Download as pdf or txt
You might also like
- Patient Admission FormDocument2 pagesPatient Admission Formelmore kakaNo ratings yet
- Penetration Testing Step-By-Step GuideDocument417 pagesPenetration Testing Step-By-Step GuideДенис Пискайкин100% (3)
- Form - Bupa Claim FormDocument2 pagesForm - Bupa Claim FormJoe Sayavongsa100% (3)
- Build A Small NetworkDocument58 pagesBuild A Small Networkthanh vienNo ratings yet
- Bupa Global Claim Form: 1 Patient'S DetailsDocument4 pagesBupa Global Claim Form: 1 Patient'S Details123owenNo ratings yet
- AXA PPP Claim Form PDFDocument2 pagesAXA PPP Claim Form PDFEleftheria AggeleaNo ratings yet
- Laya Claim FormDocument2 pagesLaya Claim FormManolo0% (1)
- Claim Form Regency For Expats PDFDocument2 pagesClaim Form Regency For Expats PDFChris DarkNo ratings yet
- WiresharkDocument8 pagesWiresharkLakshay MathurNo ratings yet
- UVMF One Bite at A Time: UVM Framework OverviewDocument22 pagesUVMF One Bite at A Time: UVM Framework OverviewmanchuricoNo ratings yet
- Claim Form: 1 Patient's DetailsDocument7 pagesClaim Form: 1 Patient's DetailsEduskill Learning CentreNo ratings yet
- BAH Bupa Global Claim Form EN APR21 0027975Document8 pagesBAH Bupa Global Claim Form EN APR21 0027975ALJABERNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Bupa Global Claim FormDocument8 pagesBupa Global Claim FormALJABERNo ratings yet
- Bupa International Claim Form: 1 Patient'S DetailsDocument4 pagesBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNo ratings yet
- BIN Claim Form 1611v11 D PDFDocument5 pagesBIN Claim Form 1611v11 D PDFAnonymous BZF0QIjDNo ratings yet
- Claim Form: Patient's Details - To Be Completed by The Person Undergoing TreatmentDocument4 pagesClaim Form: Patient's Details - To Be Completed by The Person Undergoing Treatmentpier_roNo ratings yet
- Axa Claim FormDocument2 pagesAxa Claim FormReem Mohamed El BarraniNo ratings yet
- Claim Form en Nov 08Document4 pagesClaim Form en Nov 08Juju FernsNo ratings yet
- Bupa Global Reimbursement FormDocument5 pagesBupa Global Reimbursement Formshena0% (1)
- BUPA Intl Claim Form PDFDocument4 pagesBUPA Intl Claim Form PDFisabellashNo ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- CLAIM FORM Maternity MEAF RSA 69041 3Document5 pagesCLAIM FORM Maternity MEAF RSA 69041 3Arindam ChangdarNo ratings yet
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Inter Global Claim Form 2010Document4 pagesInter Global Claim Form 2010ywa00No ratings yet
- JFR Claim Form Leonardo PreenchidoDocument3 pagesJFR Claim Form Leonardo PreenchidoNatália André RodriguesNo ratings yet
- NOW HEALTH Claim - Form - Uae - RsaDocument2 pagesNOW HEALTH Claim - Form - Uae - RsaWilliam IsaacNo ratings yet
- Axa Reimbursement Claim Form 01Document2 pagesAxa Reimbursement Claim Form 01Tarak FakhfakhNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- Test AxaDocument2 pagesTest AxaElmedina Berin HalilovićNo ratings yet
- Put Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsDocument3 pagesPut Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsTHÍCH XEM XENo ratings yet
- Disability Claim Form v3Document7 pagesDisability Claim Form v3arekp28978No ratings yet
- Reg 2-Primary Care Claim Form-31 Oct 2008Document2 pagesReg 2-Primary Care Claim Form-31 Oct 2008Pradeep KhubchandaniNo ratings yet
- AETNADocument5 pagesAETNATRTNo ratings yet
- Modulo Di Rimborso Spese Mediche ClaimForm-EnglishDocument2 pagesModulo Di Rimborso Spese Mediche ClaimForm-EnglishCarlo_Sturlese_4203No ratings yet
- Chola Health Claim FormDocument2 pagesChola Health Claim FormBalaji_Rajaman_2280No ratings yet
- BCBSTX Halliburton Intl Claim FormDocument2 pagesBCBSTX Halliburton Intl Claim FormLoganBohannonNo ratings yet
- SG Worldcare Pre AuthorisationDocument3 pagesSG Worldcare Pre Authorisationbernardlim86No ratings yet
- WISE CF W - Instructions 120216Document4 pagesWISE CF W - Instructions 120216Jotaro KujooNo ratings yet
- Subject Access Revised Application Form 26032018Document6 pagesSubject Access Revised Application Form 26032018Lynn Ross WardNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Claim Form: DD MM YY DD MM YYDocument3 pagesClaim Form: DD MM YY DD MM YYAnonymous SM6kY6tB1sNo ratings yet
- Medical Claim FormDocument1 pageMedical Claim FormAkash SrivastavaNo ratings yet
- ICICI Lombard Health Care Claim Form - Outpatient DepartmentDocument2 pagesICICI Lombard Health Care Claim Form - Outpatient Departmentanon_103901460No ratings yet
- Chubb14-345-1122 Uber Personal Injury Claim Form-INTDocument7 pagesChubb14-345-1122 Uber Personal Injury Claim Form-INTEidrian RicardoNo ratings yet
- Claim FormDocument3 pagesClaim FormInvestor ProtegeNo ratings yet
- Laya ClaimDocument2 pagesLaya ClaimManoloNo ratings yet
- BMS Patient Assistance FoundationDocument4 pagesBMS Patient Assistance FoundationJhoanna MonterolaNo ratings yet
- OPD Form IHealthcare-2Document2 pagesOPD Form IHealthcare-2Masoom Kazmi100% (1)
- Application For Membership Form: Application No.: Effectivity Date: Contract No.Document2 pagesApplication For Membership Form: Application No.: Effectivity Date: Contract No.Lizeth QuerubinNo ratings yet
- Medical Billing Process: Naveen MajetyDocument21 pagesMedical Billing Process: Naveen MajetyNaveen KumarNo ratings yet
- ReimbursementDocument2 pagesReimbursementFAZILNo ratings yet
- MET - Medical Claim Reimbursement Form in Patient - KWTDocument2 pagesMET - Medical Claim Reimbursement Form in Patient - KWTangeloriondo1217No ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- Ap Chief Minister'S Relief FundDocument6 pagesAp Chief Minister'S Relief Fundiqbal1439988100% (1)
- Claim Form: (For Reimbursement of Expenses)Document4 pagesClaim Form: (For Reimbursement of Expenses)Shankar NathNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- What Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyFrom EverandWhat Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (2)
- Preboard 3 Math STD AK 2023-24Document11 pagesPreboard 3 Math STD AK 2023-24R.Pearlsis SophiNo ratings yet
- What Is AND ?: SupplyDocument15 pagesWhat Is AND ?: SupplyR.Pearlsis SophiNo ratings yet
- E Catalgoue Make Way For The Brides of IndiaDocument61 pagesE Catalgoue Make Way For The Brides of IndiaR.Pearlsis SophiNo ratings yet
- Lakhmir Singh Chemistry Class 9 Solutions Chapter 3Document24 pagesLakhmir Singh Chemistry Class 9 Solutions Chapter 3R.Pearlsis SophiNo ratings yet
- Simply FRENCH CoursesDocument6 pagesSimply FRENCH CoursesR.Pearlsis SophiNo ratings yet
- Simply FRENCH-Terms and ConditionsDocument1 pageSimply FRENCH-Terms and ConditionsR.Pearlsis SophiNo ratings yet
- English WorkBook - 2022 IXDocument176 pagesEnglish WorkBook - 2022 IXR.Pearlsis SophiNo ratings yet
- Academic Window 2021Document29 pagesAcademic Window 2021R.Pearlsis SophiNo ratings yet
- English Literature - 2022 IXDocument166 pagesEnglish Literature - 2022 IXR.Pearlsis SophiNo ratings yet
- NCERT Exemplar Class 8 Maths Solutions Chapter 6 Visualising Solid ShapesDocument11 pagesNCERT Exemplar Class 8 Maths Solutions Chapter 6 Visualising Solid ShapesR.Pearlsis SophiNo ratings yet
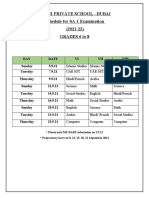
- Sa1 Schedule 2021 22Document1 pageSa1 Schedule 2021 22R.Pearlsis SophiNo ratings yet
- Report of F - CH Maribel Snigitha CiceroDocument2 pagesReport of F - CH Maribel Snigitha CiceroR.Pearlsis SophiNo ratings yet
- Fractions On Number Line and Equivalent Fractions WORKSHEET GRADE3Document5 pagesFractions On Number Line and Equivalent Fractions WORKSHEET GRADE3R.Pearlsis SophiNo ratings yet
- Design and Study On The State of Charge Estimation For Lithium-Ion Battery Pack in Electric VehicleDocument5 pagesDesign and Study On The State of Charge Estimation For Lithium-Ion Battery Pack in Electric VehiclekhasimNo ratings yet
- Types of WallsDocument3 pagesTypes of Wallsrowell naragNo ratings yet
- Global Positioning System Surveying PDFDocument328 pagesGlobal Positioning System Surveying PDFIlie RomeoNo ratings yet
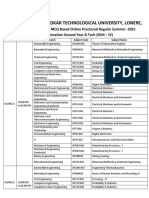
- Revised 4th Sem Time Table - FDocument5 pagesRevised 4th Sem Time Table - FJerry boyNo ratings yet
- Guidebook Hope PDFDocument34 pagesGuidebook Hope PDFDr MukeshNo ratings yet
- Cyl. Head Unit No. 6 PmeDocument5 pagesCyl. Head Unit No. 6 PmeMuhammad IshfaqNo ratings yet
- STE02 Product Sheet 1Document1 pageSTE02 Product Sheet 1AZMAN ZHNo ratings yet
- ME Lab 1 Exp 7 Bomb CalorimeterDocument18 pagesME Lab 1 Exp 7 Bomb CalorimeterJAMAL HALIBAYNo ratings yet
- IEC Contactor Specifications: Technical DataDocument114 pagesIEC Contactor Specifications: Technical DataFrancisco AyalaNo ratings yet
- Logical ReasoningDocument2 pagesLogical ReasoningAbhyudaya ShettyNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesJhon Cortez100% (1)
- MB05F MB10F: FeaturesDocument2 pagesMB05F MB10F: FeaturesCarlos AgudeloNo ratings yet
- GAA30328BAA Dcss5 Service Tool Reference List PDFDocument19 pagesGAA30328BAA Dcss5 Service Tool Reference List PDFTaufik Hidayat KurniansyahNo ratings yet
- Iphone Launch 2007 - Steve JobsDocument30 pagesIphone Launch 2007 - Steve JobsMANALI KHANDELWALNo ratings yet
- Searching Resources and Links: Director FilmDocument4 pagesSearching Resources and Links: Director FilmNAKIPEHKSNo ratings yet
- Tunnel Engineering-1Document26 pagesTunnel Engineering-1Ankit PatelNo ratings yet
- Aacm Standard DrawingsDocument7 pagesAacm Standard Drawingshussein247No ratings yet
- AWS Solutions Architect Associate Master Cheat SheetDocument124 pagesAWS Solutions Architect Associate Master Cheat SheetSapna Popat SitarNo ratings yet
- Mumbai Metro Rail Corporation (Contract Ref: Mm3-Cbs-Tve-P1) Daily Progress ReportDocument7 pagesMumbai Metro Rail Corporation (Contract Ref: Mm3-Cbs-Tve-P1) Daily Progress ReportSaurabh DwivediNo ratings yet
- Magnum DS Switchgear Common Replacement PartsDocument4 pagesMagnum DS Switchgear Common Replacement PartsCesar Santiago Marquez Yanez0% (1)
- Virtual FridgeDocument2 pagesVirtual FridgeKrishnanshu KhilareNo ratings yet
- Introduction To: Information RetrievalDocument64 pagesIntroduction To: Information RetrievalTayyaba FaisalNo ratings yet
- Watertube Boilers HaveDocument175 pagesWatertube Boilers Havenathaniel villanueva100% (1)
- Telecom Service Provider RFQDocument4 pagesTelecom Service Provider RFQKatia HasanNo ratings yet
- Tech. Data Showroom: Home ProductsDocument2 pagesTech. Data Showroom: Home ProductsSantiago ReinoNo ratings yet
- Notes On ECON3032: X Y U (XDocument2 pagesNotes On ECON3032: X Y U (XSA Smith AinaNo ratings yet