
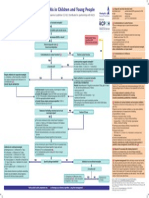
Bacterial Meningitis and Meningococcal Septicaemia in Under 16s Diagnosis of Bacterial Meningitis and Meningococcal Septicaemia in Secondary Care
Bacterial Meningitis and Meningococcal Septicaemia in Under 16s Diagnosis of Bacterial Meningitis and Meningococcal Septicaemia in Secondary Care
You might also like
- Pediatric NursingDocument22 pagesPediatric NursingDarren Mae MosadaNo ratings yet
- Admission LetterDocument4 pagesAdmission LetterYasir KNNo ratings yet
- Lesson Plan Lumbar PunctureDocument25 pagesLesson Plan Lumbar PunctureValarmathi50% (4)
- Bacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceDocument18 pagesBacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceZarwo Black UstadzNo ratings yet
- Meningitis and Lumbar PunctureDocument38 pagesMeningitis and Lumbar PunctureJeo ThomasNo ratings yet
- Fod en Niños Menores de 3 MesesDocument16 pagesFod en Niños Menores de 3 MesesPaul Gutiérrez MyrickNo ratings yet
- Diagnosis and Treatment of Bacterial Meningitis: Arch. Dis. ChildDocument7 pagesDiagnosis and Treatment of Bacterial Meningitis: Arch. Dis. Childapi-214563632No ratings yet
- Meningitis in Adults: Diagnosis and Management: PembimbingDocument45 pagesMeningitis in Adults: Diagnosis and Management: PembimbingNeny Mathilda UniplaitaNo ratings yet
- Meningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingDocument14 pagesMeningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingdilaNo ratings yet
- Guideline MeningitisDocument1 pageGuideline MeningitisAmbc Smfk-uaj100% (1)
- Infectiousdiseases 130804135335 Phpapp02Document42 pagesInfectiousdiseases 130804135335 Phpapp02OleOhhNo ratings yet
- Investigating Procalcitonin and C-Reactive Protein As Diagnostic Biomarkers in Pediatric Suspected Meningitis: A Forward-Looking Observational AnalysisDocument16 pagesInvestigating Procalcitonin and C-Reactive Protein As Diagnostic Biomarkers in Pediatric Suspected Meningitis: A Forward-Looking Observational AnalysisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bacterial Meningitis in Children - DynaMedDocument88 pagesBacterial Meningitis in Children - DynaMedCarlos CalderwoodNo ratings yet
- Reflective Journal ReadingDocument13 pagesReflective Journal Readingعبداللة العمراني الحويطيNo ratings yet
- Bacterial Meningitis in AdultsDocument55 pagesBacterial Meningitis in AdultsfjnaressiNo ratings yet
- The Febrile Infant 29 To 90 Days of Age Management UpToDateDocument74 pagesThe Febrile Infant 29 To 90 Days of Age Management UpToDateSharafuddin SalimiNo ratings yet
- Serum Procalcitonin Levels in Bacterial and Abacterial MeningitisDocument5 pagesSerum Procalcitonin Levels in Bacterial and Abacterial MeningitisSaul Gonzalez HernandezNo ratings yet
- Meningitis PresentationDocument41 pagesMeningitis PresentationO'Mark AndrewsNo ratings yet
- Bacterial Meningitis in Infants Over 3 Months of AgeDocument8 pagesBacterial Meningitis in Infants Over 3 Months of AgedrirrazabalNo ratings yet
- Newborn Sepsis GuidelineDocument2 pagesNewborn Sepsis GuidelineAmelia ArnisNo ratings yet
- Treatment of Children With COVID-19: Position Paper of The Italian Society of Pediatric Infectious DiseaseDocument17 pagesTreatment of Children With COVID-19: Position Paper of The Italian Society of Pediatric Infectious DiseasecurteanancaNo ratings yet
- Covid Ep IiDocument29 pagesCovid Ep IiLuis Armando López SosaNo ratings yet
- Neonatal InfectionsDocument41 pagesNeonatal Infectionsamid sultanNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in AdultsDocument48 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in AdultsIsmael IbrahimNo ratings yet
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- TREATMENT Bacterial MeningitisDocument32 pagesTREATMENT Bacterial MeningitisironNo ratings yet
- Research Paper On Bacterial MeningitisDocument8 pagesResearch Paper On Bacterial Meningitisvvgnzdbkf100% (1)
- Case 10 Fever PDFDocument5 pagesCase 10 Fever PDFSue HuangNo ratings yet
- Test ID: PCT Procalcitonin, Serum: Useful ForDocument5 pagesTest ID: PCT Procalcitonin, Serum: Useful ForI Nyoman Gede SemarajanaNo ratings yet
- Research Paper Bacterial MeningitisDocument4 pagesResearch Paper Bacterial Meningitisafeebovus100% (1)
- Bacterial Meningitis ThesisDocument8 pagesBacterial Meningitis ThesisRick Vogel100% (2)
- 35-Article Text-212-1-10-20200524Document4 pages35-Article Text-212-1-10-20200524SONIA AGUILAR RIVERANo ratings yet
- Clin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiDocument18 pagesClin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiJesus Salvador SerratoNo ratings yet
- Tuberculosis in ChildrenDocument4 pagesTuberculosis in ChildrenMarthin TheservantNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- Sepsis NeonatalDocument21 pagesSepsis NeonatalRaissa 'Icha' Nurwany RizalNo ratings yet
- Diagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyDocument4 pagesDiagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyChoi SpeaksNo ratings yet
- Covid 19 Pediatric Multi System Inflammatory SyndromeDocument2 pagesCovid 19 Pediatric Multi System Inflammatory SyndromeministerenqiNo ratings yet
- Guia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Document18 pagesGuia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Brenda Anali Pariona NapaNo ratings yet
- Neonatal SepsisDocument31 pagesNeonatal Sepsisanwar jabariNo ratings yet
- (Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)Document662 pages(Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)gnkgbjkgjkNo ratings yet
- PCAP ReportDocument28 pagesPCAP ReportAngeline Zamoras-ToledoNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisBhawna PandhuNo ratings yet
- Bacterial MeningitisDocument51 pagesBacterial MeningitiscaseinrenninNo ratings yet
- Bacterial Meningitis in The Neonate - Neurologic Complications - UpToDateDocument9 pagesBacterial Meningitis in The Neonate - Neurologic Complications - UpToDateAngélica PedrazaNo ratings yet
- Meningitis PDFDocument8 pagesMeningitis PDFrizeviNo ratings yet
- Frequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulDocument9 pagesFrequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulNaeem NawazNo ratings yet
- Bacterial MeningitisDocument5 pagesBacterial Meningitisjamesignacio787No ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- MengititisDocument38 pagesMengititisRas Siko SafoNo ratings yet
- Neonatal Meningitis Due To Clostridium Neonatale: A Case ReportDocument4 pagesNeonatal Meningitis Due To Clostridium Neonatale: A Case ReportCarina ColtuneacNo ratings yet
- MMC 1Document9 pagesMMC 1Maulida 04No ratings yet
- Jurnal AsliDocument8 pagesJurnal AsliDwi PurwantiNo ratings yet
- Sepsis in The Newborn - Latest NewsDocument13 pagesSepsis in The Newborn - Latest NewsBrunaNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisLeana SiñelNo ratings yet
- Clinical Features: - Initial Symptoms in Patients With MeningitisDocument12 pagesClinical Features: - Initial Symptoms in Patients With Meningitisyuii_48No ratings yet
- Meningitis in Adults - Diagnosis and Management - Young - 2018 - Internal Medicine Journal - Wiley Online LibraryDocument27 pagesMeningitis in Adults - Diagnosis and Management - Young - 2018 - Internal Medicine Journal - Wiley Online Libraryaslan tonapaNo ratings yet
- Meningitis: By-Dr Nimco A. MDDocument31 pagesMeningitis: By-Dr Nimco A. MDgibreilNo ratings yet
- C V 9 V VV VV V V VVVVVVVV V: "V "V "V "V "VDocument2 pagesC V 9 V VV VV V V VVVVVVVV V: "V "V "V "V "VCharlene Mae CalanoyNo ratings yet
- Paediatrica Indonesiana: Original ArticleDocument5 pagesPaediatrica Indonesiana: Original ArticleSyukron AmrullahNo ratings yet
- Peds InfectiousDocument8 pagesPeds InfectiousMohammad RammalNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- Stroke Differential Diagnosis and Mimics: Part 2Document9 pagesStroke Differential Diagnosis and Mimics: Part 2Natalia E PenagosNo ratings yet
- Seizure Pediatric Scenario June 2016Document4 pagesSeizure Pediatric Scenario June 2016Natalia E PenagosNo ratings yet
- Ene 15103Document8 pagesEne 15103Natalia E PenagosNo ratings yet
- Dom 14270Document19 pagesDom 14270Natalia E PenagosNo ratings yet
- Epilepsy Imaging: Approaches and ProtocolsDocument9 pagesEpilepsy Imaging: Approaches and ProtocolsNatalia E PenagosNo ratings yet
- Peeds Infection LecturesDocument190 pagesPeeds Infection LecturesAli Al.JuffairiNo ratings yet
- 282585293Document208 pages282585293hebaNo ratings yet
- Infections FarazDocument10 pagesInfections FarazM R SIFATNo ratings yet
- Lumbar Puncture ResearchDocument6 pagesLumbar Puncture Researchanon_464104226No ratings yet
- CDDocument6 pagesCDMei JoyNo ratings yet
- اسئلة neuroDocument30 pagesاسئلة neuroSoad RedaNo ratings yet
- Brain AbscessDocument2 pagesBrain AbscessIan RomanNo ratings yet
- Stool Analysis and Other Body Fluid AnalysisDocument51 pagesStool Analysis and Other Body Fluid AnalysisPutri Senna Rahayu100% (2)
- 83K English Class Examination Questions of Infectious DiseaseDocument23 pages83K English Class Examination Questions of Infectious Diseasetarun956519No ratings yet
- Intrathecal Hyaluronidase in TB Meningitis: The Unexplored AdjuvantDocument5 pagesIntrathecal Hyaluronidase in TB Meningitis: The Unexplored AdjuvantPriyanka SamalNo ratings yet
- Idr 240162 Management of Acute Bacterial Meningitis in ChildrenDocument13 pagesIdr 240162 Management of Acute Bacterial Meningitis in ChildrenindahrizkygNo ratings yet
- Epidemiology and Management Og Meningococcal MeningitisDocument12 pagesEpidemiology and Management Og Meningococcal MeningitispriyankaNo ratings yet
- Epidemic Cerebrospinal MeningitisDocument76 pagesEpidemic Cerebrospinal MeningitisAngie LawrenceNo ratings yet
- Some Imp Oneliner From VolumesDocument16 pagesSome Imp Oneliner From VolumesTejas KaleNo ratings yet
- Cases Lab 2020Document16 pagesCases Lab 2020Buushi96No ratings yet
- B) Meningococcal MeningitisDocument7 pagesB) Meningococcal MeningitisWe'am QutubNo ratings yet
- MCQ April 2015Document15 pagesMCQ April 2015Sylphana Astharica LawalataNo ratings yet
- Writing Notes: The Ideal Letter Should Have 6 PartsDocument7 pagesWriting Notes: The Ideal Letter Should Have 6 PartsMMW MNo ratings yet
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDocument7 pagesC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINo ratings yet
- Meningitis ViralDocument7 pagesMeningitis ViralTia Gustiani Poplei ViolaNo ratings yet
- Communicable Disease ChartDocument5 pagesCommunicable Disease ChartAuspice QatarNo ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- Abdullahi V Pfizer Inc PDFDocument44 pagesAbdullahi V Pfizer Inc PDFBevs DomingoNo ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
- Blog Post About National Poultry Day 2023Document63 pagesBlog Post About National Poultry Day 2023ZETTYNo ratings yet
- Date/Time Doctors Order RationaleDocument4 pagesDate/Time Doctors Order RationaleChamCham AquinoNo ratings yet
- HAAD Test 4 QuestionsDocument17 pagesHAAD Test 4 QuestionsPhine PhineNo ratings yet





























































































Download as pdf or txt
You might also like
- Pediatric NursingDocument22 pagesPediatric NursingDarren Mae MosadaNo ratings yet
- Admission LetterDocument4 pagesAdmission LetterYasir KNNo ratings yet
- Lesson Plan Lumbar PunctureDocument25 pagesLesson Plan Lumbar PunctureValarmathi50% (4)
- Bacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceDocument18 pagesBacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceZarwo Black UstadzNo ratings yet
- Meningitis and Lumbar PunctureDocument38 pagesMeningitis and Lumbar PunctureJeo ThomasNo ratings yet
- Fod en Niños Menores de 3 MesesDocument16 pagesFod en Niños Menores de 3 MesesPaul Gutiérrez MyrickNo ratings yet
- Diagnosis and Treatment of Bacterial Meningitis: Arch. Dis. ChildDocument7 pagesDiagnosis and Treatment of Bacterial Meningitis: Arch. Dis. Childapi-214563632No ratings yet
- Meningitis in Adults: Diagnosis and Management: PembimbingDocument45 pagesMeningitis in Adults: Diagnosis and Management: PembimbingNeny Mathilda UniplaitaNo ratings yet
- Meningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingDocument14 pagesMeningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingdilaNo ratings yet
- Guideline MeningitisDocument1 pageGuideline MeningitisAmbc Smfk-uaj100% (1)
- Infectiousdiseases 130804135335 Phpapp02Document42 pagesInfectiousdiseases 130804135335 Phpapp02OleOhhNo ratings yet
- Investigating Procalcitonin and C-Reactive Protein As Diagnostic Biomarkers in Pediatric Suspected Meningitis: A Forward-Looking Observational AnalysisDocument16 pagesInvestigating Procalcitonin and C-Reactive Protein As Diagnostic Biomarkers in Pediatric Suspected Meningitis: A Forward-Looking Observational AnalysisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bacterial Meningitis in Children - DynaMedDocument88 pagesBacterial Meningitis in Children - DynaMedCarlos CalderwoodNo ratings yet
- Reflective Journal ReadingDocument13 pagesReflective Journal Readingعبداللة العمراني الحويطيNo ratings yet
- Bacterial Meningitis in AdultsDocument55 pagesBacterial Meningitis in AdultsfjnaressiNo ratings yet
- The Febrile Infant 29 To 90 Days of Age Management UpToDateDocument74 pagesThe Febrile Infant 29 To 90 Days of Age Management UpToDateSharafuddin SalimiNo ratings yet
- Serum Procalcitonin Levels in Bacterial and Abacterial MeningitisDocument5 pagesSerum Procalcitonin Levels in Bacterial and Abacterial MeningitisSaul Gonzalez HernandezNo ratings yet
- Meningitis PresentationDocument41 pagesMeningitis PresentationO'Mark AndrewsNo ratings yet
- Bacterial Meningitis in Infants Over 3 Months of AgeDocument8 pagesBacterial Meningitis in Infants Over 3 Months of AgedrirrazabalNo ratings yet
- Newborn Sepsis GuidelineDocument2 pagesNewborn Sepsis GuidelineAmelia ArnisNo ratings yet
- Treatment of Children With COVID-19: Position Paper of The Italian Society of Pediatric Infectious DiseaseDocument17 pagesTreatment of Children With COVID-19: Position Paper of The Italian Society of Pediatric Infectious DiseasecurteanancaNo ratings yet
- Covid Ep IiDocument29 pagesCovid Ep IiLuis Armando López SosaNo ratings yet
- Neonatal InfectionsDocument41 pagesNeonatal Infectionsamid sultanNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in AdultsDocument48 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in AdultsIsmael IbrahimNo ratings yet
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- TREATMENT Bacterial MeningitisDocument32 pagesTREATMENT Bacterial MeningitisironNo ratings yet
- Research Paper On Bacterial MeningitisDocument8 pagesResearch Paper On Bacterial Meningitisvvgnzdbkf100% (1)
- Case 10 Fever PDFDocument5 pagesCase 10 Fever PDFSue HuangNo ratings yet
- Test ID: PCT Procalcitonin, Serum: Useful ForDocument5 pagesTest ID: PCT Procalcitonin, Serum: Useful ForI Nyoman Gede SemarajanaNo ratings yet
- Research Paper Bacterial MeningitisDocument4 pagesResearch Paper Bacterial Meningitisafeebovus100% (1)
- Bacterial Meningitis ThesisDocument8 pagesBacterial Meningitis ThesisRick Vogel100% (2)
- 35-Article Text-212-1-10-20200524Document4 pages35-Article Text-212-1-10-20200524SONIA AGUILAR RIVERANo ratings yet
- Clin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiDocument18 pagesClin Infect Dis. 2004 Tunkel 1267 84 Idsa MeningitiJesus Salvador SerratoNo ratings yet
- Tuberculosis in ChildrenDocument4 pagesTuberculosis in ChildrenMarthin TheservantNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- Sepsis NeonatalDocument21 pagesSepsis NeonatalRaissa 'Icha' Nurwany RizalNo ratings yet
- Diagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyDocument4 pagesDiagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyChoi SpeaksNo ratings yet
- Covid 19 Pediatric Multi System Inflammatory SyndromeDocument2 pagesCovid 19 Pediatric Multi System Inflammatory SyndromeministerenqiNo ratings yet
- Guia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Document18 pagesGuia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Brenda Anali Pariona NapaNo ratings yet
- Neonatal SepsisDocument31 pagesNeonatal Sepsisanwar jabariNo ratings yet
- (Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)Document662 pages(Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)gnkgbjkgjkNo ratings yet
- PCAP ReportDocument28 pagesPCAP ReportAngeline Zamoras-ToledoNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisBhawna PandhuNo ratings yet
- Bacterial MeningitisDocument51 pagesBacterial MeningitiscaseinrenninNo ratings yet
- Bacterial Meningitis in The Neonate - Neurologic Complications - UpToDateDocument9 pagesBacterial Meningitis in The Neonate - Neurologic Complications - UpToDateAngélica PedrazaNo ratings yet
- Meningitis PDFDocument8 pagesMeningitis PDFrizeviNo ratings yet
- Frequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulDocument9 pagesFrequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulNaeem NawazNo ratings yet
- Bacterial MeningitisDocument5 pagesBacterial Meningitisjamesignacio787No ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- MengititisDocument38 pagesMengititisRas Siko SafoNo ratings yet
- Neonatal Meningitis Due To Clostridium Neonatale: A Case ReportDocument4 pagesNeonatal Meningitis Due To Clostridium Neonatale: A Case ReportCarina ColtuneacNo ratings yet
- MMC 1Document9 pagesMMC 1Maulida 04No ratings yet
- Jurnal AsliDocument8 pagesJurnal AsliDwi PurwantiNo ratings yet
- Sepsis in The Newborn - Latest NewsDocument13 pagesSepsis in The Newborn - Latest NewsBrunaNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisLeana SiñelNo ratings yet
- Clinical Features: - Initial Symptoms in Patients With MeningitisDocument12 pagesClinical Features: - Initial Symptoms in Patients With Meningitisyuii_48No ratings yet
- Meningitis in Adults - Diagnosis and Management - Young - 2018 - Internal Medicine Journal - Wiley Online LibraryDocument27 pagesMeningitis in Adults - Diagnosis and Management - Young - 2018 - Internal Medicine Journal - Wiley Online Libraryaslan tonapaNo ratings yet
- Meningitis: By-Dr Nimco A. MDDocument31 pagesMeningitis: By-Dr Nimco A. MDgibreilNo ratings yet
- C V 9 V VV VV V V VVVVVVVV V: "V "V "V "V "VDocument2 pagesC V 9 V VV VV V V VVVVVVVV V: "V "V "V "V "VCharlene Mae CalanoyNo ratings yet
- Paediatrica Indonesiana: Original ArticleDocument5 pagesPaediatrica Indonesiana: Original ArticleSyukron AmrullahNo ratings yet
- Peds InfectiousDocument8 pagesPeds InfectiousMohammad RammalNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- Stroke Differential Diagnosis and Mimics: Part 2Document9 pagesStroke Differential Diagnosis and Mimics: Part 2Natalia E PenagosNo ratings yet
- Seizure Pediatric Scenario June 2016Document4 pagesSeizure Pediatric Scenario June 2016Natalia E PenagosNo ratings yet
- Ene 15103Document8 pagesEne 15103Natalia E PenagosNo ratings yet
- Dom 14270Document19 pagesDom 14270Natalia E PenagosNo ratings yet
- Epilepsy Imaging: Approaches and ProtocolsDocument9 pagesEpilepsy Imaging: Approaches and ProtocolsNatalia E PenagosNo ratings yet
- Peeds Infection LecturesDocument190 pagesPeeds Infection LecturesAli Al.JuffairiNo ratings yet
- 282585293Document208 pages282585293hebaNo ratings yet
- Infections FarazDocument10 pagesInfections FarazM R SIFATNo ratings yet
- Lumbar Puncture ResearchDocument6 pagesLumbar Puncture Researchanon_464104226No ratings yet
- CDDocument6 pagesCDMei JoyNo ratings yet
- اسئلة neuroDocument30 pagesاسئلة neuroSoad RedaNo ratings yet
- Brain AbscessDocument2 pagesBrain AbscessIan RomanNo ratings yet
- Stool Analysis and Other Body Fluid AnalysisDocument51 pagesStool Analysis and Other Body Fluid AnalysisPutri Senna Rahayu100% (2)
- 83K English Class Examination Questions of Infectious DiseaseDocument23 pages83K English Class Examination Questions of Infectious Diseasetarun956519No ratings yet
- Intrathecal Hyaluronidase in TB Meningitis: The Unexplored AdjuvantDocument5 pagesIntrathecal Hyaluronidase in TB Meningitis: The Unexplored AdjuvantPriyanka SamalNo ratings yet
- Idr 240162 Management of Acute Bacterial Meningitis in ChildrenDocument13 pagesIdr 240162 Management of Acute Bacterial Meningitis in ChildrenindahrizkygNo ratings yet
- Epidemiology and Management Og Meningococcal MeningitisDocument12 pagesEpidemiology and Management Og Meningococcal MeningitispriyankaNo ratings yet
- Epidemic Cerebrospinal MeningitisDocument76 pagesEpidemic Cerebrospinal MeningitisAngie LawrenceNo ratings yet
- Some Imp Oneliner From VolumesDocument16 pagesSome Imp Oneliner From VolumesTejas KaleNo ratings yet
- Cases Lab 2020Document16 pagesCases Lab 2020Buushi96No ratings yet
- B) Meningococcal MeningitisDocument7 pagesB) Meningococcal MeningitisWe'am QutubNo ratings yet
- MCQ April 2015Document15 pagesMCQ April 2015Sylphana Astharica LawalataNo ratings yet
- Writing Notes: The Ideal Letter Should Have 6 PartsDocument7 pagesWriting Notes: The Ideal Letter Should Have 6 PartsMMW MNo ratings yet
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDocument7 pagesC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINo ratings yet
- Meningitis ViralDocument7 pagesMeningitis ViralTia Gustiani Poplei ViolaNo ratings yet
- Communicable Disease ChartDocument5 pagesCommunicable Disease ChartAuspice QatarNo ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- Abdullahi V Pfizer Inc PDFDocument44 pagesAbdullahi V Pfizer Inc PDFBevs DomingoNo ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
- Blog Post About National Poultry Day 2023Document63 pagesBlog Post About National Poultry Day 2023ZETTYNo ratings yet
- Date/Time Doctors Order RationaleDocument4 pagesDate/Time Doctors Order RationaleChamCham AquinoNo ratings yet
- HAAD Test 4 QuestionsDocument17 pagesHAAD Test 4 QuestionsPhine PhineNo ratings yet