Download as pdf or txt
You might also like
- Chapter 8 ACCA F2Document9 pagesChapter 8 ACCA F2sikshaNo ratings yet
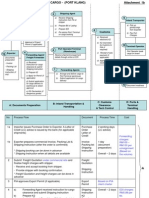
- Export + Import Process Flow - Break Bulk Cargo 27072010Document11 pagesExport + Import Process Flow - Break Bulk Cargo 27072010Ahmad Fauzi Mehat100% (1)
- Epilepsy PredDocument4 pagesEpilepsy PredDhanalekshmi YedurkarNo ratings yet
- The Application of Voxel Based Morphometery (VBM) On MRI in Temporal Lobe Epilepsy (TLE) PatientsDocument11 pagesThe Application of Voxel Based Morphometery (VBM) On MRI in Temporal Lobe Epilepsy (TLE) PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Epilepsy Pred 3Document4 pagesEpilepsy Pred 3Dhanalekshmi YedurkarNo ratings yet
- Epileptic Siezure Onset Detection Based On EEG and ECG Data FusionDocument13 pagesEpileptic Siezure Onset Detection Based On EEG and ECG Data FusionSana UllahNo ratings yet
- Sizures CNNDocument13 pagesSizures CNNSamuel CardosoNo ratings yet
- Clinical NeurophysiologyDocument32 pagesClinical NeurophysiologyPIERRELEENo ratings yet
- 356 FullDocument15 pages356 FullLeonel Ivan AngelesNo ratings yet
- A Multi-Channel Approach For Cortical Stimulation Artefact Suppression in Depth EEG Signals Using Time-Frequency and Spatial FilteringDocument12 pagesA Multi-Channel Approach For Cortical Stimulation Artefact Suppression in Depth EEG Signals Using Time-Frequency and Spatial FilteringmuraliNo ratings yet
- Lossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoDocument6 pagesLossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoOsamaNo ratings yet
- Lossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoDocument6 pagesLossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoOsamaNo ratings yet
- Deep RNN Learning For EEG Based Functional Brain State InferenceDocument6 pagesDeep RNN Learning For EEG Based Functional Brain State InferenceSuprava PatnaikNo ratings yet
- Neuroimage: Justin Ales, Thom Carney, Stanley A. KleinDocument9 pagesNeuroimage: Justin Ales, Thom Carney, Stanley A. KleinnikadonNo ratings yet
- World University of Bangladesh: Report On Radiography of The Brain (EEG)Document10 pagesWorld University of Bangladesh: Report On Radiography of The Brain (EEG)EmonNo ratings yet
- Paper 6Document7 pagesPaper 6Sweena MaryNo ratings yet
- Penelitian 1Document10 pagesPenelitian 1dietapNo ratings yet
- TMP 4 FB0Document11 pagesTMP 4 FB0FrontiersNo ratings yet
- Rapid Communication With ADocument16 pagesRapid Communication With A123No ratings yet
- Fneur 10 00094Document19 pagesFneur 10 00094JOHAN FELIPE NAVIA PIZONo ratings yet
- Combined Eeg and Mri Studies of Human Brain Function: V. Menon and S. Crottaz-HerbetteDocument31 pagesCombined Eeg and Mri Studies of Human Brain Function: V. Menon and S. Crottaz-HerbetteShalini VijayNo ratings yet
- Millisecond by Millisecond, Year by Year: Normative EEG Microstates and Developmental StagesDocument5 pagesMillisecond by Millisecond, Year by Year: Normative EEG Microstates and Developmental Stagesscribd.com@jperla.comNo ratings yet
- Deep C-LSTM Neural Network For Epileptic Seizure and Tumor Detection Using High-Dimension EEG SignalsDocument10 pagesDeep C-LSTM Neural Network For Epileptic Seizure and Tumor Detection Using High-Dimension EEG Signalsneeshu kumariNo ratings yet
- a robust unsupervised epileptic seizuresDocument11 pagesa robust unsupervised epileptic seizuresemin.ipek42No ratings yet
- Analysis of Spectral Features of EEG Signal in Bra PDFDocument7 pagesAnalysis of Spectral Features of EEG Signal in Bra PDFArturo GuzmanNo ratings yet
- Tugas Keperwatan Dasar Kelompok 3Document54 pagesTugas Keperwatan Dasar Kelompok 3Tolak HarisNo ratings yet
- Epilepsia - 2023 - Travnicek - Relative Entropy Is An Easy To Use Invasive Electroencephalographic Biomarker of TheDocument11 pagesEpilepsia - 2023 - Travnicek - Relative Entropy Is An Easy To Use Invasive Electroencephalographic Biomarker of TheJOHAN FELIPE NAVIA PIZONo ratings yet
- Artigo Hipotalamo1Document14 pagesArtigo Hipotalamo1hercules marceloNo ratings yet
- EEG - Feature ExtractionDocument5 pagesEEG - Feature Extractiondumperacct123No ratings yet
- Epilepsy Pred 4Document7 pagesEpilepsy Pred 4Dhanalekshmi YedurkarNo ratings yet
- Ausencias MeegDocument10 pagesAusencias MeegBg FloresNo ratings yet
- 2 Performance analysis of EEG seizure detection featuresDocument8 pages2 Performance analysis of EEG seizure detection featuresemin.ipek42No ratings yet
- Nice To KnowDocument8 pagesNice To KnowEs JerukNo ratings yet
- Locating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised LearningDocument10 pagesLocating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised Learning施展No ratings yet
- Cognitive State Signature Analyses Using Single Channel EEG DataDocument5 pagesCognitive State Signature Analyses Using Single Channel EEG Datahelenzhang888No ratings yet
- Compressive Wideband Power Spectrum Analysis For Eeg Signals Using Fastica and Neural NetworkDocument7 pagesCompressive Wideband Power Spectrum Analysis For Eeg Signals Using Fastica and Neural NetworkInternational Organization of Scientific Research (IOSR)No ratings yet
- Flanagan Et Al 2014 EEG-fMRI Focal Epilepsy - Local Activation and Regional NetworksDocument11 pagesFlanagan Et Al 2014 EEG-fMRI Focal Epilepsy - Local Activation and Regional NetworksCindy ZuritaNo ratings yet
- Johnson 2020 J. Neural Eng. 17 051001Document28 pagesJohnson 2020 J. Neural Eng. 17 051001Nery BorgesNo ratings yet
- BECT Spike Detection Based On Novel EEG Sequence Features and LSTM AlgorithmsDocument10 pagesBECT Spike Detection Based On Novel EEG Sequence Features and LSTM AlgorithmsatewogboNo ratings yet
- The Classification of EEG-based Winking Signals: A Transfer Learning and Random Forest ApproachDocument7 pagesThe Classification of EEG-based Winking Signals: A Transfer Learning and Random Forest ApproachDhruv TNo ratings yet
- Intraoperative NeuromonitoringDocument15 pagesIntraoperative NeuromonitoringCarolina Aguilar OtáloraNo ratings yet
- Power Spectral Analysis of Eeg As A Potential Marker in The Diagnosis of Spastic Cerebral Palsy CasesDocument7 pagesPower Spectral Analysis of Eeg As A Potential Marker in The Diagnosis of Spastic Cerebral Palsy CasesAnonymous UXBSV13c100% (1)
- Selection of Abnormal Neural Oscillation Patterns Associated With Sentence-Level Language Disorder in SchizophreniaDocument4 pagesSelection of Abnormal Neural Oscillation Patterns Associated With Sentence-Level Language Disorder in Schizophreniamarej312No ratings yet
- The Combination of EEG Source Imaging and EEG-correlated Functional MRI To Map Epileptic NetworksDocument15 pagesThe Combination of EEG Source Imaging and EEG-correlated Functional MRI To Map Epileptic NetworksDiogo SarmentoNo ratings yet
- 1 s2.0 S105381192200221X MainDocument13 pages1 s2.0 S105381192200221X MainLuís PachecoNo ratings yet
- Berard 2021Document6 pagesBerard 2021oswalt.dnNo ratings yet
- Brain Computer Interface DocumentationDocument20 pagesBrain Computer Interface DocumentationCharipally Dhanush RahulNo ratings yet
- EEGSurveyDocument19 pagesEEGSurveyGeo MeNo ratings yet
- A Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG SignalsDocument10 pagesA Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG SignalsDhanalekshmi YedurkarNo ratings yet
- Automatic Detection of Seizure ONSET in Pediatric EEGDocument9 pagesAutomatic Detection of Seizure ONSET in Pediatric EEGijesajournalNo ratings yet
- Lec 4Document24 pagesLec 4Mustafa KamelNo ratings yet
- 2021 - Functional Brain-Heart Interplay Extends To The Multifractal DomainDocument16 pages2021 - Functional Brain-Heart Interplay Extends To The Multifractal DomainVeronica JanethNo ratings yet
- J NBD 2021 105372Document10 pagesJ NBD 2021 105372bobNo ratings yet
- Review of Significant Research On EEG Based Automated Detection of Epilepsy Seizures Brain TumorDocument9 pagesReview of Significant Research On EEG Based Automated Detection of Epilepsy Seizures Brain TumorSachin GuptaNo ratings yet
- Brainsci 11 01525Document44 pagesBrainsci 11 01525Deteksi EstrusNo ratings yet
- 1 s2.0 S0169260721002686 MainDocument8 pages1 s2.0 S0169260721002686 Mainפאוזי ג'ומעהNo ratings yet
- SISCOM-Meta AnalysisDocument8 pagesSISCOM-Meta AnalysisAiswarya HariNo ratings yet
- A. Korovaichuk, J. Makarova, V. A. Makarov, N. Benito and O. HerrerasDocument15 pagesA. Korovaichuk, J. Makarova, V. A. Makarov, N. Benito and O. HerrerasFrontiersNo ratings yet
- Automated Detection of Epileptic Seizures Using Multiscale and Refined-1Document1 pageAutomated Detection of Epileptic Seizures Using Multiscale and Refined-1Bikram MajhiNo ratings yet
- Project Report On EEG MachineDocument26 pagesProject Report On EEG Machineneetubansal60% (5)
- Vasta 2018Document6 pagesVasta 2018ouazzani youssefNo ratings yet
- Anatomy by DR Naser AlBarbariDocument24 pagesAnatomy by DR Naser AlBarbariTanmay JhulkaNo ratings yet
- FPM Formula Sheet 2Document13 pagesFPM Formula Sheet 2Yolo Gamer DudeNo ratings yet
- 2017 - Electronic Control of Linear-To-circular Polarization Conversion Using A Reconfigurable MetasurfaceDocument6 pages2017 - Electronic Control of Linear-To-circular Polarization Conversion Using A Reconfigurable Metasurfaceab4azizNo ratings yet
- Construction Method (PICC)Document2 pagesConstruction Method (PICC)rheymar diwaNo ratings yet
- Maun StreamDocument22 pagesMaun StreamPrasanth ReddyNo ratings yet
- Forensic Syllabus@Document6 pagesForensic Syllabus@YocobSamandrewsNo ratings yet
- Avago HLCP j100, HDSP 48xxDocument7 pagesAvago HLCP j100, HDSP 48xxvelizarkoNo ratings yet
- Yaesu FT-1802 Operating ManualDocument88 pagesYaesu FT-1802 Operating ManualYayok S. AnggoroNo ratings yet
- Johor-Answer Physics P3-Trial SPM 2007Document6 pagesJohor-Answer Physics P3-Trial SPM 2007kamalharmozaNo ratings yet
- Mulcher TSS: User Maintenance Manual - Spare PartsDocument35 pagesMulcher TSS: User Maintenance Manual - Spare PartsSerdar FildisNo ratings yet
- BS 03900 0 2010Document26 pagesBS 03900 0 2010selvaNo ratings yet
- Preguntas y Respuestas de LESSON 16Document4 pagesPreguntas y Respuestas de LESSON 16Sebastián Monroy CatrilNo ratings yet
- Child - Cerebral PalsyDocument3 pagesChild - Cerebral PalsyJamie Icabandi67% (3)
- SRF PresentationDocument28 pagesSRF PresentationSajeev KumarNo ratings yet
- Singer 291U1, U3Document46 pagesSinger 291U1, U3Datum VivelacriqueNo ratings yet
- Bernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeDocument14 pagesBernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeSaravanan MathiNo ratings yet
- 03 Problem On Steam Turbine - RevisedDocument16 pages03 Problem On Steam Turbine - RevisedNantia AsimakopoulouNo ratings yet
- Dit 24Document1 pageDit 24Abvolt IndiaNo ratings yet
- eHYDRO SERIESDocument6 pageseHYDRO SERIESBanupriya BalasubramanianNo ratings yet
- AB 14 para Tranzystorow DarlingtonaDocument23 pagesAB 14 para Tranzystorow DarlingtonavengalamahenderNo ratings yet
- History Medicine Knowledge OrganiserDocument4 pagesHistory Medicine Knowledge OrganiserabidaNo ratings yet
- Lucas Generator and Control Box TestsDocument28 pagesLucas Generator and Control Box TestssunhuynhNo ratings yet
- Brenes 2006Document6 pagesBrenes 2006Alfonso CáceresNo ratings yet
- Tc1057-Eng-10004 0 002 PDFDocument507 pagesTc1057-Eng-10004 0 002 PDFKenaia AdeleyeNo ratings yet
- Quickstart Dx35 de en FR Es PT ZH Ja It Ru Im0044955Document2 pagesQuickstart Dx35 de en FR Es PT ZH Ja It Ru Im0044955ROSSNo ratings yet
- State Feedback Controller Design Using MATLABDocument19 pagesState Feedback Controller Design Using MATLABhariNo ratings yet
- Atlas FiltriDocument18 pagesAtlas FiltriCristi CicireanNo ratings yet