Download as docx, pdf, or txt
You might also like
- Ankylosed Primary Teeth With No Permanent Successors: What Do You Do? - Part 1Document7 pagesAnkylosed Primary Teeth With No Permanent Successors: What Do You Do? - Part 1Isabela GD GheNo ratings yet
- Diagnostic Microbiology: Identification of MicrobesDocument20 pagesDiagnostic Microbiology: Identification of MicrobesMarl EstradaNo ratings yet
- V Sharmistha DasDocument15 pagesV Sharmistha DasSharmistha DasNo ratings yet
- Virus Patho-ImmunologyDocument8 pagesVirus Patho-ImmunologySirwan SalmanNo ratings yet
- Immunological Techniques FallDocument45 pagesImmunological Techniques Fallali.menem15No ratings yet
- VirologyDocument11 pagesVirologyMarcoNo ratings yet
- Typhoid Blood Test ReportDocument3 pagesTyphoid Blood Test ReportPranay BhosaleNo ratings yet
- Immulite: Anti-HDocument28 pagesImmulite: Anti-HpinoponiNo ratings yet
- Q&A Oslo Revisi 61023Document10 pagesQ&A Oslo Revisi 61023syukriNo ratings yet
- L5 - Animal Cell BiotechDocument48 pagesL5 - Animal Cell Biotechtrieupg.22bi13431No ratings yet
- Corrected Lucidchart Week17 18 Group2 Cluster2Document15 pagesCorrected Lucidchart Week17 18 Group2 Cluster2Roan-Lhieyne Sagli Diad VenancioNo ratings yet
- Kotsiou 1994Document4 pagesKotsiou 1994Murillo MoraesNo ratings yet
- 4 CIC Immune Response Status 2p ENDocument2 pages4 CIC Immune Response Status 2p EN郑伟健No ratings yet
- Widal Agglutination Test PDFDocument5 pagesWidal Agglutination Test PDFशशांक तिवारीNo ratings yet
- Epstein-Barr Virus Super FinalDocument6 pagesEpstein-Barr Virus Super FinalStill DollNo ratings yet
- TuberculosisDocument5 pagesTuberculosislittlecandiesNo ratings yet
- 1) Serology - IntroductionDocument5 pages1) Serology - IntroductionAssem AlmoughrabiNo ratings yet
- Risk of Infection NCPDocument5 pagesRisk of Infection NCPLloyd Adrian GaffudNo ratings yet
- Immunology and SerologyDocument33 pagesImmunology and SerologyICE ADRIENNE OCAMPONo ratings yet
- Tes Lab Penyakit Infeksi Dan Tropis (April 2011)Document143 pagesTes Lab Penyakit Infeksi Dan Tropis (April 2011)Fajrul AnsarNo ratings yet
- Case Study Neonatal SepsisDocument21 pagesCase Study Neonatal SepsisLenjun0% (1)
- Comparison of Serum Neopterin Levels in Pulmonary Tuberculosis PatientsDocument3 pagesComparison of Serum Neopterin Levels in Pulmonary Tuberculosis PatientsParluhutan DolliNo ratings yet
- Normal Spontaneous Delivery Case StudyDocument8 pagesNormal Spontaneous Delivery Case Studykrystelle jade labineNo ratings yet
- 17 - Serological DiagnosisDocument9 pages17 - Serological DiagnosisTamda ShitakeNo ratings yet
- Case Report Elizabeth KingiaDocument7 pagesCase Report Elizabeth KingiaSardono WidinugrohoNo ratings yet
- PIIS1198743X14652605Document3 pagesPIIS1198743X14652605Gerald NacoNo ratings yet
- Cryptococcal Postinfectious Inflammatory Response Syndrome in An Immunocompetent HostDocument3 pagesCryptococcal Postinfectious Inflammatory Response Syndrome in An Immunocompetent HostinfectogoNo ratings yet
- Diagnostic Procedure Result Interpretation ELISA. A Test That Involves Taking A Sample of YourDocument2 pagesDiagnostic Procedure Result Interpretation ELISA. A Test That Involves Taking A Sample of YourAngeli RanocoNo ratings yet
- Lec 6Document32 pagesLec 6Ghadi AbdalazizNo ratings yet
- Q&A OsloDocument9 pagesQ&A OslosyukriNo ratings yet
- Classic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyDocument5 pagesClassic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyTanveerNo ratings yet
- Laboratory Report: It Gradually Declines. The Test May Be Negative in Early Part of First WeekDocument2 pagesLaboratory Report: It Gradually Declines. The Test May Be Negative in Early Part of First Weekdeep shahNo ratings yet
- Classic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyDocument6 pagesClassic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversydjebrutNo ratings yet
- Co AmoxyclavDocument2 pagesCo AmoxyclavHaneulNo ratings yet
- 34 FullDocument8 pages34 FullCherryNo ratings yet
- Cefuroxime Axetil (IV)Document2 pagesCefuroxime Axetil (IV)STORAGE FILENo ratings yet
- Syphilis STI (25 May)Document3 pagesSyphilis STI (25 May)Nicky Wei WeiNo ratings yet
- Antistreptolysin oDocument3 pagesAntistreptolysin oces8bautistaNo ratings yet
- Journal of Clinical Microbiology-1999-Schröter-233.fullDocument2 pagesJournal of Clinical Microbiology-1999-Schröter-233.fullFaisal JamshedNo ratings yet
- Pediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OlderDocument3 pagesPediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OldernadiahNo ratings yet
- GCP Chapter 5Document6 pagesGCP Chapter 5NamjoonieNo ratings yet
- Course Case Studies - Viral HepatitisDocument5 pagesCourse Case Studies - Viral HepatitiswqmxmNo ratings yet
- Case #4 Asthma (BSN3F, Group3)Document19 pagesCase #4 Asthma (BSN3F, Group3)Eduard GarchitorenaNo ratings yet
- Rationale The Presence ofDocument24 pagesRationale The Presence ofPia CadornaNo ratings yet
- Classic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyDocument5 pagesClassic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyFarid RzNo ratings yet
- Tests For Dengue GROUP 3Document22 pagesTests For Dengue GROUP 3chocoholic potchiNo ratings yet
- Kelompok 2 - JR Dr. Arif - Morbus HansenDocument26 pagesKelompok 2 - JR Dr. Arif - Morbus Hansenregina pingkanNo ratings yet
- New Onset Autoimmune Disease or Macrophage Activation SyndromeDocument5 pagesNew Onset Autoimmune Disease or Macrophage Activation SyndromePyaePhyoAungNo ratings yet
- (Secondary Syphilis and Human Immunodeficiency Virus (HIV) Coinfection: A Case Report)Document14 pages(Secondary Syphilis and Human Immunodeficiency Virus (HIV) Coinfection: A Case Report)ahmad unissulaNo ratings yet
- Endo GenusDocument5 pagesEndo Genuslabor baiturrahimNo ratings yet
- 1 Fever Without FocusDocument27 pages1 Fever Without Focushamzatrad949No ratings yet
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNo ratings yet
- HIV ScriptDocument4 pagesHIV ScriptEspinosa, JoshuaNo ratings yet
- Emhj 2017 23 12 821 829Document9 pagesEmhj 2017 23 12 821 829tranganhNo ratings yet
- In Vivo Assessment of Antiviral Reactivity in Chronic HIV InfectionDocument7 pagesIn Vivo Assessment of Antiviral Reactivity in Chronic HIV InfectionFrontiersNo ratings yet
- Case Report Epididymal Tuberculosis Abscess in Patient Immunocompetent (2021)Document2 pagesCase Report Epididymal Tuberculosis Abscess in Patient Immunocompetent (2021)Nghi VõNo ratings yet
- Diagnosis of Viral Infection (2021-2022)Document21 pagesDiagnosis of Viral Infection (2021-2022)Fahim JaniNo ratings yet
- Anti HCVDocument5 pagesAnti HCVFaisal JamshedNo ratings yet
- Blood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryDocument44 pagesBlood Groups & Red Cell Antigen & Their Significance.: Vishant Malik 19sbas2060001 MSC BiochemistryChaudhary Vishant MalikNo ratings yet
- Accuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in ThailandDocument4 pagesAccuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in Thailandrestu anindityaNo ratings yet
- CHIBUZODocument67 pagesCHIBUZOJanice ScatesNo ratings yet
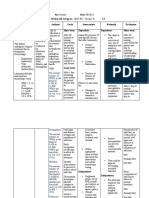
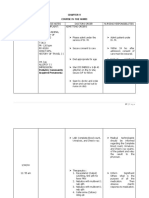
- S/ N Nursing Diagnosis Nursing Objectives Nursing Interventions Scientific Rationale EvaluationDocument3 pagesS/ N Nursing Diagnosis Nursing Objectives Nursing Interventions Scientific Rationale EvaluationJanice ScatesNo ratings yet
- 4&5project Birth AsphyxiaDocument16 pages4&5project Birth AsphyxiaJanice ScatesNo ratings yet
- Analysis of Infant and Child Mortality Trends and Differentials in Kaduna StateDocument194 pagesAnalysis of Infant and Child Mortality Trends and Differentials in Kaduna StateJanice ScatesNo ratings yet
- Anatomy of The HeartDocument7 pagesAnatomy of The HeartJanice ScatesNo ratings yet
- Burn - WikipediaDocument31 pagesBurn - WikipediaJanice ScatesNo ratings yet
- Chapter One 1.1 Background of StudyDocument39 pagesChapter One 1.1 Background of StudyJanice ScatesNo ratings yet
- First Periodical Examination in Tle 10 (Cookery) : San Juan National High School-San Antonio AnnexDocument4 pagesFirst Periodical Examination in Tle 10 (Cookery) : San Juan National High School-San Antonio AnnexMichelle Copones Llanes100% (1)
- Drugs The Straight Facts, Body Enhancement Products OptimizedDocument121 pagesDrugs The Straight Facts, Body Enhancement Products OptimizedDeathbedeli100% (3)
- Initial TemplateDocument8 pagesInitial TemplateZuj PayNo ratings yet
- Housekeeping's Cleaning Responsibilities in Front-Of-The-House Areas of The HotelDocument5 pagesHousekeeping's Cleaning Responsibilities in Front-Of-The-House Areas of The HotelThandar Swe ZinNo ratings yet
- Toaz - Info A Grade 11 Pe 2nd Sem PRDocument2 pagesToaz - Info A Grade 11 Pe 2nd Sem PRAllyn AntionNo ratings yet
- Bio Lab 11Document5 pagesBio Lab 11Sarah JaglalNo ratings yet
- Knapik 2009Document7 pagesKnapik 2009Dr XNo ratings yet
- TV Addiction Research PaperDocument5 pagesTV Addiction Research Paperc9r0s69n100% (1)
- DHHS Denial of St. Francis AppealDocument2 pagesDHHS Denial of St. Francis Appealstreiff at redstateNo ratings yet
- IJHSS - A Study On - Md. Afzalur RahmanDocument10 pagesIJHSS - A Study On - Md. Afzalur Rahmaniaset123No ratings yet
- Advertisement (Cold Drink)Document80 pagesAdvertisement (Cold Drink)Jay ParidaNo ratings yet
- TDR GEN Guidance 05.1 EngDocument19 pagesTDR GEN Guidance 05.1 EngarchicoolNo ratings yet
- FIQ - Retinal Vein OcclusionDocument31 pagesFIQ - Retinal Vein OcclusionHikban FiqhiNo ratings yet
- Chapter 2 - FINAL Concept of InclusionDocument30 pagesChapter 2 - FINAL Concept of Inclusionyohannes lemiNo ratings yet
- Pydah College of EngineeringDocument31 pagesPydah College of Engineeringkmp pssrNo ratings yet
- CS HTNDocument16 pagesCS HTNAngela Carrillo Triano67% (3)
- Drug Study Form Drug Name Classification Mechanism of Action Side Effects/ Adverse Effects Nursing Considerations/ Patient and Family TeachingDocument2 pagesDrug Study Form Drug Name Classification Mechanism of Action Side Effects/ Adverse Effects Nursing Considerations/ Patient and Family TeachingXerxes DejitoNo ratings yet
- Pengaruh Larutan Madu Terhadap Tekanan Darah Lanjut Usia HipertensiDocument10 pagesPengaruh Larutan Madu Terhadap Tekanan Darah Lanjut Usia HipertensiNopita SariNo ratings yet
- Pooling Arrangements and Diversification of RiskDocument26 pagesPooling Arrangements and Diversification of RiskMaliha TribhuNo ratings yet
- Textbook Liver Disease in Clinical Practice 1St Edition Tim Cross Eds Ebook All Chapter PDFDocument53 pagesTextbook Liver Disease in Clinical Practice 1St Edition Tim Cross Eds Ebook All Chapter PDFkenneth.london798100% (10)
- How To Write An Introduction For A Research Paper PowerpointDocument6 pagesHow To Write An Introduction For A Research Paper Powerpointefhs1rd0No ratings yet
- Horm S 23 00313 1Document32 pagesHorm S 23 00313 1andreopNo ratings yet
- Mould Pune BrochureDocument11 pagesMould Pune BrochureShiva RamanNo ratings yet
- Approach To Nursing Assessment 1Document5 pagesApproach To Nursing Assessment 1Taiye OkondoNo ratings yet
- Quality Assurance LaboratoryDocument118 pagesQuality Assurance LaboratoryMahesh KumarNo ratings yet
- International BrochureDocument12 pagesInternational BrochureI KnocksNo ratings yet
- Human Resource (HR) Policy PDFDocument55 pagesHuman Resource (HR) Policy PDFrezanur rahatNo ratings yet
- AARC Asthma COPD GuidelineDocument5 pagesAARC Asthma COPD GuidelineMarcelo JunWeiNo ratings yet
- Fatalities Nursing Home AcfDocument11 pagesFatalities Nursing Home AcfNewsChannel 9No ratings yet