Download as docx, pdf, or txt
You might also like
- Process Validation ProtocolDocument9 pagesProcess Validation ProtocolBibek Singh Mahat86% (7)
- BSBMGT517 Assessment 3 - Operational Plan: Assessment Tasks and InstructionsDocument7 pagesBSBMGT517 Assessment 3 - Operational Plan: Assessment Tasks and InstructionsArmughan Bukhari0% (1)
- BS en Iso 1833-12-2010Document12 pagesBS en Iso 1833-12-2010EmkFataAliraqNo ratings yet
- Lecture 8 Beam Deposition TechnologyDocument24 pagesLecture 8 Beam Deposition Technologyshanur begulajiNo ratings yet
- CPDD-ACC-02 Rev 01 App For Accreditation of CPD ProgramDocument2 pagesCPDD-ACC-02 Rev 01 App For Accreditation of CPD Programmcnap.2024No ratings yet
- Accreditation of CPD ProgramDocument14 pagesAccreditation of CPD ProgramBryan Delos ReyesNo ratings yet
- ACFrOgALFWz8xas JWbCIMCqNzs6l7XTFvP8z HNqoM7 MUOugJxl1CrfzyrfILTXCVuhykno4SeQx43zT3ePzOszb4xjH ZxoTucCM XXb4LTOmArVXzur TlXBQcADocument4 pagesACFrOgALFWz8xas JWbCIMCqNzs6l7XTFvP8z HNqoM7 MUOugJxl1CrfzyrfILTXCVuhykno4SeQx43zT3ePzOszb4xjH ZxoTucCM XXb4LTOmArVXzur TlXBQcAgarryNo ratings yet
- CPDD-02 Rev 03 CPD ProgramDocument2 pagesCPDD-02 Rev 03 CPD ProgramLiza MelendrezNo ratings yet
- Application Program CPDD 02 Rev 03 CPD ProgramDocument2 pagesApplication Program CPDD 02 Rev 03 CPD ProgramMarkLouiseSumugatOlandresNo ratings yet
- Cpdd-02 Rev 03 CPD ProgramDocument2 pagesCpdd-02 Rev 03 CPD ProgramKristee Ann KellyNo ratings yet
- Critical Organ FailureDocument5 pagesCritical Organ FailureRichelle FrondaNo ratings yet
- RM 005 S. 2020 PRC CPD Accreditation Updates Reminders For The Department of Education Regional Offices PDFDocument14 pagesRM 005 S. 2020 PRC CPD Accreditation Updates Reminders For The Department of Education Regional Offices PDFJOSE ROVIC VILLARINNo ratings yet
- Application For Crediting of Self-Directed and Lifelong LearningDocument2 pagesApplication For Crediting of Self-Directed and Lifelong LearningDerice TancincoNo ratings yet
- Latest Forms Attachment To TESDA Circular On PCT 2016.docx DOCSDocument32 pagesLatest Forms Attachment To TESDA Circular On PCT 2016.docx DOCSAko Lang PohNo ratings yet
- Internship Regulations: of TheDocument6 pagesInternship Regulations: of TheMostafa Ayman Mohammed NageebNo ratings yet
- CPD ProgramDocument2 pagesCPD ProgramCadornaNo ratings yet
- CPD Council For - : Application For Crediting of Self Directed and / or Lifelong LearningDocument2 pagesCPD Council For - : Application For Crediting of Self Directed and / or Lifelong Learningjade ferolinoNo ratings yet
- Regional Centre, NoidaDocument5 pagesRegional Centre, Noidabedsheet73No ratings yet
- CPDD-03 Rev 04 Self Directed Edited ArdmDocument2 pagesCPDD-03 Rev 04 Self Directed Edited ArdmMarinel June PalerNo ratings yet
- SID-CPD-03 Rev 02 Self DirectedDocument2 pagesSID-CPD-03 Rev 02 Self DirectedJeff Tingin MarceloNo ratings yet
- CPD Application FormDocument2 pagesCPD Application FormLuwalhati JusonNo ratings yet
- CPDD-02 Application For CPD ProgramDocument2 pagesCPDD-02 Application For CPD ProgramSMVP TrainingNo ratings yet
- Final Year Project SEM I 2016/2017 Safe Work ProcedureDocument2 pagesFinal Year Project SEM I 2016/2017 Safe Work ProcedureHa WiNo ratings yet
- IPBT Training For Master Teachers 3Document40 pagesIPBT Training For Master Teachers 3Mary Claire LagartoNo ratings yet
- Program Registration Forms Sea-BasedDocument28 pagesProgram Registration Forms Sea-BasedCharina Marie CaduaNo ratings yet
- PROG 2023 66845 CPD Learning Session 1Document12 pagesPROG 2023 66845 CPD Learning Session 1prc.zamboanga.regulationcpdNo ratings yet
- Final Project Guidelines MCOP-001 For Students 2Document3 pagesFinal Project Guidelines MCOP-001 For Students 2asiyafaiza666No ratings yet
- Final Project Guidelines MCOP-001 For StudentsDocument3 pagesFinal Project Guidelines MCOP-001 For Studentsvim9918No ratings yet
- SITXFIN010 Assessment 3 - ProjectDocument7 pagesSITXFIN010 Assessment 3 - ProjectsolucionesredesecNo ratings yet
- Application For Accreditation of CPD ProgramDocument2 pagesApplication For Accreditation of CPD ProgramRodney SalazarNo ratings yet
- CPD Council For DENTISTRY: Professional Regulation CommissionDocument5 pagesCPD Council For DENTISTRY: Professional Regulation Commission111111No ratings yet
- CPD SID 02 Rev 01 Application Form of CPD ProgramDocument2 pagesCPD SID 02 Rev 01 Application Form of CPD ProgramRodel D Dosano0% (1)
- mCPD-2 Form4AccreditationOfCPDProgramDocument2 pagesmCPD-2 Form4AccreditationOfCPDProgramJinky MacatuladNo ratings yet
- CPDD-02 Rev 03 CPD ProgramDocument2 pagesCPDD-02 Rev 03 CPD ProgramAubrey Tanjueco ValdecantosNo ratings yet
- SID-CPD-05 Rev 02 Completion ReportDocument2 pagesSID-CPD-05 Rev 02 Completion ReportJason toraldeNo ratings yet
- CPD 6 Application FormDocument2 pagesCPD 6 Application FormMj Ong PiersonNo ratings yet
- mCPD-3 Form4CreditingOfSelfDirectedLearningDocument2 pagesmCPD-3 Form4CreditingOfSelfDirectedLearningfigin86893No ratings yet
- REC Form 02Document7 pagesREC Form 02nelleannsoldevillaNo ratings yet
- SITHPAT006 Learner Workbook V1.1Document78 pagesSITHPAT006 Learner Workbook V1.1Rohan ShresthaNo ratings yet
- Logbook Program DiplomaDocument78 pagesLogbook Program DiplomaSai venkata KonaNo ratings yet
- New Era University: On-The-Job Training Activity ChecklistDocument2 pagesNew Era University: On-The-Job Training Activity ChecklistZharlot MendozaNo ratings yet
- ESD F3 Project Proposal A 4Document3 pagesESD F3 Project Proposal A 4JAY CEE SACRONo ratings yet
- APPLICATION FORM FOR OFFICIAL TRANSCRIPTDocument3 pagesAPPLICATION FORM FOR OFFICIAL TRANSCRIPTpranoty karanamNo ratings yet
- On The Job Training Log Book: National University of Science & TechnologyDocument56 pagesOn The Job Training Log Book: National University of Science & TechnologyAwes Sewsa100% (1)
- Ilovepdf MergedDocument24 pagesIlovepdf Mergedmadhudubey011981No ratings yet
- Program Book For Short-Term Internship As On 18-10-2022Document62 pagesProgram Book For Short-Term Internship As On 18-10-2022BaluNo ratings yet
- Notice Guidelines For Final Year Students Regarding Industrial Internship / Project (Idp / Udp) GTU Guidelines For Industrial InternshipDocument8 pagesNotice Guidelines For Final Year Students Regarding Industrial Internship / Project (Idp / Udp) GTU Guidelines For Industrial InternshipBhargav M sNo ratings yet
- Hospitality Management OJT JournalDocument23 pagesHospitality Management OJT JournalMariel PapelleroNo ratings yet
- Student AdmissionDocument1 pageStudent Admissionprojit basuNo ratings yet
- Birukab Tenkir Research ThesisDocument125 pagesBirukab Tenkir Research ThesismamilaburaNo ratings yet
- Apec Engineer Register & International Professional Engineer Register Application For RegistrationDocument3 pagesApec Engineer Register & International Professional Engineer Register Application For RegistrationWidiaNo ratings yet
- Applications Are Invited From Eligible Candidates For The Post of in Prescribed Form Available at WWW - Neeri.res - In, For The Project EntitledDocument4 pagesApplications Are Invited From Eligible Candidates For The Post of in Prescribed Form Available at WWW - Neeri.res - In, For The Project EntitledShailendra Kumar SinghNo ratings yet
- CELDA, JOHN PATRICK M. Practicum Intent Form Rev02 FillableDocument1 pageCELDA, JOHN PATRICK M. Practicum Intent Form Rev02 FillableJohn Patrick CeldaNo ratings yet
- ICPo ESDocument1 pageICPo ESVZhii First-BlueNo ratings yet
- CPDD-05 Rev 04 Completion ReportDocument2 pagesCPDD-05 Rev 04 Completion ReportMary Claire LagartoNo ratings yet
- CHR: Dignity of All CHR: Dignity of AllDocument20 pagesCHR: Dignity of All CHR: Dignity of AllJoseph Jumao-asNo ratings yet
- IphitechDocument8 pagesIphitechJohn ValenciaNo ratings yet
- Procedures Manual On Utpras Nified TVET Program Registration and Accreditation System Program RegistrationDocument1 pageProcedures Manual On Utpras Nified TVET Program Registration and Accreditation System Program Registrationzonge cruzNo ratings yet
- Practicum Form Mid Year Summer 2021Document22 pagesPracticum Form Mid Year Summer 2021Jayson GamoNo ratings yet
- BSBMGT517 Assessment 1 - Short AnswerDocument10 pagesBSBMGT517 Assessment 1 - Short Answerozdiploma assignmentsNo ratings yet
- Office of The Registrar: FM-MSU-IIT-RGTR-008 Iligan Institute of Technology Mindanao State UniversityDocument1 pageOffice of The Registrar: FM-MSU-IIT-RGTR-008 Iligan Institute of Technology Mindanao State UniversityOrlando NaparanNo ratings yet
- Construction Supervisor II: Passbooks Study GuideFrom EverandConstruction Supervisor II: Passbooks Study GuideNo ratings yet
- Jay Mariz Cagas Ramirez: Personal BackgroundDocument2 pagesJay Mariz Cagas Ramirez: Personal BackgroundJeliezle RamirezNo ratings yet
- Cristal Jane A. Doliguez: Trainings & SeminarsDocument3 pagesCristal Jane A. Doliguez: Trainings & SeminarsJeliezle RamirezNo ratings yet
- Ramirez, Jay Mariz CagasDocument2 pagesRamirez, Jay Mariz CagasJeliezle RamirezNo ratings yet
- 2 in 1 SPRAY PENDocument4 pages2 in 1 SPRAY PENJeliezle RamirezNo ratings yet
- I Am A Cheerful Person Who Sees The Bright Side oDocument2 pagesI Am A Cheerful Person Who Sees The Bright Side oJeliezle RamirezNo ratings yet
- 50 Years Data Science by Dave DonohoDocument41 pages50 Years Data Science by Dave DonohoVikram JayaramNo ratings yet
- Itu-T: Gigabit-Capable Passive Optical Networks (GPON) : General CharacteristicsDocument25 pagesItu-T: Gigabit-Capable Passive Optical Networks (GPON) : General CharacteristicsDeyber GómezNo ratings yet
- Sap Service Description For Managed Services Ams English v04 2016Document16 pagesSap Service Description For Managed Services Ams English v04 2016Karthick MNo ratings yet
- 15EC302J Vlsi Lab Students PDFDocument54 pages15EC302J Vlsi Lab Students PDFakaash ramnathNo ratings yet
- Artificial Intelligence:: Implications For Business StrategyDocument12 pagesArtificial Intelligence:: Implications For Business StrategyWilliam PolhmannNo ratings yet
- rx2620 9 8 Install ManualDocument10 pagesrx2620 9 8 Install ManualSladur BgNo ratings yet
- MDR Backlog Ldia090 - 4gDocument1 pageMDR Backlog Ldia090 - 4gJakoba FetindrainibeNo ratings yet
- Case AnalysisDocument3 pagesCase AnalysisPAA KAMAYNo ratings yet
- 1100 Series Magnetic Level Indicator - CAT1596 1Document18 pages1100 Series Magnetic Level Indicator - CAT1596 1Smith CBNo ratings yet
- What Is Data Vault ModellingDocument4 pagesWhat Is Data Vault ModellingnewelljjNo ratings yet
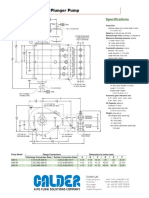
- 300Q-5 Quintuplex Plunger PumpDocument2 pages300Q-5 Quintuplex Plunger PumpJuanNo ratings yet
- Datamax I4208Document134 pagesDatamax I4208rctinkerNo ratings yet
- Groundnut@ShaliniDocument15 pagesGroundnut@Shalinishalini shuklaNo ratings yet
- Business Letter: Focus: - Mechanical Structure - Types of Business Letter - LanguageDocument36 pagesBusiness Letter: Focus: - Mechanical Structure - Types of Business Letter - LanguageNur Rizki ApriliyantoNo ratings yet
- Format Punchlist PDFDocument27 pagesFormat Punchlist PDFDuan Tokcer100% (2)
- Sample Thesis Inventory SystemDocument71 pagesSample Thesis Inventory SystemMary Joy Robles ManalaysayNo ratings yet
- 2020 Calendar Girl Pageant: Fyffe High School CafeteriaDocument3 pages2020 Calendar Girl Pageant: Fyffe High School CafeteriaJamesNo ratings yet
- CHAPTER 6 Muhammad Adi Teo Andri IrmawanDocument3 pagesCHAPTER 6 Muhammad Adi Teo Andri IrmawanMuhammad AditeoNo ratings yet
- TLE Dressmaking 10 Q3 M9Document12 pagesTLE Dressmaking 10 Q3 M9Jusanelle Cangke50% (2)
- Shadman Shahriar 1925389060 - Final Assign - SETADocument2 pagesShadman Shahriar 1925389060 - Final Assign - SETAShadman Shahriar 1925389060No ratings yet
- Scope of Work For Canopy Replacement of DRS/MRS: 1.0 GeneralDocument9 pagesScope of Work For Canopy Replacement of DRS/MRS: 1.0 GeneralDevang PatelNo ratings yet
- Final Population Age Structure, Sex Composition and Rural - Urban CompositionDocument6 pagesFinal Population Age Structure, Sex Composition and Rural - Urban CompositionMaraQuezNo ratings yet
- Twin Otter Manual - EngDocument161 pagesTwin Otter Manual - EngJoe Tateau100% (3)
- Manual KYK 30000Document20 pagesManual KYK 30000Benny ScorpyoNo ratings yet
- BD Food EditDocument9 pagesBD Food EditRashed55No ratings yet
- Yes, Because Goccs Are Essentially Commercial in NatureDocument19 pagesYes, Because Goccs Are Essentially Commercial in NatureAdah Micah PlarisanNo ratings yet
- Offer Letter - InternshipDocument3 pagesOffer Letter - InternshipSameer AhmedNo ratings yet