Download as pdf or txt
You might also like
- 2007 National Spec For Cleanliness in The NHSDocument52 pages2007 National Spec For Cleanliness in The NHSdranukapoorNo ratings yet
- El Chico de La Ultima Fila - Juan MayorgaDocument72 pagesEl Chico de La Ultima Fila - Juan MayorgaCésar LópezNo ratings yet
- Simplifying The World Health Organization Protocol 3 Steps Versus 6 Steps For Performance of Hand Hygiene in A Cluster-Randomized TrialDocument7 pagesSimplifying The World Health Organization Protocol 3 Steps Versus 6 Steps For Performance of Hand Hygiene in A Cluster-Randomized TrialManuel GuzmanNo ratings yet
- Predictors of Hand Hygiene Compliance in The Era of Alcohol-Based Hand RinseDocument8 pagesPredictors of Hand Hygiene Compliance in The Era of Alcohol-Based Hand RinseI Komang BudianaNo ratings yet
- Trsa WhitepaperDocument8 pagesTrsa Whitepapersinggih100% (1)
- 10 ArticlesDocument6 pages10 ArticlesTimilehin OgundareNo ratings yet
- Objectives:: Applying HACCP and GMP in Food Preservation ProcessesDocument8 pagesObjectives:: Applying HACCP and GMP in Food Preservation Processesomelkhair amenNo ratings yet
- 2017 Article 410Document16 pages2017 Article 410Andrew SebastianNo ratings yet
- HH Report WhoDocument15 pagesHH Report WhoBernadetta IndahNo ratings yet
- Ipc CC MisDocument1 pageIpc CC MisLorena HernandezNo ratings yet
- 9.ijerph 16 01067 PDFDocument10 pages9.ijerph 16 01067 PDFfaizan dawoodNo ratings yet
- The Principles of Good Manual The Principles of Good Manual Handling: Achieving A Consensus Handling: Achieving A ConsensusDocument121 pagesThe Principles of Good Manual The Principles of Good Manual Handling: Achieving A Consensus Handling: Achieving A ConsensusM-di El-riNo ratings yet
- Audit HH Australia PDFDocument63 pagesAudit HH Australia PDFppiNo ratings yet
- Using Effective Hand Hygiene Practice To Prevent and Control InfectionDocument6 pagesUsing Effective Hand Hygiene Practice To Prevent and Control InfectionerikNo ratings yet
- Hand Hygiene Compliance in Healthcare WorkersDocument6 pagesHand Hygiene Compliance in Healthcare WorkersRiska IndrianiNo ratings yet
- Hand Hygiene - Framework PDFDocument9 pagesHand Hygiene - Framework PDFFhirastika AnnishaNo ratings yet
- IPAC Standards 2021Document32 pagesIPAC Standards 2021Abdur Rashid KhanNo ratings yet
- Research Liquid Versus Gel Handrub Formulation A PDocument9 pagesResearch Liquid Versus Gel Handrub Formulation A PJavier Vadillo PardoNo ratings yet
- Bestpracticesinenvironmentalmonitoring RSSLpaperDocument22 pagesBestpracticesinenvironmentalmonitoring RSSLpapergombasgNo ratings yet
- Un Analisis Preliminar de La Aplicacion de Lean Six Sigma en Un Entorno de SaludDocument4 pagesUn Analisis Preliminar de La Aplicacion de Lean Six Sigma en Un Entorno de SaludGabriela AuquiNo ratings yet
- Using Effective Hand Hygiene Practice To Prevent and Control InfectionDocument6 pagesUsing Effective Hand Hygiene Practice To Prevent and Control Infectionfarida nur ainiNo ratings yet
- New Approaches in Assessing Food Intake in Epidemiology: ReviewDocument9 pagesNew Approaches in Assessing Food Intake in Epidemiology: ReviewMaría Camila Ferreira ZambranoNo ratings yet
- Fall 2013 Nurs 440 Lsa - Final DraftDocument11 pagesFall 2013 Nurs 440 Lsa - Final Draftapi-246946466No ratings yet
- Action Plan ExampleDocument6 pagesAction Plan ExampleAshmal DanielNo ratings yet
- Jnu.12274 Sistematik ReviewDocument10 pagesJnu.12274 Sistematik ReviewMastifa HanasitaNo ratings yet
- Audit of Hand HygieneDocument16 pagesAudit of Hand Hygienesmitha mohanNo ratings yet
- Pittet, 2003Document9 pagesPittet, 2003Rusida LiyaniNo ratings yet
- Jaaos D 17 00030Document7 pagesJaaos D 17 00030Mohammed FaisalNo ratings yet
- CDC - Employing Continuous Quality Improvement in Community-Based Substance Abuse ProgramsDocument15 pagesCDC - Employing Continuous Quality Improvement in Community-Based Substance Abuse ProgramsraadNo ratings yet
- Impact of A Comprehensive Workplace Hand Hygiene.25Document10 pagesImpact of A Comprehensive Workplace Hand Hygiene.25Keperawatan s1aNo ratings yet
- Hand Hygiene For All Initiative: Improving Access and Behaviour in Health Care FacilitiesDocument16 pagesHand Hygiene For All Initiative: Improving Access and Behaviour in Health Care FacilitiesMai BasionyNo ratings yet
- IC Risk Assessment & Plan (Modified)Document9 pagesIC Risk Assessment & Plan (Modified)Soha GalalNo ratings yet
- Benchmarking: A Method For Continuous Quality Improvement in HealthDocument19 pagesBenchmarking: A Method For Continuous Quality Improvement in HealthslagmercuryNo ratings yet
- Hand Hygiene Jakarta 2016 - Patricia ChingDocument72 pagesHand Hygiene Jakarta 2016 - Patricia ChingAndre KartawidjajaNo ratings yet
- 2019 Hand HygieneDocument3 pages2019 Hand HygieneRONAL YESID MONTAÑO BALLESTEROSNo ratings yet
- NHSX AI ReportDocument55 pagesNHSX AI ReporthasanveletanlicNo ratings yet
- Artículo Posible 3Document12 pagesArtículo Posible 3Jarod NavarreteNo ratings yet
- Protocol For A Mixed-Methods Realist Evaluation of A Health Service User Feedback System in BangladeshDocument8 pagesProtocol For A Mixed-Methods Realist Evaluation of A Health Service User Feedback System in BangladeshChandra Hidayat RcrNo ratings yet
- Mas YAF (1) TranslationDocument8 pagesMas YAF (1) Translationsaladass 2No ratings yet
- Do Smartphone Applications and Activity Trackers Increase Physical Activity in Adults? Systematic Review, Meta-Analysis and MetaregressionDocument13 pagesDo Smartphone Applications and Activity Trackers Increase Physical Activity in Adults? Systematic Review, Meta-Analysis and Metaregressionkarla danielaNo ratings yet
- Reading CSTIDocument6 pagesReading CSTISudhanshu ShekharNo ratings yet
- Assemble: Haccp TeamDocument22 pagesAssemble: Haccp Teamمركز ريادرون للتدريبNo ratings yet
- Life Cycle Approach To Cleaning Validation - International Journal of Pharmaceutical Sciences and ResearchDocument11 pagesLife Cycle Approach To Cleaning Validation - International Journal of Pharmaceutical Sciences and ResearchMuhammad AsifNo ratings yet
- COCU 1 NEW (SAFETY, HEALTH AND HYGIENE PRACTISE) - L2 NewDocument11 pagesCOCU 1 NEW (SAFETY, HEALTH AND HYGIENE PRACTISE) - L2 NewRoslailiAbdullahNo ratings yet
- Analysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareDocument4 pagesAnalysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareGuillermo Luis AcostaNo ratings yet
- 2019 Lean Six Sigma in HealthcareDocument3 pages2019 Lean Six Sigma in HealthcareCarlos Valdivia Seminario0% (1)
- HACCP - Step 10 - Principle 5 Corrective ActionsDocument21 pagesHACCP - Step 10 - Principle 5 Corrective ActionsTran Duy ThaNo ratings yet
- 196-1584526128 LeanhospitalDocument8 pages196-1584526128 LeanhospitalDharm Veer RathoreNo ratings yet
- Liquid Versus Gel Handrub Formulation: A Prospective Intervention StudyDocument8 pagesLiquid Versus Gel Handrub Formulation: A Prospective Intervention Studydebby claudiNo ratings yet
- 14th European Public Health Conference 2021Document1 page14th European Public Health Conference 2021Sajib Chandra RoyNo ratings yet
- Bio Medical Waste Management Manual For: ALL India Institute OF Medical Sciences NEW DelhiDocument56 pagesBio Medical Waste Management Manual For: ALL India Institute OF Medical Sciences NEW DelhiiddrxNo ratings yet
- Adherence To Hand Hygiene Guidelines - Significance of Measuring FidelityDocument9 pagesAdherence To Hand Hygiene Guidelines - Significance of Measuring FidelityiindahlubisNo ratings yet
- Article Improved Standards PracticeDocument9 pagesArticle Improved Standards PracticeswnhruNo ratings yet
- S O P (SOP) : The Most Up-To-Date Version of This SOP Can Be Viewed at The Following WebsiteDocument17 pagesS O P (SOP) : The Most Up-To-Date Version of This SOP Can Be Viewed at The Following WebsiteJetrin PriskilaNo ratings yet
- HH Monograph PDFDocument234 pagesHH Monograph PDFAnonymous WmArPQl3BNo ratings yet
- 2009 JHI Methodstoevaluate RotterDocument10 pages2009 JHI Methodstoevaluate RotterAzizah Alya RaihanNo ratings yet
- Cleaning and disinfection of food factories: a practical guideFrom EverandCleaning and disinfection of food factories: a practical guideNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Xie 2017Document10 pagesXie 2017César LópezNo ratings yet
- Preprint 20961 SubmittedDocument21 pagesPreprint 20961 SubmittedCésar LópezNo ratings yet
- A Am340eDocument19 pagesA Am340eCésar LópezNo ratings yet
- Contraception and Reproductive Planning During The COVID 19 PandemicDocument9 pagesContraception and Reproductive Planning During The COVID 19 PandemicCésar LópezNo ratings yet
- AIDS Care: Psychological and Socio-Medical Aspects of Aids/HivDocument10 pagesAIDS Care: Psychological and Socio-Medical Aspects of Aids/HivCésar LópezNo ratings yet
- Cox TVC PDFDocument2 pagesCox TVC PDFCésar LópezNo ratings yet
- Title: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruDocument20 pagesTitle: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruCésar LópezNo ratings yet
- EPDS Eng Span PDFDocument2 pagesEPDS Eng Span PDFCésar LópezNo ratings yet
- Concepts and Principles PDFDocument45 pagesConcepts and Principles PDFCésar LópezNo ratings yet
- Lec11 PDFDocument12 pagesLec11 PDFCésar LópezNo ratings yet
- Preventing Hepatitis B Virus Infection: Milestones and TargetsDocument2 pagesPreventing Hepatitis B Virus Infection: Milestones and TargetsCésar LópezNo ratings yet
- Brochure Promoting HealthDocument24 pagesBrochure Promoting HealthCésar LópezNo ratings yet
- Death Rate Variation in US Subpopulations: David A. Kindig, Christopher L. Seplaki, & Donald L. LibbyDocument7 pagesDeath Rate Variation in US Subpopulations: David A. Kindig, Christopher L. Seplaki, & Donald L. LibbyCésar LópezNo ratings yet
- CIOMS GuidelinesDocument113 pagesCIOMS GuidelinesCésar LópezNo ratings yet
- Health Equity Indicator CompendiumDocument35 pagesHealth Equity Indicator CompendiumCésar LópezNo ratings yet
- Ema StudyDocument10 pagesEma StudyCésar LópezNo ratings yet
- Vitex Negundo PDFDocument14 pagesVitex Negundo PDFamyNo ratings yet
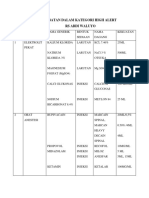
- Obat High AlertDocument5 pagesObat High AlertChia GracellaNo ratings yet
- Code Medicine Name Pack Selling Price GST MRP: AyurvedaDocument25 pagesCode Medicine Name Pack Selling Price GST MRP: Ayurvedaprabha karanNo ratings yet
- Lahore Lab: Web ReportDocument1 pageLahore Lab: Web Reportkhurram shahzadNo ratings yet
- Canna Green CBD Gummies Official) - 100% LegitimateDocument2 pagesCanna Green CBD Gummies Official) - 100% LegitimateEstellen IevkesNo ratings yet
- Immunology Report U119605: Id NoDocument1 pageImmunology Report U119605: Id Nohrashel29No ratings yet
- Clinical Trials 101 & Clinical Trial Participation: Webinar For The Canadian Cancer Survivor NetworkDocument22 pagesClinical Trials 101 & Clinical Trial Participation: Webinar For The Canadian Cancer Survivor NetworkvigneshwebNo ratings yet
- Q, S, U, V, W, X, Y, Z Januari 2021Document10 pagesQ, S, U, V, W, X, Y, Z Januari 2021Mutmainnah PeaceNo ratings yet
- Katz Index Functional Sindrom DownDocument2 pagesKatz Index Functional Sindrom DownAndrei TîrziuNo ratings yet
- AD - Daftar Produk - 27 Mei 2021Document11 pagesAD - Daftar Produk - 27 Mei 2021adhimaswicaksono1991No ratings yet
- Surgical Approaches in OtorhinolaryngologyDocument381 pagesSurgical Approaches in OtorhinolaryngologyAlice TimbNo ratings yet
- Karl C. Ablola, M.D. Karl C. Ablola, M.D.: PTR: - S2 LicenseDocument2 pagesKarl C. Ablola, M.D. Karl C. Ablola, M.D.: PTR: - S2 LicenseGabrielAblolaNo ratings yet
- NCISM - II BAMS - AyUG-RBDocument118 pagesNCISM - II BAMS - AyUG-RBTejas SinghNo ratings yet
- Tight Glycemic Control in Critically Ill PediatricDocument11 pagesTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNo ratings yet
- MRTD Form School Children MasterlistDocument16 pagesMRTD Form School Children MasterlistJenRomarateCervantesNo ratings yet
- ARTIKEL MUAMMAR CCDocument10 pagesARTIKEL MUAMMAR CCJaini SuryanaNo ratings yet
- Posology Chart-1Document2 pagesPosology Chart-1Abhishek VaghelaNo ratings yet
- Product List Ekatalog 2021 FPH With E-Catalogue Code - Rev 09092021Document42 pagesProduct List Ekatalog 2021 FPH With E-Catalogue Code - Rev 09092021arif santanaNo ratings yet
- Pediatric Orthopedic Trauma Case Atlas 2020Document803 pagesPediatric Orthopedic Trauma Case Atlas 2020Aurel Mironescu100% (1)
- Barriers To Uptake of Community-Based ProgramsDocument12 pagesBarriers To Uptake of Community-Based ProgramsAmin JemalNo ratings yet
- Code of Ethics For PharmacistsDocument3 pagesCode of Ethics For PharmacistsAmina Abba HaliruNo ratings yet
- STORZ ENDOSKOPE Flexible Intubation Video Endoscope 11302BDX Instruction ManualDocument64 pagesSTORZ ENDOSKOPE Flexible Intubation Video Endoscope 11302BDX Instruction Manualmetech8xNo ratings yet
- Equipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterDocument2 pagesEquipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterIan TuNo ratings yet
- Hfo The Complete Symposium 2Document4 pagesHfo The Complete Symposium 2SabNo ratings yet
- Immobilization of Kodkod (Leopardus Guigna) With Ketamine Hydrochloride and Xylazine HydrochlorideDocument6 pagesImmobilization of Kodkod (Leopardus Guigna) With Ketamine Hydrochloride and Xylazine HydrochlorideJacky SierasNo ratings yet
- Handbook of Ophthalmology - Amar Agarwal - 159Document5 pagesHandbook of Ophthalmology - Amar Agarwal - 159Danielle SangalangNo ratings yet
- Book 2Document22 pagesBook 2Vijay LandageNo ratings yet
- Jurnal Sains Dan KesehatanDocument14 pagesJurnal Sains Dan KesehatanTrhee Ya NovhaNo ratings yet
- Documentation in Your 3 Year and Beyond: Summer Quarter 2010Document32 pagesDocumentation in Your 3 Year and Beyond: Summer Quarter 2010Roberto ParedesNo ratings yet
- 301.885.000 02 en Bellavista Product Catalog WebDocument54 pages301.885.000 02 en Bellavista Product Catalog WebJossue LopezNo ratings yet