiscoveryNo ratings yet
- Physick to Physiology: Tales from an Oxford Life in MedicineFrom EverandPhysick to Physiology: Tales from an Oxford Life in MedicineNo ratings yet
- Brjindmed00212 0070Document2 pagesBrjindmed00212 0070Prakash PrabhakarNo ratings yet
- 02anesthesiahistory 160705083420Document48 pages02anesthesiahistory 160705083420mhita100% (1)
- Cancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Document10 pagesCancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Pilar AufrastoNo ratings yet
- William Farr DetailedDocument11 pagesWilliam Farr Detailedmuneebqayyum49No ratings yet
- The History of CPRDocument19 pagesThe History of CPRJuan Carlos AlfaroNo ratings yet
- 1099-0496 (200007) 30 1 1 Aid-Ppul1 3.0.co 2-qDocument2 pages1099-0496 (200007) 30 1 1 Aid-Ppul1 3.0.co 2-qLibre Joel IanNo ratings yet
- Brmedj03204 0051bDocument2 pagesBrmedj03204 0051bkunkkonkNo ratings yet
- Milmed 148 2 118 5Document4 pagesMilmed 148 2 118 5skripsi kapNo ratings yet
- United States Court of Appeals, Fourth CircuitDocument8 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- A Chloroform-Related Death - Analytical and Forensic AspectsDocument8 pagesA Chloroform-Related Death - Analytical and Forensic AspectsAlexandre Learth SoaresNo ratings yet
- Pulmonary Oxygen Toxicity: Investigation and Mentoring: Please ShareDocument5 pagesPulmonary Oxygen Toxicity: Investigation and Mentoring: Please ShareSudhir SainiNo ratings yet
- Astk 2024Document15 pagesAstk 2024abdallah.imjjadNo ratings yet
- Complete Eloptic Directory (OCR) PDFDocument308 pagesComplete Eloptic Directory (OCR) PDFAnonymous SCZ4uYNo ratings yet
- A History of Veterinary Anaesthesia: Historia de La Anestesia VeterinariaDocument9 pagesA History of Veterinary Anaesthesia: Historia de La Anestesia VeterinariaAxel DiazNo ratings yet
- Science 100: Science, Technology and Society: Lesson 2: Nature of TechnologyDocument9 pagesScience 100: Science, Technology and Society: Lesson 2: Nature of Technology이시연No ratings yet
- Indole-3-Acetic Acid Biosynthesis Pathways in The Plant-Beneficial Bacterium Arthrobacter Pascens ZZ21Document15 pagesIndole-3-Acetic Acid Biosynthesis Pathways in The Plant-Beneficial Bacterium Arthrobacter Pascens ZZ21AlinNo ratings yet
- Asisten Pendamping Acara IvDocument2 pagesAsisten Pendamping Acara IvAlinNo ratings yet
- Ovovivipary Refers To The Development of An Embryo Inside An Egg Within The Mother's BodyDocument3 pagesOvovivipary Refers To The Development of An Embryo Inside An Egg Within The Mother's BodyAlinNo ratings yet
- Klasifikasi Acara 7 Classis Aves Dan Mammalia: Rattus Sp. Capra SPDocument1 pageKlasifikasi Acara 7 Classis Aves Dan Mammalia: Rattus Sp. Capra SPAlinNo ratings yet
- The Effect of Seed Scarification On The GerminatioDocument5 pagesThe Effect of Seed Scarification On The GerminatioAlinNo ratings yet
- Inbreeding: Inbreedingin A Single Marriage (Inbreeding Pada Perkawinan Tunggal)Document7 pagesInbreeding: Inbreedingin A Single Marriage (Inbreeding Pada Perkawinan Tunggal)AlinNo ratings yet
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Research in Biotechnology1Document16 pagesResearch in Biotechnology1Gaurav JoshiNo ratings yet
- Vulvitis: Inflammation of The External Female Genitalia, Called The VulvaDocument11 pagesVulvitis: Inflammation of The External Female Genitalia, Called The VulvaNazurah AzmiraNo ratings yet
- Bridging AnticoagulantDocument29 pagesBridging AnticoagulantTessa OktaramdaniNo ratings yet
- Research Topics of Current ResearchDocument31 pagesResearch Topics of Current Researchmisgana etichaNo ratings yet
- Fitness Plan: Name: Date: School: Classroom TeacherDocument3 pagesFitness Plan: Name: Date: School: Classroom TeacherKaian AmorimNo ratings yet
- Chapter 35: Eye Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument5 pagesChapter 35: Eye Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Jurnal AccDocument4 pagesJurnal AccAdi W. YengNo ratings yet
- Tooth Eruption and Its Disorders Pediatric DentistryDocument157 pagesTooth Eruption and Its Disorders Pediatric DentistryIlich GarayNo ratings yet
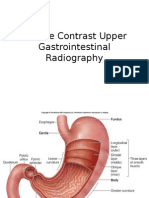
- Jurnal Double Kontras FIXDocument33 pagesJurnal Double Kontras FIXWisnuHeriPurwantoNo ratings yet
- Development of A Questionnaire To Evaluate Knowledge and Attitude of Obesity and WeightDocument10 pagesDevelopment of A Questionnaire To Evaluate Knowledge and Attitude of Obesity and WeightAHMAD NAJMIE SHAIFULLAH BIN ROSALIN MoeNo ratings yet
- DM Health Teaching PlanDocument5 pagesDM Health Teaching PlancamilatanNo ratings yet
- HallDocument804 pagesHallMichael100% (1)
- GDM TeachingDocument4 pagesGDM Teachingapi-272402391No ratings yet
- Tongue Thrusting PedoDocument32 pagesTongue Thrusting PedoFourthMolar.comNo ratings yet
- Excessive Genu Valgum FINALDocument13 pagesExcessive Genu Valgum FINALMeeraNo ratings yet
- Chest Xray Detect Lung CancerDocument9 pagesChest Xray Detect Lung CancerDesyaNo ratings yet
- Injectable and Topical Neurotoxins in Dermatology Jaad 2017Document16 pagesInjectable and Topical Neurotoxins in Dermatology Jaad 2017yolaNo ratings yet
- DDEX3-13 Writhing in The Dark (5-10)Document21 pagesDDEX3-13 Writhing in The Dark (5-10)Michael TaylorNo ratings yet
- GPAT Microbiology SyllabusDocument2 pagesGPAT Microbiology Syllabuskumar HarshNo ratings yet
- Antimicrobial Sensitivity TestingDocument21 pagesAntimicrobial Sensitivity TestingLaiba FarooqNo ratings yet
- Congestive Heart Failure: National University College of PharmacyDocument7 pagesCongestive Heart Failure: National University College of PharmacyLEO MARIENo ratings yet
- A. Classification: Taenia Solium and Taenia SaginataDocument8 pagesA. Classification: Taenia Solium and Taenia SaginataadhiNo ratings yet
- RicaDocument9 pagesRicarica mae narbaizNo ratings yet
- Management of Severe Asymptomatic Hypertension (Hypertensive Urgencies) in Adults - UpToDateDocument16 pagesManagement of Severe Asymptomatic Hypertension (Hypertensive Urgencies) in Adults - UpToDateMarcela Garzon O VelezNo ratings yet
- CDC - Stool Specimen CollectionDocument3 pagesCDC - Stool Specimen CollectionC. HidalgoNo ratings yet
- Health, Stress, and CopingDocument49 pagesHealth, Stress, and CopingMarissa BrionesNo ratings yet