
Autologous Intestinal Reconstruction Surgery
Autologous Intestinal Reconstruction Surgery
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- 3 M Mastery ProblemDocument4 pages3 M Mastery ProblemAdam Hobbs100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AnalogyDocument24 pagesAnalogyTrung TranNo ratings yet
- Broken BeautyDocument143 pagesBroken BeautyAngelica MakAngelNo ratings yet
- Soal Bahasa Inggris IX, XIDocument10 pagesSoal Bahasa Inggris IX, XIMahda zakiyahNo ratings yet
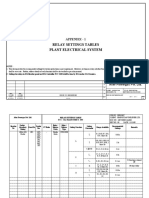
- Relay Settings TablesDocument29 pagesRelay Settings Tablesgirishprabhu1984No ratings yet
- Maclin SuitDocument5 pagesMaclin Suitnicholas.phillipsNo ratings yet
- 29 Aharavidhi PDFDocument7 pages29 Aharavidhi PDFAjitānanda DāsaNo ratings yet
- STI SP001 - SP031 Repairs 5th Edition GuidelinesDocument33 pagesSTI SP001 - SP031 Repairs 5th Edition GuidelinesJade Geronimo80% (5)
- A330 FactsDocument2 pagesA330 FactsGermanTobonNo ratings yet
- Gas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFDocument4 pagesGas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFsanjeevchhabraNo ratings yet
- 50 Most Commonly Prescribed Medications 02Document4 pages50 Most Commonly Prescribed Medications 02Jelly BeanNo ratings yet
- Blood Gas Control - Level 3 (BG Control 3)Document2 pagesBlood Gas Control - Level 3 (BG Control 3)Xuarami Estrada QuintanaNo ratings yet
- HSSC Anemia QuestionsDocument11 pagesHSSC Anemia QuestionsPooja FuloriaNo ratings yet
- AvianInsight Vol3-2012Document4 pagesAvianInsight Vol3-2012Bryan NicollNo ratings yet
- MSDS B-Kurita KF SBL-20Document1 pageMSDS B-Kurita KF SBL-20Arief SetiawanNo ratings yet
- Coastal Mitigation and Adaptation MeasuresDocument5 pagesCoastal Mitigation and Adaptation Measuresjames kaririNo ratings yet
- DS Flex Rev7 0309 PDFDocument2 pagesDS Flex Rev7 0309 PDFDavid GonzaloNo ratings yet
- Perbandingan Harga Apotek Vs PBFDocument3 pagesPerbandingan Harga Apotek Vs PBFRidho SaputraNo ratings yet
- Earth Materials and ProcessesDocument52 pagesEarth Materials and ProcessesMay Lyn BerondoNo ratings yet
- 10SV10NJ4C60Document4 pages10SV10NJ4C60GIAN FRANCO ALBERTO ARENAS VARGASNo ratings yet
- Soal PAS KLS 5 Bahasa InggrisDocument2 pagesSoal PAS KLS 5 Bahasa InggrisMahpudin Al AfganiNo ratings yet
- Plants Around UsDocument67 pagesPlants Around UsmanasmanojNo ratings yet
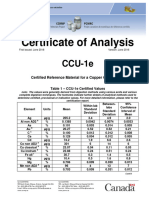
- CCU-1e Certificate enDocument6 pagesCCU-1e Certificate encencisotNo ratings yet
- Boq of House Type 250m - Tikrit CityDocument4 pagesBoq of House Type 250m - Tikrit CityHasan NabeelNo ratings yet
- PtNPs-electrochemical DepositionDocument8 pagesPtNPs-electrochemical DepositionHùng TrầnNo ratings yet
- Hypertension Course Design Iloilo Draft - Sept 14Document13 pagesHypertension Course Design Iloilo Draft - Sept 14Ruth Mary PadaNo ratings yet
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocument47 pagesNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanNo ratings yet
- Ficha3 - Unidad 1 - Jer - 5°Document3 pagesFicha3 - Unidad 1 - Jer - 5°Alberto Yepez BulejeNo ratings yet
- University of San Agustin: Senior High School DepartmentDocument3 pagesUniversity of San Agustin: Senior High School DepartmentJana Viktoria SecretoNo ratings yet
- 27 Sps Nilo and Stella Cha V CADocument3 pages27 Sps Nilo and Stella Cha V CAJunNo ratings yet



































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- 3 M Mastery ProblemDocument4 pages3 M Mastery ProblemAdam Hobbs100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AnalogyDocument24 pagesAnalogyTrung TranNo ratings yet
- Broken BeautyDocument143 pagesBroken BeautyAngelica MakAngelNo ratings yet
- Soal Bahasa Inggris IX, XIDocument10 pagesSoal Bahasa Inggris IX, XIMahda zakiyahNo ratings yet
- Relay Settings TablesDocument29 pagesRelay Settings Tablesgirishprabhu1984No ratings yet
- Maclin SuitDocument5 pagesMaclin Suitnicholas.phillipsNo ratings yet
- 29 Aharavidhi PDFDocument7 pages29 Aharavidhi PDFAjitānanda DāsaNo ratings yet
- STI SP001 - SP031 Repairs 5th Edition GuidelinesDocument33 pagesSTI SP001 - SP031 Repairs 5th Edition GuidelinesJade Geronimo80% (5)
- A330 FactsDocument2 pagesA330 FactsGermanTobonNo ratings yet
- Gas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFDocument4 pagesGas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFsanjeevchhabraNo ratings yet
- 50 Most Commonly Prescribed Medications 02Document4 pages50 Most Commonly Prescribed Medications 02Jelly BeanNo ratings yet
- Blood Gas Control - Level 3 (BG Control 3)Document2 pagesBlood Gas Control - Level 3 (BG Control 3)Xuarami Estrada QuintanaNo ratings yet
- HSSC Anemia QuestionsDocument11 pagesHSSC Anemia QuestionsPooja FuloriaNo ratings yet
- AvianInsight Vol3-2012Document4 pagesAvianInsight Vol3-2012Bryan NicollNo ratings yet
- MSDS B-Kurita KF SBL-20Document1 pageMSDS B-Kurita KF SBL-20Arief SetiawanNo ratings yet
- Coastal Mitigation and Adaptation MeasuresDocument5 pagesCoastal Mitigation and Adaptation Measuresjames kaririNo ratings yet
- DS Flex Rev7 0309 PDFDocument2 pagesDS Flex Rev7 0309 PDFDavid GonzaloNo ratings yet
- Perbandingan Harga Apotek Vs PBFDocument3 pagesPerbandingan Harga Apotek Vs PBFRidho SaputraNo ratings yet
- Earth Materials and ProcessesDocument52 pagesEarth Materials and ProcessesMay Lyn BerondoNo ratings yet
- 10SV10NJ4C60Document4 pages10SV10NJ4C60GIAN FRANCO ALBERTO ARENAS VARGASNo ratings yet
- Soal PAS KLS 5 Bahasa InggrisDocument2 pagesSoal PAS KLS 5 Bahasa InggrisMahpudin Al AfganiNo ratings yet
- Plants Around UsDocument67 pagesPlants Around UsmanasmanojNo ratings yet
- CCU-1e Certificate enDocument6 pagesCCU-1e Certificate encencisotNo ratings yet
- Boq of House Type 250m - Tikrit CityDocument4 pagesBoq of House Type 250m - Tikrit CityHasan NabeelNo ratings yet
- PtNPs-electrochemical DepositionDocument8 pagesPtNPs-electrochemical DepositionHùng TrầnNo ratings yet
- Hypertension Course Design Iloilo Draft - Sept 14Document13 pagesHypertension Course Design Iloilo Draft - Sept 14Ruth Mary PadaNo ratings yet
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocument47 pagesNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanNo ratings yet
- Ficha3 - Unidad 1 - Jer - 5°Document3 pagesFicha3 - Unidad 1 - Jer - 5°Alberto Yepez BulejeNo ratings yet
- University of San Agustin: Senior High School DepartmentDocument3 pagesUniversity of San Agustin: Senior High School DepartmentJana Viktoria SecretoNo ratings yet
- 27 Sps Nilo and Stella Cha V CADocument3 pages27 Sps Nilo and Stella Cha V CAJunNo ratings yet