
ABORTION
ABORTION
You might also like
- Intervention and Reflection Basic Issues in Medical EthicsDocument816 pagesIntervention and Reflection Basic Issues in Medical EthicsAndrea Jenkins89% (9)
- Argumentative Essay PDFDocument2 pagesArgumentative Essay PDFIman SontousidadNo ratings yet
- Obstructed LabourDocument15 pagesObstructed LaboursunilNo ratings yet
- Dysfunctional LabourDocument128 pagesDysfunctional LabourDebjyoti KarmakarNo ratings yet
- RA 9262 Sample Case and ElementsDocument20 pagesRA 9262 Sample Case and Elementswjap3100% (1)
- Wln-Normal LabourDocument45 pagesWln-Normal LabourEmmanuel MukukaNo ratings yet
- Diagnosis of PregnancyDocument42 pagesDiagnosis of PregnancyAastha BistaNo ratings yet
- 18 - Oligohydramnios and PolyhydramniosDocument3 pages18 - Oligohydramnios and PolyhydramniosSu OoNo ratings yet
- Abruptio PlacentaDocument20 pagesAbruptio PlacentaAlphine DalgoNo ratings yet
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- MalpresentationDocument19 pagesMalpresentationHanelie B. AldeaNo ratings yet
- Abnormal Uterine ActionDocument110 pagesAbnormal Uterine ActionAnnapurna DangetiNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyforbiddenleiNo ratings yet
- Gravida and Parity Practice QuestionsDocument1 pageGravida and Parity Practice QuestionsHazelynne MamucudNo ratings yet
- Diagnosi of PregnancyDocument7 pagesDiagnosi of Pregnancyglmachic021No ratings yet
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosoreNo ratings yet
- LabourDocument55 pagesLabourRobert Chileshe100% (1)
- 9fetal Well Being in PregnancyDocument10 pages9fetal Well Being in PregnancyuouoNo ratings yet
- Fetal MalpresentationDocument28 pagesFetal MalpresentationAhmed Gh Al-zechrawiNo ratings yet
- Antenatal AssessmentDocument46 pagesAntenatal AssessmentmariaNo ratings yet
- Abnormal LabourDocument12 pagesAbnormal Labourabidul hoqueNo ratings yet
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Abnormal Uterine Action (10 Files Merged)Document277 pagesAbnormal Uterine Action (10 Files Merged)Liji GeorgeNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Breech DeliveryDocument6 pagesBreech DeliveryNyoman TapayanaNo ratings yet
- Normal Labour in Obstetric2Document17 pagesNormal Labour in Obstetric2Tejasvi ChavdaNo ratings yet
- Effectiveness of Planned Teaching Program On Knowledge About Management of Pregnancy-Induced Hypertension and Birth Preparedness Among Antenatal Mothers With Pregnancy-Induced HypertensionDocument6 pagesEffectiveness of Planned Teaching Program On Knowledge About Management of Pregnancy-Induced Hypertension and Birth Preparedness Among Antenatal Mothers With Pregnancy-Induced Hypertensionsanvar soniNo ratings yet
- Physiology of The Menstrual Cycle 1Document22 pagesPhysiology of The Menstrual Cycle 1annonymousNo ratings yet
- Fetal MalpresentationDocument83 pagesFetal MalpresentationArianJubaneNo ratings yet
- Vacuum ExtractionDocument6 pagesVacuum ExtractionAhmad MuhyiNo ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- GDMDocument30 pagesGDMCharlz ZipaganNo ratings yet
- Normal PuerperiumDocument23 pagesNormal Puerperiumnaga maniNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Obsteric EmergenciesDocument48 pagesObsteric EmergenciesNurul AshikinNo ratings yet
- Multiple PregnancyDocument21 pagesMultiple PregnancyMazlina Maidin100% (1)
- Skills Training Manual BookDocument51 pagesSkills Training Manual BookAndi RahmaNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- 1-Evidence Based Midwifery CareDocument11 pages1-Evidence Based Midwifery CarepriyankaNo ratings yet
- Placenta and Fetal Membrane-6614Document45 pagesPlacenta and Fetal Membrane-6614Incredible DivineNo ratings yet
- Antepartum Fetal MonitoringDocument9 pagesAntepartum Fetal MonitoringDoc Prince CaballeroNo ratings yet
- Obg Qus Set 3Document24 pagesObg Qus Set 3RajaNo ratings yet
- ApgarDocument4 pagesApgarjaysille09100% (1)
- Postpartum Hemorrhage PPHDocument70 pagesPostpartum Hemorrhage PPHLoungayvan BatuyogNo ratings yet
- Postpartum ComplicationsDocument16 pagesPostpartum Complicationshoohoo100% (1)
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Introduction To Maternal NursingDocument128 pagesIntroduction To Maternal NursingNathalina DeepikaNo ratings yet
- M.M. College of Nursing: Assignment ON Different Signs During PregnancyDocument4 pagesM.M. College of Nursing: Assignment ON Different Signs During PregnancyNadiya RashidNo ratings yet
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Shubrat Singh: EctopicDocument25 pagesShubrat Singh: Ectopicshubham royalNo ratings yet
- 2 Abnormal LaborDocument88 pages2 Abnormal LaborThya HakimNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- Introduction To Obstetrics & Midwifery CareDocument18 pagesIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaNo ratings yet
- Vaginal Examination ChecklistDocument2 pagesVaginal Examination ChecklistANNENo ratings yet
- Family Life EducationDocument6 pagesFamily Life EducationKALAI AKSHAYANo ratings yet
- Factors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarDocument58 pagesFactors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarChukwu SolomonNo ratings yet
- EclampsiaDocument47 pagesEclampsiarranindyaprabasaryNo ratings yet
- Physiology of First Stage of LabourDocument3 pagesPhysiology of First Stage of Labourfortuneholiness11No ratings yet
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- Infant and Young Child FeedingDocument31 pagesInfant and Young Child FeedingKhair Soomro100% (2)
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Management of Labor and DeliveryFrom EverandManagement of Labor and DeliveryGeorge A. MaconesNo ratings yet
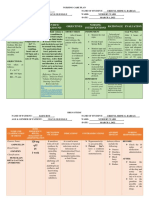
- Cues Nursing Diagnosis Scientific Background Nursing Objectives Nursing Interventions Rationale EvaluationDocument1 pageCues Nursing Diagnosis Scientific Background Nursing Objectives Nursing Interventions Rationale EvaluationCristyl Shine BariaoNo ratings yet
- I&IDocument7 pagesI&ICristyl Shine BariaoNo ratings yet
- Questionniare (REVISED)Document2 pagesQuestionniare (REVISED)Cristyl Shine BariaoNo ratings yet
- 2 Drug Study (Mvh-ns3 Bariao, Cristyl Shine G.)Document2 pages2 Drug Study (Mvh-ns3 Bariao, Cristyl Shine G.)Cristyl Shine BariaoNo ratings yet
- NCP and Drug Study (Isph-Gs Nursery)Document4 pagesNCP and Drug Study (Isph-Gs Nursery)Cristyl Shine BariaoNo ratings yet
- BROCHURE (CHN-Different Family Planning)Document2 pagesBROCHURE (CHN-Different Family Planning)Cristyl Shine BariaoNo ratings yet
- Abortion Background: ClassificationDocument8 pagesAbortion Background: ClassificationCristyl Shine BariaoNo ratings yet
- 4 Drug Study (Opd)Document4 pages4 Drug Study (Opd)Cristyl Shine BariaoNo ratings yet
- 2 NCPDocument3 pages2 NCPCristyl Shine BariaoNo ratings yet
- 2 NCP & 3 Drug StudyDocument6 pages2 NCP & 3 Drug StudyCristyl Shine BariaoNo ratings yet
- Assessment (Self Defense)Document3 pagesAssessment (Self Defense)Cristyl Shine BariaoNo ratings yet
- Abortion in A Utilitarian PerspectiveDocument8 pagesAbortion in A Utilitarian PerspectiveMae Pursia OrbonNo ratings yet
- The World's Abortion Laws - Center For Reproductive RightsDocument8 pagesThe World's Abortion Laws - Center For Reproductive RightsCarolina carol87No ratings yet
- SAS 13 - Capangpangan, Trisha Mariz M.Document3 pagesSAS 13 - Capangpangan, Trisha Mariz M.Bernadeth Barrientos ZamoraNo ratings yet
- New Scientist - 26 10 2019Document60 pagesNew Scientist - 26 10 2019Như Mai100% (1)
- Abortion in The PhilippinesDocument4 pagesAbortion in The PhilippinesChristine Joy PrestozaNo ratings yet
- Rough DraftDocument4 pagesRough Draftapi-533690138No ratings yet
- Ethical Issues Pertaining To AbortionDocument38 pagesEthical Issues Pertaining To AbortionRoman MamunNo ratings yet
- Women in The Serbian Orthodox Church HisDocument30 pagesWomen in The Serbian Orthodox Church HisGajevic SlavenNo ratings yet
- Prelims Lecture BNP RevisedDocument65 pagesPrelims Lecture BNP RevisedjeshemaNo ratings yet
- Green Mile EssayDocument7 pagesGreen Mile Essaygatxsknbf100% (1)
- Essay Writing For Pismp StudentDocument11 pagesEssay Writing For Pismp StudentismiliyanaNo ratings yet
- Abortion Debate SpeechDocument6 pagesAbortion Debate SpeechStefan Pirone100% (1)
- Prenatal Management of AnencephalyDocument5 pagesPrenatal Management of AnencephalyarifsandroNo ratings yet
- English Pamphlet Senior G10-G12-1 PDFDocument141 pagesEnglish Pamphlet Senior G10-G12-1 PDFKasweka Mukoko100% (7)
- Sept2009 PDFDocument3 pagesSept2009 PDFStéphane Gimenez FerrerNo ratings yet
- JWHO V Currier Amended ComplaintDocument59 pagesJWHO V Currier Amended ComplaintRuss LatinoNo ratings yet
- MTP Bill 2020Document16 pagesMTP Bill 2020Natasha BhasinNo ratings yet
- Abortion Paper Rough DraftDocument7 pagesAbortion Paper Rough Draftapi-263195518No ratings yet
- Argumentative Essay On AbortionDocument2 pagesArgumentative Essay On Abortion12 Dy NicoleNo ratings yet
- Maged Alqaed Final EssayDocument6 pagesMaged Alqaed Final Essayapi-284900400No ratings yet
- Baby Dumping (SR)Document4 pagesBaby Dumping (SR)Nina RoroNo ratings yet
- AbortoDocument8 pagesAbortoDelsoNo ratings yet
- Sanctuary Cities For The UnbornDocument2 pagesSanctuary Cities For The UnbornRob LauciusNo ratings yet
- Abortion TypesDocument19 pagesAbortion TypesFany MaldoNo ratings yet
- Cdi 3: Special Crime Investigation: Circumstances. Any Legally Married Person Who, Having Surprised His SpouseDocument9 pagesCdi 3: Special Crime Investigation: Circumstances. Any Legally Married Person Who, Having Surprised His SpouseJake CopradeNo ratings yet
- Bahasa Inggris Kelas XIIDocument8 pagesBahasa Inggris Kelas XIIDekrit Feryzon Peter Kusuma50% (2)
- Times Leader 07-02-2012Document20 pagesTimes Leader 07-02-2012The Times LeaderNo ratings yet


































































































Download as pdf or txt
You might also like
- Intervention and Reflection Basic Issues in Medical EthicsDocument816 pagesIntervention and Reflection Basic Issues in Medical EthicsAndrea Jenkins89% (9)
- Argumentative Essay PDFDocument2 pagesArgumentative Essay PDFIman SontousidadNo ratings yet
- Obstructed LabourDocument15 pagesObstructed LaboursunilNo ratings yet
- Dysfunctional LabourDocument128 pagesDysfunctional LabourDebjyoti KarmakarNo ratings yet
- RA 9262 Sample Case and ElementsDocument20 pagesRA 9262 Sample Case and Elementswjap3100% (1)
- Wln-Normal LabourDocument45 pagesWln-Normal LabourEmmanuel MukukaNo ratings yet
- Diagnosis of PregnancyDocument42 pagesDiagnosis of PregnancyAastha BistaNo ratings yet
- 18 - Oligohydramnios and PolyhydramniosDocument3 pages18 - Oligohydramnios and PolyhydramniosSu OoNo ratings yet
- Abruptio PlacentaDocument20 pagesAbruptio PlacentaAlphine DalgoNo ratings yet
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- MalpresentationDocument19 pagesMalpresentationHanelie B. AldeaNo ratings yet
- Abnormal Uterine ActionDocument110 pagesAbnormal Uterine ActionAnnapurna DangetiNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyforbiddenleiNo ratings yet
- Gravida and Parity Practice QuestionsDocument1 pageGravida and Parity Practice QuestionsHazelynne MamucudNo ratings yet
- Diagnosi of PregnancyDocument7 pagesDiagnosi of Pregnancyglmachic021No ratings yet
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosoreNo ratings yet
- LabourDocument55 pagesLabourRobert Chileshe100% (1)
- 9fetal Well Being in PregnancyDocument10 pages9fetal Well Being in PregnancyuouoNo ratings yet
- Fetal MalpresentationDocument28 pagesFetal MalpresentationAhmed Gh Al-zechrawiNo ratings yet
- Antenatal AssessmentDocument46 pagesAntenatal AssessmentmariaNo ratings yet
- Abnormal LabourDocument12 pagesAbnormal Labourabidul hoqueNo ratings yet
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Abnormal Uterine Action (10 Files Merged)Document277 pagesAbnormal Uterine Action (10 Files Merged)Liji GeorgeNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Breech DeliveryDocument6 pagesBreech DeliveryNyoman TapayanaNo ratings yet
- Normal Labour in Obstetric2Document17 pagesNormal Labour in Obstetric2Tejasvi ChavdaNo ratings yet
- Effectiveness of Planned Teaching Program On Knowledge About Management of Pregnancy-Induced Hypertension and Birth Preparedness Among Antenatal Mothers With Pregnancy-Induced HypertensionDocument6 pagesEffectiveness of Planned Teaching Program On Knowledge About Management of Pregnancy-Induced Hypertension and Birth Preparedness Among Antenatal Mothers With Pregnancy-Induced Hypertensionsanvar soniNo ratings yet
- Physiology of The Menstrual Cycle 1Document22 pagesPhysiology of The Menstrual Cycle 1annonymousNo ratings yet
- Fetal MalpresentationDocument83 pagesFetal MalpresentationArianJubaneNo ratings yet
- Vacuum ExtractionDocument6 pagesVacuum ExtractionAhmad MuhyiNo ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- GDMDocument30 pagesGDMCharlz ZipaganNo ratings yet
- Normal PuerperiumDocument23 pagesNormal Puerperiumnaga maniNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Obsteric EmergenciesDocument48 pagesObsteric EmergenciesNurul AshikinNo ratings yet
- Multiple PregnancyDocument21 pagesMultiple PregnancyMazlina Maidin100% (1)
- Skills Training Manual BookDocument51 pagesSkills Training Manual BookAndi RahmaNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- 1-Evidence Based Midwifery CareDocument11 pages1-Evidence Based Midwifery CarepriyankaNo ratings yet
- Placenta and Fetal Membrane-6614Document45 pagesPlacenta and Fetal Membrane-6614Incredible DivineNo ratings yet
- Antepartum Fetal MonitoringDocument9 pagesAntepartum Fetal MonitoringDoc Prince CaballeroNo ratings yet
- Obg Qus Set 3Document24 pagesObg Qus Set 3RajaNo ratings yet
- ApgarDocument4 pagesApgarjaysille09100% (1)
- Postpartum Hemorrhage PPHDocument70 pagesPostpartum Hemorrhage PPHLoungayvan BatuyogNo ratings yet
- Postpartum ComplicationsDocument16 pagesPostpartum Complicationshoohoo100% (1)
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Introduction To Maternal NursingDocument128 pagesIntroduction To Maternal NursingNathalina DeepikaNo ratings yet
- M.M. College of Nursing: Assignment ON Different Signs During PregnancyDocument4 pagesM.M. College of Nursing: Assignment ON Different Signs During PregnancyNadiya RashidNo ratings yet
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Shubrat Singh: EctopicDocument25 pagesShubrat Singh: Ectopicshubham royalNo ratings yet
- 2 Abnormal LaborDocument88 pages2 Abnormal LaborThya HakimNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- Introduction To Obstetrics & Midwifery CareDocument18 pagesIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaNo ratings yet
- Vaginal Examination ChecklistDocument2 pagesVaginal Examination ChecklistANNENo ratings yet
- Family Life EducationDocument6 pagesFamily Life EducationKALAI AKSHAYANo ratings yet
- Factors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarDocument58 pagesFactors Influencing Umbilical Cord Care Practices Among Mothers Attending Infant Welfare Clinic in Selected PrimarChukwu SolomonNo ratings yet
- EclampsiaDocument47 pagesEclampsiarranindyaprabasaryNo ratings yet
- Physiology of First Stage of LabourDocument3 pagesPhysiology of First Stage of Labourfortuneholiness11No ratings yet
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- Infant and Young Child FeedingDocument31 pagesInfant and Young Child FeedingKhair Soomro100% (2)
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Management of Labor and DeliveryFrom EverandManagement of Labor and DeliveryGeorge A. MaconesNo ratings yet
- Cues Nursing Diagnosis Scientific Background Nursing Objectives Nursing Interventions Rationale EvaluationDocument1 pageCues Nursing Diagnosis Scientific Background Nursing Objectives Nursing Interventions Rationale EvaluationCristyl Shine BariaoNo ratings yet
- I&IDocument7 pagesI&ICristyl Shine BariaoNo ratings yet
- Questionniare (REVISED)Document2 pagesQuestionniare (REVISED)Cristyl Shine BariaoNo ratings yet
- 2 Drug Study (Mvh-ns3 Bariao, Cristyl Shine G.)Document2 pages2 Drug Study (Mvh-ns3 Bariao, Cristyl Shine G.)Cristyl Shine BariaoNo ratings yet
- NCP and Drug Study (Isph-Gs Nursery)Document4 pagesNCP and Drug Study (Isph-Gs Nursery)Cristyl Shine BariaoNo ratings yet
- BROCHURE (CHN-Different Family Planning)Document2 pagesBROCHURE (CHN-Different Family Planning)Cristyl Shine BariaoNo ratings yet
- Abortion Background: ClassificationDocument8 pagesAbortion Background: ClassificationCristyl Shine BariaoNo ratings yet
- 4 Drug Study (Opd)Document4 pages4 Drug Study (Opd)Cristyl Shine BariaoNo ratings yet
- 2 NCPDocument3 pages2 NCPCristyl Shine BariaoNo ratings yet
- 2 NCP & 3 Drug StudyDocument6 pages2 NCP & 3 Drug StudyCristyl Shine BariaoNo ratings yet
- Assessment (Self Defense)Document3 pagesAssessment (Self Defense)Cristyl Shine BariaoNo ratings yet
- Abortion in A Utilitarian PerspectiveDocument8 pagesAbortion in A Utilitarian PerspectiveMae Pursia OrbonNo ratings yet
- The World's Abortion Laws - Center For Reproductive RightsDocument8 pagesThe World's Abortion Laws - Center For Reproductive RightsCarolina carol87No ratings yet
- SAS 13 - Capangpangan, Trisha Mariz M.Document3 pagesSAS 13 - Capangpangan, Trisha Mariz M.Bernadeth Barrientos ZamoraNo ratings yet
- New Scientist - 26 10 2019Document60 pagesNew Scientist - 26 10 2019Như Mai100% (1)
- Abortion in The PhilippinesDocument4 pagesAbortion in The PhilippinesChristine Joy PrestozaNo ratings yet
- Rough DraftDocument4 pagesRough Draftapi-533690138No ratings yet
- Ethical Issues Pertaining To AbortionDocument38 pagesEthical Issues Pertaining To AbortionRoman MamunNo ratings yet
- Women in The Serbian Orthodox Church HisDocument30 pagesWomen in The Serbian Orthodox Church HisGajevic SlavenNo ratings yet
- Prelims Lecture BNP RevisedDocument65 pagesPrelims Lecture BNP RevisedjeshemaNo ratings yet
- Green Mile EssayDocument7 pagesGreen Mile Essaygatxsknbf100% (1)
- Essay Writing For Pismp StudentDocument11 pagesEssay Writing For Pismp StudentismiliyanaNo ratings yet
- Abortion Debate SpeechDocument6 pagesAbortion Debate SpeechStefan Pirone100% (1)
- Prenatal Management of AnencephalyDocument5 pagesPrenatal Management of AnencephalyarifsandroNo ratings yet
- English Pamphlet Senior G10-G12-1 PDFDocument141 pagesEnglish Pamphlet Senior G10-G12-1 PDFKasweka Mukoko100% (7)
- Sept2009 PDFDocument3 pagesSept2009 PDFStéphane Gimenez FerrerNo ratings yet
- JWHO V Currier Amended ComplaintDocument59 pagesJWHO V Currier Amended ComplaintRuss LatinoNo ratings yet
- MTP Bill 2020Document16 pagesMTP Bill 2020Natasha BhasinNo ratings yet
- Abortion Paper Rough DraftDocument7 pagesAbortion Paper Rough Draftapi-263195518No ratings yet
- Argumentative Essay On AbortionDocument2 pagesArgumentative Essay On Abortion12 Dy NicoleNo ratings yet
- Maged Alqaed Final EssayDocument6 pagesMaged Alqaed Final Essayapi-284900400No ratings yet
- Baby Dumping (SR)Document4 pagesBaby Dumping (SR)Nina RoroNo ratings yet
- AbortoDocument8 pagesAbortoDelsoNo ratings yet
- Sanctuary Cities For The UnbornDocument2 pagesSanctuary Cities For The UnbornRob LauciusNo ratings yet
- Abortion TypesDocument19 pagesAbortion TypesFany MaldoNo ratings yet
- Cdi 3: Special Crime Investigation: Circumstances. Any Legally Married Person Who, Having Surprised His SpouseDocument9 pagesCdi 3: Special Crime Investigation: Circumstances. Any Legally Married Person Who, Having Surprised His SpouseJake CopradeNo ratings yet
- Bahasa Inggris Kelas XIIDocument8 pagesBahasa Inggris Kelas XIIDekrit Feryzon Peter Kusuma50% (2)
- Times Leader 07-02-2012Document20 pagesTimes Leader 07-02-2012The Times LeaderNo ratings yet