Download as pdf or txt
You might also like
- VAC Swachh Bharat - 230612 - 155724Document14 pagesVAC Swachh Bharat - 230612 - 155724Tera Kal92% (13)
- Delhi's Street Food and Its Impact On EconomyDocument25 pagesDelhi's Street Food and Its Impact On Economyhitesh mendirattaNo ratings yet
- Color Climax Teenage Sex No 21 1981 PDFDocument2 pagesColor Climax Teenage Sex No 21 1981 PDFLeon10% (10)
- Periodontal Treatment of Excessive Gingival DisplayDocument12 pagesPeriodontal Treatment of Excessive Gingival DisplayJuan Carlos CárcamoNo ratings yet
- Sinha's Comprehensive Anxiety Test (SCAT)Document9 pagesSinha's Comprehensive Anxiety Test (SCAT)Pragya100% (13)
- User Manual ECG EDAN SE-3Document104 pagesUser Manual ECG EDAN SE-3Andreé Montúfar100% (1)
- SMJv2168 174basel 2Document8 pagesSMJv2168 174basel 2ريام الموسويNo ratings yet
- Gumy SmileDocument8 pagesGumy Smiledr. gusfarizNo ratings yet
- Monaco 2005Document8 pagesMonaco 2005Django BoyeeNo ratings yet
- Gummy Smile - Diag and Treatment PlanDocument3 pagesGummy Smile - Diag and Treatment PlanalazharadelNo ratings yet
- Diagnosisandtreatment Approachestoa"Gummy Smile": Harry Dym,, Robert Pierre IiDocument9 pagesDiagnosisandtreatment Approachestoa"Gummy Smile": Harry Dym,, Robert Pierre Ii刘雨樵No ratings yet
- Lip Reposition Surgery A New Call in PeriodonticsDocument4 pagesLip Reposition Surgery A New Call in PeriodonticsMaysaa mahdiNo ratings yet
- Gummy Smile or Surgical or Ortho PDFDocument19 pagesGummy Smile or Surgical or Ortho PDFHenry MandalasNo ratings yet
- Gummy Smile and Its Management: Review ArticleDocument8 pagesGummy Smile and Its Management: Review Articleريام الموسويNo ratings yet
- 10.21307 - Aoj 2020 021Document11 pages10.21307 - Aoj 2020 021Saumya SinghNo ratings yet
- Al Ammar 2018Document9 pagesAl Ammar 2018Wayan Sutresna YasaNo ratings yet
- Digital Smile Design ConceptDocument19 pagesDigital Smile Design ConceptDiego GomesNo ratings yet
- Smile Analysis What To MeasureDocument6 pagesSmile Analysis What To MeasureAli RazaNo ratings yet
- Case ReportDocument8 pagesCase ReportrtyNo ratings yet
- Periodontal Esthetic Surgery To Improve A Natural Smile Report Case With 2 Year Follow UpDocument5 pagesPeriodontal Esthetic Surgery To Improve A Natural Smile Report Case With 2 Year Follow UpzooooeNo ratings yet
- Articulo Smile DesignDocument17 pagesArticulo Smile DesignmonicaordonezNo ratings yet
- Calamia JR, Et Al. Smile Design and Treatment Planning With The Help of A Comprehensive Esthetic Evaluation Form. Dent Clin North Am. 2011Document24 pagesCalamia JR, Et Al. Smile Design and Treatment Planning With The Help of A Comprehensive Esthetic Evaluation Form. Dent Clin North Am. 2011justin4leNo ratings yet
- Extract Pages From 74425 - FixedDocument20 pagesExtract Pages From 74425 - Fixeddrgayen6042No ratings yet
- Thesis On Smile AnalysisDocument8 pagesThesis On Smile Analysiscoawokugg100% (2)
- Evaluation of Different EstheticDocument8 pagesEvaluation of Different EstheticSebastián BernalNo ratings yet
- Smile PhotographDocument7 pagesSmile Photographpopat78No ratings yet
- Smile EstheticsDocument7 pagesSmile EstheticsAnuNo ratings yet
- l51482 Copy 150416082242 Conversion Gate02Document6 pagesl51482 Copy 150416082242 Conversion Gate02ريام الموسويNo ratings yet
- Excessive Gingival Display - FinalDocument11 pagesExcessive Gingival Display - FinalPhilippe Bocanegra FernándezNo ratings yet
- Facial Aesthetics 2Document9 pagesFacial Aesthetics 2Putri Morteza100% (1)
- Jco - 2005 03 155Document14 pagesJco - 2005 03 155ريام الموسويNo ratings yet
- The Relationship Between The Lip Length and SmileDocument5 pagesThe Relationship Between The Lip Length and SmileanushiNo ratings yet
- Rationale of Total Arch Intrusion For Gummy Smile CorrectionDocument16 pagesRationale of Total Arch Intrusion For Gummy Smile CorrectionJair OliveiraNo ratings yet
- Wal Drop 2008Document12 pagesWal Drop 2008César RodríguezNo ratings yet
- Digital Smile Design Concept PDFDocument18 pagesDigital Smile Design Concept PDFAndyRamosLopezNo ratings yet
- Single Phase Correction of Tongue Thrust Habit AloDocument7 pagesSingle Phase Correction of Tongue Thrust Habit AloAkhil SinghNo ratings yet
- The Eight Components of A Balanced SmileDocument13 pagesThe Eight Components of A Balanced SmilemahmoudhamdyelhariryNo ratings yet
- Knowledge About Gummy Smile and Its Treatment Options Among Dental StudentsDocument7 pagesKnowledge About Gummy Smile and Its Treatment Options Among Dental StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Lip Exercises in Orthodontics: A Review Article: April 2022Document11 pagesA Lip Exercises in Orthodontics: A Review Article: April 2022habeebNo ratings yet
- Smile BalancedDocument29 pagesSmile Balancedchirag sahgalNo ratings yet
- Gummy Smile: A Narrative ReviewDocument3 pagesGummy Smile: A Narrative ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impacto IncisivosDocument8 pagesImpacto Incisivoshector rinconNo ratings yet
- Adult Gummy Smile Correction With Temporary Skeletal Anchorage DevicesDocument14 pagesAdult Gummy Smile Correction With Temporary Skeletal Anchorage DevicesMarlon Cespedes AlccaNo ratings yet
- Periodontal Plastic Surgery For Treatment of GummyDocument6 pagesPeriodontal Plastic Surgery For Treatment of GummyLilian CalianiNo ratings yet
- 10.1007@s10006 020 00857 4Document6 pages10.1007@s10006 020 00857 4Martha Lia Castaño EcheverryNo ratings yet
- Smile in Orthodontics: Review: Nikhil Verma, Ashish Garg, Samprita Sahu, Sapna Verma, Neetu Shah, Amit TiwariDocument4 pagesSmile in Orthodontics: Review: Nikhil Verma, Ashish Garg, Samprita Sahu, Sapna Verma, Neetu Shah, Amit TiwariPulkit BimalNo ratings yet
- Pi Is 1073874613000777Document14 pagesPi Is 1073874613000777drzana78No ratings yet
- Lip Lowering SurgeryDocument15 pagesLip Lowering SurgeryPrathik RaiNo ratings yet
- Smile Design: Nicholas C. Davis, DDS, MAGDDocument20 pagesSmile Design: Nicholas C. Davis, DDS, MAGDPriyanka GandhiNo ratings yet
- Smile Line and Periodontium Visibility: Clinical and Research ReportDocument9 pagesSmile Line and Periodontium Visibility: Clinical and Research ReportbkprosthoNo ratings yet
- Triangular Frenotomy A Novel Technique For Gummy Smile CorrectionDocument4 pagesTriangular Frenotomy A Novel Technique For Gummy Smile CorrectionRAKERNAS PDGI XINo ratings yet
- Lecrure 7 Clinical Diagnosis 4th StageDocument16 pagesLecrure 7 Clinical Diagnosis 4th StageIbrahim HysamNo ratings yet
- IMPLANTOLOGÍA. Tarnow Dental Implantology Numbers Clinicians Need To KnowDocument17 pagesIMPLANTOLOGÍA. Tarnow Dental Implantology Numbers Clinicians Need To KnowKenigal14No ratings yet
- Macro, Mini and Microesthetics-AparnaDocument95 pagesMacro, Mini and Microesthetics-AparnaSruthy BlissNo ratings yet
- The Effect of Increasing Vertical Dimension of Occlusion On Facial AestheticsDocument5 pagesThe Effect of Increasing Vertical Dimension of Occlusion On Facial AestheticsWilliam YuwonoNo ratings yet
- A Safe and Effective Lip Augmentation Method: The Step-by-Step Φ (Phi) TechniqueDocument7 pagesA Safe and Effective Lip Augmentation Method: The Step-by-Step Φ (Phi) TechniqueDr. Hilder HernandezNo ratings yet
- A Systematic Diagnostic Scheme For Excessive Gingival Display JCDocument33 pagesA Systematic Diagnostic Scheme For Excessive Gingival Display JCobula reddyNo ratings yet
- Gummy Smile - IntegrativeDocument3 pagesGummy Smile - IntegrativeNingombam Robinson SinghNo ratings yet
- Turk J Orthod 26 58 enDocument7 pagesTurk J Orthod 26 58 enPulkit BimalNo ratings yet
- Periodontal Plastic Surgery To Improve AestheticsDocument7 pagesPeriodontal Plastic Surgery To Improve AestheticsElizabet KalmykovaNo ratings yet
- Lip RepositioningDocument5 pagesLip RepositioningNurul Novita SuhartonoNo ratings yet
- Al Taki 2016Document12 pagesAl Taki 2016Jessi RecaldeNo ratings yet
- Shaping Lips With FillersDocument4 pagesShaping Lips With FillersElaine Medeiros75% (4)
- Aesthetics Revision Very GoodDocument62 pagesAesthetics Revision Very GoodAndre3893No ratings yet
- Various Types of Ligation Ties in Orthodontics: ArticleDocument7 pagesVarious Types of Ligation Ties in Orthodontics: ArticlemeghaNo ratings yet
- One-Phase Versus Two-Phase Treatment: Boston, MassDocument4 pagesOne-Phase Versus Two-Phase Treatment: Boston, MassmeghaNo ratings yet
- Intrusion Mechanics in Orthodontics: A Review: Author List: DR - HarishatramDocument9 pagesIntrusion Mechanics in Orthodontics: A Review: Author List: DR - HarishatrammeghaNo ratings yet
- To Open or To Close Space - That Is The Missing Lateral Incisor QuestionDocument9 pagesTo Open or To Close Space - That Is The Missing Lateral Incisor QuestionmeghaNo ratings yet
- 1.1 Theories of Growth ControlDocument57 pages1.1 Theories of Growth Controlmegha100% (1)
- Theories of Growth Control 2Document77 pagesTheories of Growth Control 2meghaNo ratings yet
- Theories of Growth Control 2Document77 pagesTheories of Growth Control 2meghaNo ratings yet
- POSTERDocument3 pagesPOSTERmeghaNo ratings yet
- J.C Tongue & Malocclusion - Copy (Recovered)Document81 pagesJ.C Tongue & Malocclusion - Copy (Recovered)meghaNo ratings yet
- Introduction To Public HealthDocument9 pagesIntroduction To Public HealthGerard Emmanuel KamdemNo ratings yet
- Business STD QP Set-1Document14 pagesBusiness STD QP Set-1Om ZaveriNo ratings yet
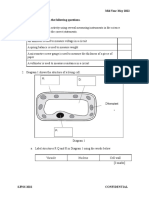
- F2 Mid-Year Exam Section BDocument3 pagesF2 Mid-Year Exam Section BAnne Marian Anak JOSEPHNo ratings yet
- HeroDocument1 pageHeroEdward CullenNo ratings yet
- OB QCGH OPD GuideDocument3 pagesOB QCGH OPD Guidemark100% (1)
- Chapter 05 - Summary NotesDocument4 pagesChapter 05 - Summary NotesNlh NguyễnNo ratings yet
- Leadership Development For Students of Color - KarmaHall Edu (2024)Document1 pageLeadership Development For Students of Color - KarmaHall Edu (2024)marcelNo ratings yet
- Department of Biochemistry - Biochemistry Department - UMDCDocument17 pagesDepartment of Biochemistry - Biochemistry Department - UMDCTuf backlinkingNo ratings yet
- Heat Stress - Temperature - HSEDocument6 pagesHeat Stress - Temperature - HSEZhang ChuangNo ratings yet
- Thermolite 890 Stabilizer - PSSDocument3 pagesThermolite 890 Stabilizer - PSSQwerty RoyalNo ratings yet
- Monitoring and Evaluation ME PlanDocument12 pagesMonitoring and Evaluation ME PlanMirAfghan GhulamiPoorNo ratings yet
- Exercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Document320 pagesExercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Diego CardosoNo ratings yet
- RETRATRUTIDEDocument13 pagesRETRATRUTIDECristobal Alvarado LivacicNo ratings yet
- Mona NasrallahDocument1 pageMona NasrallahWa3d HalabiNo ratings yet
- OXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPDocument73 pagesOXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPChris ZantiraNo ratings yet
- Psycho-Cybernetics by Maxwell MaltzDocument2 pagesPsycho-Cybernetics by Maxwell Maltz杨文博No ratings yet
- The Effects of Sleep Deprivation On Academic Performance of Grade 12 Students in Eastern Visayas State UniversityDocument6 pagesThe Effects of Sleep Deprivation On Academic Performance of Grade 12 Students in Eastern Visayas State UniversityizzvonNo ratings yet
- AH102 Module 3Document50 pagesAH102 Module 3leona edwardsNo ratings yet
- Class IX To XII Students: Times NieDocument4 pagesClass IX To XII Students: Times NiePranavNo ratings yet
- Bioenergetics of Exercising HumansDocument26 pagesBioenergetics of Exercising HumansMasajes A DomicilioNo ratings yet
- Ag Listing 05oct2023Document98 pagesAg Listing 05oct2023kiranduggarajuNo ratings yet
- Pulsed Electro Magnetic Energy (PEME)Document9 pagesPulsed Electro Magnetic Energy (PEME)NATARAJAN KAVITHANo ratings yet
- GPG PS003 Cold Formed BendsDocument80 pagesGPG PS003 Cold Formed BendsNirvana RamkissoonNo ratings yet
- (M. Black, H.W. Pritchard) Desiccation and SurvivaDocument26 pages(M. Black, H.W. Pritchard) Desiccation and SurvivaLuis PedreroNo ratings yet
- Concept Map PDFDocument1 pageConcept Map PDFcaleb andersonNo ratings yet