Download as docx, pdf, or txt
You might also like
- Beck Youth Inventories™ - Second Edition (BYI™-II)Document2 pagesBeck Youth Inventories™ - Second Edition (BYI™-II)Sana Khan67% (3)
- Yener Balan (Author)_ Karen Murrell (Author)_ Christopher Bryant Lentz (Author) - Big Book of Emergency Department Psychiatry_ a Guide to Patient Centered Operational Improvement-Productivity Press (2Document373 pagesYener Balan (Author)_ Karen Murrell (Author)_ Christopher Bryant Lentz (Author) - Big Book of Emergency Department Psychiatry_ a Guide to Patient Centered Operational Improvement-Productivity Press (2Jesús FloresNo ratings yet
- Apa Sample PaperDocument4 pagesApa Sample Paperapi-246564619No ratings yet
- A COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFDocument13 pagesA COGNITIVE BEHAVIOURAL THEORY OF ANOREXIA NERVOSA - Fairburn, Cooper, Shafran, 1998 PDFAnonymous yMuS0wINo ratings yet
- Eating DisordersDocument10 pagesEating Disordersapi-347625375No ratings yet
- Case Presentation: NeurologyDocument19 pagesCase Presentation: NeurologySydrex SarmientoNo ratings yet
- Eating and Feeding Disorder LatestDocument16 pagesEating and Feeding Disorder LatestSiti MuslihaNo ratings yet
- Case Study 2 Bear HoskinDocument6 pagesCase Study 2 Bear HoskinAdam100% (1)
- Annotated BibliographyDocument5 pagesAnnotated Bibliographyapi-399404406100% (2)
- Bipolar NCPDocument2 pagesBipolar NCPweehdinga89% (9)
- Eating Disorders: Manos, Bencio, Fernandes, ParaisoDocument66 pagesEating Disorders: Manos, Bencio, Fernandes, ParaisoShannen FernandezNo ratings yet
- Feeding and Eating Disorder Review LectureDocument4 pagesFeeding and Eating Disorder Review LectureMane SharNo ratings yet
- Eating and Feeding DisordersDocument28 pagesEating and Feeding DisordersGeofry OdhiamboNo ratings yet
- Eating Disorders 1Document11 pagesEating Disorders 1karlaNo ratings yet
- Eating Disorders Encopresis & Enuresis Sexual Disorders Future TrendsDocument38 pagesEating Disorders Encopresis & Enuresis Sexual Disorders Future TrendsVictoria Castillo TamayoNo ratings yet
- Dr. Radhakrishnan G. Assistant Professor & Mrs. K.Sugavanaselvi, Ph.D. ScholarDocument6 pagesDr. Radhakrishnan G. Assistant Professor & Mrs. K.Sugavanaselvi, Ph.D. ScholarnagarajanNo ratings yet
- Binge Eating Disorder (Niddk)Document6 pagesBinge Eating Disorder (Niddk)rodolfo_green_1No ratings yet
- Binge Eating DisorderDocument5 pagesBinge Eating DisorderNizamNo ratings yet
- Hypo Active Sexual DesireDocument23 pagesHypo Active Sexual DesireVisham BhimullNo ratings yet
- Eating Disorders 1Document46 pagesEating Disorders 1Heba_Al_KhozaeNo ratings yet
- Eating DisorderDocument47 pagesEating DisorderRujuta BaramateNo ratings yet
- Binge EatingDocument10 pagesBinge Eatingapi-298326412No ratings yet
- Review of The Worldwide Epidemiology of Eating DisordersDocument4 pagesReview of The Worldwide Epidemiology of Eating DisordersInês RodriguesNo ratings yet
- 7th National Nutrition SurveyDocument2 pages7th National Nutrition SurveyJorace VillamilNo ratings yet
- Mood, Anxiety and PersonalityDocument109 pagesMood, Anxiety and PersonalityRahul ShitoleNo ratings yet
- Lesson Plan Example 3Document9 pagesLesson Plan Example 3api-548834133No ratings yet
- Classification of Feeding and Eating DisordersDocument13 pagesClassification of Feeding and Eating DisordersMagito JayaNo ratings yet
- Why Am I Binge EatingDocument3 pagesWhy Am I Binge EatingDeep SpoonNo ratings yet
- Eating Disorders: by Dr. Min Min Phyo 20 August 2019Document74 pagesEating Disorders: by Dr. Min Min Phyo 20 August 2019thu thuNo ratings yet
- A Case Report of Obsessive-Compulsive DisorderDocument6 pagesA Case Report of Obsessive-Compulsive DisorderfonsoalNo ratings yet
- Adolescent Development: Physical and Emotional DevelopmentDocument14 pagesAdolescent Development: Physical and Emotional DevelopmentAoi Sora100% (1)
- Patient Education For Patient With Anorexia NervosaDocument2 pagesPatient Education For Patient With Anorexia NervosaRidha Ramdani RahmahNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- Eating Disorders Reading AssignmentDocument2 pagesEating Disorders Reading AssignmentNasratullah sahebzadaNo ratings yet
- Nutrition For Preschoolers (NTLC)Document35 pagesNutrition For Preschoolers (NTLC)Keerthana VNo ratings yet
- Nutrition and Dietary Pattern: Chap-5Document41 pagesNutrition and Dietary Pattern: Chap-5Imad AgarwalNo ratings yet
- Eating Disorders: by Group A1: Marwa Alsaleh, Zahra Almousa, Maha Alshrywi, Israa AlagnamDocument28 pagesEating Disorders: by Group A1: Marwa Alsaleh, Zahra Almousa, Maha Alshrywi, Israa AlagnamYuki HimeNo ratings yet
- Binge Eating y EmocionesDocument7 pagesBinge Eating y EmocionesGemma OrtizNo ratings yet
- Nutritional Biochemistry For Undergraduates - 102524Document13 pagesNutritional Biochemistry For Undergraduates - 102524Amal MohammedNo ratings yet
- Understanding: Body Dysmorphic DisorderDocument14 pagesUnderstanding: Body Dysmorphic DisordervivienNo ratings yet
- Eating DisordersDocument11 pagesEating Disordersapi-295926477No ratings yet
- Eating Disorders: Anorexia, Bulimia and Binge Eating DisorderDocument17 pagesEating Disorders: Anorexia, Bulimia and Binge Eating DisorderGreysi Alvarez100% (1)
- Functional Gastrointestinal Disorders: Ilmu Kesehatan Anak, 2018Document78 pagesFunctional Gastrointestinal Disorders: Ilmu Kesehatan Anak, 2018Rahmawan MapiantoNo ratings yet
- Eating and Feeding Disorders: Presented byDocument44 pagesEating and Feeding Disorders: Presented by-sparkle1234No ratings yet
- Culture Bound Syndromes NotesDocument7 pagesCulture Bound Syndromes NotesPragnya NidugondaNo ratings yet
- Most To Least Most To Least: ST ND RD THDocument4 pagesMost To Least Most To Least: ST ND RD THRommel SarjNo ratings yet
- Substance Use Disorders in Children and AdolescentsDocument21 pagesSubstance Use Disorders in Children and AdolescentsagelvezonNo ratings yet
- Guia - AdolescentesDocument6 pagesGuia - AdolescentesCentro De Psicoterapia Condesa100% (1)
- Behavioral Models of Binge-Type EatingDocument8 pagesBehavioral Models of Binge-Type Eatingpechy83No ratings yet
- When Food Becomes An EnemyDocument60 pagesWhen Food Becomes An Enemyditha timbrezaNo ratings yet
- Conceptual Models of Child Malnutrition The ACF Approach in Mental Health and Care Practices 01.2013Document76 pagesConceptual Models of Child Malnutrition The ACF Approach in Mental Health and Care Practices 01.2013yayuk dwi n100% (1)
- Bipolar Children-Cutting-Edge Controversy Insights and ResearchDocument176 pagesBipolar Children-Cutting-Edge Controversy Insights and Researchdariaevelin100% (1)
- Eating Disorders About More Than FoodDocument8 pagesEating Disorders About More Than Foodandrea diazgranadosNo ratings yet
- Family Scenario ProjectDocument13 pagesFamily Scenario Projectapi-265296849100% (2)
- Management of Childhood and Adolescent DisordersDocument26 pagesManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Nutrition in Health and Illness: For 2 Yr Nursing StudentsDocument46 pagesNutrition in Health and Illness: For 2 Yr Nursing StudentsGizachew Asimare100% (2)
- Eating Psychosexual Disorders Abuse ViolenceDocument106 pagesEating Psychosexual Disorders Abuse ViolenceMaria Pina Barbado PonceNo ratings yet
- The Role of Diet and Nutrition On Mental Health and WellbeingDocument2 pagesThe Role of Diet and Nutrition On Mental Health and Wellbeingtimea_gheneaNo ratings yet
- NCM 105 LEC Finals 1Document17 pagesNCM 105 LEC Finals 1Syed FlyntNo ratings yet
- Gender DysphoriaDocument9 pagesGender Dysphoriaapi-658923788No ratings yet
- Anorexia Research PaperDocument6 pagesAnorexia Research Paperapi-273806201100% (1)
- Case Study 11Document3 pagesCase Study 11api-347141638No ratings yet
- Masters and Johnson - The Sexual Response CycleDocument3 pagesMasters and Johnson - The Sexual Response Cycle19PSY05 ATULYA VENKATESHNo ratings yet
- Schizophernia - Unit 1Document15 pagesSchizophernia - Unit 119PSY05 ATULYA VENKATESHNo ratings yet
- Eating Disorders - CausesDocument2 pagesEating Disorders - Causes19PSY05 ATULYA VENKATESHNo ratings yet
- PracsDocument44 pagesPracs19PSY05 ATULYA VENKATESHNo ratings yet
- Psycho-Social Influences On Mood DisordersDocument4 pagesPsycho-Social Influences On Mood Disorders19PSY05 ATULYA VENKATESHNo ratings yet
- Female Sexual Interest Arousal DisorderDocument2 pagesFemale Sexual Interest Arousal Disorder19PSY05 ATULYA VENKATESHNo ratings yet
- Active Marketing Strategy in Perspective: "It's So Simple, W H y Didn ? I Think of It Lvi YseirDocument4 pagesActive Marketing Strategy in Perspective: "It's So Simple, W H y Didn ? I Think of It Lvi Yseir:-*kiss youNo ratings yet
- Gppw Project Dias (Автосохраненный) - КопияDocument24 pagesGppw Project Dias (Автосохраненный) - КопияDias YussupovNo ratings yet
- Sinha'S Comprehensive Anxiety Test by A.K.P. Sinha) : (SCAT) (Document9 pagesSinha'S Comprehensive Anxiety Test by A.K.P. Sinha) : (SCAT) (Ritu KumarNo ratings yet
- Psychological Safety-SangamDocument8 pagesPsychological Safety-SangamSangam AcharyaNo ratings yet
- Definition Essay On DepressionDocument4 pagesDefinition Essay On Depressionertzyzbaf100% (2)
- Family Systems Solution FocusedDocument5 pagesFamily Systems Solution FocusedAnis SuzanaNo ratings yet
- Southern Luzon State University College of Allied Medicine Lucban, QuezonDocument4 pagesSouthern Luzon State University College of Allied Medicine Lucban, QuezonDan HizonNo ratings yet
- Health Services in Boarding School: An Oasis of Care, Counseling, and ComfortDocument11 pagesHealth Services in Boarding School: An Oasis of Care, Counseling, and ComfortsyahrilNo ratings yet
- Ch. 18 Prepu MCDocument16 pagesCh. 18 Prepu MCTrixie Myr AndoyNo ratings yet
- Examples of DBT HomeworkDocument5 pagesExamples of DBT Homeworkerr05xmv100% (1)
- How To Stop Being ParanoidDocument10 pagesHow To Stop Being ParanoidCharmaine AlipayoNo ratings yet
- Under Codependent BehaviorsDocument3 pagesUnder Codependent BehaviorsYungstonNo ratings yet
- CBRS-Self-Report Assessment ReportDocument24 pagesCBRS-Self-Report Assessment ReportRafael Sanchez0% (3)
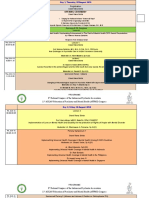
- JADWAL KONAS PDSKJI 8 Dan AFPMH 15 Semarang 2016Document5 pagesJADWAL KONAS PDSKJI 8 Dan AFPMH 15 Semarang 2016sariNo ratings yet
- CH 10 Mental Healthin VietnamDocument18 pagesCH 10 Mental Healthin Vietnammidnight proximaNo ratings yet
- Dll-Week-4 UcspDocument3 pagesDll-Week-4 UcspMark Anthony Amad0% (1)
- Pediatric Rehabilitation: The ICF-CY Model As Concept For TreatmentDocument2 pagesPediatric Rehabilitation: The ICF-CY Model As Concept For TreatmentAtet KurniadiNo ratings yet
- 21 - Stop Motion Ijertv12n4 - 13Document7 pages21 - Stop Motion Ijertv12n4 - 13derlingkepplerNo ratings yet
- 1467-6427 00198Document14 pages1467-6427 00198Fausto Adrián Rodríguez LópezNo ratings yet
- P.Davies CV July 2020Document32 pagesP.Davies CV July 2020Nane AgataoNo ratings yet
- History Taking in Psychiatry-1Document30 pagesHistory Taking in Psychiatry-1Rajalingam JanarthanNo ratings yet
- Research PaperDocument2 pagesResearch PaperGabrielle Gale BurogNo ratings yet
- Chinchu C 2023 Balancing Regulation and Autonomy Ncahp Act and The Psychology Profession in IndiaDocument6 pagesChinchu C 2023 Balancing Regulation and Autonomy Ncahp Act and The Psychology Profession in IndiaezazpsychologistNo ratings yet
- Perinatal Psychiatry: Moderator: Dr. Navkiran S. MahajanDocument51 pagesPerinatal Psychiatry: Moderator: Dr. Navkiran S. MahajanAarti GuptaNo ratings yet
- 1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersDocument4 pages1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersRita Prince0% (1)
- Siny Tosh 74785Document3 pagesSiny Tosh 74785Rajesh tonyNo ratings yet