Download as pdf or txt
You might also like
- Ambulatory Service Center Pro FormaDocument20 pagesAmbulatory Service Center Pro FormajorhnNo ratings yet
- DND 3.5 Character Sheet PDFDocument2 pagesDND 3.5 Character Sheet PDFSeth100% (1)
- Ryuutama Character Sheet - Ultimate Final Interactive Combo PackDocument4 pagesRyuutama Character Sheet - Ultimate Final Interactive Combo PackLawrence Augustine MingoaNo ratings yet
- Internal Medicine Progress Note TemplateDocument2 pagesInternal Medicine Progress Note Templatehector100% (1)
- Landing Capability (Weather) You Need: Fuel Penalty Factor/endurance You HaveDocument1 pageLanding Capability (Weather) You Need: Fuel Penalty Factor/endurance You HaveGeorge Tsolis100% (1)
- MEDIF Garuda Indonesia NewDocument3 pagesMEDIF Garuda Indonesia NewMuhammad Fikri Firmansyah100% (2)
- Air Safety Report: Flight and Weather DetailsDocument15 pagesAir Safety Report: Flight and Weather DetailsRazvan AzamfireiNo ratings yet
- Skills: STR DEX CON ACDocument6 pagesSkills: STR DEX CON ACLiivi TantaalNo ratings yet
- Conan Character Sheet - Basic v1Document3 pagesConan Character Sheet - Basic v1Kyle HoodNo ratings yet
- Autonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic DysreflexiaDocument14 pagesAutonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic Dysreflexiajacque zidaneNo ratings yet
- Introduction To PeriodontologyDocument33 pagesIntroduction To PeriodontologyEmine Alaaddinoglu100% (1)
- Dementia Toolkit PDFDocument92 pagesDementia Toolkit PDFDana Socolov100% (1)
- Medif Form SaudiaDocument3 pagesMedif Form SaudiaBijoy ThomasNo ratings yet
- Medif: Information Sheet For Passengers Requiring Special AssistanceDocument3 pagesMedif: Information Sheet For Passengers Requiring Special AssistanceAsm MohiuddinNo ratings yet
- MEDIF Singapore AirlinesDocument3 pagesMEDIF Singapore AirlinesAviasiNo ratings yet
- Asr FormDocument14 pagesAsr FormRedouane BelaassiriNo ratings yet
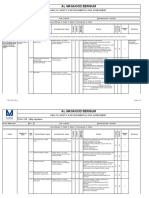
- Free Text Drop Down List: Contractor / Company To Complete Only Column A To VDocument15 pagesFree Text Drop Down List: Contractor / Company To Complete Only Column A To VAndika DamanikNo ratings yet
- Financial Proposal - Selection of Travel AgencyDocument2 pagesFinancial Proposal - Selection of Travel AgencytaqsapNo ratings yet
- Anomalous Investigations Character SheetsDocument2 pagesAnomalous Investigations Character SheetsshaunNo ratings yet
- Euroncap 2022 Isuzu D Max Crew Cab DatasheetDocument17 pagesEuroncap 2022 Isuzu D Max Crew Cab DatasheetQuiroa, Antonio JNo ratings yet
- Appendix 5.1 JSA VCP Installation Rev 0Document17 pagesAppendix 5.1 JSA VCP Installation Rev 0BELLANo ratings yet
- Evaluation Des Risques TRAVAIL EN HAUTEURDocument2 pagesEvaluation Des Risques TRAVAIL EN HAUTEURSaid BendahaneNo ratings yet
- AMB 172-016 LiftingDocument3 pagesAMB 172-016 LiftingRues AgNo ratings yet
- Dragonmech - Character SheetDocument2 pagesDragonmech - Character SheetBioskline100% (1)
- Qatar Airways - Trip SummaryDocument1 pageQatar Airways - Trip Summaryacftravel23No ratings yet
- ProfileDocument1 pageProfileEagle EyeNo ratings yet
- HIRAC July 2009 RMX - East Java - Rev - Nov - 2009Document6 pagesHIRAC July 2009 RMX - East Java - Rev - Nov - 2009Syafrian Udin NewNo ratings yet
- ZED Partner Carriers: For 9W and S2 Employees Annexure A: List of Zed PartnersDocument4 pagesZED Partner Carriers: For 9W and S2 Employees Annexure A: List of Zed PartnersAakash SawaimoonNo ratings yet
- Options - Make A Booking - Emirates ADocument2 pagesOptions - Make A Booking - Emirates AUmasankarNo ratings yet
- MI AD&D2CharacterRecordSheetsFighterDocument2 pagesMI AD&D2CharacterRecordSheetsFighterMattyNo ratings yet
- 2020 Isuzu D-Max Euro NCAPDocument17 pages2020 Isuzu D-Max Euro NCAPcarbasemyNo ratings yet
- Hyundai Engineering & Construction Co., Ltd. HAMAD MEDICAL CITY Construction Package CP-300B Hospital Fit Out ProjectDocument4 pagesHyundai Engineering & Construction Co., Ltd. HAMAD MEDICAL CITY Construction Package CP-300B Hospital Fit Out ProjectYounis Khan100% (1)
- RA For TC DismantlingDocument13 pagesRA For TC Dismantlingsalauddin0mohammedNo ratings yet
- Review Your Booking: Cdg-DelDocument2 pagesReview Your Booking: Cdg-Delradhika1992No ratings yet
- #Hiradec - DeaeratorDocument6 pages#Hiradec - DeaeratorPankaj PandeyNo ratings yet
- FadingSuns 3rd CharacterSheet InteractiveaDocument4 pagesFadingSuns 3rd CharacterSheet InteractiveaJaime d'AsmaëlNo ratings yet
- MI AD&D2CharacterRecordSheetsMultiDocument2 pagesMI AD&D2CharacterRecordSheetsMultiNeil RawlsNo ratings yet
- Cagulong Angglica: RG Breyae San Jope SamaDocument5 pagesCagulong Angglica: RG Breyae San Jope SamaJunel Alberca TandejanNo ratings yet
- Picto Flow Chart (GD Red Tide Contingency Plan) 08032018Document1 pagePicto Flow Chart (GD Red Tide Contingency Plan) 08032018Mohammad Jahangir AlamNo ratings yet
- Veristar Info: Login PasswordDocument8 pagesVeristar Info: Login Passwordbagja dwiandyNo ratings yet
- Picto Flowchart (GD Oil Spill Contingency Plan) 080318Document1 pagePicto Flowchart (GD Oil Spill Contingency Plan) 080318Mohammad Jahangir AlamNo ratings yet
- Proper Communication Should Be Done During Working While Using 2 or More Chain Block - Work Must Be Done With Proper SupervisionDocument2 pagesProper Communication Should Be Done During Working While Using 2 or More Chain Block - Work Must Be Done With Proper SupervisionDautsons InfratechNo ratings yet
- Concrete Repair RISK ASSESSMENTDocument5 pagesConcrete Repair RISK ASSESSMENTVimal ViswanathNo ratings yet
- Florida Manufacturing Companies MapDocument1 pageFlorida Manufacturing Companies MapzondmemeNo ratings yet
- BoardingCard 270662931 PSA TIADocument1 pageBoardingCard 270662931 PSA TIAËmbla DanaNo ratings yet
- AD&D - 2 Page - Oriental Adventures Player Character Record PDFDocument4 pagesAD&D - 2 Page - Oriental Adventures Player Character Record PDFTess Mercer100% (1)
- PathFinder 2E Test Toon 1Document4 pagesPathFinder 2E Test Toon 1andrew bamptonNo ratings yet
- Business Rules - Dispatch Package Builder (DXPB) - Flight Support - ConfluenceDocument2 pagesBusiness Rules - Dispatch Package Builder (DXPB) - Flight Support - ConfluenceGiridhar BoyinaNo ratings yet
- Dental Health Record: Department of EducationDocument1 pageDental Health Record: Department of EducationReymark FuentesNo ratings yet
- Thief - Assassin - MonkDocument2 pagesThief - Assassin - MonkAsiri ArasauNo ratings yet
- Homebrew PaperSheet LinedDocument1 pageHomebrew PaperSheet LinedCreativeKillJoiNo ratings yet
- Road Asphalt Works-Epc10-Ra-74-R0Document5 pagesRoad Asphalt Works-Epc10-Ra-74-R0tariq1987100% (3)
- Las Vegas McCarran Airport Terminal MapsDocument2 pagesLas Vegas McCarran Airport Terminal MapsFelix ChanNo ratings yet
- Royal Commission Risk Assessment Form: Risk Assessment For Testing & Commissioning of Overhead CranesDocument2 pagesRoyal Commission Risk Assessment Form: Risk Assessment For Testing & Commissioning of Overhead CranesLenaj Ebron100% (3)
- Jha 2023Document2 pagesJha 2023Leo TabitaNo ratings yet
- Anji Kumar Varsu ResumeDocument2 pagesAnji Kumar Varsu Resumevenkatha harishNo ratings yet
- Palin ContractDocument6 pagesPalin ContractCaliforniaWatchNo ratings yet
- Certification Request FormsDocument14 pagesCertification Request FormsCharles DoriaNo ratings yet
- Toledo City ApplicationDocument1 pageToledo City Applicationsass23No ratings yet
- Tour Expense FormatDocument1 pageTour Expense FormatPreetam DashNo ratings yet
- مراجعة اللغة الانجليزية للصف الاول الثانوي ترم اول مستر محمد فوزيDocument30 pagesمراجعة اللغة الانجليزية للصف الاول الثانوي ترم اول مستر محمد فوزيBahi AliNo ratings yet
- Eticket Itinerary / Receipt: Booking DetailsDocument4 pagesEticket Itinerary / Receipt: Booking DetailsAlmerio AmaralNo ratings yet
- Eticket Itinerary / Receipt: Booking DetailsDocument4 pagesEticket Itinerary / Receipt: Booking DetailsSolikhinNo ratings yet
- Gengigel For GingivitisDocument7 pagesGengigel For GingivitisIka Dewi RahmawatiNo ratings yet
- Chennai HospitalsDocument6 pagesChennai HospitalsGp MishraNo ratings yet
- Acute Interstitial Nephritis 2Document19 pagesAcute Interstitial Nephritis 2Paul SinsNo ratings yet
- Oswestry Disability QuestionnaireDocument2 pagesOswestry Disability Questionnaireapi-240982565No ratings yet
- Bronchiectasis: Case & ReviewDocument40 pagesBronchiectasis: Case & ReviewKhaled S. HarbNo ratings yet
- Tramm Aspen Professional DevelopmentDocument10 pagesTramm Aspen Professional Developmentapi-743605049No ratings yet
- Su Jok, Twist Therapy AND Smile MeditationDocument7 pagesSu Jok, Twist Therapy AND Smile MeditationprateekNo ratings yet
- Gardasil VAERS Adverse ReactionsDocument1,824 pagesGardasil VAERS Adverse Reactionsmcdonald.rr100% (2)
- كل أسئلة اللثة لامتحان الهيئةDocument41 pagesكل أسئلة اللثة لامتحان الهيئةMohamed KudaihNo ratings yet
- RRLDocument18 pagesRRLChristian Dave Tad-awanNo ratings yet
- Personal Injury Ire FormDocument2 pagesPersonal Injury Ire FormBioVeda Health and Wellness CentersNo ratings yet
- NDEPDocument4 pagesNDEPAkame MurasameNo ratings yet
- Bricks Intensive Reading - L2 - Word List BDocument16 pagesBricks Intensive Reading - L2 - Word List BNathaniel McleodNo ratings yet
- Kishi2019-Carvedilol and Bisoprolol As Initial Therapy For Adult HypertensionDocument8 pagesKishi2019-Carvedilol and Bisoprolol As Initial Therapy For Adult HypertensionfikriafisNo ratings yet
- Lesson 3 Patient Classification SystemDocument22 pagesLesson 3 Patient Classification SystemTanya WilliamsNo ratings yet
- A Review of The Crown Lengthening Surgery The BasiDocument8 pagesA Review of The Crown Lengthening Surgery The BasiPaTt Tyy RodríguezNo ratings yet
- Final Case Study IndividualDocument38 pagesFinal Case Study IndividualAna LuisaNo ratings yet
- Running Head: 1: PolypharmacyDocument3 pagesRunning Head: 1: PolypharmacyjosephNo ratings yet
- Report in MAPEHDocument2 pagesReport in MAPEHDavid Con RiveroNo ratings yet
- Indian - MDR 2017 - Form ListDocument3 pagesIndian - MDR 2017 - Form ListRegulatory QualityNo ratings yet
- Diagnosis and Treatment PlanningDocument66 pagesDiagnosis and Treatment PlanningVincent SerNo ratings yet
- Emergency and Disaster Nursing NewDocument42 pagesEmergency and Disaster Nursing Newlalufebrian hendika25No ratings yet
- No Jab For Me: Did You Know?Document13 pagesNo Jab For Me: Did You Know?Jamie RobinsonNo ratings yet
- Physical Distancing, Face MaskDocument16 pagesPhysical Distancing, Face MaskshdudvegNo ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet