
A Review of Innovative Teaching Methods: Special Report
A Review of Innovative Teaching Methods: Special Report
You might also like
- ByDesign Subscription Billing CPI Configuration Guide 1902Document21 pagesByDesign Subscription Billing CPI Configuration Guide 1902nagaurjunaNo ratings yet
- Value of Research in The Area of InterestDocument36 pagesValue of Research in The Area of InterestRex Michael50% (8)
- 03 Task Performance 1 HCIDocument2 pages03 Task Performance 1 HCIKurt RaferNo ratings yet
- Modern Image Quality AssessmentDocument157 pagesModern Image Quality AssessmentRazii AbrahamNo ratings yet
- Unreal Engine GameDocument20 pagesUnreal Engine GameartNo ratings yet
- WritingDocument1 pageWritingIvan LazaroNo ratings yet
- Innovative TeachingDocument13 pagesInnovative TeachingShine BasayNo ratings yet
- Learning Preferences and Competencies of Radiologic Technology InternsDocument13 pagesLearning Preferences and Competencies of Radiologic Technology InternsIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet
- Thesis JeraldDocument7 pagesThesis Jeraldaljohn anticristoNo ratings yet
- 6Document7 pages6GSL SMART LABNo ratings yet
- AttentionDocument7 pagesAttentionChandra EkaNo ratings yet
- Enhancing Occupational Therapy Students Knowledge, Competence, Awareness and Interest in AccessibilityDocument8 pagesEnhancing Occupational Therapy Students Knowledge, Competence, Awareness and Interest in Accessibilityying reenNo ratings yet
- 1 s2.0 S1078817422000633 MainDocument7 pages1 s2.0 S1078817422000633 MainYamah PrincewillNo ratings yet
- CurriculumDocument114 pagesCurriculumMuhammad TariqNo ratings yet
- Dissertation InstrumentationDocument5 pagesDissertation InstrumentationCustomPaperWritingServicesUK100% (1)
- E-Learning Experience For Medical EducationDocument4 pagesE-Learning Experience For Medical Educationangelo.dibernardo63No ratings yet
- AECT - Definition of Educational TechnologyDocument16 pagesAECT - Definition of Educational TechnologyGd JohandanaNo ratings yet
- Medu 14194Document2 pagesMedu 14194ZoeNo ratings yet
- 10 1016@j Radi 2018 06 011Document8 pages10 1016@j Radi 2018 06 011Ricky Cahyasari PutraNo ratings yet
- Expanding Training Capacity For Radiographer Reporting UsingDocument6 pagesExpanding Training Capacity For Radiographer Reporting UsingC JoanesNo ratings yet
- Ecology and Evolution - 2020 - McDevitt - Lessons and Recommendations From Three Decades As An NSF REU Site A Call ForDocument29 pagesEcology and Evolution - 2020 - McDevitt - Lessons and Recommendations From Three Decades As An NSF REU Site A Call Foree wwNo ratings yet
- Duarte 2022Document12 pagesDuarte 2022Juan Carlos FloresNo ratings yet
- Clinical Education: MLS Student PerceptionsDocument6 pagesClinical Education: MLS Student PerceptionsUlfat NiazyNo ratings yet
- Tracey Pieterse (2016)Document10 pagesTracey Pieterse (2016)sigit hartantoNo ratings yet
- Specialty: Journal of Applied Behavior Analysis NumberDocument6 pagesSpecialty: Journal of Applied Behavior Analysis NumberalpNo ratings yet
- 070.2017.DesJardin - Near Peer Point of CareUltrasoundDocument9 pages070.2017.DesJardin - Near Peer Point of CareUltrasoundSergio San Juan DertkigilNo ratings yet
- Screening tool-SRDocument13 pagesScreening tool-SRSri purwantiNo ratings yet
- D20 ResearchDocument53 pagesD20 ResearchedmondNo ratings yet
- Multimedia Principal MayerDocument10 pagesMultimedia Principal Mayerandhika pradnyanaNo ratings yet
- 16Document2 pages16Walisson BarbosaNo ratings yet
- Teach USDocument6 pagesTeach USjonargNo ratings yet
- National Ultrasound Curriculum For Medical.4Document7 pagesNational Ultrasound Curriculum For Medical.4josephNo ratings yet
- English FinalsDocument28 pagesEnglish FinalsMark M. Alipio100% (1)
- Thesis RaritanDocument6 pagesThesis Raritandwtt67ef100% (2)
- Developing A Multimedia Courseware Using Cognitive Load TheoryDocument10 pagesDeveloping A Multimedia Courseware Using Cognitive Load TheorySMNo ratings yet
- Intro To RT Module 1Document2 pagesIntro To RT Module 1Jerel Waga UbarcoNo ratings yet
- Mashups For Learning - EditorialDocument3 pagesMashups For Learning - EditorialMartinNo ratings yet
- MeduloblastomaDocument12 pagesMeduloblastomaJonathanNo ratings yet
- New Normal CovidDocument2 pagesNew Normal Covidتغريد عبادةNo ratings yet
- Wong2022 Article CriticalCareUltrasoundDocument3 pagesWong2022 Article CriticalCareUltrasoundA. RaufNo ratings yet
- The Importance of Venipuncture Among The Third Year Radiologic Technology Students of Lyceum-Northwestern UniversityDocument17 pagesThe Importance of Venipuncture Among The Third Year Radiologic Technology Students of Lyceum-Northwestern UniversityCJ EvangelistaNo ratings yet
- Nurse Education Today: ReviewDocument12 pagesNurse Education Today: ReviewAlexsander SarmientoNo ratings yet
- The Usefulness and AcceptanceDocument7 pagesThe Usefulness and AcceptanceFATIMAH WANDANo ratings yet
- Seminar Prest UbthDocument19 pagesSeminar Prest UbthChioma PaschalineNo ratings yet
- Research For GramarianDocument66 pagesResearch For GramarianDelfhringerNo ratings yet
- Radiological Protection in The Perspective of HealthDocument4 pagesRadiological Protection in The Perspective of Healthhizwa harunNo ratings yet
- Living World Lesson Revised-1 1 C1aDocument15 pagesLiving World Lesson Revised-1 1 C1aapi-408497454No ratings yet
- Radiography: D. Sapkaroski, M. Mundy, M.R. DimmockDocument6 pagesRadiography: D. Sapkaroski, M. Mundy, M.R. DimmockFelipe RuizNo ratings yet
- Teaching and Learning Innovation in Present and Future of Human Anatomy Course in RSUDocument9 pagesTeaching and Learning Innovation in Present and Future of Human Anatomy Course in RSUPaul AndreasNo ratings yet
- 2016 - Developing An Ipad App For Assessment in Dance Movement TherapyDocument9 pages2016 - Developing An Ipad App For Assessment in Dance Movement TherapykriithigaNo ratings yet
- The Perception of Anatomy Teaching Among UK Medical StudentsDocument4 pagesThe Perception of Anatomy Teaching Among UK Medical StudentsPaul AndreasNo ratings yet
- Ma'am Finny 3Document10 pagesMa'am Finny 3Maria Peeva MahseyaNo ratings yet
- Reflection BAA Article SubmissionDocument11 pagesReflection BAA Article SubmissionRodrigoSantannaNo ratings yet
- The Most Effective Way of Delivering A Train-The-TrainersProgram A Systematic ReviewDocument12 pagesThe Most Effective Way of Delivering A Train-The-TrainersProgram A Systematic ReviewWendolyne RiosNo ratings yet
- Technology-Aided Assessments of Sensorimotor Function: Current Use, Barriers and Future Directions in The View of Different StakeholdersDocument17 pagesTechnology-Aided Assessments of Sensorimotor Function: Current Use, Barriers and Future Directions in The View of Different Stakeholderssiva82kNo ratings yet
- Eraut Report Into Surgical Training / ISCP - FullDocument69 pagesEraut Report Into Surgical Training / ISCP - FullAssociation of Surgeons in TrainingNo ratings yet
- The Arts in Psychotherapy: Kim Dunphy, Sue Mullane, Laura AllenDocument9 pagesThe Arts in Psychotherapy: Kim Dunphy, Sue Mullane, Laura AllenBogdanAnagnastopolNo ratings yet
- Portfolio Assessment Practice Teachers Early ExpeDocument15 pagesPortfolio Assessment Practice Teachers Early ExpeJovi AbabanNo ratings yet
- Texto02 PDFDocument8 pagesTexto02 PDFUBA ARTESNo ratings yet
- Practitioners' Perceptions of The Picture Exchange Communication System ForDocument8 pagesPractitioners' Perceptions of The Picture Exchange Communication System ForMuhammad Shehr YarNo ratings yet
- Canvas ManuscriptDocument32 pagesCanvas ManuscriptAnna CapillanNo ratings yet
- BSIR 2018 Essay - Teodros TrunehDocument2 pagesBSIR 2018 Essay - Teodros Trunehvefijo4087No ratings yet
- Danielson Aligned Lesson Plan 1 For MSDocument7 pagesDanielson Aligned Lesson Plan 1 For MSMTSEDENTONNo ratings yet
- Practical Radiation OncologyFrom EverandPractical Radiation OncologySupriya MallickNo ratings yet
- The Schoolwide Enrichment Model in Science: A Hands-On Approach for Engaging Young ScientistsFrom EverandThe Schoolwide Enrichment Model in Science: A Hands-On Approach for Engaging Young ScientistsRating: 5 out of 5 stars5/5 (1)
- Assosa University College of Computing and Informatics Department of Computer ScienceDocument22 pagesAssosa University College of Computing and Informatics Department of Computer ScienceseiyfuNo ratings yet
- Java Console (Standard Input Output)Document24 pagesJava Console (Standard Input Output)Albert OmondiNo ratings yet
- Institutional DevelopmentDocument19 pagesInstitutional Developmentwarda wisaalNo ratings yet
- Nodeb Data Configuration: InternalDocument57 pagesNodeb Data Configuration: InternalcurtiskamotoNo ratings yet
- Day 1Document2 pagesDay 1Hoa QuynhNo ratings yet
- POWER BI (DEC-2023) Updates SummaryDocument30 pagesPOWER BI (DEC-2023) Updates Summaryyuvvraj111No ratings yet
- Smartone Mobile CommunicationsDocument1 pageSmartone Mobile CommunicationsYonca Ahmet100% (2)
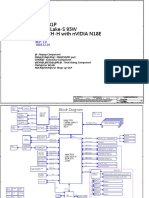
- Compal LA-G881P DDQ70 r1.0Document99 pagesCompal LA-G881P DDQ70 r1.0le04u100% (1)
- Tled 430w - Kristen Slate - Tpack Template Creating Fall20Document2 pagesTled 430w - Kristen Slate - Tpack Template Creating Fall20api-583361652No ratings yet
- Uc600 Bas-Prg010-En 12june2012Document8 pagesUc600 Bas-Prg010-En 12june2012cauvongkhongmauNo ratings yet
- HN7740S Broadband Satellite Router With Integrated VoIPDocument2 pagesHN7740S Broadband Satellite Router With Integrated VoIPMurillo M CarvalhoNo ratings yet
- Network Automation Cookbook Pdf00017Document5 pagesNetwork Automation Cookbook Pdf00017Dang KhueNo ratings yet
- Concept of Loading Text File To Ta Ble in ODI 12CDocument23 pagesConcept of Loading Text File To Ta Ble in ODI 12Cravi_405No ratings yet
- Computers: Machine-Learning-Based Emotion Recognition System Using EEG SignalsDocument15 pagesComputers: Machine-Learning-Based Emotion Recognition System Using EEG SignalslakshitNo ratings yet
- Welcome To CS256 31427Document46 pagesWelcome To CS256 31427Ramses MalalayNo ratings yet
- Week 1 Technical Appendix TemplateDocument3 pagesWeek 1 Technical Appendix Templatebender1686No ratings yet
- Question BankDocument2 pagesQuestion BanksangeethaNo ratings yet
- Mikrotik 2Document6 pagesMikrotik 2candelario jimenezNo ratings yet
- Solar & Energy StorageDocument10 pagesSolar & Energy StorageEku EmmanuelNo ratings yet
- Data-Collector-eSolar WiFi-DDocument1 pageData-Collector-eSolar WiFi-DFuad KrichouNo ratings yet
- Powerpoint Presentation On Java: Name - Devendra Kumar Mishra Roll No. - 1735110020Document26 pagesPowerpoint Presentation On Java: Name - Devendra Kumar Mishra Roll No. - 1735110020Devendra MishraNo ratings yet
- AIRA Modular Customizer Manual e PDFDocument41 pagesAIRA Modular Customizer Manual e PDFAndi Fadillah Muhammad100% (1)
- Installation Guide: AP6522 Access PointDocument56 pagesInstallation Guide: AP6522 Access PointJarek GawedaNo ratings yet
- VDMP3 Plug-In Voice Module V1.2: ProgrammingDocument2 pagesVDMP3 Plug-In Voice Module V1.2: ProgrammingMpampis KommenosNo ratings yet
- Experiment No 9: Install and Configure DNS ServerDocument7 pagesExperiment No 9: Install and Configure DNS ServerChandresh PrasadNo ratings yet
























































































Download as pdf or txt
You might also like
- ByDesign Subscription Billing CPI Configuration Guide 1902Document21 pagesByDesign Subscription Billing CPI Configuration Guide 1902nagaurjunaNo ratings yet
- Value of Research in The Area of InterestDocument36 pagesValue of Research in The Area of InterestRex Michael50% (8)
- 03 Task Performance 1 HCIDocument2 pages03 Task Performance 1 HCIKurt RaferNo ratings yet
- Modern Image Quality AssessmentDocument157 pagesModern Image Quality AssessmentRazii AbrahamNo ratings yet
- Unreal Engine GameDocument20 pagesUnreal Engine GameartNo ratings yet
- WritingDocument1 pageWritingIvan LazaroNo ratings yet
- Innovative TeachingDocument13 pagesInnovative TeachingShine BasayNo ratings yet
- Learning Preferences and Competencies of Radiologic Technology InternsDocument13 pagesLearning Preferences and Competencies of Radiologic Technology InternsIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet
- Thesis JeraldDocument7 pagesThesis Jeraldaljohn anticristoNo ratings yet
- 6Document7 pages6GSL SMART LABNo ratings yet
- AttentionDocument7 pagesAttentionChandra EkaNo ratings yet
- Enhancing Occupational Therapy Students Knowledge, Competence, Awareness and Interest in AccessibilityDocument8 pagesEnhancing Occupational Therapy Students Knowledge, Competence, Awareness and Interest in Accessibilityying reenNo ratings yet
- 1 s2.0 S1078817422000633 MainDocument7 pages1 s2.0 S1078817422000633 MainYamah PrincewillNo ratings yet
- CurriculumDocument114 pagesCurriculumMuhammad TariqNo ratings yet
- Dissertation InstrumentationDocument5 pagesDissertation InstrumentationCustomPaperWritingServicesUK100% (1)
- E-Learning Experience For Medical EducationDocument4 pagesE-Learning Experience For Medical Educationangelo.dibernardo63No ratings yet
- AECT - Definition of Educational TechnologyDocument16 pagesAECT - Definition of Educational TechnologyGd JohandanaNo ratings yet
- Medu 14194Document2 pagesMedu 14194ZoeNo ratings yet
- 10 1016@j Radi 2018 06 011Document8 pages10 1016@j Radi 2018 06 011Ricky Cahyasari PutraNo ratings yet
- Expanding Training Capacity For Radiographer Reporting UsingDocument6 pagesExpanding Training Capacity For Radiographer Reporting UsingC JoanesNo ratings yet
- Ecology and Evolution - 2020 - McDevitt - Lessons and Recommendations From Three Decades As An NSF REU Site A Call ForDocument29 pagesEcology and Evolution - 2020 - McDevitt - Lessons and Recommendations From Three Decades As An NSF REU Site A Call Foree wwNo ratings yet
- Duarte 2022Document12 pagesDuarte 2022Juan Carlos FloresNo ratings yet
- Clinical Education: MLS Student PerceptionsDocument6 pagesClinical Education: MLS Student PerceptionsUlfat NiazyNo ratings yet
- Tracey Pieterse (2016)Document10 pagesTracey Pieterse (2016)sigit hartantoNo ratings yet
- Specialty: Journal of Applied Behavior Analysis NumberDocument6 pagesSpecialty: Journal of Applied Behavior Analysis NumberalpNo ratings yet
- 070.2017.DesJardin - Near Peer Point of CareUltrasoundDocument9 pages070.2017.DesJardin - Near Peer Point of CareUltrasoundSergio San Juan DertkigilNo ratings yet
- Screening tool-SRDocument13 pagesScreening tool-SRSri purwantiNo ratings yet
- D20 ResearchDocument53 pagesD20 ResearchedmondNo ratings yet
- Multimedia Principal MayerDocument10 pagesMultimedia Principal Mayerandhika pradnyanaNo ratings yet
- 16Document2 pages16Walisson BarbosaNo ratings yet
- Teach USDocument6 pagesTeach USjonargNo ratings yet
- National Ultrasound Curriculum For Medical.4Document7 pagesNational Ultrasound Curriculum For Medical.4josephNo ratings yet
- English FinalsDocument28 pagesEnglish FinalsMark M. Alipio100% (1)
- Thesis RaritanDocument6 pagesThesis Raritandwtt67ef100% (2)
- Developing A Multimedia Courseware Using Cognitive Load TheoryDocument10 pagesDeveloping A Multimedia Courseware Using Cognitive Load TheorySMNo ratings yet
- Intro To RT Module 1Document2 pagesIntro To RT Module 1Jerel Waga UbarcoNo ratings yet
- Mashups For Learning - EditorialDocument3 pagesMashups For Learning - EditorialMartinNo ratings yet
- MeduloblastomaDocument12 pagesMeduloblastomaJonathanNo ratings yet
- New Normal CovidDocument2 pagesNew Normal Covidتغريد عبادةNo ratings yet
- Wong2022 Article CriticalCareUltrasoundDocument3 pagesWong2022 Article CriticalCareUltrasoundA. RaufNo ratings yet
- The Importance of Venipuncture Among The Third Year Radiologic Technology Students of Lyceum-Northwestern UniversityDocument17 pagesThe Importance of Venipuncture Among The Third Year Radiologic Technology Students of Lyceum-Northwestern UniversityCJ EvangelistaNo ratings yet
- Nurse Education Today: ReviewDocument12 pagesNurse Education Today: ReviewAlexsander SarmientoNo ratings yet
- The Usefulness and AcceptanceDocument7 pagesThe Usefulness and AcceptanceFATIMAH WANDANo ratings yet
- Seminar Prest UbthDocument19 pagesSeminar Prest UbthChioma PaschalineNo ratings yet
- Research For GramarianDocument66 pagesResearch For GramarianDelfhringerNo ratings yet
- Radiological Protection in The Perspective of HealthDocument4 pagesRadiological Protection in The Perspective of Healthhizwa harunNo ratings yet
- Living World Lesson Revised-1 1 C1aDocument15 pagesLiving World Lesson Revised-1 1 C1aapi-408497454No ratings yet
- Radiography: D. Sapkaroski, M. Mundy, M.R. DimmockDocument6 pagesRadiography: D. Sapkaroski, M. Mundy, M.R. DimmockFelipe RuizNo ratings yet
- Teaching and Learning Innovation in Present and Future of Human Anatomy Course in RSUDocument9 pagesTeaching and Learning Innovation in Present and Future of Human Anatomy Course in RSUPaul AndreasNo ratings yet
- 2016 - Developing An Ipad App For Assessment in Dance Movement TherapyDocument9 pages2016 - Developing An Ipad App For Assessment in Dance Movement TherapykriithigaNo ratings yet
- The Perception of Anatomy Teaching Among UK Medical StudentsDocument4 pagesThe Perception of Anatomy Teaching Among UK Medical StudentsPaul AndreasNo ratings yet
- Ma'am Finny 3Document10 pagesMa'am Finny 3Maria Peeva MahseyaNo ratings yet
- Reflection BAA Article SubmissionDocument11 pagesReflection BAA Article SubmissionRodrigoSantannaNo ratings yet
- The Most Effective Way of Delivering A Train-The-TrainersProgram A Systematic ReviewDocument12 pagesThe Most Effective Way of Delivering A Train-The-TrainersProgram A Systematic ReviewWendolyne RiosNo ratings yet
- Technology-Aided Assessments of Sensorimotor Function: Current Use, Barriers and Future Directions in The View of Different StakeholdersDocument17 pagesTechnology-Aided Assessments of Sensorimotor Function: Current Use, Barriers and Future Directions in The View of Different Stakeholderssiva82kNo ratings yet
- Eraut Report Into Surgical Training / ISCP - FullDocument69 pagesEraut Report Into Surgical Training / ISCP - FullAssociation of Surgeons in TrainingNo ratings yet
- The Arts in Psychotherapy: Kim Dunphy, Sue Mullane, Laura AllenDocument9 pagesThe Arts in Psychotherapy: Kim Dunphy, Sue Mullane, Laura AllenBogdanAnagnastopolNo ratings yet
- Portfolio Assessment Practice Teachers Early ExpeDocument15 pagesPortfolio Assessment Practice Teachers Early ExpeJovi AbabanNo ratings yet
- Texto02 PDFDocument8 pagesTexto02 PDFUBA ARTESNo ratings yet
- Practitioners' Perceptions of The Picture Exchange Communication System ForDocument8 pagesPractitioners' Perceptions of The Picture Exchange Communication System ForMuhammad Shehr YarNo ratings yet
- Canvas ManuscriptDocument32 pagesCanvas ManuscriptAnna CapillanNo ratings yet
- BSIR 2018 Essay - Teodros TrunehDocument2 pagesBSIR 2018 Essay - Teodros Trunehvefijo4087No ratings yet
- Danielson Aligned Lesson Plan 1 For MSDocument7 pagesDanielson Aligned Lesson Plan 1 For MSMTSEDENTONNo ratings yet
- Practical Radiation OncologyFrom EverandPractical Radiation OncologySupriya MallickNo ratings yet
- The Schoolwide Enrichment Model in Science: A Hands-On Approach for Engaging Young ScientistsFrom EverandThe Schoolwide Enrichment Model in Science: A Hands-On Approach for Engaging Young ScientistsRating: 5 out of 5 stars5/5 (1)
- Assosa University College of Computing and Informatics Department of Computer ScienceDocument22 pagesAssosa University College of Computing and Informatics Department of Computer ScienceseiyfuNo ratings yet
- Java Console (Standard Input Output)Document24 pagesJava Console (Standard Input Output)Albert OmondiNo ratings yet
- Institutional DevelopmentDocument19 pagesInstitutional Developmentwarda wisaalNo ratings yet
- Nodeb Data Configuration: InternalDocument57 pagesNodeb Data Configuration: InternalcurtiskamotoNo ratings yet
- Day 1Document2 pagesDay 1Hoa QuynhNo ratings yet
- POWER BI (DEC-2023) Updates SummaryDocument30 pagesPOWER BI (DEC-2023) Updates Summaryyuvvraj111No ratings yet
- Smartone Mobile CommunicationsDocument1 pageSmartone Mobile CommunicationsYonca Ahmet100% (2)
- Compal LA-G881P DDQ70 r1.0Document99 pagesCompal LA-G881P DDQ70 r1.0le04u100% (1)
- Tled 430w - Kristen Slate - Tpack Template Creating Fall20Document2 pagesTled 430w - Kristen Slate - Tpack Template Creating Fall20api-583361652No ratings yet
- Uc600 Bas-Prg010-En 12june2012Document8 pagesUc600 Bas-Prg010-En 12june2012cauvongkhongmauNo ratings yet
- HN7740S Broadband Satellite Router With Integrated VoIPDocument2 pagesHN7740S Broadband Satellite Router With Integrated VoIPMurillo M CarvalhoNo ratings yet
- Network Automation Cookbook Pdf00017Document5 pagesNetwork Automation Cookbook Pdf00017Dang KhueNo ratings yet
- Concept of Loading Text File To Ta Ble in ODI 12CDocument23 pagesConcept of Loading Text File To Ta Ble in ODI 12Cravi_405No ratings yet
- Computers: Machine-Learning-Based Emotion Recognition System Using EEG SignalsDocument15 pagesComputers: Machine-Learning-Based Emotion Recognition System Using EEG SignalslakshitNo ratings yet
- Welcome To CS256 31427Document46 pagesWelcome To CS256 31427Ramses MalalayNo ratings yet
- Week 1 Technical Appendix TemplateDocument3 pagesWeek 1 Technical Appendix Templatebender1686No ratings yet
- Question BankDocument2 pagesQuestion BanksangeethaNo ratings yet
- Mikrotik 2Document6 pagesMikrotik 2candelario jimenezNo ratings yet
- Solar & Energy StorageDocument10 pagesSolar & Energy StorageEku EmmanuelNo ratings yet
- Data-Collector-eSolar WiFi-DDocument1 pageData-Collector-eSolar WiFi-DFuad KrichouNo ratings yet
- Powerpoint Presentation On Java: Name - Devendra Kumar Mishra Roll No. - 1735110020Document26 pagesPowerpoint Presentation On Java: Name - Devendra Kumar Mishra Roll No. - 1735110020Devendra MishraNo ratings yet
- AIRA Modular Customizer Manual e PDFDocument41 pagesAIRA Modular Customizer Manual e PDFAndi Fadillah Muhammad100% (1)
- Installation Guide: AP6522 Access PointDocument56 pagesInstallation Guide: AP6522 Access PointJarek GawedaNo ratings yet
- VDMP3 Plug-In Voice Module V1.2: ProgrammingDocument2 pagesVDMP3 Plug-In Voice Module V1.2: ProgrammingMpampis KommenosNo ratings yet
- Experiment No 9: Install and Configure DNS ServerDocument7 pagesExperiment No 9: Install and Configure DNS ServerChandresh PrasadNo ratings yet