
Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022
Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022
You might also like
- Higher Everyday Inside Vol 2Document378 pagesHigher Everyday Inside Vol 2Akomolafe Olumide TundeNo ratings yet
- Leukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Document16 pagesLeukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Arnab Ghosh100% (1)
- Emergency Care (Hemophilia)Document30 pagesEmergency Care (Hemophilia)Nica Georgelle Maniego SamonteNo ratings yet
- Vibrio CholeraeDocument15 pagesVibrio Choleraetaimoor100% (1)
- Anne Frank - The Diary of A Young GirlDocument73 pagesAnne Frank - The Diary of A Young Girlnoelia almada33% (3)
- RRLfor Gasoline StationDocument6 pagesRRLfor Gasoline StationWellan Joy Dela Fuerta100% (1)
- Leukemia PDFDocument63 pagesLeukemia PDFErfan Syahid AzhariNo ratings yet
- LEUKEMIADocument20 pagesLEUKEMIAHafsaNo ratings yet
- Lymphomas and LeukemiasDocument27 pagesLymphomas and LeukemiasgraceNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Nephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)Document26 pagesNephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)GENERAL sharpNo ratings yet
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Goitre: Dr. Sandhya Gupta Assistant Professor General SurgeryDocument59 pagesGoitre: Dr. Sandhya Gupta Assistant Professor General SurgerySandhya guptaNo ratings yet
- Pediatric DMDocument39 pagesPediatric DMmy Lord JesusNo ratings yet
- Fistula in AnoDocument21 pagesFistula in AnoHannah LeiNo ratings yet
- Miliary TB NewDocument23 pagesMiliary TB Newzakariah kamalNo ratings yet
- Lecture Hemophilia and Thrombocytopenic PurpuraDocument55 pagesLecture Hemophilia and Thrombocytopenic PurpuraaymenNo ratings yet
- GoitreDocument6 pagesGoitreJohn Vladimir A. BulagsayNo ratings yet
- VASCULITISDocument79 pagesVASCULITISSol CamusNo ratings yet
- Hirschprung DiseaseDocument9 pagesHirschprung DiseaseRajeev JhaNo ratings yet
- InhalDocument33 pagesInhallupeNo ratings yet
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaNo ratings yet
- Leukemia)Document66 pagesLeukemia)Arianne BugnaNo ratings yet
- Parathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismDocument25 pagesParathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismZahrah El FaradisaNo ratings yet
- Hiv Transmission ModesDocument28 pagesHiv Transmission ModeskimaniNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- WILMs TumorDocument3 pagesWILMs TumorLorie May GuillangNo ratings yet
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocument55 pagesBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNo ratings yet
- Breast DisorderDocument89 pagesBreast DisorderYang TayengNo ratings yet
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Seminar ON Peptic Ulcer: Presented By: Ms. Sweta SinghDocument26 pagesSeminar ON Peptic Ulcer: Presented By: Ms. Sweta Singhshweta singhNo ratings yet
- Mannitol: Half-Life Onset Peak DurationDocument3 pagesMannitol: Half-Life Onset Peak DurationAmit MartinNo ratings yet
- Corneal UlcersDocument18 pagesCorneal UlcersAvinash NagarNo ratings yet
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Final OG 5Document95 pagesFinal OG 5sanjay vigneshNo ratings yet
- MeaslesDocument23 pagesMeaslesadwait marhattaNo ratings yet
- Hematuria in ChildrenDocument26 pagesHematuria in ChildrenNovenZefanya100% (1)
- National Guidelines For Screening of Hypothyroidism During PregnancyDocument48 pagesNational Guidelines For Screening of Hypothyroidism During PregnancyManish Chandra PrabhakarNo ratings yet
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaNo ratings yet
- Diverticular Disease RingkasanDocument20 pagesDiverticular Disease RingkasanSuardimanAchoNo ratings yet
- Hemophilia A&bDocument33 pagesHemophilia A&bLovelyNo ratings yet
- Case Study For LeukemiaDocument5 pagesCase Study For LeukemiaGabbii CincoNo ratings yet
- Coagulation DisordersDocument14 pagesCoagulation Disorderssusan_grace123No ratings yet
- Brucellosis 2Document70 pagesBrucellosis 2Zara IftikharNo ratings yet
- Benign Ovarian TumorsDocument38 pagesBenign Ovarian Tumorssimi yNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisKhalid Mahmud Arifin100% (1)
- BreastDocument2 pagesBreastPretty UNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Megaloblastic Anemias: Dept of Medicine AcmsDocument71 pagesMegaloblastic Anemias: Dept of Medicine Acmskunal ghosh100% (1)
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoNo ratings yet
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- Poisoning in ChildrenDocument11 pagesPoisoning in ChildrenAndriana HalfienNo ratings yet
- CSF AnalysisDocument6 pagesCSF Analysisfrederico_No ratings yet
- Family Planning Training Resource PackageDocument16 pagesFamily Planning Training Resource PackageorriNo ratings yet
- Osh State UniversityDocument14 pagesOsh State Universitykhuzaima9No ratings yet
- Acute Leukemia: Thirunavukkarasu MurugappanDocument22 pagesAcute Leukemia: Thirunavukkarasu MurugappanFelix Allen100% (1)
- Tumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .Document10 pagesTumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .mnr hmcNo ratings yet
- Cushing DiseaseDocument24 pagesCushing DiseaseSuci AlimaNo ratings yet
- Hemorrhagic Disease of The NewbornDocument2 pagesHemorrhagic Disease of The NewbornsucirahmiiiiiiNo ratings yet
- Fibroadenoma of BreastDocument7 pagesFibroadenoma of BreastA. PathakNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- Thyroid Disorders SeminarDocument86 pagesThyroid Disorders SeminarsmrutuNo ratings yet
- Gestational Trophoblastic DiseaseDocument4 pagesGestational Trophoblastic DiseasePrincess PlateroNo ratings yet
- Sankarabharanamu 2 PDFDocument7 pagesSankarabharanamu 2 PDFAdiNav PabKasNo ratings yet
- Samsung SH09xWH SH12xWH SERVICE MANUALDocument46 pagesSamsung SH09xWH SH12xWH SERVICE MANUALIoannis Perperis100% (1)
- Back Filing JsaDocument10 pagesBack Filing Jsashahazam4uNo ratings yet
- Euro Currency MarketDocument33 pagesEuro Currency Marketsfkokane83% (6)
- Theology Finals - Grade 11Document7 pagesTheology Finals - Grade 11Sophia BiancaNo ratings yet
- Tascam Us2400 ManualDocument24 pagesTascam Us2400 ManualDiego Guirado JimenezNo ratings yet
- Garden Staff Position Description 2015Document1 pageGarden Staff Position Description 2015congressheightsontheriseNo ratings yet
- Home Booklet Answer Key: Level 2Document2 pagesHome Booklet Answer Key: Level 2deniz erdemNo ratings yet
- Wa0000.Document16 pagesWa0000.Gurunath MetriNo ratings yet
- Module Week 9Document3 pagesModule Week 9Hanz Kirby Reyes FranciaNo ratings yet
- Fixture For Centering Connecting RodDocument2 pagesFixture For Centering Connecting Rodarie prasetyaNo ratings yet
- 20 K CatalogDocument126 pages20 K Catalogjchristoe2613No ratings yet
- BS 873-7 - 1984 Road Traffic Signs and Internally Illuminated Bollards Specification For Posts and FittingsDocument16 pagesBS 873-7 - 1984 Road Traffic Signs and Internally Illuminated Bollards Specification For Posts and Fittingspaul reyesNo ratings yet
- Fire Pump Field Acceptance TestDocument23 pagesFire Pump Field Acceptance Testwalitedison100% (1)
- Machiavelli'S Critique of Christianity: Paul-Erik KorvelaDocument31 pagesMachiavelli'S Critique of Christianity: Paul-Erik KorvelaMichael MungaiNo ratings yet
- Wastewater Treatment: D. Jim Livingston Asst. Prof. of ChemistryDocument22 pagesWastewater Treatment: D. Jim Livingston Asst. Prof. of ChemistryJim LivingstonNo ratings yet
- Cleanupdrive Project ProposalDocument13 pagesCleanupdrive Project ProposalAllyn Chabill AlmiranteNo ratings yet
- DP086LA: Doosan Infracore Generator EngineDocument4 pagesDP086LA: Doosan Infracore Generator EnginehirararaNo ratings yet
- Qualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Document2 pagesQualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Mikael Salamanca100% (1)
- Sustainable Development and Its CharacteristicsDocument3 pagesSustainable Development and Its CharacteristicsToxic XitNo ratings yet
- Progres Capturepro Software: Advance Your Image ResultsDocument2 pagesProgres Capturepro Software: Advance Your Image ResultsHAITHM MURSHEDNo ratings yet
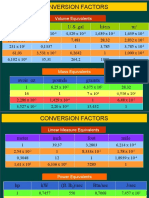
- Conversion Factors: in FT U.S. Gal Liters MDocument8 pagesConversion Factors: in FT U.S. Gal Liters MSamuel MahendraNo ratings yet
- 2019 Gynecomastia EAA Clinical Practice Guidelines PDFDocument16 pages2019 Gynecomastia EAA Clinical Practice Guidelines PDFRaluk BalaceanuNo ratings yet
- Daniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)Document3 pagesDaniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)AidanNo ratings yet
- Resource Pack - Science - Year 1 - Human Body and SensesDocument19 pagesResource Pack - Science - Year 1 - Human Body and Sensesnur fazlynaNo ratings yet
- Introduction To FEX and Cisco Nexus CommandsDocument29 pagesIntroduction To FEX and Cisco Nexus CommandsNagarajanNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Higher Everyday Inside Vol 2Document378 pagesHigher Everyday Inside Vol 2Akomolafe Olumide TundeNo ratings yet
- Leukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Document16 pagesLeukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Arnab Ghosh100% (1)
- Emergency Care (Hemophilia)Document30 pagesEmergency Care (Hemophilia)Nica Georgelle Maniego SamonteNo ratings yet
- Vibrio CholeraeDocument15 pagesVibrio Choleraetaimoor100% (1)
- Anne Frank - The Diary of A Young GirlDocument73 pagesAnne Frank - The Diary of A Young Girlnoelia almada33% (3)
- RRLfor Gasoline StationDocument6 pagesRRLfor Gasoline StationWellan Joy Dela Fuerta100% (1)
- Leukemia PDFDocument63 pagesLeukemia PDFErfan Syahid AzhariNo ratings yet
- LEUKEMIADocument20 pagesLEUKEMIAHafsaNo ratings yet
- Lymphomas and LeukemiasDocument27 pagesLymphomas and LeukemiasgraceNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Nephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)Document26 pagesNephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)GENERAL sharpNo ratings yet
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Goitre: Dr. Sandhya Gupta Assistant Professor General SurgeryDocument59 pagesGoitre: Dr. Sandhya Gupta Assistant Professor General SurgerySandhya guptaNo ratings yet
- Pediatric DMDocument39 pagesPediatric DMmy Lord JesusNo ratings yet
- Fistula in AnoDocument21 pagesFistula in AnoHannah LeiNo ratings yet
- Miliary TB NewDocument23 pagesMiliary TB Newzakariah kamalNo ratings yet
- Lecture Hemophilia and Thrombocytopenic PurpuraDocument55 pagesLecture Hemophilia and Thrombocytopenic PurpuraaymenNo ratings yet
- GoitreDocument6 pagesGoitreJohn Vladimir A. BulagsayNo ratings yet
- VASCULITISDocument79 pagesVASCULITISSol CamusNo ratings yet
- Hirschprung DiseaseDocument9 pagesHirschprung DiseaseRajeev JhaNo ratings yet
- InhalDocument33 pagesInhallupeNo ratings yet
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaNo ratings yet
- Leukemia)Document66 pagesLeukemia)Arianne BugnaNo ratings yet
- Parathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismDocument25 pagesParathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismZahrah El FaradisaNo ratings yet
- Hiv Transmission ModesDocument28 pagesHiv Transmission ModeskimaniNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- WILMs TumorDocument3 pagesWILMs TumorLorie May GuillangNo ratings yet
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocument55 pagesBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNo ratings yet
- Breast DisorderDocument89 pagesBreast DisorderYang TayengNo ratings yet
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Seminar ON Peptic Ulcer: Presented By: Ms. Sweta SinghDocument26 pagesSeminar ON Peptic Ulcer: Presented By: Ms. Sweta Singhshweta singhNo ratings yet
- Mannitol: Half-Life Onset Peak DurationDocument3 pagesMannitol: Half-Life Onset Peak DurationAmit MartinNo ratings yet
- Corneal UlcersDocument18 pagesCorneal UlcersAvinash NagarNo ratings yet
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Final OG 5Document95 pagesFinal OG 5sanjay vigneshNo ratings yet
- MeaslesDocument23 pagesMeaslesadwait marhattaNo ratings yet
- Hematuria in ChildrenDocument26 pagesHematuria in ChildrenNovenZefanya100% (1)
- National Guidelines For Screening of Hypothyroidism During PregnancyDocument48 pagesNational Guidelines For Screening of Hypothyroidism During PregnancyManish Chandra PrabhakarNo ratings yet
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaNo ratings yet
- Diverticular Disease RingkasanDocument20 pagesDiverticular Disease RingkasanSuardimanAchoNo ratings yet
- Hemophilia A&bDocument33 pagesHemophilia A&bLovelyNo ratings yet
- Case Study For LeukemiaDocument5 pagesCase Study For LeukemiaGabbii CincoNo ratings yet
- Coagulation DisordersDocument14 pagesCoagulation Disorderssusan_grace123No ratings yet
- Brucellosis 2Document70 pagesBrucellosis 2Zara IftikharNo ratings yet
- Benign Ovarian TumorsDocument38 pagesBenign Ovarian Tumorssimi yNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisKhalid Mahmud Arifin100% (1)
- BreastDocument2 pagesBreastPretty UNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Megaloblastic Anemias: Dept of Medicine AcmsDocument71 pagesMegaloblastic Anemias: Dept of Medicine Acmskunal ghosh100% (1)
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoNo ratings yet
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- Poisoning in ChildrenDocument11 pagesPoisoning in ChildrenAndriana HalfienNo ratings yet
- CSF AnalysisDocument6 pagesCSF Analysisfrederico_No ratings yet
- Family Planning Training Resource PackageDocument16 pagesFamily Planning Training Resource PackageorriNo ratings yet
- Osh State UniversityDocument14 pagesOsh State Universitykhuzaima9No ratings yet
- Acute Leukemia: Thirunavukkarasu MurugappanDocument22 pagesAcute Leukemia: Thirunavukkarasu MurugappanFelix Allen100% (1)
- Tumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .Document10 pagesTumors of Kidney: Dr.K.Sathish Kumar, MD (Hom) .mnr hmcNo ratings yet
- Cushing DiseaseDocument24 pagesCushing DiseaseSuci AlimaNo ratings yet
- Hemorrhagic Disease of The NewbornDocument2 pagesHemorrhagic Disease of The NewbornsucirahmiiiiiiNo ratings yet
- Fibroadenoma of BreastDocument7 pagesFibroadenoma of BreastA. PathakNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- Thyroid Disorders SeminarDocument86 pagesThyroid Disorders SeminarsmrutuNo ratings yet
- Gestational Trophoblastic DiseaseDocument4 pagesGestational Trophoblastic DiseasePrincess PlateroNo ratings yet
- Sankarabharanamu 2 PDFDocument7 pagesSankarabharanamu 2 PDFAdiNav PabKasNo ratings yet
- Samsung SH09xWH SH12xWH SERVICE MANUALDocument46 pagesSamsung SH09xWH SH12xWH SERVICE MANUALIoannis Perperis100% (1)
- Back Filing JsaDocument10 pagesBack Filing Jsashahazam4uNo ratings yet
- Euro Currency MarketDocument33 pagesEuro Currency Marketsfkokane83% (6)
- Theology Finals - Grade 11Document7 pagesTheology Finals - Grade 11Sophia BiancaNo ratings yet
- Tascam Us2400 ManualDocument24 pagesTascam Us2400 ManualDiego Guirado JimenezNo ratings yet
- Garden Staff Position Description 2015Document1 pageGarden Staff Position Description 2015congressheightsontheriseNo ratings yet
- Home Booklet Answer Key: Level 2Document2 pagesHome Booklet Answer Key: Level 2deniz erdemNo ratings yet
- Wa0000.Document16 pagesWa0000.Gurunath MetriNo ratings yet
- Module Week 9Document3 pagesModule Week 9Hanz Kirby Reyes FranciaNo ratings yet
- Fixture For Centering Connecting RodDocument2 pagesFixture For Centering Connecting Rodarie prasetyaNo ratings yet
- 20 K CatalogDocument126 pages20 K Catalogjchristoe2613No ratings yet
- BS 873-7 - 1984 Road Traffic Signs and Internally Illuminated Bollards Specification For Posts and FittingsDocument16 pagesBS 873-7 - 1984 Road Traffic Signs and Internally Illuminated Bollards Specification For Posts and Fittingspaul reyesNo ratings yet
- Fire Pump Field Acceptance TestDocument23 pagesFire Pump Field Acceptance Testwalitedison100% (1)
- Machiavelli'S Critique of Christianity: Paul-Erik KorvelaDocument31 pagesMachiavelli'S Critique of Christianity: Paul-Erik KorvelaMichael MungaiNo ratings yet
- Wastewater Treatment: D. Jim Livingston Asst. Prof. of ChemistryDocument22 pagesWastewater Treatment: D. Jim Livingston Asst. Prof. of ChemistryJim LivingstonNo ratings yet
- Cleanupdrive Project ProposalDocument13 pagesCleanupdrive Project ProposalAllyn Chabill AlmiranteNo ratings yet
- DP086LA: Doosan Infracore Generator EngineDocument4 pagesDP086LA: Doosan Infracore Generator EnginehirararaNo ratings yet
- Qualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Document2 pagesQualitative Analysis For Active Sulfur Species in Fuels and Solvents (Doctor Test)Mikael Salamanca100% (1)
- Sustainable Development and Its CharacteristicsDocument3 pagesSustainable Development and Its CharacteristicsToxic XitNo ratings yet
- Progres Capturepro Software: Advance Your Image ResultsDocument2 pagesProgres Capturepro Software: Advance Your Image ResultsHAITHM MURSHEDNo ratings yet
- Conversion Factors: in FT U.S. Gal Liters MDocument8 pagesConversion Factors: in FT U.S. Gal Liters MSamuel MahendraNo ratings yet
- 2019 Gynecomastia EAA Clinical Practice Guidelines PDFDocument16 pages2019 Gynecomastia EAA Clinical Practice Guidelines PDFRaluk BalaceanuNo ratings yet
- Daniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)Document3 pagesDaniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)AidanNo ratings yet
- Resource Pack - Science - Year 1 - Human Body and SensesDocument19 pagesResource Pack - Science - Year 1 - Human Body and Sensesnur fazlynaNo ratings yet
- Introduction To FEX and Cisco Nexus CommandsDocument29 pagesIntroduction To FEX and Cisco Nexus CommandsNagarajanNo ratings yet