Download as pdf or txt
You might also like
- Registration of Additional Qualification 26 1 BDocument8 pagesRegistration of Additional Qualification 26 1 BAnup Kumar BhattacharyaNo ratings yet
- Hospital Document Star Health Insurance Hospital MOU Draft PDFDocument8 pagesHospital Document Star Health Insurance Hospital MOU Draft PDFNamrata SinghNo ratings yet
- Emergency Department Nursing Flow SheetDocument2 pagesEmergency Department Nursing Flow SheetDessi KayNo ratings yet
- Hospital Document Hospital Infrastructure CheckListDocument12 pagesHospital Document Hospital Infrastructure CheckListsrisaravanan100% (1)
- Hospital Empanelment Request Form PDFDocument2 pagesHospital Empanelment Request Form PDFAnonymous JwgyIweP76% (41)
- Hospital Document Hospital Information Form (PSP)Document6 pagesHospital Document Hospital Information Form (PSP)DR.Umesh Patkar0% (1)
- Hospital Document Hospital Information Form (PSP)Document7 pagesHospital Document Hospital Information Form (PSP)DR.Umesh PatkarNo ratings yet
- Antenatal FormDocument1 pageAntenatal Formtami_web2No ratings yet
- Claim Submission Check ListDocument2 pagesClaim Submission Check ListTanmoy Pal ChowdhuryNo ratings yet
- Gestational Diabetes Case Study With Questions For The Undergraduate NurseDocument46 pagesGestational Diabetes Case Study With Questions For The Undergraduate NurseAndrea Donmyer100% (1)
- Solanine Toxin-2Document13 pagesSolanine Toxin-2Daz Jones100% (2)
- Star Health and Allied Insurance Company Limited Tariff Statement - Mini SOC (FINALISED)Document1 pageStar Health and Allied Insurance Company Limited Tariff Statement - Mini SOC (FINALISED)Sanket Sahare100% (1)
- Star Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDocument2 pagesStar Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormManish Kumar100% (2)
- Request Form PDFDocument2 pagesRequest Form PDFManish KumarNo ratings yet
- Vision E-Medi Empanelment Check ListDocument1 pageVision E-Medi Empanelment Check ListvijenderkumarNo ratings yet
- Star Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDocument2 pagesStar Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDeepak Kaushik0% (1)
- Hospital Document Star Health Insurance Hospital MOUDocument9 pagesHospital Document Star Health Insurance Hospital MOUSanket Sahare100% (1)
- Discharge Summary FormatDocument14 pagesDischarge Summary Formatenumula kumarNo ratings yet
- Hospital Document Hospital Empanelment Request FormDocument2 pagesHospital Document Hospital Empanelment Request FormsrisaravananNo ratings yet
- Hospital Document List of Procedures For ANHDocument16 pagesHospital Document List of Procedures For ANHsrisaravanan67% (3)
- Hospital Document Hospital Empanelment Request FormDocument2 pagesHospital Document Hospital Empanelment Request Formsashanka mishra100% (2)
- Rail Concession FormDocument2 pagesRail Concession FormNeel SarkarNo ratings yet
- MOU CanteenDocument3 pagesMOU CanteenT AnandNo ratings yet
- QIC Claim Form ReimbursementDocument1 pageQIC Claim Form ReimbursementJec Amrac25% (4)
- Aggrement Blood BankDocument2 pagesAggrement Blood BankVIKAS PANERINo ratings yet
- Adamjee In-Patient Claim Reimbursement FormDocument2 pagesAdamjee In-Patient Claim Reimbursement Formhashamqazi100% (1)
- Pre-Hospital Assessment Sheet: Triage ScoreDocument2 pagesPre-Hospital Assessment Sheet: Triage Scoreratna purwitasariNo ratings yet
- Molecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassDocument4 pagesMolecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassmeezNo ratings yet
- Deluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingDocument13 pagesDeluxe & Above /others - Single Room A/C Sharing / Single Non A/c General Ward / Multi SharingSanket SahareNo ratings yet
- Abu Dhabi Int'L Marine Sports Club: Service Level Agreement (SLA) ForDocument9 pagesAbu Dhabi Int'L Marine Sports Club: Service Level Agreement (SLA) ForEymen AslanNo ratings yet
- Check ListDocument2 pagesCheck Listtyagi.vishal8323No ratings yet
- 20-Admission of PatientDocument3 pages20-Admission of Patientakositabon100% (1)
- Medical Report FormDocument1 pageMedical Report FormimamNo ratings yet
- Equipment ListDocument1 pageEquipment ListBOOKREADER_NOWNo ratings yet
- Strike Off Whichever Is Not ApplicableDocument1 pageStrike Off Whichever Is Not ApplicableSrisachidanand ShuklaNo ratings yet
- Form 2Document1 pageForm 2info.arnts100% (1)
- Nabh PolicyDocument4 pagesNabh PolicySanjay KadamNo ratings yet
- Memorandum of Understanding: CategoriesDocument2 pagesMemorandum of Understanding: CategoriesIkram Hospital GujratNo ratings yet
- Claims Document Ready ReckonerDocument19 pagesClaims Document Ready ReckonernandukyNo ratings yet
- AIOS Consent Forms Hindi EnglishDocument194 pagesAIOS Consent Forms Hindi EnglishNarendra PandaNo ratings yet
- Primary and Secondary Healthcare DepartmentDocument25 pagesPrimary and Secondary Healthcare Departmentdanesh rangoNo ratings yet
- IRDA - Pre Auth FormDocument6 pagesIRDA - Pre Auth FormarunNo ratings yet
- GIPSADocument37 pagesGIPSAsohalsingh1No ratings yet
- Cashless Consent FormDocument1 pageCashless Consent FormM/s Microtech100% (1)
- 93c0cfcf A0bf 4229 Bb8f 97d2ccffdda0Document8 pages93c0cfcf A0bf 4229 Bb8f 97d2ccffdda0Sanjay KadamNo ratings yet
- NABH AgreementDocument14 pagesNABH AgreementBOOKREADER_NOWNo ratings yet
- High Risks Medicines List: SR.N O Medicines Name Dosage FormsDocument2 pagesHigh Risks Medicines List: SR.N O Medicines Name Dosage FormsrahatNo ratings yet
- MAXsaket1triff1718 PDFDocument143 pagesMAXsaket1triff1718 PDFNeha LolNo ratings yet
- Clinical Pathology: Test Name Result Unit Biological Reference Interval Urine R & MDocument5 pagesClinical Pathology: Test Name Result Unit Biological Reference Interval Urine R & MAbhishek ChaudharyNo ratings yet
- Discharge SummaryDocument4 pagesDischarge SummaryharshitNo ratings yet
- Fatima Jinnah Chest and General Hospital: COVID-19 Test ReportDocument1 pageFatima Jinnah Chest and General Hospital: COVID-19 Test ReportMuhammad IlyasNo ratings yet
- Institute of Nephrourology Victoria Hospital Campus, Bangalore 560 002 Opd Feedback FormDocument1 pageInstitute of Nephrourology Victoria Hospital Campus, Bangalore 560 002 Opd Feedback Formnabh2019 inuNo ratings yet
- Test Description Value(s) Unit(s) Reference Range: Pt/InrDocument2 pagesTest Description Value(s) Unit(s) Reference Range: Pt/InrSuhas KapseNo ratings yet
- MS-001 (2) Clinical Priv Form Urology 2019Document4 pagesMS-001 (2) Clinical Priv Form Urology 2019Athira Rajan100% (1)
- GE Cardiac CCTA Protocol - 042617Document17 pagesGE Cardiac CCTA Protocol - 042617Toufik Toufik100% (1)
- Rajeev Udaiwal BillDocument7 pagesRajeev Udaiwal BillNityanand Bonlya100% (1)
- Investigation FormatDocument2 pagesInvestigation FormatVinoth PaulNo ratings yet
- Donation CircularDocument2 pagesDonation CircularprashanthNo ratings yet
- Declaration Form (Pan Card, Payee Name and Hospital Name)Document1 pageDeclaration Form (Pan Card, Payee Name and Hospital Name)BOOKREADER_NOW100% (1)
- New Patient AdmitDocument2 pagesNew Patient AdmitNetradeep Narayansa DagduNo ratings yet
- Molecular Biology: Test Name Results Units Ref. Range MethodDocument1 pageMolecular Biology: Test Name Results Units Ref. Range MethodNivesh SindhuNo ratings yet
- Dummy BillDocument5 pagesDummy BillBasanta DashNo ratings yet
- By Registered Post /courier: HEGIC-HS-02099Document10 pagesBy Registered Post /courier: HEGIC-HS-02099Deepak KaushikNo ratings yet
- HDFC ERGO General Insurance Company Limited: To, The Service ProviderDocument20 pagesHDFC ERGO General Insurance Company Limited: To, The Service ProviderDeepak KaushikNo ratings yet
- Quality Survey QuestionnaireDocument13 pagesQuality Survey QuestionnaireDeepak KaushikNo ratings yet
- Pre Auth Part CDocument9 pagesPre Auth Part CDeepak KaushikNo ratings yet
- PPN Declaration LetterDocument1 pagePPN Declaration LetterDeepak KaushikNo ratings yet
- Star Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDocument2 pagesStar Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDeepak Kaushik0% (1)
- Chinese Fragrant Qigong: Qigong Association of America 27133 Forest Springs Lane Corvallis, OR 97330Document28 pagesChinese Fragrant Qigong: Qigong Association of America 27133 Forest Springs Lane Corvallis, OR 97330mardones100% (3)
- Probiotic Efficiency of Spirulina Platensis - Stimulating Growth of Lactic Acid BacteriaDocument4 pagesProbiotic Efficiency of Spirulina Platensis - Stimulating Growth of Lactic Acid BacteriastanleystNo ratings yet
- Psychology Sham)Document5 pagesPsychology Sham)Rey MendozaNo ratings yet
- Amazing Tamarind Health Benefits For MenDocument9 pagesAmazing Tamarind Health Benefits For MenElena Watson100% (1)
- Zinc OxideDocument4 pagesZinc OxideyundayundaaNo ratings yet
- Name: Switchword Pairs: Application/Description Switchword Pairs Add - Info. (If Applicable)Document8 pagesName: Switchword Pairs: Application/Description Switchword Pairs Add - Info. (If Applicable)shrinidhik@gmailcom100% (1)
- Policy WordingsDocument15 pagesPolicy Wordingsmohit07441No ratings yet
- SandostatinDocument3 pagesSandostatinTarek yahiaNo ratings yet
- Top 200 DrugsDocument9 pagesTop 200 DrugsSachin KumarNo ratings yet
- Common ICD 10 CodesDocument2 pagesCommon ICD 10 CodesAhmadNo ratings yet
- Kelompok Dan Nama Ilmiah Kaderisasi 2019Document3 pagesKelompok Dan Nama Ilmiah Kaderisasi 2019Yopi NurhikmahNo ratings yet
- CHRAM Report - June 2010Document17 pagesCHRAM Report - June 2010franckmartin86No ratings yet
- A Universal Model of Diagnostic Reasoning.14Document7 pagesA Universal Model of Diagnostic Reasoning.14Emília SantocheNo ratings yet
- Paclitaxel HandoutDocument5 pagesPaclitaxel HandoutFikaNo ratings yet
- Final Bio Botany Material8.8.22emDocument352 pagesFinal Bio Botany Material8.8.22emGAMING WITH STARNo ratings yet
- Annotated Bibliography - Marijuana LegalizationDocument9 pagesAnnotated Bibliography - Marijuana Legalizationapi-311263095100% (1)
- Common Tests During PregnancyDocument7 pagesCommon Tests During Pregnancyrraja2k2No ratings yet
- англ (MY FUTURE PROFESSION)Document2 pagesангл (MY FUTURE PROFESSION)настяNo ratings yet
- Insurance Batch 2Document14 pagesInsurance Batch 2Radel LlagasNo ratings yet
- Stomach and Intestine Lesson 15Document25 pagesStomach and Intestine Lesson 15Nicholson SalgadoNo ratings yet
- Computer Vision-Based Plant Disease Identification System A Review PDFDocument20 pagesComputer Vision-Based Plant Disease Identification System A Review PDFarjun105flashNo ratings yet
- Varna Swareeyam of Charaka Indriya Sthana - An Explorative StudyDocument26 pagesVarna Swareeyam of Charaka Indriya Sthana - An Explorative StudyPrasad MamidiNo ratings yet
- An Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownDocument35 pagesAn Introduction To Haematopoiesis Prof Vernon Louw Clinical Haematology University of Cape TownAmmaarah IsaacsNo ratings yet
- The Acceptability of Manzanita Fruit As A TeaDocument17 pagesThe Acceptability of Manzanita Fruit As A TeaRinalyn MedranoNo ratings yet
- Electronic Bulletin: International Civil Aviation OrganizationDocument13 pagesElectronic Bulletin: International Civil Aviation OrganizationRohit JoshiNo ratings yet
- Case Study-ASTHMADocument19 pagesCase Study-ASTHMAFritzielove BayawaNo ratings yet
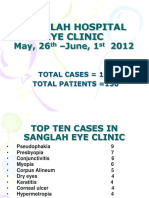
- SanglahDocument13 pagesSanglahIzzarIzzarNo ratings yet
- Hematocolpos Secondary To Imperforate Hymen: Clinical ImagesDocument2 pagesHematocolpos Secondary To Imperforate Hymen: Clinical ImagesQonny WelendriNo ratings yet