Download as docx, pdf, or txt
You might also like
- Swab ResultDocument1 pageSwab ResultPrince Calimbo VillaNo ratings yet
- Epilepsia EpicongressDocument245 pagesEpilepsia EpicongressВасилий КоптеловNo ratings yet
- Presentation 1Document31 pagesPresentation 1Nice YouNo ratings yet
- TUMOR MATA FX TranslateDocument34 pagesTUMOR MATA FX TranslateAisyahNo ratings yet
- Melanoma (Rosai)Document11 pagesMelanoma (Rosai)Eldimson BermudoNo ratings yet
- OM Lecture 1Document12 pagesOM Lecture 1abood kofahiNo ratings yet
- وسام عوض Benign Skin Tumor-5 (Muhadharaty)Document6 pagesوسام عوض Benign Skin Tumor-5 (Muhadharaty)Alaa AhmedNo ratings yet
- Skin Cancer ShowDocument57 pagesSkin Cancer ShowNice YouNo ratings yet
- Skin CancerDocument5 pagesSkin CancerEl FaroukNo ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- Open Access Textbook of General Surgery: Melanoma Jej KrigeDocument6 pagesOpen Access Textbook of General Surgery: Melanoma Jej KrigeZakkiyah PatelNo ratings yet
- Melanoma MalignaDocument28 pagesMelanoma MalignaDila Muflikhy PutriNo ratings yet
- Skin LesionDocument23 pagesSkin Lesion5alifa55No ratings yet
- Melanotic Lesions of Head and Neck RegionDocument66 pagesMelanotic Lesions of Head and Neck RegionAshish VyasNo ratings yet
- Rich Text Editor FileDocument1 pageRich Text Editor FilePeter AbikoyeNo ratings yet
- Benign Skin LesionsDocument109 pagesBenign Skin Lesionsrinaldy IX9No ratings yet
- Benignskinlesions 141227191914 Conversion Gate01 PDFDocument109 pagesBenignskinlesions 141227191914 Conversion Gate01 PDFrinaldy IX9No ratings yet
- Benign and Malignant Tumor of The Oral CavityDocument82 pagesBenign and Malignant Tumor of The Oral CavitymelNo ratings yet
- Skin Cancers: Assistant Larisa PoroshinaDocument42 pagesSkin Cancers: Assistant Larisa PoroshinaMed PoxNo ratings yet
- Histologic Criteria For Diagnosing Primary Cutaneous Malignant MelanomaDocument7 pagesHistologic Criteria For Diagnosing Primary Cutaneous Malignant Melanomadaniel satyoNo ratings yet
- 08-Skin TumoursDocument8 pages08-Skin TumoursChris Tan100% (1)
- TumourDocument7 pagesTumourعلي احمد جواد حسينNo ratings yet
- Skin Tumors: Dr. Ihsan Al-Turfy Consultant Dermatologist College of Medicine/Baghdad MBCHB, DDV, Ficms, CabdDocument149 pagesSkin Tumors: Dr. Ihsan Al-Turfy Consultant Dermatologist College of Medicine/Baghdad MBCHB, DDV, Ficms, CabdRomi WijiantoNo ratings yet
- Skin TumDocument9 pagesSkin TumElsa OctaviaNo ratings yet
- Skin Cancers. Malignant MelanomaDocument53 pagesSkin Cancers. Malignant MelanomaАбдул Насер МохаммадізмаелNo ratings yet
- Skin CancersDocument39 pagesSkin CancersNatz BatzNo ratings yet
- Malignant Epithelial Non-Odontogenic Tumors 2Document11 pagesMalignant Epithelial Non-Odontogenic Tumors 2samamustafa.2003No ratings yet
- Malignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologyDocument50 pagesMalignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologypriyaNo ratings yet
- Orofacial PigmentationsDocument86 pagesOrofacial PigmentationsFadwa El-FeituriNo ratings yet
- Lésions Pigmentées VulvairesDocument9 pagesLésions Pigmentées VulvairesMarande LisaNo ratings yet
- Skin CancerDocument7 pagesSkin Cancerعبدالعزيز احمد علي عتشNo ratings yet
- Managing Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDocument15 pagesManaging Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDian Ariska SNo ratings yet
- 3.skin PathologyDocument38 pages3.skin PathologyFaisal MehboobNo ratings yet
- Nevus Spitz - Everlasting Diagnostic Difficulties - The ReviewDocument6 pagesNevus Spitz - Everlasting Diagnostic Difficulties - The ReviewCristi PopescuNo ratings yet
- Lighter Shades of Pale-The Histopathology of Disorders of PigmentationDocument17 pagesLighter Shades of Pale-The Histopathology of Disorders of Pigmentationdr.syafril SpJPNo ratings yet
- Nonsquamous Cell Malignant Tumours of The Oral Cavity: An OverviewDocument6 pagesNonsquamous Cell Malignant Tumours of The Oral Cavity: An Overviewranggadr0% (1)
- Tumor of The EyeDocument40 pagesTumor of The EyeGustiAngriAngalan100% (1)
- NEOPLASMA GANAS KULIT KBKDocument51 pagesNEOPLASMA GANAS KULIT KBKSisca FeronikaNo ratings yet
- Leg, Arm, and Chest Papules: ERM ASEDocument9 pagesLeg, Arm, and Chest Papules: ERM ASEdeenutz93No ratings yet
- 7 Tumor KulitDocument102 pages7 Tumor KulitRyo RyozNo ratings yet
- Cancerous Lesion in Oral: DRG Rina Kartika Sari SPPM Departemen Ilmu Penyakit Mulut FKG UnissulaDocument50 pagesCancerous Lesion in Oral: DRG Rina Kartika Sari SPPM Departemen Ilmu Penyakit Mulut FKG UnissulamufiNo ratings yet
- Pigmented Skin LesionsDocument51 pagesPigmented Skin LesionsclikgoNo ratings yet
- Skin DiseasesDocument11 pagesSkin DiseasesPipoy Amy100% (1)
- 21 Benign Skin TumorsDocument4 pages21 Benign Skin TumorsAbdul Ghaffar AbdullahNo ratings yet
- Disorders of Pigmentation: John C. Mavropoulos and Bernard A. CohenDocument21 pagesDisorders of Pigmentation: John C. Mavropoulos and Bernard A. Cohendeby sepangNo ratings yet
- Benign Skin TumoursDocument7 pagesBenign Skin TumoursMan LorNo ratings yet
- 7 - Skin TumorsDocument56 pages7 - Skin TumorsRazane AbouzaidNo ratings yet
- MRCPCH - Important Skin DiseasesDocument42 pagesMRCPCH - Important Skin DiseasesarjumandNo ratings yet
- Skin CancersDocument46 pagesSkin CancersHadi AbdulhadiNo ratings yet
- BenignDocument63 pagesBenignAFREEN SADAFNo ratings yet
- Epithelium IIDocument44 pagesEpithelium IIRanjit DanielNo ratings yet
- Congenital and Hereditary Skin DisorderDocument85 pagesCongenital and Hereditary Skin DisorderNwosu Ogbonna GabrielNo ratings yet
- Eye Pathology: Dr. Jusuf FantoniDocument8 pagesEye Pathology: Dr. Jusuf Fantonitutor tujuhNo ratings yet
- 7 Tumor KulitDocument102 pages7 Tumor KulitTher RayNo ratings yet
- Dermal and Subcutaneous TumorsDocument76 pagesDermal and Subcutaneous Tumorsreeves_coolNo ratings yet
- Melanocytic TumorsDocument11 pagesMelanocytic TumorsalfonsoNo ratings yet
- Anatomi Dan Fisiologi KuliitDocument40 pagesAnatomi Dan Fisiologi KuliitZulfani AdhiyatmiNo ratings yet
- Pigmented Lesions of The Skin That You Must Diagnose With ConfidenceDocument23 pagesPigmented Lesions of The Skin That You Must Diagnose With ConfidenceDeba P SarmaNo ratings yet
- Tumors of The Eye: Antony Halim I4061162030Document64 pagesTumors of The Eye: Antony Halim I4061162030Bella Faradiska YuandaNo ratings yet
- 2.11.1 Benign and Malignant Skin LesionsDocument14 pages2.11.1 Benign and Malignant Skin LesionsZayan SyedNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Guide To Implementation: A Guide To The Implementation of The WHO Multimodal Hand Hygiene Improvement StrategyDocument4 pagesGuide To Implementation: A Guide To The Implementation of The WHO Multimodal Hand Hygiene Improvement StrategyNuzhah Al-idrusNo ratings yet
- 13.30 DR Arunraj Navaratnarajah - The Septic PatientDocument49 pages13.30 DR Arunraj Navaratnarajah - The Septic PatientagusNo ratings yet
- Medication AdministrationDocument134 pagesMedication Administrationaryanmohamad210No ratings yet
- EDSC2019 Scientific ProgramDocument6 pagesEDSC2019 Scientific Programheart911hotmail.comNo ratings yet
- Muta LikDocument4 pagesMuta Likoral pathNo ratings yet
- Human Herpes VirusesDocument40 pagesHuman Herpes Virusesfiea241089No ratings yet
- Cahokia Heights EPA ComplaintDocument2 pagesCahokia Heights EPA ComplaintKavahn MansouriNo ratings yet
- Topic OutlineDocument4 pagesTopic OutlineQuitet GutibNo ratings yet
- Shoulder DysfociaDocument92 pagesShoulder DysfociaKagomie SaskieNo ratings yet
- Infection of The Urinary Tract: Campbell-Walsh 11th ED, CH12Document109 pagesInfection of The Urinary Tract: Campbell-Walsh 11th ED, CH12Sirawit Namkaeng ChoksuchatNo ratings yet
- Gastric CáncerDocument206 pagesGastric CáncerjorgehogNo ratings yet
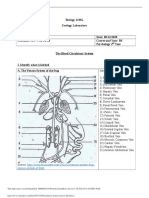
- Circulatory System Answer SheetDocument4 pagesCirculatory System Answer SheetMarlie TobiseNo ratings yet
- Environmental ListeriaDocument5 pagesEnvironmental ListeriaAlifah MauludinahNo ratings yet
- Neurological Disorders - SIMCLEXDocument10 pagesNeurological Disorders - SIMCLEXLLLJJJNo ratings yet
- Hospital Pharmacy - LECTURE 8Document34 pagesHospital Pharmacy - LECTURE 8Anish Kumar A100% (1)
- Full Programme 9Document18 pagesFull Programme 9Borneo CTVSNo ratings yet
- Localisation of Spinal Cord LesionsDocument218 pagesLocalisation of Spinal Cord LesionsGoh Sheen YeeNo ratings yet
- Switching To Risankizumab From Ustekinumab or Adalimumab in Plaque Psoriasis Patients Improves PASI and DLQI Outcomes For Sub Optimal RespondersDocument8 pagesSwitching To Risankizumab From Ustekinumab or Adalimumab in Plaque Psoriasis Patients Improves PASI and DLQI Outcomes For Sub Optimal RespondersPablo OliveraNo ratings yet
- Human Health Risk AssessmentDocument4 pagesHuman Health Risk AssessmentfakharNo ratings yet
- Maternal Quiz NotesDocument79 pagesMaternal Quiz NotesPasay Trisha Faye Y.No ratings yet
- GL Valvole CardiacheDocument49 pagesGL Valvole CardiacheAFA.BLSNo ratings yet
- Cepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishDocument2 pagesCepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishTchouala DentrishNo ratings yet
- Abdominal Trauma - Dr. Febiansyah Ibrahim, SPB-KBDDocument32 pagesAbdominal Trauma - Dr. Febiansyah Ibrahim, SPB-KBDPrandyNo ratings yet
- Roxana Flavia Ilies, Andreea CatanaDocument1 pageRoxana Flavia Ilies, Andreea CatanaLaura CristinaNo ratings yet
- Pretest Intravenous Therapy and Blood Transfusion NCM 118-RLE Part 1. Label The Following. 39 PointsDocument5 pagesPretest Intravenous Therapy and Blood Transfusion NCM 118-RLE Part 1. Label The Following. 39 Pointsgabrielle magdaraogNo ratings yet
- B Braun RegionalanesthesiaportfolioproductcatalogDocument33 pagesB Braun RegionalanesthesiaportfolioproductcatalogMohammad BilalNo ratings yet
- Sem Dial 2021 CRRT PrinciplesDocument8 pagesSem Dial 2021 CRRT PrinciplesArun KumarNo ratings yet
- Determining The Glomerular Filtration Rate: Andani Puspita Rani 1315244Document15 pagesDetermining The Glomerular Filtration Rate: Andani Puspita Rani 1315244AndreasJoviantoNo ratings yet