Download as docx, pdf, or txt
You might also like
- Freebie Bundle-50 PagesDocument75 pagesFreebie Bundle-50 PagesKarla Seravalli86% (7)
- Research ProposalDocument5 pagesResearch ProposalAishwarya Bharath100% (2)
- ACLS Manual Provider 2016Document207 pagesACLS Manual Provider 2016AhmedShareef100% (9)
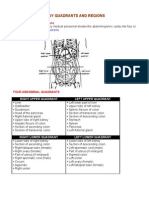
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- Glomerulonephritis-1 (Dr. Soffa)Document58 pagesGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriNo ratings yet
- Robinson Pathology Chapter 20 KidneyDocument11 pagesRobinson Pathology Chapter 20 KidneyElina Drits100% (1)
- Journal OPDDocument18 pagesJournal OPDKate WeyganNo ratings yet
- Chapter 8 Renal DiseaseDocument13 pagesChapter 8 Renal DiseaseAlanah JaneNo ratings yet
- AUBF Group 1 Chapter 8Document12 pagesAUBF Group 1 Chapter 8Gerald John PazNo ratings yet
- Glomerulonephritis: Lecturer Prof. Yu.R. KovalevDocument39 pagesGlomerulonephritis: Lecturer Prof. Yu.R. Kovalevalfaz lakhani100% (1)
- Screenshot 2022-12-05 at 15.41.06Document122 pagesScreenshot 2022-12-05 at 15.41.06Senuri ManthripalaNo ratings yet
- What Is Glomerulonephritis?Document7 pagesWhat Is Glomerulonephritis?SSNo ratings yet
- Postgrad Med J 2003 Vinen 206 13Document9 pagesPostgrad Med J 2003 Vinen 206 13Raka ArifirmandaNo ratings yet
- Acute Glomerulonephritis (AGN) OverviewDocument8 pagesAcute Glomerulonephritis (AGN) OverviewRalph Wwarren ReyesNo ratings yet
- Glomerular DsDocument18 pagesGlomerular Dsnathan asfahaNo ratings yet
- Glomerular DiseasesDocument31 pagesGlomerular DiseasesLALITH SAI KNo ratings yet
- NEPHRITISDocument37 pagesNEPHRITISJay RathvaNo ratings yet
- Lecture 4 (1of3) - Nephritic SyndromeDocument45 pagesLecture 4 (1of3) - Nephritic SyndromeAliye BaramNo ratings yet
- What Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inDocument6 pagesWhat Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inAnnapoorna SHNo ratings yet
- Nephritic SyndromeDocument24 pagesNephritic SyndromeMuhamed Al Rohani100% (2)
- 10 Primary Glumerulopathies III - GKDocument2 pages10 Primary Glumerulopathies III - GKGerarld Immanuel KairupanNo ratings yet
- ACUTE GLOMERULONEPHRITIS Refers To A Specific Set of Renal Diseases in Which An ImmunologicDocument3 pagesACUTE GLOMERULONEPHRITIS Refers To A Specific Set of Renal Diseases in Which An ImmunologicAdrian MallarNo ratings yet
- Nephritic Syndrome - Armando HasudunganDocument14 pagesNephritic Syndrome - Armando HasudunganzahraaNo ratings yet
- Causes of Acute GlomerulonephritisDocument8 pagesCauses of Acute GlomerulonephritisShielah YacubNo ratings yet
- Acute Glomerulonephritis: Background, Pathophysiology, EtiologyDocument5 pagesAcute Glomerulonephritis: Background, Pathophysiology, Etiology'Riku' Pratiwie TunaNo ratings yet
- Isolated Glomerular Disease With Recurrent Gross HematuriaDocument17 pagesIsolated Glomerular Disease With Recurrent Gross HematuriaArun GeorgeNo ratings yet
- GLOMERULONEPHRITIS (Bright's Disease)Document8 pagesGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JNo ratings yet
- Secundary Glomerular LesionsDocument2 pagesSecundary Glomerular LesionsGlogogeanu Cristina AndreeaNo ratings yet
- Nephrotic SyndromeDocument1 pageNephrotic Syndromedhruv kumarNo ratings yet
- GlomerulonephritisDocument59 pagesGlomerulonephritistressNo ratings yet
- Nephrotic SyndromeDocument65 pagesNephrotic SyndromemejulNo ratings yet
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- Rapidly Progressive GlomerulonephritisDocument17 pagesRapidly Progressive GlomerulonephritisEasyOrientDNo ratings yet
- Renal Diseases IDocument17 pagesRenal Diseases IPoojaNo ratings yet
- Acute GlomerulonephritisDocument4 pagesAcute GlomerulonephritisJulliza Joy PandiNo ratings yet
- 3&4 Glomerular Diseases and Nephrotic SyndromeDocument46 pages3&4 Glomerular Diseases and Nephrotic SyndromeTor Koang ThorNo ratings yet
- Nephrotic SyndDocument21 pagesNephrotic Synd238439904No ratings yet
- Primary Glomerulonephritis UG LectureDocument50 pagesPrimary Glomerulonephritis UG LectureMalik Mohammad AzharuddinNo ratings yet
- MANUSCRIPTDocument11 pagesMANUSCRIPTANA DelafuenteNo ratings yet
- Acute: Poststreptococca L Glomerulonephri TisDocument28 pagesAcute: Poststreptococca L Glomerulonephri TisLeroy Christy LawalataNo ratings yet
- Review Article: An Approach To The Child With Acute GlomerulonephritisDocument4 pagesReview Article: An Approach To The Child With Acute GlomerulonephritisLu Jordy LuhurNo ratings yet
- Enfermedad GlomerularDocument23 pagesEnfermedad GlomerularAlejandro beuses morrNo ratings yet
- Nephrotic Vs Nephritic SyndromeDocument80 pagesNephrotic Vs Nephritic Syndromevan016_bunnyNo ratings yet
- Lecture Note On Renal Diseases For Medical Students - GNDocument10 pagesLecture Note On Renal Diseases For Medical Students - GNEsayas KebedeNo ratings yet
- Acute Glomerulonephriti S: Group 3Document25 pagesAcute Glomerulonephriti S: Group 3AradhanaRamchandaniNo ratings yet
- AUBF Lec Week#8 Renal DiseasesDocument10 pagesAUBF Lec Week#8 Renal DiseasesLexaNatalieConcepcionJuntadoNo ratings yet
- GlomerulonephritisDocument58 pagesGlomerulonephritisJosa Anggi Pratama0% (1)
- AUBF Renal DiseasesDocument3 pagesAUBF Renal DiseasesAngela LaglivaNo ratings yet
- 14 Kidney Diseases PDFDocument128 pages14 Kidney Diseases PDFMayur WakchaureNo ratings yet
- Glomer Ds TadDocument190 pagesGlomer Ds TadHaileprince MekonnenNo ratings yet
- Glomerulonephritis: Nameesha Natasha Naidu 20130105Document26 pagesGlomerulonephritis: Nameesha Natasha Naidu 20130105AliMalikNo ratings yet
- C C C C: CC CC CCCC CC CCC CC C CCCC CC CCC C CC C CCCCC CCC CC C C CCCC CDocument1 pageC C C C: CC CC CCCC CC CCC CC C CCCC CC CCC C CC C CCCCC CCC CC C C CCCC CGabriel Rosales RM RNNo ratings yet
- Acute Glomerulonephritis (AGN)Document5 pagesAcute Glomerulonephritis (AGN)smashayielNo ratings yet
- Nephrotic Syndrome in Children-LectureDocument52 pagesNephrotic Syndrome in Children-LectureLubinda SitaliNo ratings yet
- 2 Glomerular DiseasesDocument48 pages2 Glomerular DiseasesDammaqsaa W BiyyanaaNo ratings yet
- Glomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateDocument23 pagesGlomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateRaiya MallickNo ratings yet
- Glomerulonefritis Menbrano Prol N Engl J Med 2012Document13 pagesGlomerulonefritis Menbrano Prol N Engl J Med 2012Francisco Rebollar GarduñoNo ratings yet
- Acute GlomerulonephritisDocument28 pagesAcute GlomerulonephritisPaul SinsNo ratings yet
- Agn PDFDocument6 pagesAgn PDFMohamed ZiadaNo ratings yet
- Gus156 Slide Ginjal Dan Saluran KemihDocument128 pagesGus156 Slide Ginjal Dan Saluran KemihRina ChairunnisaNo ratings yet
- Seminar On Nephrotic Syndrome: Medical Surgical NursingDocument15 pagesSeminar On Nephrotic Syndrome: Medical Surgical NursingGargi MP100% (1)
- Comprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingFrom EverandComprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingNo ratings yet
- Leukocyte Adhesion Deficiency SyndromeDocument25 pagesLeukocyte Adhesion Deficiency SyndromeperioassNo ratings yet
- ATCM JOURNAL September 2014 - 21Document60 pagesATCM JOURNAL September 2014 - 21Ivonne Flores FernándezNo ratings yet
- Brain DominanceDocument33 pagesBrain DominanceAndreea Ilie100% (1)
- Bioenergetics, Biological Oxidation and The Respiration Chain Bioenergetics and ATPDocument43 pagesBioenergetics, Biological Oxidation and The Respiration Chain Bioenergetics and ATPEmenintaNo ratings yet
- MHMC EquipmentsDocument2 pagesMHMC EquipmentsMarvinNo ratings yet
- Medical Complications of Type 2 DiabetesDocument422 pagesMedical Complications of Type 2 DiabetesMayracpp.16No ratings yet
- Drug Study: Phinma University of PangasinanDocument1 pageDrug Study: Phinma University of PangasinanVoid LessNo ratings yet
- Care NewbornDocument38 pagesCare NewbornRaja0% (1)
- Bee Stings Immunology Allergy and Treatment Marterre PDFDocument9 pagesBee Stings Immunology Allergy and Treatment Marterre PDFOktaviana Sari DewiNo ratings yet
- Lattice Corneal DystrophyDocument7 pagesLattice Corneal DystrophyPhilip McNelsonNo ratings yet
- Thyroid Gland Clinical Chemistry 2 (Laboratory) : LessonDocument4 pagesThyroid Gland Clinical Chemistry 2 (Laboratory) : LessonCherry Ann ColechaNo ratings yet
- Animal BehaviourDocument5 pagesAnimal BehaviourthinaNo ratings yet
- Revisi AnestesiDocument1 pageRevisi AnestesiWelmi Sulfatri IshakNo ratings yet
- Adrenergic Agonists and AntagonistsDocument9 pagesAdrenergic Agonists and Antagonistsstephanienwafor18No ratings yet
- Botanical Actions Reference Sheet: Botanical Action Description Physiology ExamplesDocument2 pagesBotanical Actions Reference Sheet: Botanical Action Description Physiology ExamplesDeo DoktorNo ratings yet
- Neuroanatomy Quiz BeeDocument55 pagesNeuroanatomy Quiz BeeJulienne Sanchez-Salazar100% (3)
- Fi ADocument67 pagesFi AalfonsoNo ratings yet
- Ren 10Document1 pageRen 10ray72roNo ratings yet
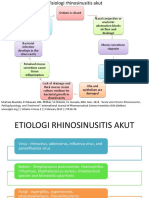
- THT RhinosinusitisDocument8 pagesTHT RhinosinusitismeiliaNo ratings yet
- BiochemistryDocument21 pagesBiochemistryS V S VardhanNo ratings yet
- Neuronal Integration and CurcuitsDocument5 pagesNeuronal Integration and CurcuitsOdyNo ratings yet
- AMES TestDocument11 pagesAMES TestJarena Ria ZolinaNo ratings yet
- Congenital Hydrocephalus: Case PresentationDocument35 pagesCongenital Hydrocephalus: Case PresentationIan Mizzel A. Dulfina100% (1)
- What Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorDocument22 pagesWhat Process Is Best Seen Using A Perpendicular CR With The Elbow in Acute Flexion and With The Posterior Aspect of The Humerus Adjacent To The Image ReceptorKalpana ParajuliNo ratings yet
- Summary Adaptations How Animals Survive UploadDocument26 pagesSummary Adaptations How Animals Survive UploadLearnRoots100% (1)
- Drug Study NCP SoapieDocument15 pagesDrug Study NCP Soapiemikrobyo_ng_wmsuNo ratings yet