Download as pdf or txt
You might also like
- CRANOBOOKREVIEW TheOxygenAdvantageTheSimpleScientificallyProvenBreathingTechniquesforaHealthierSlimmerFasterandFitterYouDocument4 pagesCRANOBOOKREVIEW TheOxygenAdvantageTheSimpleScientificallyProvenBreathingTechniquesforaHealthierSlimmerFasterandFitterYouSantiago RuizNo ratings yet
- Meat PackagingDocument22 pagesMeat PackagingkuldeepakpandeyNo ratings yet
- Emsp 1355 !!! Co2Document17 pagesEmsp 1355 !!! Co2acctsacctsNo ratings yet
- Avances en Terapia de Rehabilitacion CardiopulmonarDocument13 pagesAvances en Terapia de Rehabilitacion CardiopulmonarMaría Camila Zuluaga AriasNo ratings yet
- Biomechanical Impacts of Forward Head Posture On The Respiratory FunctionDocument16 pagesBiomechanical Impacts of Forward Head Posture On The Respiratory Functionnoflin oxyaniNo ratings yet
- Breathing Re-Education and Phenotypes of Sleep Apnea - A ReviewDocument21 pagesBreathing Re-Education and Phenotypes of Sleep Apnea - A ReviewKarol SilveiraNo ratings yet
- Review of Leslie Kaminoff's 'The Anatomy of Yoga'Document11 pagesReview of Leslie Kaminoff's 'The Anatomy of Yoga'gingergarlicNo ratings yet
- Fibrosis PulmonarDocument7 pagesFibrosis PulmonarCarlos Challco ApazaNo ratings yet
- Evaluación Manual Del DiafragmaDocument8 pagesEvaluación Manual Del DiafragmaSilvia Victoria SavaroNo ratings yet
- Breathwork in Body Psychotherapy Towards A More Unified Theory and PracticeDocument14 pagesBreathwork in Body Psychotherapy Towards A More Unified Theory and PracticeSiyao LiNo ratings yet
- The Basic Breathwork Book: A Fundamental Guide to Enhancing Health, Performance and MindfulnessFrom EverandThe Basic Breathwork Book: A Fundamental Guide to Enhancing Health, Performance and MindfulnessNo ratings yet
- Penatalaksanaan Fisioterapi Pada Asma Bronkhial Di RSKP Respira JogjakartaDocument40 pagesPenatalaksanaan Fisioterapi Pada Asma Bronkhial Di RSKP Respira Jogjakartanidafathiyyahm06No ratings yet
- Fisiologia Respiratoria para Anestesiologos 2019 PDFDocument14 pagesFisiologia Respiratoria para Anestesiologos 2019 PDFAlvarez Flores GilmerNo ratings yet
- ANA101 Respiratory System DR GIEDocument44 pagesANA101 Respiratory System DR GIEMarian Kyla MarianoNo ratings yet
- Cardiovascular Response To ExerciseDocument18 pagesCardiovascular Response To ExerciseChristian JaraNo ratings yet
- Tai Chi Latihan Pikiran-Tubuh Pada Pasien Dengan PPOK: Protokol Penelitian Untuk Uji Coba Terkontrol Secara AcakDocument13 pagesTai Chi Latihan Pikiran-Tubuh Pada Pasien Dengan PPOK: Protokol Penelitian Untuk Uji Coba Terkontrol Secara AcakaisNo ratings yet
- Guidelines For The Physiotherapy Management of Chronic Obstructive Pulmonary DiseaseDocument7 pagesGuidelines For The Physiotherapy Management of Chronic Obstructive Pulmonary DiseaseAyu AryaDewi PasyaViraNo ratings yet
- 210074.full 2Document14 pages210074.full 2Bayu TriNo ratings yet
- Journal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathDocument9 pagesJournal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathALiint Nissa NisaniestNo ratings yet
- Journal Critique On Dyspnea Running Head: Journal Critique On Dyspnea 1Document4 pagesJournal Critique On Dyspnea Running Head: Journal Critique On Dyspnea 1api-19644228No ratings yet
- BORGES F. DOS S. Et Al. Fundamentals of The Use of Ozone Therapy in The Treatment of Aesthetic Disorders A ReviewDocument31 pagesBORGES F. DOS S. Et Al. Fundamentals of The Use of Ozone Therapy in The Treatment of Aesthetic Disorders A ReviewFernandoFernandesNo ratings yet
- Altered Respiratory Function in PatientsDocument8 pagesAltered Respiratory Function in PatientsJaime SousaNo ratings yet
- Fundamentals of Work PhysiologyDocument26 pagesFundamentals of Work PhysiologyEl morroNo ratings yet
- Physical Activity, Sedentary Behaviour and Sleep in COPD Guidelines: A Systematic ReviewDocument14 pagesPhysical Activity, Sedentary Behaviour and Sleep in COPD Guidelines: A Systematic ReviewVitória PinhoNo ratings yet
- Effect of Adjuvant Yoga Therapy in Patients With COPD.Document6 pagesEffect of Adjuvant Yoga Therapy in Patients With COPD.Achudan JiiNo ratings yet
- Frontiers in Respiratory Physiology - Grand ChallengeDocument2 pagesFrontiers in Respiratory Physiology - Grand ChallengeAlfi OktafaniNo ratings yet
- Aerobic Training, Muscle Stretching Jurnal 2Document10 pagesAerobic Training, Muscle Stretching Jurnal 2Bunga Mitra MampuNo ratings yet
- PhysicalTreatments v4n3p169 enDocument6 pagesPhysicalTreatments v4n3p169 enJulenda CintarinovaNo ratings yet
- REVIEW SERIES: Physiotherapy Techniques For Respiratory DiseaseDocument10 pagesREVIEW SERIES: Physiotherapy Techniques For Respiratory DiseaseDewi aNo ratings yet
- Revistakineto 3Document8 pagesRevistakineto 3Ölvedi Tünde TimeaNo ratings yet
- Quantifiable Effects of Osteopathic Manipulative Techniques PDFDocument5 pagesQuantifiable Effects of Osteopathic Manipulative Techniques PDFRodrigo MedinaNo ratings yet
- Unit 3 OverviewDocument13 pagesUnit 3 OverviewDxmplesNo ratings yet
- Fisioterapi Ppok EngDocument7 pagesFisioterapi Ppok EngEi lessonNo ratings yet
- Loliveira,+2 Vol 14,+Calmon+CMSDocument5 pagesLoliveira,+2 Vol 14,+Calmon+CMSRafii KhairuddinNo ratings yet
- PIIS2666379122004748Document15 pagesPIIS2666379122004748will magNo ratings yet
- Curso Liberação 8Document8 pagesCurso Liberação 8IzabelNo ratings yet
- Smart Breath 2014-05-26 Book ENGDocument34 pagesSmart Breath 2014-05-26 Book ENGAndrej MilutinovicNo ratings yet
- Physiol Text CH 1Document13 pagesPhysiol Text CH 1vivexvivianNo ratings yet
- An Osteopathic Approach To Rib Somatic Dysfunction in Respiratory DisordersDocument2 pagesAn Osteopathic Approach To Rib Somatic Dysfunction in Respiratory DisorderssenseosteopatiaNo ratings yet
- Alc03 02 CopdDocument4 pagesAlc03 02 CopdDonna PakpahanNo ratings yet
- Jurnal BronchitisDocument23 pagesJurnal BronchitisErlis SinambelaNo ratings yet
- Yellow and Blue Modern Art Festival Pamphlet Trifold BrochureDocument2 pagesYellow and Blue Modern Art Festival Pamphlet Trifold BrochureMary Roselen MonayaNo ratings yet
- Applied PsychophysiologyDocument8 pagesApplied PsychophysiologyDiego MartínezNo ratings yet
- Jessica - 1Document4 pagesJessica - 1imensah22No ratings yet
- Breathing Dysfunction and ScreeningDocument13 pagesBreathing Dysfunction and ScreeningMarius Andre VisserNo ratings yet
- Cochrane - Yoga Dysfunctional BreathingDocument9 pagesCochrane - Yoga Dysfunctional Breathingsariah-jemimaNo ratings yet
- Unit 7 Blood PressureDocument11 pagesUnit 7 Blood PressureQ O R Y A N INo ratings yet
- 1 s2.0 S2095754822000539 Main AXia 2022Document9 pages1 s2.0 S2095754822000539 Main AXia 2022Louis JinNo ratings yet
- Heart Rate Variability Biofeedback Increases Baroreflex Gain and Peak Expiratory FlowDocument17 pagesHeart Rate Variability Biofeedback Increases Baroreflex Gain and Peak Expiratory FlowLuis A Gil PantojaNo ratings yet
- Current Developments and Future Directions in Respiratory PhysiotherapyDocument13 pagesCurrent Developments and Future Directions in Respiratory PhysiotherapykiranNo ratings yet
- Copd Response of The Respiratory Muscles To Rehabilitation inDocument7 pagesCopd Response of The Respiratory Muscles To Rehabilitation inoanceaNo ratings yet
- Key Points: Breathe - December 2017 - Volume 13 - No 4Document12 pagesKey Points: Breathe - December 2017 - Volume 13 - No 4thania devianithaNo ratings yet
- Muscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewDocument7 pagesMuscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewICA MULIADI VALENTINE HULUNo ratings yet
- The Oxygen Therapy: Current Medicinal Chemistry January 2013Document25 pagesThe Oxygen Therapy: Current Medicinal Chemistry January 2013Violeta TamarovaNo ratings yet
- Effect of Various Breathing Techniques On The Quality of Life in Patients With Mild To Moderate Asthma A Narrative ReviewDocument6 pagesEffect of Various Breathing Techniques On The Quality of Life in Patients With Mild To Moderate Asthma A Narrative ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Italia Final Version - Ozone Therapy in Covid-19 - 18 July 2021 - Maria Emilia Gadelha SerraDocument155 pagesItalia Final Version - Ozone Therapy in Covid-19 - 18 July 2021 - Maria Emilia Gadelha SerraCybelle LiraNo ratings yet
- COPDDocument7 pagesCOPDBalqis DamanikNo ratings yet
- Balloon TherapyDocument6 pagesBalloon TherapyIntan NingsihNo ratings yet
- THE BUTEYKO METHOD (Translated): The secret of controlled breathing for health, well-being and vitalityFrom EverandTHE BUTEYKO METHOD (Translated): The secret of controlled breathing for health, well-being and vitalityNo ratings yet
- Full Download Book Advanced District Heating and Cooling DHC Systems PDFDocument41 pagesFull Download Book Advanced District Heating and Cooling DHC Systems PDFchristopher.cordova849100% (35)
- Adsorption Equilibrium of Methane, Carbon Dioxide, and Nitrogen On Zeolite 13X at High PressuresDocument7 pagesAdsorption Equilibrium of Methane, Carbon Dioxide, and Nitrogen On Zeolite 13X at High Pressuresswlim9999No ratings yet
- Our Carbon Hoofprint: Diane Mayerfeld EditorDocument233 pagesOur Carbon Hoofprint: Diane Mayerfeld Editorzx lNo ratings yet
- Planting Your Aquarium PDFDocument12 pagesPlanting Your Aquarium PDFdraganana66No ratings yet
- Our Fragile Planet - Geosphere - The Land and Its UsesDocument217 pagesOur Fragile Planet - Geosphere - The Land and Its Useslelo2k3100% (1)
- Leighton & Murray 1966Document9 pagesLeighton & Murray 1966maurobioNo ratings yet
- 41.1.69 AOAC Official Method 999.02 Oil in OilseedsDocument3 pages41.1.69 AOAC Official Method 999.02 Oil in OilseedsAdufe RufaiNo ratings yet
- 2nd PERIODICAL TESTDocument6 pages2nd PERIODICAL TESTSheryl R. ValienteNo ratings yet
- Duoline 20 - Reasons WhyDocument4 pagesDuoline 20 - Reasons Whycasda73No ratings yet
- Megasan Catalog enDocument108 pagesMegasan Catalog enMhd Maher Al BairoutiNo ratings yet
- Approaches To Extend Gastro Intestine TransitDocument33 pagesApproaches To Extend Gastro Intestine Transitpragati trivediNo ratings yet
- MN Kmno4 PDFDocument16 pagesMN Kmno4 PDFMir Mustafa AliNo ratings yet
- EVS - Complete Lab ManualDocument26 pagesEVS - Complete Lab Manualsendtoashutosh1No ratings yet
- Combustion For Energy ConversionDocument30 pagesCombustion For Energy ConversionJohn LingNo ratings yet
- Mars Atmosphere Resource Recovery System: MarrsDocument18 pagesMars Atmosphere Resource Recovery System: MarrsClifford StoneNo ratings yet
- Fire Extinguisher: Home About Us Product Contact UsDocument3 pagesFire Extinguisher: Home About Us Product Contact UsaditNo ratings yet
- EV20001 - Environmental Science - (Mid Sem Exam Autumn 2016Document5 pagesEV20001 - Environmental Science - (Mid Sem Exam Autumn 2016Abhinaba SahaNo ratings yet
- Ecotape Primer Msds Rev-4 09-17Document5 pagesEcotape Primer Msds Rev-4 09-17Teguh SilaNo ratings yet
- Ironmaking and SteelmakingDocument436 pagesIronmaking and SteelmakingSandip KumarNo ratings yet
- Table of Contents by Author: Blue Paper TitleDocument26 pagesTable of Contents by Author: Blue Paper TitleDavid Almanza PerezNo ratings yet
- MRK Sugar MillsDocument15 pagesMRK Sugar MillsVasanth Kumar100% (1)
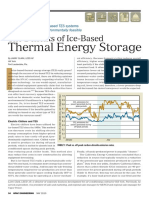
- Thermal Energy Storage: The Benefits of Ice-BasedDocument4 pagesThermal Energy Storage: The Benefits of Ice-BasedinnuRVNo ratings yet
- MSDS 681039Document9 pagesMSDS 681039toshibastabiNo ratings yet
- 4a-Design-Total FloodingDocument61 pages4a-Design-Total FloodingAhmad SalahNo ratings yet
- Factsheet Column Fraction at Ion FeyeConDocument2 pagesFactsheet Column Fraction at Ion FeyeConTianjinvinceNo ratings yet
- Esiat2014 PDFDocument7 pagesEsiat2014 PDFnauval.archNo ratings yet
- Practice Pas Xi EnglishDocument6 pagesPractice Pas Xi EnglishNysa MuktikusumaNo ratings yet
- Chapter - 7 Respiration in PlantsDocument6 pagesChapter - 7 Respiration in Plantsben martinNo ratings yet
- Water Content of Gases and Liquids Water Solubility in Liquid HydrocarbonsDocument7 pagesWater Content of Gases and Liquids Water Solubility in Liquid HydrocarbonsnguNo ratings yet