
Art GEBA
Art GEBA
You might also like
- Case Study 1Document13 pagesCase Study 1JoseDavidSierraLugoNo ratings yet
- CHCDIV002 Learner Guide V1.1Document69 pagesCHCDIV002 Learner Guide V1.1Nilu Thapa100% (3)
- Summer 2021Document23 pagesSummer 2021Paul BluemnerNo ratings yet
- Prof. Khafaji - Oswego.Document24 pagesProf. Khafaji - Oswego.Nur Hamizah Md Fuzi86% (7)
- Institute For Career Research - Career As An Epidemiologist - Public Health Specialists Searching For The Causes and Cures of Diseases and EpidemicsDocument30 pagesInstitute For Career Research - Career As An Epidemiologist - Public Health Specialists Searching For The Causes and Cures of Diseases and EpidemicsCynthia CNo ratings yet
- Personal StatementDocument4 pagesPersonal StatementssdasdNo ratings yet
- Diarrhoea Morbidity and Mortality in Older Children Adolescents and AdultsDocument12 pagesDiarrhoea Morbidity and Mortality in Older Children Adolescents and AdultsDelia KrisnasariNo ratings yet
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Document28 pagesDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNo ratings yet
- Clinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisgustiNo ratings yet
- Study DesignDocument3 pagesStudy Designmusa onyango obuyaNo ratings yet
- Epi Descriptive Study DesignsDocument4 pagesEpi Descriptive Study DesignsAndrea BardalesNo ratings yet
- Thesis EpidemiologyDocument6 pagesThesis Epidemiologykatieparkersaintpaul100% (3)
- CHN 2Document13 pagesCHN 2Claire Maurice JuaneroNo ratings yet
- Diarrhea Incidence in Low-And Middle-Income Countries in 1990 and 2010: A Systematic ReviewDocument7 pagesDiarrhea Incidence in Low-And Middle-Income Countries in 1990 and 2010: A Systematic ReviewRirin PurbaNo ratings yet
- EpidemiologyDocument7 pagesEpidemiologyInoxcent MoonNo ratings yet
- Annotated BibliographyDocument12 pagesAnnotated BibliographyJOSEPHNo ratings yet
- Principles of Epidemiology - Lesson 1 - Section 7Document3 pagesPrinciples of Epidemiology - Lesson 1 - Section 7Faria bukhariNo ratings yet
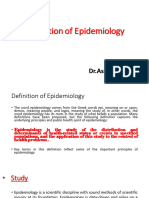
- Definition of EpidemiologyDocument3 pagesDefinition of EpidemiologyAnneke RamadhantyNo ratings yet
- Epidem. Lecture 1 & 2Document18 pagesEpidem. Lecture 1 & 2sajad abasew100% (1)
- EPI Lecture1Document43 pagesEPI Lecture1SoloNo ratings yet
- Survival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorDocument10 pagesSurvival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorGetachew GemedaNo ratings yet
- FoodborneDocument7 pagesFoodborneMara MoránNo ratings yet
- QA, Module Module 2 Methods and Epidemiology of DiseasesDocument12 pagesQA, Module Module 2 Methods and Epidemiology of DiseasesPriyank LashkariNo ratings yet
- EpidemiologyDocument64 pagesEpidemiologyNisha FatmaNo ratings yet
- LSHTM Study Designs NOTES LSTHMDocument39 pagesLSHTM Study Designs NOTES LSTHMKELVIN MAYOMBONo ratings yet
- Introduction of EpiDocument22 pagesIntroduction of Epidrrana.alshabiNo ratings yet
- The Vaccine Book 2nd EditionDocument61 pagesThe Vaccine Book 2nd Editiontom.dimaggio515100% (41)
- Epidemiology With Part 2 (Complete) 2Document59 pagesEpidemiology With Part 2 (Complete) 2nahNo ratings yet
- EpidemiologyDocument72 pagesEpidemiologyharshitadedhaworkNo ratings yet
- P.Epidemiology (5.6)Document12 pagesP.Epidemiology (5.6)Rawan SedkyNo ratings yet
- Uses of EpidemiologyDocument28 pagesUses of EpidemiologyBinita Shakya0% (1)
- Jurnal KedokteranDocument18 pagesJurnal KedokteranelvandryNo ratings yet
- Amit Kumar KumawatDocument9 pagesAmit Kumar KumawatAmit Kumar kumawatNo ratings yet
- EpidemiologyDocument10 pagesEpidemiologyMUTHUKUMARANNo ratings yet
- Epidemiiology SeminarDocument15 pagesEpidemiiology SeminarMugu 123No ratings yet
- Tugas Merangkum Epidemiologi Safira M.20.02.050Document5 pagesTugas Merangkum Epidemiologi Safira M.20.02.050safira saalNo ratings yet
- 1st LectureDocument6 pages1st LectureNoreen FæţįmæNo ratings yet
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Epidemiologi of HFMDDocument16 pagesEpidemiologi of HFMDJimmy AmbaritaNo ratings yet
- Severe Acute Hepatitis of Unknown Aetiology in Children-What Is Known?Document9 pagesSevere Acute Hepatitis of Unknown Aetiology in Children-What Is Known?Dr Meenakshi ParwaniNo ratings yet
- Epidemiology & Health Information: NU1103 Tara Brookes @tarapb8Document40 pagesEpidemiology & Health Information: NU1103 Tara Brookes @tarapb8smartisaacNo ratings yet
- Concept of EpidemiologyDocument40 pagesConcept of EpidemiologyAshim PoudelNo ratings yet
- Study Types TranscriptDocument12 pagesStudy Types TranscriptALYA MAULIDANo ratings yet
- Descriptive EpidemiologyDocument7 pagesDescriptive EpidemiologyVineeta JoseNo ratings yet
- Prevalence of TB-HIV Co-Infection in Countries Except ChinaDocument8 pagesPrevalence of TB-HIV Co-Infection in Countries Except ChinaElizabeth AmezcuaNo ratings yet
- EPI Lecture Note April 2005, YemaneDocument132 pagesEPI Lecture Note April 2005, YemaneGetahun TekleNo ratings yet
- Diarrea en QuimioterapiaDocument6 pagesDiarrea en QuimioterapiaPaola DiazNo ratings yet
- Global Illness and Deaths Caused by Rotavirus Disease in ChildrenDocument8 pagesGlobal Illness and Deaths Caused by Rotavirus Disease in ChildrenElena NazâruNo ratings yet
- Global H Pylori DataDocument10 pagesGlobal H Pylori DataSohail ManzoorNo ratings yet
- Unit 8 Applications of Epidemiology in Community Health 1Document5 pagesUnit 8 Applications of Epidemiology in Community Health 1Aizeen MiguelNo ratings yet
- Epidemiology - Intro - 11Document58 pagesEpidemiology - Intro - 11Tin WannNo ratings yet
- Keski Rahkonenetal2008Epidemiologyofeatingdisorders AnupdateDocument12 pagesKeski Rahkonenetal2008Epidemiologyofeatingdisorders AnupdateHelena OliveiraNo ratings yet
- Methods Used in EpidemologyDocument53 pagesMethods Used in EpidemologySameera banuNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- 200 Supplement - 1 S9Document7 pages200 Supplement - 1 S9Kollar RolandNo ratings yet
- EDA. Pediatrics 2010Document12 pagesEDA. Pediatrics 2010Carkos MorenoNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Estimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextDocument33 pagesEstimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextAli AlyousfeNo ratings yet
- A Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedDocument16 pagesA Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedHow ToNo ratings yet
- Prospective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineDocument30 pagesProspective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineMona SamiNo ratings yet
- Term Paper EpidemiologyDocument8 pagesTerm Paper Epidemiologyc5m07hh9100% (1)
- MC-No.-08-s.-2020-Interim-Guidelines-COVID - 19 - Esigned-MC8-2020 To Agencies PALD 4-3-20Document8 pagesMC-No.-08-s.-2020-Interim-Guidelines-COVID - 19 - Esigned-MC8-2020 To Agencies PALD 4-3-20JoTanlogonOcate-AmbongNo ratings yet
- Bioprocess Technology: Course Code: BTB 701 Credit Units: 03Document5 pagesBioprocess Technology: Course Code: BTB 701 Credit Units: 03Sahil GuptaNo ratings yet
- 53 JMSCRDocument7 pages53 JMSCRAddinul FitryNo ratings yet
- List of Programs, Projects and Activities (Ppas) in SchoolsDocument2 pagesList of Programs, Projects and Activities (Ppas) in Schoolscjade08100% (5)
- 2 Cholinergic BlockersDocument49 pages2 Cholinergic BlockersAmanuel MaruNo ratings yet
- PM&QS Capability Statement - GSKDocument58 pagesPM&QS Capability Statement - GSKcollincucNo ratings yet
- Cukb Materi ViiDocument34 pagesCukb Materi Viirandybayu235No ratings yet
- Reducing Vulnerability of Individuals and FamiliesDocument1 pageReducing Vulnerability of Individuals and FamilieshaykoNo ratings yet
- Allergic Conjunctivitis JournalDocument15 pagesAllergic Conjunctivitis JournalSisiliaElfaniPebiantiaNo ratings yet
- Detailed System Design: 4.1. Use Case DiagramDocument4 pagesDetailed System Design: 4.1. Use Case DiagramammaraNo ratings yet
- SOP For Tarpaulin Sealing of Transportation Truck - 21Document5 pagesSOP For Tarpaulin Sealing of Transportation Truck - 21syed aquib100% (1)
- Design Manual For Small Wastewater Works 2009-1Document62 pagesDesign Manual For Small Wastewater Works 2009-1VichekaNo ratings yet
- Case Study PsychiaDocument6 pagesCase Study PsychiaJay Jay GwapoNo ratings yet
- MEDITATIONS, QUOTES Vol 35Document52 pagesMEDITATIONS, QUOTES Vol 35Ardelean Gheorghe CornelNo ratings yet
- Lasers in Dermatology: Four Decades of Progress: Review ArticleDocument5 pagesLasers in Dermatology: Four Decades of Progress: Review ArticledtramirNo ratings yet
- Anti Acid OsDocument13 pagesAnti Acid OsnicolaslanchNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- Midterm Exam Campus JournalismDocument3 pagesMidterm Exam Campus JournalismReñer Aquino BystanderNo ratings yet
- SA U5 Law of Tort - Final Web PDFDocument6 pagesSA U5 Law of Tort - Final Web PDFsaidatuladani100% (1)
- Capsule: 500 MG Injection: 100Document2 pagesCapsule: 500 MG Injection: 100Melissa Marie CustodioNo ratings yet
- MN Thesis Stream Progress ReportDocument4 pagesMN Thesis Stream Progress ReportFarhana AnuarNo ratings yet
- Final Exam Review Sheet1 Mental Health NursingDocument30 pagesFinal Exam Review Sheet1 Mental Health NursingSarah S100% (5)
- SWMS (Cable Glanding and Termination )Document6 pagesSWMS (Cable Glanding and Termination )PRIYESH . K. PRIYANNo ratings yet
- Gcse Catering Coursework Task 2Document6 pagesGcse Catering Coursework Task 2fqvtmyzid100% (2)
- Internet Addiction SurveyDocument19 pagesInternet Addiction SurveyKapitanNo ratings yet
- Model Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentDocument5 pagesModel Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentphuongthaospkNo ratings yet
- SITXFSA101 Assessment 1Document6 pagesSITXFSA101 Assessment 1Jakub25% (8)
























































































Download as pdf or txt
You might also like
- Case Study 1Document13 pagesCase Study 1JoseDavidSierraLugoNo ratings yet
- CHCDIV002 Learner Guide V1.1Document69 pagesCHCDIV002 Learner Guide V1.1Nilu Thapa100% (3)
- Summer 2021Document23 pagesSummer 2021Paul BluemnerNo ratings yet
- Prof. Khafaji - Oswego.Document24 pagesProf. Khafaji - Oswego.Nur Hamizah Md Fuzi86% (7)
- Institute For Career Research - Career As An Epidemiologist - Public Health Specialists Searching For The Causes and Cures of Diseases and EpidemicsDocument30 pagesInstitute For Career Research - Career As An Epidemiologist - Public Health Specialists Searching For The Causes and Cures of Diseases and EpidemicsCynthia CNo ratings yet
- Personal StatementDocument4 pagesPersonal StatementssdasdNo ratings yet
- Diarrhoea Morbidity and Mortality in Older Children Adolescents and AdultsDocument12 pagesDiarrhoea Morbidity and Mortality in Older Children Adolescents and AdultsDelia KrisnasariNo ratings yet
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Document28 pagesDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNo ratings yet
- Clinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisgustiNo ratings yet
- Study DesignDocument3 pagesStudy Designmusa onyango obuyaNo ratings yet
- Epi Descriptive Study DesignsDocument4 pagesEpi Descriptive Study DesignsAndrea BardalesNo ratings yet
- Thesis EpidemiologyDocument6 pagesThesis Epidemiologykatieparkersaintpaul100% (3)
- CHN 2Document13 pagesCHN 2Claire Maurice JuaneroNo ratings yet
- Diarrhea Incidence in Low-And Middle-Income Countries in 1990 and 2010: A Systematic ReviewDocument7 pagesDiarrhea Incidence in Low-And Middle-Income Countries in 1990 and 2010: A Systematic ReviewRirin PurbaNo ratings yet
- EpidemiologyDocument7 pagesEpidemiologyInoxcent MoonNo ratings yet
- Annotated BibliographyDocument12 pagesAnnotated BibliographyJOSEPHNo ratings yet
- Principles of Epidemiology - Lesson 1 - Section 7Document3 pagesPrinciples of Epidemiology - Lesson 1 - Section 7Faria bukhariNo ratings yet
- Definition of EpidemiologyDocument3 pagesDefinition of EpidemiologyAnneke RamadhantyNo ratings yet
- Epidem. Lecture 1 & 2Document18 pagesEpidem. Lecture 1 & 2sajad abasew100% (1)
- EPI Lecture1Document43 pagesEPI Lecture1SoloNo ratings yet
- Survival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorDocument10 pagesSurvival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorGetachew GemedaNo ratings yet
- FoodborneDocument7 pagesFoodborneMara MoránNo ratings yet
- QA, Module Module 2 Methods and Epidemiology of DiseasesDocument12 pagesQA, Module Module 2 Methods and Epidemiology of DiseasesPriyank LashkariNo ratings yet
- EpidemiologyDocument64 pagesEpidemiologyNisha FatmaNo ratings yet
- LSHTM Study Designs NOTES LSTHMDocument39 pagesLSHTM Study Designs NOTES LSTHMKELVIN MAYOMBONo ratings yet
- Introduction of EpiDocument22 pagesIntroduction of Epidrrana.alshabiNo ratings yet
- The Vaccine Book 2nd EditionDocument61 pagesThe Vaccine Book 2nd Editiontom.dimaggio515100% (41)
- Epidemiology With Part 2 (Complete) 2Document59 pagesEpidemiology With Part 2 (Complete) 2nahNo ratings yet
- EpidemiologyDocument72 pagesEpidemiologyharshitadedhaworkNo ratings yet
- P.Epidemiology (5.6)Document12 pagesP.Epidemiology (5.6)Rawan SedkyNo ratings yet
- Uses of EpidemiologyDocument28 pagesUses of EpidemiologyBinita Shakya0% (1)
- Jurnal KedokteranDocument18 pagesJurnal KedokteranelvandryNo ratings yet
- Amit Kumar KumawatDocument9 pagesAmit Kumar KumawatAmit Kumar kumawatNo ratings yet
- EpidemiologyDocument10 pagesEpidemiologyMUTHUKUMARANNo ratings yet
- Epidemiiology SeminarDocument15 pagesEpidemiiology SeminarMugu 123No ratings yet
- Tugas Merangkum Epidemiologi Safira M.20.02.050Document5 pagesTugas Merangkum Epidemiologi Safira M.20.02.050safira saalNo ratings yet
- 1st LectureDocument6 pages1st LectureNoreen FæţįmæNo ratings yet
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Epidemiologi of HFMDDocument16 pagesEpidemiologi of HFMDJimmy AmbaritaNo ratings yet
- Severe Acute Hepatitis of Unknown Aetiology in Children-What Is Known?Document9 pagesSevere Acute Hepatitis of Unknown Aetiology in Children-What Is Known?Dr Meenakshi ParwaniNo ratings yet
- Epidemiology & Health Information: NU1103 Tara Brookes @tarapb8Document40 pagesEpidemiology & Health Information: NU1103 Tara Brookes @tarapb8smartisaacNo ratings yet
- Concept of EpidemiologyDocument40 pagesConcept of EpidemiologyAshim PoudelNo ratings yet
- Study Types TranscriptDocument12 pagesStudy Types TranscriptALYA MAULIDANo ratings yet
- Descriptive EpidemiologyDocument7 pagesDescriptive EpidemiologyVineeta JoseNo ratings yet
- Prevalence of TB-HIV Co-Infection in Countries Except ChinaDocument8 pagesPrevalence of TB-HIV Co-Infection in Countries Except ChinaElizabeth AmezcuaNo ratings yet
- EPI Lecture Note April 2005, YemaneDocument132 pagesEPI Lecture Note April 2005, YemaneGetahun TekleNo ratings yet
- Diarrea en QuimioterapiaDocument6 pagesDiarrea en QuimioterapiaPaola DiazNo ratings yet
- Global Illness and Deaths Caused by Rotavirus Disease in ChildrenDocument8 pagesGlobal Illness and Deaths Caused by Rotavirus Disease in ChildrenElena NazâruNo ratings yet
- Global H Pylori DataDocument10 pagesGlobal H Pylori DataSohail ManzoorNo ratings yet
- Unit 8 Applications of Epidemiology in Community Health 1Document5 pagesUnit 8 Applications of Epidemiology in Community Health 1Aizeen MiguelNo ratings yet
- Epidemiology - Intro - 11Document58 pagesEpidemiology - Intro - 11Tin WannNo ratings yet
- Keski Rahkonenetal2008Epidemiologyofeatingdisorders AnupdateDocument12 pagesKeski Rahkonenetal2008Epidemiologyofeatingdisorders AnupdateHelena OliveiraNo ratings yet
- Methods Used in EpidemologyDocument53 pagesMethods Used in EpidemologySameera banuNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- 200 Supplement - 1 S9Document7 pages200 Supplement - 1 S9Kollar RolandNo ratings yet
- EDA. Pediatrics 2010Document12 pagesEDA. Pediatrics 2010Carkos MorenoNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Estimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextDocument33 pagesEstimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextAli AlyousfeNo ratings yet
- A Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedDocument16 pagesA Systematic Review On The Development of Asthma and Allergic Diseases in Relation To International Immigration: The Leading Role of The Environment ConfirmedHow ToNo ratings yet
- Prospective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineDocument30 pagesProspective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineMona SamiNo ratings yet
- Term Paper EpidemiologyDocument8 pagesTerm Paper Epidemiologyc5m07hh9100% (1)
- MC-No.-08-s.-2020-Interim-Guidelines-COVID - 19 - Esigned-MC8-2020 To Agencies PALD 4-3-20Document8 pagesMC-No.-08-s.-2020-Interim-Guidelines-COVID - 19 - Esigned-MC8-2020 To Agencies PALD 4-3-20JoTanlogonOcate-AmbongNo ratings yet
- Bioprocess Technology: Course Code: BTB 701 Credit Units: 03Document5 pagesBioprocess Technology: Course Code: BTB 701 Credit Units: 03Sahil GuptaNo ratings yet
- 53 JMSCRDocument7 pages53 JMSCRAddinul FitryNo ratings yet
- List of Programs, Projects and Activities (Ppas) in SchoolsDocument2 pagesList of Programs, Projects and Activities (Ppas) in Schoolscjade08100% (5)
- 2 Cholinergic BlockersDocument49 pages2 Cholinergic BlockersAmanuel MaruNo ratings yet
- PM&QS Capability Statement - GSKDocument58 pagesPM&QS Capability Statement - GSKcollincucNo ratings yet
- Cukb Materi ViiDocument34 pagesCukb Materi Viirandybayu235No ratings yet
- Reducing Vulnerability of Individuals and FamiliesDocument1 pageReducing Vulnerability of Individuals and FamilieshaykoNo ratings yet
- Allergic Conjunctivitis JournalDocument15 pagesAllergic Conjunctivitis JournalSisiliaElfaniPebiantiaNo ratings yet
- Detailed System Design: 4.1. Use Case DiagramDocument4 pagesDetailed System Design: 4.1. Use Case DiagramammaraNo ratings yet
- SOP For Tarpaulin Sealing of Transportation Truck - 21Document5 pagesSOP For Tarpaulin Sealing of Transportation Truck - 21syed aquib100% (1)
- Design Manual For Small Wastewater Works 2009-1Document62 pagesDesign Manual For Small Wastewater Works 2009-1VichekaNo ratings yet
- Case Study PsychiaDocument6 pagesCase Study PsychiaJay Jay GwapoNo ratings yet
- MEDITATIONS, QUOTES Vol 35Document52 pagesMEDITATIONS, QUOTES Vol 35Ardelean Gheorghe CornelNo ratings yet
- Lasers in Dermatology: Four Decades of Progress: Review ArticleDocument5 pagesLasers in Dermatology: Four Decades of Progress: Review ArticledtramirNo ratings yet
- Anti Acid OsDocument13 pagesAnti Acid OsnicolaslanchNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- Midterm Exam Campus JournalismDocument3 pagesMidterm Exam Campus JournalismReñer Aquino BystanderNo ratings yet
- SA U5 Law of Tort - Final Web PDFDocument6 pagesSA U5 Law of Tort - Final Web PDFsaidatuladani100% (1)
- Capsule: 500 MG Injection: 100Document2 pagesCapsule: 500 MG Injection: 100Melissa Marie CustodioNo ratings yet
- MN Thesis Stream Progress ReportDocument4 pagesMN Thesis Stream Progress ReportFarhana AnuarNo ratings yet
- Final Exam Review Sheet1 Mental Health NursingDocument30 pagesFinal Exam Review Sheet1 Mental Health NursingSarah S100% (5)
- SWMS (Cable Glanding and Termination )Document6 pagesSWMS (Cable Glanding and Termination )PRIYESH . K. PRIYANNo ratings yet
- Gcse Catering Coursework Task 2Document6 pagesGcse Catering Coursework Task 2fqvtmyzid100% (2)
- Internet Addiction SurveyDocument19 pagesInternet Addiction SurveyKapitanNo ratings yet
- Model Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentDocument5 pagesModel Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentphuongthaospkNo ratings yet
- SITXFSA101 Assessment 1Document6 pagesSITXFSA101 Assessment 1Jakub25% (8)