Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Task 1 - Model AnswerDocument4 pagesTask 1 - Model AnswerShauryaNo ratings yet
- Chapter 4Document79 pagesChapter 4Clarizza0% (1)
- Emerging Space MarketsDocument153 pagesEmerging Space MarketsAlexandru Toncu100% (1)
- Fresh AHU ComparisonDocument8 pagesFresh AHU Comparisonevo2oo2No ratings yet
- Example 3 Relating Downhole Rate With The Rate at Standard ConditionsDocument8 pagesExample 3 Relating Downhole Rate With The Rate at Standard ConditionsMaisam AbbasNo ratings yet
- Changing Landscape of Recruitment IndustryDocument5 pagesChanging Landscape of Recruitment IndustryNupur SinghNo ratings yet
- How To React To Bad Christmas GiftsDocument3 pagesHow To React To Bad Christmas GiftszakupowamaniaczkaNo ratings yet
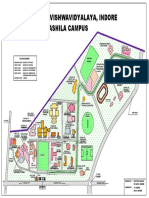
- Devi Ahilya Vishwavidyalaya, Indore Takshashila Campus: Vigyan BhawanDocument1 pageDevi Ahilya Vishwavidyalaya, Indore Takshashila Campus: Vigyan BhawankapasNo ratings yet
- The Sinister Genius of Qassem Soleimani - WSJ PDFDocument5 pagesThe Sinister Genius of Qassem Soleimani - WSJ PDFMuhammad Anique RawnNo ratings yet
- Certificate: Internal External PrincipalDocument36 pagesCertificate: Internal External PrincipalNitesh kuraheNo ratings yet
- CCR Load Calculator 2014-03-13Document41 pagesCCR Load Calculator 2014-03-13Yahya AlkaffNo ratings yet
- Neyhns: Eticket ItineraryDocument3 pagesNeyhns: Eticket Itineraryadi saputraNo ratings yet
- CTDI Phantom User's GuideDocument18 pagesCTDI Phantom User's GuideAida Cristiana SanduNo ratings yet
- Triangular Sum Labeling NEWDocument33 pagesTriangular Sum Labeling NEWMurugananthamParamasivamNo ratings yet
- Cicol NT Slurry: Constructive SolutionsDocument3 pagesCicol NT Slurry: Constructive SolutionstalatzahoorNo ratings yet
- Me 04-601Document15 pagesMe 04-601Vishnu DasNo ratings yet
- MS Fragmentation Functional Groups (Compatibility Mode)Document68 pagesMS Fragmentation Functional Groups (Compatibility Mode)Adriana Estefanía HPNo ratings yet
- Overseas Manpower SuppliersDocument10 pagesOverseas Manpower SuppliersAshwini Nair0% (1)
- Climate Variability and Climate Change 2016Document91 pagesClimate Variability and Climate Change 2016Laila Guarin100% (1)
- SGP TR 012Document276 pagesSGP TR 012Kevin Devalentino Versi IINo ratings yet
- Understanding The Transfer of Prepositions: Arabic To EnglishDocument7 pagesUnderstanding The Transfer of Prepositions: Arabic To Englishwaa2000No ratings yet
- Syllabus: Cambridge Igcse First Language EnglishDocument52 pagesSyllabus: Cambridge Igcse First Language EnglishNdache PermataNo ratings yet
- New Hptu Syllabus CSEDocument138 pagesNew Hptu Syllabus CSEerankursharma1985No ratings yet
- BD BBL, Crystal Identification SystemsDocument40 pagesBD BBL, Crystal Identification SystemsAnabell Sanchez PuertinezNo ratings yet
- Environmental Systems and Societies Paper 3 SLDocument15 pagesEnvironmental Systems and Societies Paper 3 SLAfra LamisaNo ratings yet
- PreliminariesDocument11 pagesPreliminariesGhabbFloresPalNo ratings yet
- Profitability and Marketability of The Top 55 U.S. Commercial BanksDocument19 pagesProfitability and Marketability of The Top 55 U.S. Commercial BanksSasa LuNo ratings yet
- CAR-T TherapyDocument14 pagesCAR-T TherapyrameshaachariarNo ratings yet
- A Seminar Report On: An International Study On A Risk of Cyber TerrorismDocument7 pagesA Seminar Report On: An International Study On A Risk of Cyber TerrorismManish SakalkarNo ratings yet
- KFC225 Operating HandbookDocument25 pagesKFC225 Operating HandbooksunaryaNo ratings yet