Download as pdf or txt
You might also like
- AANA Advanced Arthroscopy The KneeDocument291 pagesAANA Advanced Arthroscopy The KneeNguyễn Hồ Huy HoàngNo ratings yet
- Deltoides AnteriorDocument4 pagesDeltoides AnteriorJose Antonio Pareja-EstebanNo ratings yet
- Early Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairDocument9 pagesEarly Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairJane Elisabeth WauranNo ratings yet
- WestsideDocument7 pagesWestsideBrandon C WilliamsNo ratings yet
- Comparative Study On Active Release Technique Versus Myofascial Release Technique For Upper Trapezius Muscle Spasm - 1663653511Document4 pagesComparative Study On Active Release Technique Versus Myofascial Release Technique For Upper Trapezius Muscle Spasm - 1663653511Mohitha ParlaNo ratings yet
- Lit PaperDocument7 pagesLit Paperapi-679438371No ratings yet
- Miller 2016Document9 pagesMiller 2016Dario GerpeNo ratings yet
- Gregory F. Marchetti, Jennica Bellanca, Susan L. Whitney, James Chia-Cheng Lin, Mark C. Musolino, Gabriel R. Furman and Mark S. RedfernDocument9 pagesGregory F. Marchetti, Jennica Bellanca, Susan L. Whitney, James Chia-Cheng Lin, Mark C. Musolino, Gabriel R. Furman and Mark S. RedfernferbednarskiNo ratings yet
- Rodrigo Py Gonçalves Barreto Bilateral MagneticDocument8 pagesRodrigo Py Gonçalves Barreto Bilateral MagneticfilipecorsairNo ratings yet
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezNo ratings yet
- Arthroscopic Surgery or Physical Therapy For Patients With Femoroacetabular Impingement SyndromeDocument9 pagesArthroscopic Surgery or Physical Therapy For Patients With Femoroacetabular Impingement SyndromeEricNo ratings yet
- Aquatic Exercise Therapy For People With Parkinson Disease: A Randomized Controlled TrialDocument8 pagesAquatic Exercise Therapy For People With Parkinson Disease: A Randomized Controlled Trialalika nailaNo ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument12 pagesThis Item Is The Archived Peer-Reviewed Author-Version ofK scuddsNo ratings yet
- Tveter 2014Document8 pagesTveter 2014Thays VotaçõesNo ratings yet
- Yjmt 30 1992090Document13 pagesYjmt 30 1992090Luis Sebastian Arango OspinaNo ratings yet
- 2004 Mcclure PTDocument17 pages2004 Mcclure PTBruno FellipeNo ratings yet
- Aquatic Circuit Training Including Aqua-Cycling in Patients With Knee Osteoarthritis: A Feasibility StudyDocument6 pagesAquatic Circuit Training Including Aqua-Cycling in Patients With Knee Osteoarthritis: A Feasibility StudygalihNo ratings yet
- Lasbleiz 2014 - Diagnostic Value Rotator Cuff 1-S2.0-S1877065714016509-MainDocument16 pagesLasbleiz 2014 - Diagnostic Value Rotator Cuff 1-S2.0-S1877065714016509-MainIkhsan JohnsonNo ratings yet
- Klapp MethodDocument7 pagesKlapp MethodRJLeddaNo ratings yet
- Hydrotherapy Improves Pain and Function in Older Women With Knee Osteoarthritis - A Randomized Controlled TrialDocument8 pagesHydrotherapy Improves Pain and Function in Older Women With Knee Osteoarthritis - A Randomized Controlled TrialFrescura BanNo ratings yet
- 1 s2.0 S1836955320300278 MainDocument8 pages1 s2.0 S1836955320300278 MainVebby BiLspenzhamNo ratings yet
- Return-to-Sport Testing After Medial Patellofemoral Ligament Reconstruction in Adolescent AthletesDocument7 pagesReturn-to-Sport Testing After Medial Patellofemoral Ligament Reconstruction in Adolescent AthletesiwanNo ratings yet
- Short-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical TrialDocument9 pagesShort-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical Trialvidisanjaya21No ratings yet
- HVT With Lumbar Disc HerniationDocument12 pagesHVT With Lumbar Disc HerniationSheena McLennanNo ratings yet
- 2017 Article 1388Document10 pages2017 Article 1388MonikaNo ratings yet
- Kuhn2013 PDFDocument9 pagesKuhn2013 PDFNati GallardoNo ratings yet
- Goniometric Reliability of Shoulder MeasurementsDocument6 pagesGoniometric Reliability of Shoulder MeasurementssaswepakNo ratings yet
- 10 1016@j Jse 2019 10 013Document12 pages10 1016@j Jse 2019 10 013Gustavo BECERRA PERDOMONo ratings yet
- USWR v5n1p11 enDocument8 pagesUSWR v5n1p11 enSoare Elena-CosminaNo ratings yet
- 2023 Brock Et Al. - Improving Directional Control of The Upper Limb in Severe Stroke - Efficacy of The Bobath Concept - A Pilot Randomised TrialDocument9 pages2023 Brock Et Al. - Improving Directional Control of The Upper Limb in Severe Stroke - Efficacy of The Bobath Concept - A Pilot Randomised TrialMarko MarkićNo ratings yet
- The Effects of Bobath-Based Trunk Exercises On Trunk Control, Functional Capacity, Balance, and Gait: A Pilot Randomized Controlled TrialDocument9 pagesThe Effects of Bobath-Based Trunk Exercises On Trunk Control, Functional Capacity, Balance, and Gait: A Pilot Randomized Controlled Trialnandhini raguNo ratings yet
- Clinical Effects of Proprioceptive Thumb ExerciseDocument9 pagesClinical Effects of Proprioceptive Thumb Exercisejc596ncf2hNo ratings yet
- Diafragma Ant Posterior ChainDocument7 pagesDiafragma Ant Posterior ChainJulijus MotiejunasNo ratings yet
- The Effectiveness of Manual Physical Therapy and Exercise For Mechanical Neck Pain - A Randomized Clinical TrialDocument8 pagesThe Effectiveness of Manual Physical Therapy and Exercise For Mechanical Neck Pain - A Randomized Clinical TrialHarshoi KrishannaNo ratings yet
- Comparison Between Manual Traction, Manual Opening Technique and Combination in Patients With Cervical Radiculopathy: Randomized Control TrialDocument6 pagesComparison Between Manual Traction, Manual Opening Technique and Combination in Patients With Cervical Radiculopathy: Randomized Control TrialEka BagaskaraNo ratings yet
- To Compare The Effects of Maitland MobilizationDocument4 pagesTo Compare The Effects of Maitland MobilizationravichandragoudaNo ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument20 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeNo ratings yet
- Hamstring Shortness Among Undergraduate StudentsDocument6 pagesHamstring Shortness Among Undergraduate StudentsMr DanielNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- Physical Therapy in Sport: Literature ReviewDocument9 pagesPhysical Therapy in Sport: Literature ReviewPrincess Dianna SulitNo ratings yet
- Effectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisDocument10 pagesEffectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisraquelbibiNo ratings yet
- Joc60156 2451 2459Document9 pagesJoc60156 2451 2459cooperorthopaedicsNo ratings yet
- Analyzing Spinal Curves For Prolong Sitting in University Going StudentsDocument8 pagesAnalyzing Spinal Curves For Prolong Sitting in University Going StudentsMr DanielNo ratings yet
- JurnalDocument10 pagesJurnalAlifia RizqiNo ratings yet
- Does The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCDocument26 pagesDoes The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCEri KafexhiNo ratings yet
- Kristenen, NeckmusclebalanceDocument9 pagesKristenen, NeckmusclebalancePhooi Yee LauNo ratings yet
- 9 FullDocument15 pages9 FulllipemagalhaesNo ratings yet
- Orthopaedic JournalDocument6 pagesOrthopaedic JournalZiad AlazthaNo ratings yet
- Longitudinal Analysis of The Recovery of Trunk Control and Upper Extremity Following Stroke: An Individual Growth Curve ApproachDocument17 pagesLongitudinal Analysis of The Recovery of Trunk Control and Upper Extremity Following Stroke: An Individual Growth Curve ApproachWoffe SoloNo ratings yet
- Journal PPT - Imt 3Document39 pagesJournal PPT - Imt 3Iqbal KhanNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- How Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?Document6 pagesHow Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?JoNo ratings yet
- Adding Mobilisation With Movement To Exercise ... Reid Vicenzino 2022Document8 pagesAdding Mobilisation With Movement To Exercise ... Reid Vicenzino 2022patinoomar67No ratings yet
- Effects of Motor Imagery On Strength, Range of MotionDocument11 pagesEffects of Motor Imagery On Strength, Range of Motionseroxat2005No ratings yet
- Satpute 2018Document9 pagesSatpute 2018Mahmoud Abo AlfaNo ratings yet
- Free Paper Presentations0000Document94 pagesFree Paper Presentations0000Syed Imroz KhanNo ratings yet
- تنزيلDocument7 pagesتنزيلDr Abdallah BahaaNo ratings yet
- Pi Is 000399931300453 XDocument7 pagesPi Is 000399931300453 XFarhaanKhanHaleemNo ratings yet
- Impact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsDocument4 pagesImpact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsCristian Florin CrasmaruNo ratings yet
- PT Hip-OA 2014Document11 pagesPT Hip-OA 2014GeorgeKielingNo ratings yet
- Spinal Tumor Surgery: A Case-Based ApproachFrom EverandSpinal Tumor Surgery: A Case-Based ApproachDaniel M. SciubbaNo ratings yet
- Campbells Operative Orthopaedics 4 Volume Set 14Th Edition Frederick M Azar Full Chapter PDFDocument69 pagesCampbells Operative Orthopaedics 4 Volume Set 14Th Edition Frederick M Azar Full Chapter PDFyiotisbatist90100% (9)
- Cirurgia Da Articulação Temporomandibular para Distúrbio InternoDocument14 pagesCirurgia Da Articulação Temporomandibular para Distúrbio InternoMatheus MoraisNo ratings yet
- Congenital Muscular Torticollis - A Proposal For Treatment and PhysiotherapyDocument10 pagesCongenital Muscular Torticollis - A Proposal For Treatment and PhysiotherapyevinovianiNo ratings yet
- K Taping in Pediatrics Basics Techniques Indications 2016 EditionDocument154 pagesK Taping in Pediatrics Basics Techniques Indications 2016 EditionMariale Segura Ramirez100% (1)
- Congenital Lower Limb DeformitiesDocument47 pagesCongenital Lower Limb DeformitiesAmerico BarbosaNo ratings yet
- MovSciLec MSC 2101 Week16Document11 pagesMovSciLec MSC 2101 Week16Mary SotoNo ratings yet
- DR - Fatima Ejaz PT Ms Neurophysical Therapy: Organization and Administration of Emergency CareDocument19 pagesDR - Fatima Ejaz PT Ms Neurophysical Therapy: Organization and Administration of Emergency Carekim suhoNo ratings yet
- PTH 5217: Pediatric Physiotherapy Case Presentation Topic: Brachial Plexus Injury-Erb'S PalsyDocument57 pagesPTH 5217: Pediatric Physiotherapy Case Presentation Topic: Brachial Plexus Injury-Erb'S PalsySylvia LoongNo ratings yet
- Piriformis Tightness ResearchDocument53 pagesPiriformis Tightness Researchzubair khalidNo ratings yet
- Establishing Core Stability in RehabilitationDocument25 pagesEstablishing Core Stability in RehabilitationPaulo ZulluNo ratings yet
- The Roots Value of Each Branch Is Given in BracketsDocument8 pagesThe Roots Value of Each Branch Is Given in BracketsAneela PervezNo ratings yet
- Sports MassageDocument8 pagesSports MassageFairus ZainudinNo ratings yet
- 2019HattoriUSGLLS10.1007 - s12178 019 09592 0Document15 pages2019HattoriUSGLLS10.1007 - s12178 019 09592 0krizkyNo ratings yet
- Psychiatric RehabilitationDocument36 pagesPsychiatric RehabilitationbolutifeNo ratings yet
- Sparrc Institute CoimbatoreDocument1 pageSparrc Institute CoimbatoreKalyana SundaramNo ratings yet
- 1665578086932-Q Bank A Physio Officer 5Document23 pages1665578086932-Q Bank A Physio Officer 5mosaNo ratings yet
- TMD Part 4 Appliance TherapyDocument7 pagesTMD Part 4 Appliance Therapyimane boujoualNo ratings yet
- Anatomical Terms of MovementDocument12 pagesAnatomical Terms of MovementRIANE JADE CADALIG PENATNo ratings yet
- Role of PhysiotherapyDocument22 pagesRole of PhysiotherapyKate PurcellNo ratings yet
- PG Syllabus Surgery & RadiologyDocument28 pagesPG Syllabus Surgery & RadiologyMAYANK MEENANo ratings yet
- Femoral Triangle - Borders, Contents and Mnemonics - KenhubDocument7 pagesFemoral Triangle - Borders, Contents and Mnemonics - Kenhubو عجلت اليك ربي لترضيNo ratings yet
- Therapeutic Exercise From Theory To Practice (Michael Higgins)Document843 pagesTherapeutic Exercise From Theory To Practice (Michael Higgins)Pooja Jugdar Deshmukh100% (3)
- EMS14 EMS Products Only Catalogue 2022 V17 FINAL ScreenDocument20 pagesEMS14 EMS Products Only Catalogue 2022 V17 FINAL ScreenAbdallah MohamedNo ratings yet
- Barefoot Massage TherapyuzukwDocument2 pagesBarefoot Massage Therapyuzukwwindgreen80No ratings yet
- Gait Resource Humb5000 - Rebecca HoDocument3 pagesGait Resource Humb5000 - Rebecca Hoapi-722611753No ratings yet
- Advanced Physiotherapeutic SyllabusDocument1 pageAdvanced Physiotherapeutic SyllabusAnup SharmaNo ratings yet
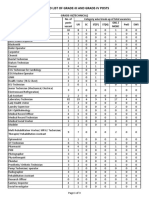
- Revised List of Grade-III Grade-IV Posts 0Document3 pagesRevised List of Grade-III Grade-IV Posts 0CLASHING ELECTRONo ratings yet
- Managing Low Back Pain: Exercise, Manual Therapy, and EducationDocument1 pageManaging Low Back Pain: Exercise, Manual Therapy, and Educationgraciela rosario guija rodriguezNo ratings yet
- Knee Mechanics and Pathomechanics (1st Year)Document109 pagesKnee Mechanics and Pathomechanics (1st Year)MUGISHA GratienNo ratings yet