
Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: 10. Urinary System
Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: 10. Urinary System
You might also like
- Lab Report BioDocument9 pagesLab Report BioArissa SyaminaNo ratings yet
- Nursing TheoristsDocument34 pagesNursing TheoristsTrizza VelosoNo ratings yet
- GCS Assessment Aid English PDFDocument1 pageGCS Assessment Aid English PDFSila OntitaNo ratings yet
- LECTURE 3 - Body Cells and TissuesDocument11 pagesLECTURE 3 - Body Cells and TissuesGGonzales KarlaNo ratings yet
- Guidelines-For-Bsc - New. Physical StructureDocument15 pagesGuidelines-For-Bsc - New. Physical Structurepriyanka bhavsarNo ratings yet
- Assessment of SkinDocument11 pagesAssessment of SkinShreyas WalvekarNo ratings yet
- Note Cards: Marlyn L. Patriarca English Department Maypajo High SchoolDocument8 pagesNote Cards: Marlyn L. Patriarca English Department Maypajo High SchoolMarlyn Laurio-patriarcaNo ratings yet
- A Pre Experimental Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Towards Safe Handling of Chemotherapeutics Drugs Among Staff Nurses in C.H.R.I Gwalior M.PDocument6 pagesA Pre Experimental Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Towards Safe Handling of Chemotherapeutics Drugs Among Staff Nurses in C.H.R.I Gwalior M.PEditor IJTSRDNo ratings yet
- BSC Nursing Syllabus First YearDocument22 pagesBSC Nursing Syllabus First YearDiksha chaudharyNo ratings yet
- Health Assessment 2Document9 pagesHealth Assessment 2Mandira NagNo ratings yet
- Lesson 1 The Evidence Based Practice ModelDocument19 pagesLesson 1 The Evidence Based Practice ModelProject MedbooksNo ratings yet
- Trends in Midwifry and ObstetricsDocument8 pagesTrends in Midwifry and ObstetricsVarna MohanNo ratings yet
- Critique 2Document16 pagesCritique 2Nilesh HudekarNo ratings yet
- BurnDocument30 pagesBurnMamata BeheraNo ratings yet
- Best Stoma Care Service in Pune - Kaizen Gastro CareDocument4 pagesBest Stoma Care Service in Pune - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- Mechanical Ventilation 2015Document18 pagesMechanical Ventilation 2015Nauman GilaniNo ratings yet
- Asthma 1Document33 pagesAsthma 1Dalitso nkhomaNo ratings yet
- Deficiency Diseases - Class 6, Components of FoodDocument5 pagesDeficiency Diseases - Class 6, Components of FoodPriyaNo ratings yet
- Gastrointestinal DrugDocument29 pagesGastrointestinal DrugJeneyse Ajap BalcenaNo ratings yet
- Seminar On Fluids and Electrolyte ImbalanceDocument69 pagesSeminar On Fluids and Electrolyte ImbalanceShib Shankar Roy100% (4)
- PPT - TissuesDocument55 pagesPPT - TissuesTarun Bisen100% (1)
- 05 N259 41199Document17 pages05 N259 41199JyotiNo ratings yet
- An Objective Gives ActionDocument18 pagesAn Objective Gives ActionrinkuNo ratings yet
- NEPHROSISDocument31 pagesNEPHROSISvinnu kalyanNo ratings yet
- Guidelines For Establishment of Nursing CollegeDocument8 pagesGuidelines For Establishment of Nursing CollegeRakesh SharmaNo ratings yet
- 3Document232 pages3Dipeshwari ThakreNo ratings yet
- BR AsthmaDocument17 pagesBR AsthmaAkarsh RamNo ratings yet
- Drug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingDocument12 pagesDrug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingBhoomika PandeyNo ratings yet
- Urinary-Catheterization (1)Document31 pagesUrinary-Catheterization (1)hazel jamisNo ratings yet
- Assessing The Integumentary SystemDocument199 pagesAssessing The Integumentary SystemHyacinth Jane Dela PeñaNo ratings yet
- Machinery, Equipments & LinenDocument73 pagesMachinery, Equipments & Linenbuvan eswarNo ratings yet
- Scopes of Community Health Nursing Education PracticalDocument16 pagesScopes of Community Health Nursing Education PracticalSANCHAYEETANo ratings yet
- BMW Lesson PlanDocument18 pagesBMW Lesson PlanBharat Singh BanshiwalNo ratings yet
- Oxygen Therapy and Administration V2Document32 pagesOxygen Therapy and Administration V2SteffiNo ratings yet
- Educational Preparation: Career Opportunities, Professional Advancement, Role and Scope of Nursing EducationDocument18 pagesEducational Preparation: Career Opportunities, Professional Advancement, Role and Scope of Nursing EducationPinki BarmanNo ratings yet
- Emergency and Disaster Nursing NewDocument42 pagesEmergency and Disaster Nursing Newlalufebrian hendika25No ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- First Year B.Sc. Nursing Question Paper 2007Document11 pagesFirst Year B.Sc. Nursing Question Paper 2007Biju Antony100% (2)
- Case Study On Head InjuryDocument15 pagesCase Study On Head InjuryPriya SinghNo ratings yet
- Clinical Rotation Plan For B.SCDocument1 pageClinical Rotation Plan For B.SCMadhuNo ratings yet
- Excreta DisposalDocument55 pagesExcreta DisposalproddaturNo ratings yet
- Vital Signs and TestingDocument47 pagesVital Signs and TestingRegina Garrard100% (1)
- PDF Unit Plan For Sem 1Document17 pagesPDF Unit Plan For Sem 1Diksha chaudharyNo ratings yet
- Norcet Notes PDFDocument4 pagesNorcet Notes PDFmonishaNo ratings yet
- NCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Document55 pagesNCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Joseph DusichNo ratings yet
- The West Bengal University of Health SciencesDocument9 pagesThe West Bengal University of Health Sciencesbhaskar rayNo ratings yet
- CryotherapyDocument35 pagesCryotherapyRusty RyanNo ratings yet
- Print: Stoma Care Background InformationDocument9 pagesPrint: Stoma Care Background InformationNote3 Note3No ratings yet
- Final ResearchDocument22 pagesFinal ResearchDrPreeti Thakur ChouhanNo ratings yet
- Care Plans-Cholelithiasis NewDocument14 pagesCare Plans-Cholelithiasis NewSUNIL KUMARNo ratings yet
- Paediatric Booklet by Win Nursing CoachingDocument116 pagesPaediatric Booklet by Win Nursing CoachingAkshya YadavNo ratings yet
- Immunization Programme: National Health MissionDocument11 pagesImmunization Programme: National Health MissionAnimaNo ratings yet
- Lesson Plan On: DocumentationDocument8 pagesLesson Plan On: DocumentationNehaNo ratings yet
- Course Planning1Document73 pagesCourse Planning1reshma nejarNo ratings yet
- Lesson Plan On Infection ControlDocument8 pagesLesson Plan On Infection ControlAnonymous hYMWbANo ratings yet
- 01 ProjectDocument30 pages01 Projectkarunyabathula100% (1)
- Glasgow Coma ScaleDocument94 pagesGlasgow Coma Scaleriya priyaNo ratings yet
- Knowledge, Attitude and Practice Exercise During Pregnancy Among Antenatal Mothers at KondencheryDocument8 pagesKnowledge, Attitude and Practice Exercise During Pregnancy Among Antenatal Mothers at KondencheryEditor IJTSRDNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- BloodDocument22 pagesBloodSandeepNo ratings yet
- Digestive SystemDocument57 pagesDigestive SystemnidhichakravortyNo ratings yet
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: EnergeticsDocument8 pagesDr. Naitik D Trivedi & Dr. Upama N. Trivedi: EnergeticsKunal DangatNo ratings yet
- BiochemistryDocument9 pagesBiochemistryKunal DangatNo ratings yet
- Reproductive SystemDocument23 pagesReproductive SystemKunal DangatNo ratings yet
- Computers As Data Analysis in Preclinical Devlopment CA Unit-VDocument13 pagesComputers As Data Analysis in Preclinical Devlopment CA Unit-VKunal DangatNo ratings yet
- Important Short Questions & Answers: Human Anatomy & Physiology HAP 20114Document12 pagesImportant Short Questions & Answers: Human Anatomy & Physiology HAP 20114Kunal DangatNo ratings yet
- HAP - II First ExpDocument8 pagesHAP - II First ExpKunal DangatNo ratings yet
- Continuous Assessment Evs-1Document12 pagesContinuous Assessment Evs-1Kunal DangatNo ratings yet
- Presentation (14) RohitDocument23 pagesPresentation (14) RohitKunal DangatNo ratings yet
- (5145) - 204 First Year B. Pharmacy 1.2.4. Human Anatomy Physiology - Ii (2013 Pattern) (Semester-II)Document2 pages(5145) - 204 First Year B. Pharmacy 1.2.4. Human Anatomy Physiology - Ii (2013 Pattern) (Semester-II)Kunal DangatNo ratings yet
- Harahap S N 2021 - Identifikasi Senyawa Eugenol Pada Buah Jambu Biji DNGN Gc-MsDocument12 pagesHarahap S N 2021 - Identifikasi Senyawa Eugenol Pada Buah Jambu Biji DNGN Gc-MsSeptynelya ThenuNo ratings yet
- PMS Theory Chapter3Document47 pagesPMS Theory Chapter3moulitechNo ratings yet
- NASM21472: National Aerospace StandardDocument10 pagesNASM21472: National Aerospace StandardGeorgeNo ratings yet
- Grundfosliterature 2950863Document82 pagesGrundfosliterature 2950863Paris AnabelNo ratings yet
- LanoPro Multi Grease EP2 MSDSDocument7 pagesLanoPro Multi Grease EP2 MSDSlionelmaroofNo ratings yet
- 8th Science. 9th Bio. 10th ChemDocument25 pages8th Science. 9th Bio. 10th ChemMudassir HussainNo ratings yet
- Toefl StructureDocument7 pagesToefl StructureAdelia DerifniNo ratings yet
- 1.2 Your Science LaboratoryDocument18 pages1.2 Your Science LaboratoryCHAI SZE JIA MoeNo ratings yet
- S1 WEEK 12 ReportDocument12 pagesS1 WEEK 12 ReportMuhammad Bello BabaNo ratings yet
- Alchemy Was A Protoscientific Tradition Practiced in AsiaDocument2 pagesAlchemy Was A Protoscientific Tradition Practiced in AsiaAnonymousNo ratings yet
- AQA GCSE Combined Science Chemistry Paper 1 Higher Question PaperDocument17 pagesAQA GCSE Combined Science Chemistry Paper 1 Higher Question PaperSharmila MaheswaranNo ratings yet
- 2017 Manual-CH1202Document24 pages2017 Manual-CH1202Anuraj LahaNo ratings yet
- 2-Chemistry For Civil EngineersDocument6 pages2-Chemistry For Civil EngineersYusf ari jerjisNo ratings yet
- Specimen MS - Paper 1 OCR Chemistry As-LevelDocument17 pagesSpecimen MS - Paper 1 OCR Chemistry As-LevelAbdullah HassanyNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument17 pagesSafety Data Sheet: 1. IdentificationFina Mustika SimanjuntakNo ratings yet
- Duoline20 API BrochDocument4 pagesDuoline20 API BrochredaNo ratings yet
- CV - Thomas Lee - Aug 2023Document5 pagesCV - Thomas Lee - Aug 2023jacobNo ratings yet
- Cetiol Sensoft (OPP)Document1 pageCetiol Sensoft (OPP)paromanikNo ratings yet
- Perawatan Kolom GCDocument12 pagesPerawatan Kolom GCRafi Pratama SetiawanNo ratings yet
- Tonomet RI Tonomet RI: Oleh: Dr. Ibnu Gilang Syawali Oleh: Dr. Ibnu Gilang SyawaliDocument12 pagesTonomet RI Tonomet RI: Oleh: Dr. Ibnu Gilang Syawali Oleh: Dr. Ibnu Gilang SyawaliIbnu Gilang SyawaliNo ratings yet
- Cambridge O Level: Chemistry 5070/12Document16 pagesCambridge O Level: Chemistry 5070/12Raahin RahimNo ratings yet
- EsabbbDocument2 pagesEsabbbkismikloshun55No ratings yet
- Senior Biology 1 Q1 - M9 For PrintingDocument41 pagesSenior Biology 1 Q1 - M9 For PrintingMARIBETH RAMOSNo ratings yet
- jfnr06 2 p047 054 Mlichova PDFDocument8 pagesjfnr06 2 p047 054 Mlichova PDFTatum NilamsariNo ratings yet
- Iec TS 62073-2016Document24 pagesIec TS 62073-2016Marco IllanesNo ratings yet
- Composite 1Document27 pagesComposite 1jenan h.albayatiiNo ratings yet
- 3 Steps To Clean MoneyDocument3 pages3 Steps To Clean Moneykhan AliNo ratings yet
- Stress Analysis of Polycarbonate Spur Gears For Sugarcane Juice Machine Using FEADocument6 pagesStress Analysis of Polycarbonate Spur Gears For Sugarcane Juice Machine Using FEAOptimuz TsNo ratings yet
- Sample Question PaperDocument8 pagesSample Question Paperpr gamingNo ratings yet
































































































Download as pdf or txt
You might also like
- Lab Report BioDocument9 pagesLab Report BioArissa SyaminaNo ratings yet
- Nursing TheoristsDocument34 pagesNursing TheoristsTrizza VelosoNo ratings yet
- GCS Assessment Aid English PDFDocument1 pageGCS Assessment Aid English PDFSila OntitaNo ratings yet
- LECTURE 3 - Body Cells and TissuesDocument11 pagesLECTURE 3 - Body Cells and TissuesGGonzales KarlaNo ratings yet
- Guidelines-For-Bsc - New. Physical StructureDocument15 pagesGuidelines-For-Bsc - New. Physical Structurepriyanka bhavsarNo ratings yet
- Assessment of SkinDocument11 pagesAssessment of SkinShreyas WalvekarNo ratings yet
- Note Cards: Marlyn L. Patriarca English Department Maypajo High SchoolDocument8 pagesNote Cards: Marlyn L. Patriarca English Department Maypajo High SchoolMarlyn Laurio-patriarcaNo ratings yet
- A Pre Experimental Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Towards Safe Handling of Chemotherapeutics Drugs Among Staff Nurses in C.H.R.I Gwalior M.PDocument6 pagesA Pre Experimental Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Towards Safe Handling of Chemotherapeutics Drugs Among Staff Nurses in C.H.R.I Gwalior M.PEditor IJTSRDNo ratings yet
- BSC Nursing Syllabus First YearDocument22 pagesBSC Nursing Syllabus First YearDiksha chaudharyNo ratings yet
- Health Assessment 2Document9 pagesHealth Assessment 2Mandira NagNo ratings yet
- Lesson 1 The Evidence Based Practice ModelDocument19 pagesLesson 1 The Evidence Based Practice ModelProject MedbooksNo ratings yet
- Trends in Midwifry and ObstetricsDocument8 pagesTrends in Midwifry and ObstetricsVarna MohanNo ratings yet
- Critique 2Document16 pagesCritique 2Nilesh HudekarNo ratings yet
- BurnDocument30 pagesBurnMamata BeheraNo ratings yet
- Best Stoma Care Service in Pune - Kaizen Gastro CareDocument4 pagesBest Stoma Care Service in Pune - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- Mechanical Ventilation 2015Document18 pagesMechanical Ventilation 2015Nauman GilaniNo ratings yet
- Asthma 1Document33 pagesAsthma 1Dalitso nkhomaNo ratings yet
- Deficiency Diseases - Class 6, Components of FoodDocument5 pagesDeficiency Diseases - Class 6, Components of FoodPriyaNo ratings yet
- Gastrointestinal DrugDocument29 pagesGastrointestinal DrugJeneyse Ajap BalcenaNo ratings yet
- Seminar On Fluids and Electrolyte ImbalanceDocument69 pagesSeminar On Fluids and Electrolyte ImbalanceShib Shankar Roy100% (4)
- PPT - TissuesDocument55 pagesPPT - TissuesTarun Bisen100% (1)
- 05 N259 41199Document17 pages05 N259 41199JyotiNo ratings yet
- An Objective Gives ActionDocument18 pagesAn Objective Gives ActionrinkuNo ratings yet
- NEPHROSISDocument31 pagesNEPHROSISvinnu kalyanNo ratings yet
- Guidelines For Establishment of Nursing CollegeDocument8 pagesGuidelines For Establishment of Nursing CollegeRakesh SharmaNo ratings yet
- 3Document232 pages3Dipeshwari ThakreNo ratings yet
- BR AsthmaDocument17 pagesBR AsthmaAkarsh RamNo ratings yet
- Drug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingDocument12 pagesDrug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingBhoomika PandeyNo ratings yet
- Urinary-Catheterization (1)Document31 pagesUrinary-Catheterization (1)hazel jamisNo ratings yet
- Assessing The Integumentary SystemDocument199 pagesAssessing The Integumentary SystemHyacinth Jane Dela PeñaNo ratings yet
- Machinery, Equipments & LinenDocument73 pagesMachinery, Equipments & Linenbuvan eswarNo ratings yet
- Scopes of Community Health Nursing Education PracticalDocument16 pagesScopes of Community Health Nursing Education PracticalSANCHAYEETANo ratings yet
- BMW Lesson PlanDocument18 pagesBMW Lesson PlanBharat Singh BanshiwalNo ratings yet
- Oxygen Therapy and Administration V2Document32 pagesOxygen Therapy and Administration V2SteffiNo ratings yet
- Educational Preparation: Career Opportunities, Professional Advancement, Role and Scope of Nursing EducationDocument18 pagesEducational Preparation: Career Opportunities, Professional Advancement, Role and Scope of Nursing EducationPinki BarmanNo ratings yet
- Emergency and Disaster Nursing NewDocument42 pagesEmergency and Disaster Nursing Newlalufebrian hendika25No ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- First Year B.Sc. Nursing Question Paper 2007Document11 pagesFirst Year B.Sc. Nursing Question Paper 2007Biju Antony100% (2)
- Case Study On Head InjuryDocument15 pagesCase Study On Head InjuryPriya SinghNo ratings yet
- Clinical Rotation Plan For B.SCDocument1 pageClinical Rotation Plan For B.SCMadhuNo ratings yet
- Excreta DisposalDocument55 pagesExcreta DisposalproddaturNo ratings yet
- Vital Signs and TestingDocument47 pagesVital Signs and TestingRegina Garrard100% (1)
- PDF Unit Plan For Sem 1Document17 pagesPDF Unit Plan For Sem 1Diksha chaudharyNo ratings yet
- Norcet Notes PDFDocument4 pagesNorcet Notes PDFmonishaNo ratings yet
- NCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Document55 pagesNCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Joseph DusichNo ratings yet
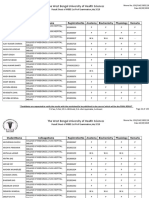
- The West Bengal University of Health SciencesDocument9 pagesThe West Bengal University of Health Sciencesbhaskar rayNo ratings yet
- CryotherapyDocument35 pagesCryotherapyRusty RyanNo ratings yet
- Print: Stoma Care Background InformationDocument9 pagesPrint: Stoma Care Background InformationNote3 Note3No ratings yet
- Final ResearchDocument22 pagesFinal ResearchDrPreeti Thakur ChouhanNo ratings yet
- Care Plans-Cholelithiasis NewDocument14 pagesCare Plans-Cholelithiasis NewSUNIL KUMARNo ratings yet
- Paediatric Booklet by Win Nursing CoachingDocument116 pagesPaediatric Booklet by Win Nursing CoachingAkshya YadavNo ratings yet
- Immunization Programme: National Health MissionDocument11 pagesImmunization Programme: National Health MissionAnimaNo ratings yet
- Lesson Plan On: DocumentationDocument8 pagesLesson Plan On: DocumentationNehaNo ratings yet
- Course Planning1Document73 pagesCourse Planning1reshma nejarNo ratings yet
- Lesson Plan On Infection ControlDocument8 pagesLesson Plan On Infection ControlAnonymous hYMWbANo ratings yet
- 01 ProjectDocument30 pages01 Projectkarunyabathula100% (1)
- Glasgow Coma ScaleDocument94 pagesGlasgow Coma Scaleriya priyaNo ratings yet
- Knowledge, Attitude and Practice Exercise During Pregnancy Among Antenatal Mothers at KondencheryDocument8 pagesKnowledge, Attitude and Practice Exercise During Pregnancy Among Antenatal Mothers at KondencheryEditor IJTSRDNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- BloodDocument22 pagesBloodSandeepNo ratings yet
- Digestive SystemDocument57 pagesDigestive SystemnidhichakravortyNo ratings yet
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: EnergeticsDocument8 pagesDr. Naitik D Trivedi & Dr. Upama N. Trivedi: EnergeticsKunal DangatNo ratings yet
- BiochemistryDocument9 pagesBiochemistryKunal DangatNo ratings yet
- Reproductive SystemDocument23 pagesReproductive SystemKunal DangatNo ratings yet
- Computers As Data Analysis in Preclinical Devlopment CA Unit-VDocument13 pagesComputers As Data Analysis in Preclinical Devlopment CA Unit-VKunal DangatNo ratings yet
- Important Short Questions & Answers: Human Anatomy & Physiology HAP 20114Document12 pagesImportant Short Questions & Answers: Human Anatomy & Physiology HAP 20114Kunal DangatNo ratings yet
- HAP - II First ExpDocument8 pagesHAP - II First ExpKunal DangatNo ratings yet
- Continuous Assessment Evs-1Document12 pagesContinuous Assessment Evs-1Kunal DangatNo ratings yet
- Presentation (14) RohitDocument23 pagesPresentation (14) RohitKunal DangatNo ratings yet
- (5145) - 204 First Year B. Pharmacy 1.2.4. Human Anatomy Physiology - Ii (2013 Pattern) (Semester-II)Document2 pages(5145) - 204 First Year B. Pharmacy 1.2.4. Human Anatomy Physiology - Ii (2013 Pattern) (Semester-II)Kunal DangatNo ratings yet
- Harahap S N 2021 - Identifikasi Senyawa Eugenol Pada Buah Jambu Biji DNGN Gc-MsDocument12 pagesHarahap S N 2021 - Identifikasi Senyawa Eugenol Pada Buah Jambu Biji DNGN Gc-MsSeptynelya ThenuNo ratings yet
- PMS Theory Chapter3Document47 pagesPMS Theory Chapter3moulitechNo ratings yet
- NASM21472: National Aerospace StandardDocument10 pagesNASM21472: National Aerospace StandardGeorgeNo ratings yet
- Grundfosliterature 2950863Document82 pagesGrundfosliterature 2950863Paris AnabelNo ratings yet
- LanoPro Multi Grease EP2 MSDSDocument7 pagesLanoPro Multi Grease EP2 MSDSlionelmaroofNo ratings yet
- 8th Science. 9th Bio. 10th ChemDocument25 pages8th Science. 9th Bio. 10th ChemMudassir HussainNo ratings yet
- Toefl StructureDocument7 pagesToefl StructureAdelia DerifniNo ratings yet
- 1.2 Your Science LaboratoryDocument18 pages1.2 Your Science LaboratoryCHAI SZE JIA MoeNo ratings yet
- S1 WEEK 12 ReportDocument12 pagesS1 WEEK 12 ReportMuhammad Bello BabaNo ratings yet
- Alchemy Was A Protoscientific Tradition Practiced in AsiaDocument2 pagesAlchemy Was A Protoscientific Tradition Practiced in AsiaAnonymousNo ratings yet
- AQA GCSE Combined Science Chemistry Paper 1 Higher Question PaperDocument17 pagesAQA GCSE Combined Science Chemistry Paper 1 Higher Question PaperSharmila MaheswaranNo ratings yet
- 2017 Manual-CH1202Document24 pages2017 Manual-CH1202Anuraj LahaNo ratings yet
- 2-Chemistry For Civil EngineersDocument6 pages2-Chemistry For Civil EngineersYusf ari jerjisNo ratings yet
- Specimen MS - Paper 1 OCR Chemistry As-LevelDocument17 pagesSpecimen MS - Paper 1 OCR Chemistry As-LevelAbdullah HassanyNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument17 pagesSafety Data Sheet: 1. IdentificationFina Mustika SimanjuntakNo ratings yet
- Duoline20 API BrochDocument4 pagesDuoline20 API BrochredaNo ratings yet
- CV - Thomas Lee - Aug 2023Document5 pagesCV - Thomas Lee - Aug 2023jacobNo ratings yet
- Cetiol Sensoft (OPP)Document1 pageCetiol Sensoft (OPP)paromanikNo ratings yet
- Perawatan Kolom GCDocument12 pagesPerawatan Kolom GCRafi Pratama SetiawanNo ratings yet
- Tonomet RI Tonomet RI: Oleh: Dr. Ibnu Gilang Syawali Oleh: Dr. Ibnu Gilang SyawaliDocument12 pagesTonomet RI Tonomet RI: Oleh: Dr. Ibnu Gilang Syawali Oleh: Dr. Ibnu Gilang SyawaliIbnu Gilang SyawaliNo ratings yet
- Cambridge O Level: Chemistry 5070/12Document16 pagesCambridge O Level: Chemistry 5070/12Raahin RahimNo ratings yet
- EsabbbDocument2 pagesEsabbbkismikloshun55No ratings yet
- Senior Biology 1 Q1 - M9 For PrintingDocument41 pagesSenior Biology 1 Q1 - M9 For PrintingMARIBETH RAMOSNo ratings yet
- jfnr06 2 p047 054 Mlichova PDFDocument8 pagesjfnr06 2 p047 054 Mlichova PDFTatum NilamsariNo ratings yet
- Iec TS 62073-2016Document24 pagesIec TS 62073-2016Marco IllanesNo ratings yet
- Composite 1Document27 pagesComposite 1jenan h.albayatiiNo ratings yet
- 3 Steps To Clean MoneyDocument3 pages3 Steps To Clean Moneykhan AliNo ratings yet
- Stress Analysis of Polycarbonate Spur Gears For Sugarcane Juice Machine Using FEADocument6 pagesStress Analysis of Polycarbonate Spur Gears For Sugarcane Juice Machine Using FEAOptimuz TsNo ratings yet
- Sample Question PaperDocument8 pagesSample Question Paperpr gamingNo ratings yet