Download as docx, pdf, or txt
You might also like
- Oh No, It's A Big Fat Bitch SpayDocument8 pagesOh No, It's A Big Fat Bitch SpayWilliam Chandler100% (1)
- Achilles Repair ProtocolDocument19 pagesAchilles Repair ProtocolRobertNo ratings yet
- 1860 N95 Particulate Respirator Spec Sheet - FINAL - V4 PDFDocument2 pages1860 N95 Particulate Respirator Spec Sheet - FINAL - V4 PDFgeeko geekNo ratings yet
- Jejunogastric Intussusception: Prior To Procedure Procedure Post-Procedure DischargeDocument7 pagesJejunogastric Intussusception: Prior To Procedure Procedure Post-Procedure DischargeMariano MarbellaNo ratings yet
- Sex ChangeDocument41 pagesSex Changeiura echin67% (3)
- Sex ModifyDocument41 pagesSex Modifyshyam rana100% (1)
- TotalAbdomHysterBilateralSalpingoOophorectPelvicNodeDissection EndometrialCancer TH PD9300Document36 pagesTotalAbdomHysterBilateralSalpingoOophorectPelvicNodeDissection EndometrialCancer TH PD9300Red StohlNo ratings yet
- RicaDocument9 pagesRicarica mae narbaizNo ratings yet
- Permanent ContraceptionDocument33 pagesPermanent Contraceptionshyama seerviNo ratings yet
- Abstracts BookDocument186 pagesAbstracts BookGabriel Laurentiu CucuNo ratings yet
- Midwifery - SterlizationDocument39 pagesMidwifery - SterlizationEsha KuttiNo ratings yet
- Permanent Methods of Contraception (Surgical Sterilization) : VasectomyDocument7 pagesPermanent Methods of Contraception (Surgical Sterilization) : VasectomyEmAr ExNo ratings yet
- Advanced Laparoscopic Hysterectomy SurgeryDocument2 pagesAdvanced Laparoscopic Hysterectomy SurgeryManu GynecologyNo ratings yet
- Rangkuman TeratomaDocument22 pagesRangkuman TeratomaFelicia Fernanda IskandarNo ratings yet
- Agenesis VaginaDocument6 pagesAgenesis Vaginai305No ratings yet
- Benefits and Risks of SterilizationDocument29 pagesBenefits and Risks of Sterilizationvado_727No ratings yet
- Running Head: Uterine TransplantationDocument9 pagesRunning Head: Uterine TransplantationEsther MNo ratings yet
- Surgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyDocument3 pagesSurgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyMary Ann LunnayNo ratings yet
- STERILIZATION2Document2 pagesSTERILIZATION2Fatima Diane S. MondejarNo ratings yet
- Permanent Family PlanningDocument36 pagesPermanent Family PlanningNilakshi Barik MandalNo ratings yet
- Vaginal Agenesis PDFDocument4 pagesVaginal Agenesis PDFBill HarmanNo ratings yet
- What Is Microsurgical Tubal Ligation Reversal?Document2 pagesWhat Is Microsurgical Tubal Ligation Reversal?Andy WijayaNo ratings yet
- O 18hnif9237qkmoa1frbent5nh8Document3 pagesO 18hnif9237qkmoa1frbent5nh8bandizrichardNo ratings yet
- Participate IN Various Programmes VasectomyDocument6 pagesParticipate IN Various Programmes Vasectomyvenkat krishnanNo ratings yet
- CystorrhaphyDocument7 pagesCystorrhaphyKit LaraNo ratings yet
- Transgender TransplantDocument1 pageTransgender Transplantmudabber.musawerNo ratings yet
- Masculinizing and Defeminizing Gend - 2023 - Best Practice - Research Clinical ODocument10 pagesMasculinizing and Defeminizing Gend - 2023 - Best Practice - Research Clinical OannisanadyapNo ratings yet
- Vaginal Cuff 2Document5 pagesVaginal Cuff 2Aulia Rizqi MulyaniNo ratings yet
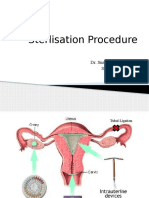
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalDocument30 pagesSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaNo ratings yet
- DR - Mohammed Abdalla Egypt. Domiat G. Hospital: Controversies in GynecologyDocument66 pagesDR - Mohammed Abdalla Egypt. Domiat G. Hospital: Controversies in Gynecologymadmax500No ratings yet
- GDNRSS Phalloplasty March 22Document16 pagesGDNRSS Phalloplasty March 22Breno Mendes CardosoNo ratings yet
- Overview of Current Trends in Hysterectomy: ReviewDocument13 pagesOverview of Current Trends in Hysterectomy: ReviewFranklin Salirrosas CernaNo ratings yet
- Total Laparoscopic Hysterectomy (TLH) : Patient Information Patient InformationDocument7 pagesTotal Laparoscopic Hysterectomy (TLH) : Patient Information Patient InformationMUKUL SAXENANo ratings yet
- 0814 OBG Kho v9Document5 pages0814 OBG Kho v9subrata dasNo ratings yet
- SCP BSUG July 2017Document15 pagesSCP BSUG July 2017Yasir K. HaniNo ratings yet
- HysterectomyDocument6 pagesHysterectomyIcicNo ratings yet
- SeminarDocument41 pagesSeminarJilliane OriaNo ratings yet
- Ocua Urologytoday VolumeiDocument8 pagesOcua Urologytoday Volumeiapi-249405525No ratings yet
- Hysterectomy Dancel 2BSN3Document4 pagesHysterectomy Dancel 2BSN3Nichole DancelNo ratings yet
- Gender Transition: Surgery: A Guide For MtfsDocument32 pagesGender Transition: Surgery: A Guide For MtfsfrancesNo ratings yet
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- HysterectomyDocument5 pagesHysterectomyТанзиля Миндубаева МЛ-209No ratings yet
- Hysterectomy: Frequently Asked Questions FAQ008 Special ProceduresDocument4 pagesHysterectomy: Frequently Asked Questions FAQ008 Special ProceduresGrace Noviyanthi SinambelaNo ratings yet
- Total Abdominal Hysterectomy Bilateral SaphingoDocument7 pagesTotal Abdominal Hysterectomy Bilateral SaphingoAndrea BroccoliNo ratings yet
- Medical & Surgical ProceduresDocument12 pagesMedical & Surgical ProceduresAmina Sani GedeNo ratings yet
- Total Abdominal Hysterectomy - Bilateral Salpingo-Oophorectomy and OmentectomyDocument36 pagesTotal Abdominal Hysterectomy - Bilateral Salpingo-Oophorectomy and OmentectomyVignesh JayaNo ratings yet
- Aesthetic Surgery of Female External GenitaliaDocument13 pagesAesthetic Surgery of Female External GenitaliaJavier Villalón Quiroz100% (1)
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- Hysterectomy: The American College of Obstetricians and GynecologistsDocument0 pagesHysterectomy: The American College of Obstetricians and Gynecologistsmonir61No ratings yet
- Gynecological Aspectsof Transgender Healthcare 2009Document10 pagesGynecological Aspectsof Transgender Healthcare 2009Iris LopezNo ratings yet
- What Is Bilateral Tubal LigationDocument42 pagesWhat Is Bilateral Tubal LigationAldrich ArquizaNo ratings yet
- Ablasi EndometriumDocument3 pagesAblasi EndometriumHarby SatriaNo ratings yet
- 2016 Ovarian Mature Cystic TeratomDocument7 pages2016 Ovarian Mature Cystic Teratompaula rangelNo ratings yet
- Vaginal HysterectomyDocument5 pagesVaginal Hysterectomysensitivity23No ratings yet
- Transvaginal MorcellationDocument8 pagesTransvaginal Morcellationsanjayb1976gmailcomNo ratings yet
- Before and After Radical Prostate Surgery: Information and Resource GuideFrom EverandBefore and After Radical Prostate Surgery: Information and Resource GuideNo ratings yet
- Birth Control: How To Decide: Tubal Ligation (Tubes Tied)Document7 pagesBirth Control: How To Decide: Tubal Ligation (Tubes Tied)EmAr ExNo ratings yet
- Vaginal Agenesis or HypoplasiaDocument18 pagesVaginal Agenesis or Hypoplasianikd_6No ratings yet
- ProstactomyDocument18 pagesProstactomyBharat BhushanNo ratings yet
- TAH and BSO (TAH-BSO) Is Still Considered The Standard Operative Procedure For Patients With Endometrial CancerDocument3 pagesTAH and BSO (TAH-BSO) Is Still Considered The Standard Operative Procedure For Patients With Endometrial CancerVanessa VillanuevaNo ratings yet
- Trends of Various Techniques of Tubectomy: A Five Year Study in A Tertiary InstituteDocument4 pagesTrends of Various Techniques of Tubectomy: A Five Year Study in A Tertiary InstituteJer KelNo ratings yet
- Literature Review EpisiotomyDocument6 pagesLiterature Review Episiotomyafmztopfhgveie100% (1)
- How To Overcome Mental FatigueDocument3 pagesHow To Overcome Mental FatigueBook Reader100% (1)
- The Neuroscience of Déjà VuDocument2 pagesThe Neuroscience of Déjà VuBook ReaderNo ratings yet
- It's Déjà Vu All Over Again: Posted April 21, 2018, David Ludden PH.DDocument3 pagesIt's Déjà Vu All Over Again: Posted April 21, 2018, David Ludden PH.DBook ReaderNo ratings yet
- Legacy Lessons of Symbolic ImmortalityDocument3 pagesLegacy Lessons of Symbolic ImmortalityBook ReaderNo ratings yet
- The Art of Self-Forgiveness - Rick Hanson, PHDDocument3 pagesThe Art of Self-Forgiveness - Rick Hanson, PHDBook ReaderNo ratings yet
- Transgender Visibility Guide 042013Document32 pagesTransgender Visibility Guide 042013Book ReaderNo ratings yet
- Death AnxietyDocument4 pagesDeath AnxietyBook ReaderNo ratings yet
- Unwanted Mental Intrusions in Anxiety Disorders:: A Modified Cognitive-Behavioral ApproachDocument22 pagesUnwanted Mental Intrusions in Anxiety Disorders:: A Modified Cognitive-Behavioral ApproachBook ReaderNo ratings yet
- Healing Your Shame and Guilt Through SelfDocument7 pagesHealing Your Shame and Guilt Through SelfBook Reader100% (1)
- 7 Famous Transgender People From History You Can Mention Next Time Someone SaysDocument4 pages7 Famous Transgender People From History You Can Mention Next Time Someone SaysBook ReaderNo ratings yet
- Living Authentically: Coming OutDocument27 pagesLiving Authentically: Coming OutBook ReaderNo ratings yet
- Remembering Ben Barres, The Trailblazing Trans Neuroscientist and Mentor, On His BirthdayDocument2 pagesRemembering Ben Barres, The Trailblazing Trans Neuroscientist and Mentor, On His BirthdayBook ReaderNo ratings yet
- Panic Attacks and Panic DisorderDocument5 pagesPanic Attacks and Panic DisorderBook ReaderNo ratings yet
- Building Body Acceptance - 04 - Reducing Checking and Reassurance SeekingDocument15 pagesBuilding Body Acceptance - 04 - Reducing Checking and Reassurance SeekingBook ReaderNo ratings yet
- Building Body Acceptance - 01 - Understanding Body Dysmorphic DisorderDocument12 pagesBuilding Body Acceptance - 01 - Understanding Body Dysmorphic DisorderBook ReaderNo ratings yet
- Building Body Acceptance - 02 - What Keeps BDD GoingDocument14 pagesBuilding Body Acceptance - 02 - What Keeps BDD GoingBook ReaderNo ratings yet
- How Can You Stop A Panic AttackDocument3 pagesHow Can You Stop A Panic AttackBook ReaderNo ratings yet
- Do You Live With AnxietyDocument4 pagesDo You Live With AnxietyBook ReaderNo ratings yet
- 4 Things To Remember The Next Time YouDocument3 pages4 Things To Remember The Next Time YouBook ReaderNo ratings yet
- Labelling: Cognitive Distortions That Fuel AngerDocument2 pagesLabelling: Cognitive Distortions That Fuel AngerBook ReaderNo ratings yet
- 7 Strategies To Help You Live With UncertaintyDocument4 pages7 Strategies To Help You Live With UncertaintyBook ReaderNo ratings yet
- Understanding Anger: The Emotional Response CycleDocument3 pagesUnderstanding Anger: The Emotional Response CycleBook ReaderNo ratings yet
- 7 Effective Thought-Stopping Techniques For Anxiety: How Do I Stop Worrying So Much?Document2 pages7 Effective Thought-Stopping Techniques For Anxiety: How Do I Stop Worrying So Much?Book ReaderNo ratings yet
- Worksheet Consequences of AddictionDocument2 pagesWorksheet Consequences of AddictionBook ReaderNo ratings yet
- MPSG 2-0 InfographicDocument1 pageMPSG 2-0 InfographicNorzaherawati Aryani Md TahirNo ratings yet
- MRI of Spinal Cord P1Document6 pagesMRI of Spinal Cord P1BenjaminNo ratings yet
- TAOMS20 Abstract BookDocument238 pagesTAOMS20 Abstract BookTaha ÖzerNo ratings yet
- Millenium Gold Medal Award 2021Document1 pageMillenium Gold Medal Award 2021Shiwali SinghNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative DentistryAna Maria Montoya GomezNo ratings yet
- Tuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewDocument9 pagesTuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewHendra SalehNo ratings yet
- Adverse Event Report Form 2 PDFDocument4 pagesAdverse Event Report Form 2 PDFtosadeliNo ratings yet
- Dok Gudang Alkes 2023 MasterDocument64 pagesDok Gudang Alkes 2023 MasterRuang Bersalin MentengNo ratings yet
- What Are GallstonesDocument15 pagesWhat Are GallstonesStepyn SalvadorNo ratings yet
- Physiotherapy in Pre and Post Operative Spine SurgeriesDocument45 pagesPhysiotherapy in Pre and Post Operative Spine SurgeriesNaveen KumarNo ratings yet
- Swing Lock Partial Denture SOWMYADocument22 pagesSwing Lock Partial Denture SOWMYASanNo ratings yet
- Mastr Time Table July-2014 CDocument1 pageMastr Time Table July-2014 Capi-87967494No ratings yet
- Aofog Aofog: Executive Board & Council Members President's MessageDocument16 pagesAofog Aofog: Executive Board & Council Members President's MessageHisteroscopia.esNo ratings yet
- History of DentistryDocument24 pagesHistory of DentistryEzhilarasi INo ratings yet
- Region 10Document43 pagesRegion 10martslugz60% (5)
- Evaluation and Management of The Polytraumatized Patient in Various CentersDocument1 pageEvaluation and Management of The Polytraumatized Patient in Various CentersVfor VendettaNo ratings yet
- Productos Cataloguo Tappa PDFDocument10 pagesProductos Cataloguo Tappa PDFjavier jimenezNo ratings yet
- Schwartz's Principles of Surgery ABSITE and Board Review, 9th EdDocument2 pagesSchwartz's Principles of Surgery ABSITE and Board Review, 9th Edvnnv101.raceacNo ratings yet
- Impaired Skin IntegrityDocument2 pagesImpaired Skin Integritykingpin100% (1)
- CEO - CaninesDocument17 pagesCEO - CaninesAlina EsanuNo ratings yet
- Jaha 120 017275Document150 pagesJaha 120 017275Leonardo LiswojoNo ratings yet
- Giordano 2019Document7 pagesGiordano 2019ananda halimNo ratings yet
- Internship LogbookDocument9 pagesInternship Logbooksarhang talebaniNo ratings yet
- Intra-Operative Peritoneal Lavage - Who Does It An PDFDocument5 pagesIntra-Operative Peritoneal Lavage - Who Does It An PDFAd NanNo ratings yet
- New PDF ResumeDocument3 pagesNew PDF Resumesunita gogate0% (2)
- Nailing Vs Plate in Humerus FXDocument4 pagesNailing Vs Plate in Humerus FXBalsam TeineNo ratings yet
- TBlegen Resume Feb 23Document3 pagesTBlegen Resume Feb 23TerrianneNo ratings yet