Download as pdf or txt
You might also like
- Nursing Care Plans (NCP) of Abruptio PlacentaDocument13 pagesNursing Care Plans (NCP) of Abruptio PlacentaKath76% (21)
- Chapter 7: Nursing Care of The Family Having Difficulty Conceiving A ChildDocument17 pagesChapter 7: Nursing Care of The Family Having Difficulty Conceiving A ChildTiffany Joy QuiliopeNo ratings yet
- BioethicsCasesEEI 316232215 PDFDocument38 pagesBioethicsCasesEEI 316232215 PDFAman UllahNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJanine Erika Julom BrillantesNo ratings yet
- HIV & AIDS PreventionDocument48 pagesHIV & AIDS PreventionkiookabNo ratings yet
- The Omaha System-FinalDocument21 pagesThe Omaha System-FinalerajanejNo ratings yet
- Hereditary SpherocytosisDocument39 pagesHereditary SpherocytosisjoannaNo ratings yet
- Volume ImpairmentDocument32 pagesVolume ImpairmentAcohCChaoNo ratings yet
- 01 Chapter Anti InfectiveDocument90 pages01 Chapter Anti InfectiveMSKCNo ratings yet
- Newborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesDocument7 pagesNewborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesGenn Medrano GirayNo ratings yet
- PoliomyelitisDocument4 pagesPoliomyelitisGerard Adad Misa100% (1)
- Community DiagnosisDocument184 pagesCommunity Diagnosisstephanie valerioNo ratings yet
- Case Study AGE With Signs of DehydrationDocument27 pagesCase Study AGE With Signs of DehydrationZhenmeiNo ratings yet
- Bioethics CU 1Document1 pageBioethics CU 1ImongheartNo ratings yet
- Preseptal CellulitisDocument4 pagesPreseptal CellulitisKm PlegariaNo ratings yet
- Medical and Nursing Management Nursing Care PlanDocument7 pagesMedical and Nursing Management Nursing Care PlanPau-pau BasiNo ratings yet
- Case Study CSDocument21 pagesCase Study CSThessa Lonica GarciaNo ratings yet
- Management of Patients With Intestinal and Rectal DisordersDocument33 pagesManagement of Patients With Intestinal and Rectal DisordersDoneva Lyn MedinaNo ratings yet
- 2 Assisting Clients To Use Incentive Spirometer DosdosDocument3 pages2 Assisting Clients To Use Incentive Spirometer DosdosBianca Mikaela DosdosNo ratings yet
- 10 Golden Rules For Administering Drug SafetyDocument17 pages10 Golden Rules For Administering Drug SafetyBien OcampoNo ratings yet
- Case Study On Toxic GoiterDocument5 pagesCase Study On Toxic GoiterRein EstradaNo ratings yet
- CATAINA, Maria Elizabeth D. - Case-scenario-DRDocument3 pagesCATAINA, Maria Elizabeth D. - Case-scenario-DRMarielle CatainaNo ratings yet
- Ectopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Document10 pagesEctopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- A. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherDocument70 pagesA. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherMwansaay Twain HolyNo ratings yet
- Pilitter 2Document2 pagesPilitter 2Jenny VilleNo ratings yet
- MARY GRACE (CHN) Final Presentation For FNCPDocument6 pagesMARY GRACE (CHN) Final Presentation For FNCPMary grace VirayNo ratings yet
- Criteria Good Fair Poor Rationale Justification XDocument3 pagesCriteria Good Fair Poor Rationale Justification XJaye DangoNo ratings yet
- NCM 107 1.2Document2 pagesNCM 107 1.2Clint Mikael EulatrizNo ratings yet
- Module I Group WorkDocument6 pagesModule I Group WorkNur Sanaani100% (1)
- The Expanded Program On ImmunizationDocument5 pagesThe Expanded Program On ImmunizationLovelyn B. OliverosNo ratings yet
- Diffrent Between Medical Asepsis and Surgical AsepDocument5 pagesDiffrent Between Medical Asepsis and Surgical AsepShafiq AimieNo ratings yet
- Experiment 7Document7 pagesExperiment 7kimber_gado100% (2)
- Pott Disease 1223292121651385 8Document54 pagesPott Disease 1223292121651385 8Ismail SalimNo ratings yet
- GRP 3 2 Renal Nephrectomy NCPDocument6 pagesGRP 3 2 Renal Nephrectomy NCPPam RomeroNo ratings yet
- Case Presentation Second Year 2nd SemesterDocument36 pagesCase Presentation Second Year 2nd SemesterJohn Robert PescadorNo ratings yet
- Bea-Case StudyDocument21 pagesBea-Case Studybea pegadNo ratings yet
- 2016 Chronic Hypertension in PregnancyDocument13 pages2016 Chronic Hypertension in PregnancydkasisNo ratings yet
- Genitourinary AssessementDocument46 pagesGenitourinary AssessementShenaNo ratings yet
- Rafols, Janna Mae L. 3F-2C OR QuestionsDocument8 pagesRafols, Janna Mae L. 3F-2C OR QuestionsJan Crizza Dale R. FrancoNo ratings yet
- Tonsillitis and AdenoiditisDocument12 pagesTonsillitis and AdenoiditisHannah Angelu CabadingNo ratings yet
- Public Health Nurse Nursing ProceduresDocument9 pagesPublic Health Nurse Nursing ProcedureskzbreakerrNo ratings yet
- BioethicsDocument11 pagesBioethicsgabbybibobuNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthClouiseNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument4 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- Health Assessment ToolDocument3 pagesHealth Assessment ToolGail GenturalezNo ratings yet
- Demography & Mortality Rates: by Dr. Muhammad Bilal ShahDocument39 pagesDemography & Mortality Rates: by Dr. Muhammad Bilal ShahmuhammadbilalshahNo ratings yet
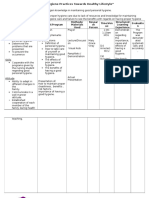
- Task 1. Assessing Your Understanding: Ethical Principle Example in Nursing PracticeDocument4 pagesTask 1. Assessing Your Understanding: Ethical Principle Example in Nursing PracticeRanz Kenneth G. FrandoNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJay-ar Batara SorianoNo ratings yet
- Ru Ward ClassDocument12 pagesRu Ward ClassAmal MUTIANo ratings yet
- Endometrial Hyperplasia - Gyn ReviewDocument18 pagesEndometrial Hyperplasia - Gyn ReviewFedrik Monte Kristo LimbongNo ratings yet
- Annotated Group 2 Impetigo Concept Mapping 1Document30 pagesAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANONo ratings yet
- GonorrheaDocument7 pagesGonorrheaEköw Santiago JavierNo ratings yet
- Chapter 6 - MCNDocument2 pagesChapter 6 - MCNPrincess Queenie OlarteNo ratings yet
- NCP DiarrheaDocument2 pagesNCP DiarrheaPrincess Xzmae RamirezNo ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Explor LaparotomyDocument14 pagesExplor LaparotomyGracia NievesNo ratings yet
- Caesarean Section4817080565385082090Document38 pagesCaesarean Section4817080565385082090DoaaNo ratings yet
- Eunice Foote and GHG HWDocument8 pagesEunice Foote and GHG HWSteffiNo ratings yet
- CalcCarbonFootprint StudentHODocument4 pagesCalcCarbonFootprint StudentHOSteffiNo ratings yet
- Pediatric Vital Sign Normal RangesDocument1 pagePediatric Vital Sign Normal RangesSteffiNo ratings yet
- CHN 2-Borderfree++Module 5Document20 pagesCHN 2-Borderfree++Module 5SteffiNo ratings yet
- 4 - Historical Perspective in Nursing and ComputerDocument13 pages4 - Historical Perspective in Nursing and ComputerSteffiNo ratings yet
- FDAR FormatDocument1 pageFDAR FormatSteffiNo ratings yet
- ANESTHESIADocument53 pagesANESTHESIASteffiNo ratings yet
- Drug Study Misoprostol PDFDocument5 pagesDrug Study Misoprostol PDFSteffiNo ratings yet
- 6 - Computer SystemDocument18 pages6 - Computer SystemSteffiNo ratings yet
- Urinary CatheterizationDocument41 pagesUrinary CatheterizationSteffiNo ratings yet
- InstrumentsDocument55 pagesInstrumentsSteffiNo ratings yet
- 11 Core Elements of Evidence - Based Gerontological Nursing PracticeDocument29 pages11 Core Elements of Evidence - Based Gerontological Nursing PracticeSteffiNo ratings yet
- A Nursing Case Study On EctopicPregnancy PDFDocument60 pagesA Nursing Case Study On EctopicPregnancy PDFSteffiNo ratings yet
- Oxygen Therapy and Administration V2Document32 pagesOxygen Therapy and Administration V2SteffiNo ratings yet
- Module 4 - Community Health AssessmentDocument8 pagesModule 4 - Community Health AssessmentSteffi100% (1)
- Nanotechnology 1Document4 pagesNanotechnology 1SteffiNo ratings yet
- Vital Signs BP: CR: RR: Temp: HT WT: O2 Saturation: Biophysical Psychosocial and Functional AssessmentDocument2 pagesVital Signs BP: CR: RR: Temp: HT WT: O2 Saturation: Biophysical Psychosocial and Functional AssessmentSteffiNo ratings yet
- 7 Summary Understanding Chronic IllnessDocument4 pages7 Summary Understanding Chronic IllnessSteffiNo ratings yet
- Module 5 - E-Health and Community DevelopmentDocument28 pagesModule 5 - E-Health and Community DevelopmentSteffi100% (2)
- Pleural Effusion Secondary To Community Acquired Pneumonia PathophysiologyDocument5 pagesPleural Effusion Secondary To Community Acquired Pneumonia PathophysiologySteffiNo ratings yet
- Fluid and ElectrolyteDocument26 pagesFluid and ElectrolyteSteffiNo ratings yet
- Cholecyctitis Nursing Concept Map DocDocument1 pageCholecyctitis Nursing Concept Map DocSteffiNo ratings yet
- 8 Summary Major Chronic Illness of Older Adult Understanding The Pathophysiology and Nursing InterventionDocument21 pages8 Summary Major Chronic Illness of Older Adult Understanding The Pathophysiology and Nursing InterventionSteffiNo ratings yet
- 9 Summary Health Education in Chronic IllnessDocument5 pages9 Summary Health Education in Chronic IllnessSteffiNo ratings yet
- Patient Profile: de La Salle-Lipa College of NursingDocument37 pagesPatient Profile: de La Salle-Lipa College of NursingSteffiNo ratings yet
- Ob Case 3 ChartDocument6 pagesOb Case 3 ChartSteffiNo ratings yet
- Applications That Support Nursing ResearchDocument23 pagesApplications That Support Nursing ResearchSteffiNo ratings yet
- Patient Profile: de La Salle-Lipa College of NursingDocument37 pagesPatient Profile: de La Salle-Lipa College of NursingSteffiNo ratings yet
- NCP Ineffective Tissue PerfusionDocument4 pagesNCP Ineffective Tissue PerfusionSteffiNo ratings yet
- Case Presentation: Neonatal Sepsis: Submitted byDocument22 pagesCase Presentation: Neonatal Sepsis: Submitted bySteffiNo ratings yet
- PUERPERIUMDocument42 pagesPUERPERIUMKBDNo ratings yet
- UNwanted Teenage PregnancyDocument7 pagesUNwanted Teenage PregnancyHisan Ainun Nissa Al khoironiNo ratings yet
- Gynecomastia Incidence Causes and TreatmentDocument9 pagesGynecomastia Incidence Causes and TreatmentAqshaNo ratings yet
- Oxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United StatesDocument9 pagesOxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United Statesstat madeeasyNo ratings yet
- 5534 21456 1 PBDocument8 pages5534 21456 1 PBAkhawat Ahir ZamanNo ratings yet
- Journal InfertilitasDocument7 pagesJournal InfertilitasNanda Safira AlisaNo ratings yet
- Nur 146 (Rle)Document138 pagesNur 146 (Rle)Antoinette PeleñaNo ratings yet
- Atosiban-5ml InfusionDocument5 pagesAtosiban-5ml InfusionMd. Abdur RahmanNo ratings yet
- Lupus NephritisDocument39 pagesLupus NephritisGowrisangarNo ratings yet
- (Introduction) Psychological Health and Life Experiences of Pregnant Adolescent Mothers in JamaicaDocument17 pages(Introduction) Psychological Health and Life Experiences of Pregnant Adolescent Mothers in JamaicaSebastian CrayNo ratings yet
- Abnormal Vaginal BleedingDocument2 pagesAbnormal Vaginal BleedingPrincess Gee OdanNo ratings yet
- Nursing Care of Clients With Reproductive Health ProblemsDocument100 pagesNursing Care of Clients With Reproductive Health ProblemsHassen ZabalaNo ratings yet
- Finals - MCN RLEDocument6 pagesFinals - MCN RLEKorean GirlNo ratings yet
- Chapter 1Document2 pagesChapter 1青No ratings yet
- PTSD After ChildbirthDocument3 pagesPTSD After ChildbirthJayla LadsonNo ratings yet
- Menopause Dan KlimakteriumDocument20 pagesMenopause Dan KlimakteriumAlfix AnugrahNo ratings yet
- Obstetric Anaesthesia: Dr/Ismail Ahmed Anesthesia Consultant MD Al Azhar University EgyptDocument25 pagesObstetric Anaesthesia: Dr/Ismail Ahmed Anesthesia Consultant MD Al Azhar University EgyptRun HajNo ratings yet
- 2 Sexual Reproduction in Flowering PlantsDocument5 pages2 Sexual Reproduction in Flowering PlantsPreeti AgrawalNo ratings yet
- Faktor Maternal Dan Pola Makan Dengan Kejadian Kekurangan Energi Kronik Pada Ibu Hamil Di Wilayah Kerja Uptd Puskesmas KangkungDocument8 pagesFaktor Maternal Dan Pola Makan Dengan Kejadian Kekurangan Energi Kronik Pada Ibu Hamil Di Wilayah Kerja Uptd Puskesmas KangkungMaria TamarNo ratings yet
- EndocrinologyDocument25 pagesEndocrinologyMaryam ShahzadiNo ratings yet
- Jamia Millia Islamia University Faculty of LawDocument22 pagesJamia Millia Islamia University Faculty of LawTaiyabaNo ratings yet
- A Woman PortraitDocument1 pageA Woman PortraitAloysius Ferry Setiawan DaryantoNo ratings yet
- Gestational Diabetes MellitusDocument29 pagesGestational Diabetes MellitusWed LodNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- New BeginningsDocument19 pagesNew BeginningsSalma TariqNo ratings yet
- Science Matters Volume B - Term 1-2Document61 pagesScience Matters Volume B - Term 1-2Andrea Nguyen100% (2)
- Low Birth WeightDocument20 pagesLow Birth Weightsandhyaa7srinivassanNo ratings yet
- Iron Deficiency AnemiaDocument16 pagesIron Deficiency AnemiaSaboorMalikNo ratings yet
- Acute Uterine InversionDocument9 pagesAcute Uterine Inversionvictor onapaNo ratings yet