
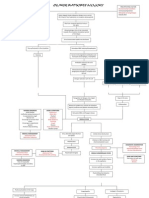
Gonorrhea and Syphylis Pa Tho Physiology
Gonorrhea and Syphylis Pa Tho Physiology
You might also like
- Pathophysiology of PharyngitisDocument1 pagePathophysiology of PharyngitisKRISTINE BULACAN100% (1)
- Feu GP FGTDocument16 pagesFeu GP FGTAla'a Emerald AguamNo ratings yet
- Meningitis PathoDocument2 pagesMeningitis PathoGlenn Asuncion Pagaduan50% (2)
- Pa Tho Physiology of DengueDocument1 pagePa Tho Physiology of Denguesinister17100% (1)
- PATHOPHYSIOLOGY-PTB - FinalDocument1 pagePATHOPHYSIOLOGY-PTB - FinaliamMye100% (1)
- Microbial Diseases of The Skin and Eyes (Microbiology Chapter 21)Document82 pagesMicrobial Diseases of The Skin and Eyes (Microbiology Chapter 21)Katrina Isabel100% (1)
- 1.pathophysiology of MeningitisDocument1 page1.pathophysiology of Meningitisshielamaygo05100% (1)
- Pathophysiology of TuberculosisDocument2 pagesPathophysiology of TuberculosisLeikkaNo ratings yet
- Pathophysiology Acute Pyelonephritis: Precipitating FactorsDocument2 pagesPathophysiology Acute Pyelonephritis: Precipitating Factorsgodwinkent888No ratings yet
- Pathophysiology of Syphilis & GonorrheaDocument14 pagesPathophysiology of Syphilis & GonorrheasourabhNo ratings yet
- Patho DengueDocument3 pagesPatho DengueLindy Shane BoncalesNo ratings yet
- PneumoniaDocument1 pagePneumoniaAyen FornollesNo ratings yet
- Dengue FeverDocument8 pagesDengue Feverramoli1988No ratings yet
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Path o Physiology of SyphilisDocument1 pagePath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- Pathophysiology Acute Bacterial MeningitisDocument2 pagesPathophysiology Acute Bacterial MeningitisNadira Farah PrayogoNo ratings yet
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoNo ratings yet
- Case Study GonorrheaDocument37 pagesCase Study GonorrheaAnge MinguitoNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- Pathophysiology (Book-Based) : CystitisDocument9 pagesPathophysiology (Book-Based) : CystitisIrish EspinosaNo ratings yet
- Pathophysiology of Meningococcal Meningitis and SepticaemiaDocument8 pagesPathophysiology of Meningococcal Meningitis and SepticaemiaEugen TarnovschiNo ratings yet
- Precipitating Factors Predisposing Factors: LegendDocument2 pagesPrecipitating Factors Predisposing Factors: LegendAlvin Dagumbal100% (1)
- D. Pa Tho Physiology of PneumoniaDocument4 pagesD. Pa Tho Physiology of PneumoniaBill Clinton Lamira BabanNo ratings yet
- MeaslesDocument7 pagesMeaslesKarl FloresNo ratings yet
- Pathophysiology of Varicella Zoster Virus-ChickenpoxDocument8 pagesPathophysiology of Varicella Zoster Virus-ChickenpoxXerxes DejitoNo ratings yet
- Malaria PathophysiologyDocument2 pagesMalaria PathophysiologyMaecy PasionNo ratings yet
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraNo ratings yet
- Pathophysiology Dengue Hemorrhagic FeverDocument1 pagePathophysiology Dengue Hemorrhagic FeverShiella Heart Malana100% (1)
- Pathophysiology TBDocument2 pagesPathophysiology TBJhen DeguzmanNo ratings yet
- Non-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The AmericasDocument2 pagesNon-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The Americaschristian quiaoitNo ratings yet
- Hodgkins LymphomaDocument3 pagesHodgkins LymphomaLefe Arvie Dela PeñaNo ratings yet
- Dengue PathophysiologyDocument1 pageDengue PathophysiologyRafael Miguel Alon Protacio50% (2)
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562100% (1)
- Chlamydia TrachomatisDocument7 pagesChlamydia TrachomatisDewi SetiawatiNo ratings yet
- Lower Respiratory InfectionsDocument44 pagesLower Respiratory Infectionstummalapalli venkateswara raoNo ratings yet
- Rabies PathophysiologyDocument1 pageRabies PathophysiologyMichael Urrutia100% (1)
- Pathophysiology: Incubation StageDocument3 pagesPathophysiology: Incubation StageWilliam Soneja CalapiniNo ratings yet
- AGE PathophysiologyDocument2 pagesAGE Pathophysiologyjosephcanlas67% (3)
- Concept Map Group 1Document1 pageConcept Map Group 1eric macabiog100% (1)
- Dengue Hemorrhagic Fever PathophysiologyDocument4 pagesDengue Hemorrhagic Fever PathophysiologyKirk Espanol BigstoneNo ratings yet
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocument2 pagesPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaNo ratings yet
- Concepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionDocument9 pagesConcepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionKristine KimNo ratings yet
- Ascariasis: Pathophysiology, Clinical Manifesta7ons and TreatmentDocument9 pagesAscariasis: Pathophysiology, Clinical Manifesta7ons and TreatmentJUAN CAMILO GARCIA ZAPATANo ratings yet
- Dengue Case StudyDocument16 pagesDengue Case StudyJayselle FelipeNo ratings yet
- DengueDocument4 pagesDengueKathleen DimacaliNo ratings yet
- Pcap PathoDocument2 pagesPcap PathoLardel CarayNo ratings yet
- Pathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionDocument2 pagesPathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionStephanie GapuzNo ratings yet
- 4 - PathophysiologyDocument7 pages4 - PathophysiologyApril GiraoNo ratings yet
- Pathophysiology Dengue 2Document4 pagesPathophysiology Dengue 2KatherineNo ratings yet
- Pathophysiology of AmoebiasisDocument1 pagePathophysiology of AmoebiasisCathy AcquiatanNo ratings yet
- GonorrheaDocument7 pagesGonorrheaEköw Santiago JavierNo ratings yet
- Amoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byDocument8 pagesAmoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byJamie JunioNo ratings yet
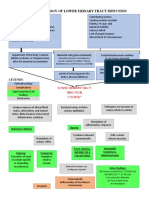
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- PATHOPHYSIOLOGY of DENGUEDocument2 pagesPATHOPHYSIOLOGY of DENGUEKenrick Randell IbanaNo ratings yet
- Chickenpox 1Document7 pagesChickenpox 1Nica Joy CandelarioNo ratings yet
- BAJADO, Allyssa Mae D. Microbiology 1Document25 pagesBAJADO, Allyssa Mae D. Microbiology 1Hernandez SakuraNo ratings yet
- Female Reproductive System: Oleh: Dr. Ilhami Romus, SppaDocument78 pagesFemale Reproductive System: Oleh: Dr. Ilhami Romus, SppaWorldhealthNo ratings yet
- Non-Plaque Induced GingivitisDocument30 pagesNon-Plaque Induced GingivitisDentist AymanNo ratings yet
- A. Pelvic Inflamatory Desease (PID) : PerfringensDocument6 pagesA. Pelvic Inflamatory Desease (PID) : PerfringensMegan LewisNo ratings yet
- Bacterial Infections of SkinDocument72 pagesBacterial Infections of SkinSiddharth DashNo ratings yet


























































Download as doc, pdf, or txt
You might also like
- Pathophysiology of PharyngitisDocument1 pagePathophysiology of PharyngitisKRISTINE BULACAN100% (1)
- Feu GP FGTDocument16 pagesFeu GP FGTAla'a Emerald AguamNo ratings yet
- Meningitis PathoDocument2 pagesMeningitis PathoGlenn Asuncion Pagaduan50% (2)
- Pa Tho Physiology of DengueDocument1 pagePa Tho Physiology of Denguesinister17100% (1)
- PATHOPHYSIOLOGY-PTB - FinalDocument1 pagePATHOPHYSIOLOGY-PTB - FinaliamMye100% (1)
- Microbial Diseases of The Skin and Eyes (Microbiology Chapter 21)Document82 pagesMicrobial Diseases of The Skin and Eyes (Microbiology Chapter 21)Katrina Isabel100% (1)
- 1.pathophysiology of MeningitisDocument1 page1.pathophysiology of Meningitisshielamaygo05100% (1)
- Pathophysiology of TuberculosisDocument2 pagesPathophysiology of TuberculosisLeikkaNo ratings yet
- Pathophysiology Acute Pyelonephritis: Precipitating FactorsDocument2 pagesPathophysiology Acute Pyelonephritis: Precipitating Factorsgodwinkent888No ratings yet
- Pathophysiology of Syphilis & GonorrheaDocument14 pagesPathophysiology of Syphilis & GonorrheasourabhNo ratings yet
- Patho DengueDocument3 pagesPatho DengueLindy Shane BoncalesNo ratings yet
- PneumoniaDocument1 pagePneumoniaAyen FornollesNo ratings yet
- Dengue FeverDocument8 pagesDengue Feverramoli1988No ratings yet
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Path o Physiology of SyphilisDocument1 pagePath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- Pathophysiology Acute Bacterial MeningitisDocument2 pagesPathophysiology Acute Bacterial MeningitisNadira Farah PrayogoNo ratings yet
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoNo ratings yet
- Case Study GonorrheaDocument37 pagesCase Study GonorrheaAnge MinguitoNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- Pathophysiology (Book-Based) : CystitisDocument9 pagesPathophysiology (Book-Based) : CystitisIrish EspinosaNo ratings yet
- Pathophysiology of Meningococcal Meningitis and SepticaemiaDocument8 pagesPathophysiology of Meningococcal Meningitis and SepticaemiaEugen TarnovschiNo ratings yet
- Precipitating Factors Predisposing Factors: LegendDocument2 pagesPrecipitating Factors Predisposing Factors: LegendAlvin Dagumbal100% (1)
- D. Pa Tho Physiology of PneumoniaDocument4 pagesD. Pa Tho Physiology of PneumoniaBill Clinton Lamira BabanNo ratings yet
- MeaslesDocument7 pagesMeaslesKarl FloresNo ratings yet
- Pathophysiology of Varicella Zoster Virus-ChickenpoxDocument8 pagesPathophysiology of Varicella Zoster Virus-ChickenpoxXerxes DejitoNo ratings yet
- Malaria PathophysiologyDocument2 pagesMalaria PathophysiologyMaecy PasionNo ratings yet
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraNo ratings yet
- Pathophysiology Dengue Hemorrhagic FeverDocument1 pagePathophysiology Dengue Hemorrhagic FeverShiella Heart Malana100% (1)
- Pathophysiology TBDocument2 pagesPathophysiology TBJhen DeguzmanNo ratings yet
- Non-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The AmericasDocument2 pagesNon-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The Americaschristian quiaoitNo ratings yet
- Hodgkins LymphomaDocument3 pagesHodgkins LymphomaLefe Arvie Dela PeñaNo ratings yet
- Dengue PathophysiologyDocument1 pageDengue PathophysiologyRafael Miguel Alon Protacio50% (2)
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562100% (1)
- Chlamydia TrachomatisDocument7 pagesChlamydia TrachomatisDewi SetiawatiNo ratings yet
- Lower Respiratory InfectionsDocument44 pagesLower Respiratory Infectionstummalapalli venkateswara raoNo ratings yet
- Rabies PathophysiologyDocument1 pageRabies PathophysiologyMichael Urrutia100% (1)
- Pathophysiology: Incubation StageDocument3 pagesPathophysiology: Incubation StageWilliam Soneja CalapiniNo ratings yet
- AGE PathophysiologyDocument2 pagesAGE Pathophysiologyjosephcanlas67% (3)
- Concept Map Group 1Document1 pageConcept Map Group 1eric macabiog100% (1)
- Dengue Hemorrhagic Fever PathophysiologyDocument4 pagesDengue Hemorrhagic Fever PathophysiologyKirk Espanol BigstoneNo ratings yet
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocument2 pagesPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaNo ratings yet
- Concepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionDocument9 pagesConcepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionKristine KimNo ratings yet
- Ascariasis: Pathophysiology, Clinical Manifesta7ons and TreatmentDocument9 pagesAscariasis: Pathophysiology, Clinical Manifesta7ons and TreatmentJUAN CAMILO GARCIA ZAPATANo ratings yet
- Dengue Case StudyDocument16 pagesDengue Case StudyJayselle FelipeNo ratings yet
- DengueDocument4 pagesDengueKathleen DimacaliNo ratings yet
- Pcap PathoDocument2 pagesPcap PathoLardel CarayNo ratings yet
- Pathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionDocument2 pagesPathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionStephanie GapuzNo ratings yet
- 4 - PathophysiologyDocument7 pages4 - PathophysiologyApril GiraoNo ratings yet
- Pathophysiology Dengue 2Document4 pagesPathophysiology Dengue 2KatherineNo ratings yet
- Pathophysiology of AmoebiasisDocument1 pagePathophysiology of AmoebiasisCathy AcquiatanNo ratings yet
- GonorrheaDocument7 pagesGonorrheaEköw Santiago JavierNo ratings yet
- Amoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byDocument8 pagesAmoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byJamie JunioNo ratings yet
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- PATHOPHYSIOLOGY of DENGUEDocument2 pagesPATHOPHYSIOLOGY of DENGUEKenrick Randell IbanaNo ratings yet
- Chickenpox 1Document7 pagesChickenpox 1Nica Joy CandelarioNo ratings yet
- BAJADO, Allyssa Mae D. Microbiology 1Document25 pagesBAJADO, Allyssa Mae D. Microbiology 1Hernandez SakuraNo ratings yet
- Female Reproductive System: Oleh: Dr. Ilhami Romus, SppaDocument78 pagesFemale Reproductive System: Oleh: Dr. Ilhami Romus, SppaWorldhealthNo ratings yet
- Non-Plaque Induced GingivitisDocument30 pagesNon-Plaque Induced GingivitisDentist AymanNo ratings yet
- A. Pelvic Inflamatory Desease (PID) : PerfringensDocument6 pagesA. Pelvic Inflamatory Desease (PID) : PerfringensMegan LewisNo ratings yet
- Bacterial Infections of SkinDocument72 pagesBacterial Infections of SkinSiddharth DashNo ratings yet