Download as pdf or txt
You might also like
- Mrinalini Sarabhai - The Voice of HeartDocument294 pagesMrinalini Sarabhai - The Voice of Heartmrinalini_mishra89% (9)
- Kampfflieger Italian AFV'sDocument2 pagesKampfflieger Italian AFV'sLaduss100% (4)
- The French New Wave - Chris Darke (4th Ed) PDFDocument28 pagesThe French New Wave - Chris Darke (4th Ed) PDFLefteris MakedonasNo ratings yet
- Personal Protective EqptDocument8 pagesPersonal Protective EqptSana AbbasNo ratings yet
- IPArchCytolHistopatholRes 5 2 111 1151Document6 pagesIPArchCytolHistopatholRes 5 2 111 1151LyonTrioréNo ratings yet
- Ijgmp - Guidelines For Safe Handling of Dead Bodies During Covid-19Document6 pagesIjgmp - Guidelines For Safe Handling of Dead Bodies During Covid-19iaset123No ratings yet
- Healthcare Workers' Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra LeoneDocument5 pagesHealthcare Workers' Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra LeoneAlfa DexterNo ratings yet
- A Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Document18 pagesA Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Zihan Zetira100% (1)
- Guide To Forensic Pathology Practice For Death Cases Related To Coronavirus Disease 2019 COVID 19 Trial DraftDocument8 pagesGuide To Forensic Pathology Practice For Death Cases Related To Coronavirus Disease 2019 COVID 19 Trial DraftDavid AlvarezNo ratings yet
- Healthcare Workers' Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra LeoneDocument19 pagesHealthcare Workers' Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra LeoneAlfa DexterNo ratings yet
- Ijgmp - Procedure For Management and Discarding of Deceased Bodies in Covid-19Document12 pagesIjgmp - Procedure For Management and Discarding of Deceased Bodies in Covid-19iaset123No ratings yet
- UntitledDocument7 pagesUntitledlavanya gowdaNo ratings yet
- COVID 19PartI IP2020Document12 pagesCOVID 19PartI IP2020hanady shehataNo ratings yet
- Clinical Immunology: Review ArticleDocument9 pagesClinical Immunology: Review ArticleSimon Peter SiansakaNo ratings yet
- Historia de Nuevo CoronavirusDocument6 pagesHistoria de Nuevo CoronavirusGiiszs AlvarezNo ratings yet
- PDF en InglésDocument8 pagesPDF en InglésJuan Carlos Najera OrtízNo ratings yet
- CM442 49 Covid-19Document7 pagesCM442 49 Covid-19Mohammed DookaliNo ratings yet
- Current Situation of Coronavirus Disease Covid19 Review ArticleDocument4 pagesCurrent Situation of Coronavirus Disease Covid19 Review ArticleasuscribdNo ratings yet
- Clinical Orthodontic Management During The COVID-19 PandemicDocument12 pagesClinical Orthodontic Management During The COVID-19 PandemicakNo ratings yet
- Paga Stem (B) FoDocument6 pagesPaga Stem (B) FoChristian Paul A. AsicoNo ratings yet
- Covid Disease 2019Document1 pageCovid Disease 2019Rolando NABUSNo ratings yet
- COVID 19 The Catastrophe of Our TimeDocument13 pagesCOVID 19 The Catastrophe of Our TimegygyNo ratings yet
- Jclinpath 2020 206522.fullDocument4 pagesJclinpath 2020 206522.fullRobert StevenNo ratings yet
- The Role of Masks and Respirator Protection Against Sars-Cov-2Document2 pagesThe Role of Masks and Respirator Protection Against Sars-Cov-2Esther Margaretha YolandaNo ratings yet
- Resolution of Coronavirus Disease 2019 COVID 19Document12 pagesResolution of Coronavirus Disease 2019 COVID 19Job GonzagaNo ratings yet
- COVID-19 Among Healthcare Workers: Risk of Exposure, Impacts and Biosafety Measures - A ReviewDocument16 pagesCOVID-19 Among Healthcare Workers: Risk of Exposure, Impacts and Biosafety Measures - A ReviewEdwin Santiago Delgado RospigliosiNo ratings yet
- Coronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy: Pradip - Dashraath - Vijayakumar@nuhs - Edu.sgDocument11 pagesCoronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy: Pradip - Dashraath - Vijayakumar@nuhs - Edu.sgMedecinBissMedNo ratings yet
- Knowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentDocument49 pagesKnowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentOmima MuhammedNo ratings yet
- Resolution of Coronavirus Disease 2019 (COVID-19) : Expert Review of Anti-Infective TherapyDocument12 pagesResolution of Coronavirus Disease 2019 (COVID-19) : Expert Review of Anti-Infective TherapyJevera JoshuaNo ratings yet
- International Journal of Infectious Diseases: EditorialDocument3 pagesInternational Journal of Infectious Diseases: EditorialAdrian BeteringheNo ratings yet
- Sajed & Amgain, 2020Document3 pagesSajed & Amgain, 2020NUR ATIKA BINTI HALIMNo ratings yet
- Acceptance and Attitudes Toward COVID-19 Vaccines: A Cross-Sectional Study From JordanDocument15 pagesAcceptance and Attitudes Toward COVID-19 Vaccines: A Cross-Sectional Study From JordanAmira SekrettNo ratings yet
- Influenza Virus 2021Document6 pagesInfluenza Virus 2021cdsaludNo ratings yet
- Otopsi Pada Dugaan Kasus Covid-19Document12 pagesOtopsi Pada Dugaan Kasus Covid-19Inna Mutmainnah MusaNo ratings yet
- BBRC Vol 14 No 04 2021-46Document7 pagesBBRC Vol 14 No 04 2021-46Dr Sharique AliNo ratings yet
- Intensive Care Unit Setup For COVID-19Document7 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Chaurasia, Pal - 2020 - Application of Machine Learning Time Series Analysis For Prediction COVID-19 Pandemic-AnnotatedDocument13 pagesChaurasia, Pal - 2020 - Application of Machine Learning Time Series Analysis For Prediction COVID-19 Pandemic-AnnotatedZipeng WuNo ratings yet
- Protecting Chinese Healthcare Workers While Combating The 2019 Novel CoronavirusDocument2 pagesProtecting Chinese Healthcare Workers While Combating The 2019 Novel CoronaviruschristienNo ratings yet
- Attitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudyDocument7 pagesAttitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudydauntlessNo ratings yet
- 1 s2.0 S2352301820301648 MainDocument11 pages1 s2.0 S2352301820301648 MainNunungTriwahyuniNo ratings yet
- Preparedness of Africa For The Coronavirus Disease 2019 (Covid-19)Document6 pagesPreparedness of Africa For The Coronavirus Disease 2019 (Covid-19)Warner LlaveNo ratings yet
- Covid 19: Rajni SharmaDocument33 pagesCovid 19: Rajni SharmaJuan CruzNo ratings yet
- Coronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowDocument6 pagesCoronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowswabrijNo ratings yet
- Ijerph 19 15601Document9 pagesIjerph 19 15601Zamri Mat SamanNo ratings yet
- Pone 0236918Document13 pagesPone 0236918MegbaruNo ratings yet
- Containment Plan: Novel Coronavirus Disease 2019 (COVID 19)Document22 pagesContainment Plan: Novel Coronavirus Disease 2019 (COVID 19)Mayank MishraNo ratings yet
- COVID-19: International Journal of Trend in Scientific Research and Development (IJTSRD)Document5 pagesCOVID-19: International Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- A Review On COVID-19: A Global and Sri Lanka PerspectiveDocument8 pagesA Review On COVID-19: A Global and Sri Lanka PerspectiveajmrdNo ratings yet
- CHAPTER 1 2 Final ResearchDocument16 pagesCHAPTER 1 2 Final ResearchZhaena Julien BalceNo ratings yet
- Review Article: Safety Recommendations For Forensic Laboratory Staff During COVID-19 PandemicDocument9 pagesReview Article: Safety Recommendations For Forensic Laboratory Staff During COVID-19 Pandemicchavez.tel9No ratings yet
- Abbasi Oshaghi2020Document11 pagesAbbasi Oshaghi2020Kim MinhNo ratings yet
- Comparison of Inflammatory Markers Between Covid Vaccinated Population and Naturally Infected PopulationDocument9 pagesComparison of Inflammatory Markers Between Covid Vaccinated Population and Naturally Infected PopulationIJAR JOURNALNo ratings yet
- Journal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewDocument15 pagesJournal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewOscar Oswaldo SCNo ratings yet
- Dental Considerations After The Outbreak of 2019 Novel Coronavirus Disease: A Review of LiteratureDocument7 pagesDental Considerations After The Outbreak of 2019 Novel Coronavirus Disease: A Review of Literatureharshita parasharNo ratings yet
- WHO 2019 Ncov IPC - Masks 2020.3 EngDocument5 pagesWHO 2019 Ncov IPC - Masks 2020.3 EngStephanie SommerfeldNo ratings yet
- Akk Jurnal Internasional 1Document7 pagesAkk Jurnal Internasional 1Onnii SltrNo ratings yet
- AdvBiomedRes10124-2776492 074244Document8 pagesAdvBiomedRes10124-2776492 074244sarhang talebaniNo ratings yet
- Jessica Le - Covid-19Document3 pagesJessica Le - Covid-19api-523306558No ratings yet
- An Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)Document13 pagesAn Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)ayoubNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Nurseslabs PDFDocument21 pagesCoronavirus Disease 2019 (COVID-19) - Nurseslabs PDFSanket TelangNo ratings yet
- WHO Masks GuidelinesDocument5 pagesWHO Masks GuidelinesLarryDCurtisNo ratings yet
- Fracture Non-Union Epidemiology and Treatment: Trauma June 2015Document10 pagesFracture Non-Union Epidemiology and Treatment: Trauma June 2015Muhammad RaflirNo ratings yet
- Incidence, Etiology and Management of Acute Anterior Uveitis: A Hospital Based StudyDocument6 pagesIncidence, Etiology and Management of Acute Anterior Uveitis: A Hospital Based StudyMuhammad RaflirNo ratings yet
- Prevalence of Blindness in Patients With Uveitis: Original ResearchDocument4 pagesPrevalence of Blindness in Patients With Uveitis: Original ResearchMuhammad RaflirNo ratings yet
- Case Report Intususepsi 2Document4 pagesCase Report Intususepsi 2Muhammad RaflirNo ratings yet
- Rheumatoid Arthritis-Associated Aortitis: A Case Report and Literature ReviewDocument7 pagesRheumatoid Arthritis-Associated Aortitis: A Case Report and Literature ReviewMuhammad RaflirNo ratings yet
- Hands Function and Rheumatoid Arthritis Case ReporDocument4 pagesHands Function and Rheumatoid Arthritis Case ReporMuhammad RaflirNo ratings yet
- The Atypical Presentation of Rheumatoid Arthritis in An Elderly Woman: A Case ReportDocument2 pagesThe Atypical Presentation of Rheumatoid Arthritis in An Elderly Woman: A Case ReportMuhammad RaflirNo ratings yet
- 1234 FBM203Document16 pages1234 FBM203andresg417No ratings yet
- GIS Question Bank - SRM Valliammai PDFDocument12 pagesGIS Question Bank - SRM Valliammai PDFDr.Suriya SaravananNo ratings yet
- هامThe Literature ReviewDocument3 pagesهامThe Literature Reviewايهاب غزالة100% (1)
- Health Education Plan For PTBDocument2 pagesHealth Education Plan For PTBSheena ClaireNo ratings yet
- DavidBourchier IlliberalDemocracyinIndonesiaDocument322 pagesDavidBourchier IlliberalDemocracyinIndonesiapbisleadNo ratings yet
- AG - C3, S1 - FunsheetDocument1 pageAG - C3, S1 - FunsheetTARSEHSNo ratings yet
- 151 VidculversdfiuxbrogDocument212 pages151 VidculversdfiuxbrogWilson Valderrama PajueloNo ratings yet
- Kryotec Engine: Tightening Torque (No ReuseDocument1 pageKryotec Engine: Tightening Torque (No ReuseSomnath9850No ratings yet
- Taj HotelDocument36 pagesTaj HotelDharitRathod100% (1)
- Carianna Resume 2016Document2 pagesCarianna Resume 2016api-331898004No ratings yet
- Universal Grammar Approaches: in First Language AcquisitionDocument6 pagesUniversal Grammar Approaches: in First Language AcquisitionMark Vincent Z. PadillaNo ratings yet
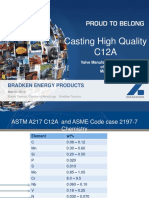
- Casting High Quality C12A: Bradken Energy ProductsDocument37 pagesCasting High Quality C12A: Bradken Energy Productsdelta lab sangliNo ratings yet
- Prophet Hope Khoza - See in The SpiritDocument36 pagesProphet Hope Khoza - See in The SpiritMiguel SierraNo ratings yet
- Goldscmidt AlgoDocument4 pagesGoldscmidt AlgochayanpathakNo ratings yet
- Problems Facing Science Teachers in PublDocument12 pagesProblems Facing Science Teachers in PublEquity KonceptsNo ratings yet
- Custom Organ Design ModuleDocument20 pagesCustom Organ Design ModuleDoh-ManNo ratings yet
- Practice Set in Inorganic ChemistryDocument3 pagesPractice Set in Inorganic ChemistryKalachuchiNo ratings yet
- Introduction of The Topic: SWOT Analysis (Alternatively SWOT Matrix) Is An Acronym For Strengths, WeaknessDocument59 pagesIntroduction of The Topic: SWOT Analysis (Alternatively SWOT Matrix) Is An Acronym For Strengths, WeaknessStarNo ratings yet
- Science FPDDocument8 pagesScience FPDapi-397408254No ratings yet
- Cookery 10 Quarter 3 Las 3Document4 pagesCookery 10 Quarter 3 Las 3Michole Godwin RegalaNo ratings yet
- PWC Managing Innovation Pharma PDFDocument20 pagesPWC Managing Innovation Pharma PDFAryan RsNo ratings yet
- Logic Gate Investigatory PDFDocument12 pagesLogic Gate Investigatory PDFGaurang MathurNo ratings yet
- OTEC Advanced Composite Cold Water Pipe: Final Technical ReportDocument160 pagesOTEC Advanced Composite Cold Water Pipe: Final Technical ReportFauzan Hizbu RahmanNo ratings yet
- Project ReportDocument10 pagesProject ReportSpecialspace Pvt LtdNo ratings yet
- Brand Engagement With Brand ExpressionDocument27 pagesBrand Engagement With Brand ExpressionArun KCNo ratings yet
- Basic Types of CakeDocument13 pagesBasic Types of CakeJoyNo ratings yet
- Topic Test - Genetics MemoDocument5 pagesTopic Test - Genetics Memomaiselatebogo4No ratings yet