Download as pdf or txt
You might also like
- Cpje Secrets Preview 2021Document12 pagesCpje Secrets Preview 2021Diana Pham100% (3)
- P66 B1 M5 Lufthansa PDFDocument196 pagesP66 B1 M5 Lufthansa PDFDAVID FAJARDO PUERTO100% (1)
- Compendium of Logistics Policies Volume III PDFDocument219 pagesCompendium of Logistics Policies Volume III PDFDon-Juan Casanova92% (12)
- 10-11 - Anti-Hyperlipidemic Drugs (Summary SAQ and MCQS)Document6 pages10-11 - Anti-Hyperlipidemic Drugs (Summary SAQ and MCQS)Purvak Mahajan100% (1)
- Diabetes Topic DiscussionDocument9 pagesDiabetes Topic DiscussionSamNo ratings yet
- Coagulation DrugsDocument1 pageCoagulation Drugsmed testNo ratings yet
- Antihyperglycemic Agents Comparison Chart PDFDocument9 pagesAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- Type 2 Diabetes Mellitus (T2DM) Adult Treatment PathwayDocument2 pagesType 2 Diabetes Mellitus (T2DM) Adult Treatment PathwayFaidil Akbar100% (1)
- Quick Reference Guide - Management of Diabetes 1 2022 Version FINALDocument20 pagesQuick Reference Guide - Management of Diabetes 1 2022 Version FINALHigh Class Education (H.C.Education)No ratings yet
- DM TYPE 2 by THEADocument29 pagesDM TYPE 2 by THEAThea SelinaNo ratings yet
- DM TTTDocument2 pagesDM TTTBell GatesNo ratings yet
- Mono Dual Triple Therapy DiabetesDocument1 pageMono Dual Triple Therapy DiabetesbharatNo ratings yet
- Diabetes Type 2 Treatment AlgorithmDocument25 pagesDiabetes Type 2 Treatment AlgorithmJ Wong100% (1)
- Table 173-3 - Agents Used For Treatment of Type 1 or Type 2 DiDocument2 pagesTable 173-3 - Agents Used For Treatment of Type 1 or Type 2 DiKiran ShelkeNo ratings yet
- Table 1. Antihyperglycemic Agents For Use in Type 2 DiabetesDocument5 pagesTable 1. Antihyperglycemic Agents For Use in Type 2 DiabeteszeiarraNo ratings yet
- Approach 2024Document25 pagesApproach 2024light tweenNo ratings yet
- Sylfonylurea: Class Generic Trade Store NotesDocument4 pagesSylfonylurea: Class Generic Trade Store NotesMohammadSAL-RawashdehNo ratings yet
- CPG T2DM 6th Edition 2020 13042021Document4 pagesCPG T2DM 6th Edition 2020 13042021harisa yasmanNo ratings yet
- Non Insulin Management of DM - PPTX 2Document33 pagesNon Insulin Management of DM - PPTX 2Meno AliNo ratings yet
- 43 The Importance of Diabetes ManagementDocument33 pages43 The Importance of Diabetes ManagementHarli AMNo ratings yet
- Therapeutics Diabetes DrugchartDocument4 pagesTherapeutics Diabetes DrugchartSharan SahotaNo ratings yet
- ADA 2023.-154-159 - OrganizedDocument6 pagesADA 2023.-154-159 - OrganizedEfren BalsecaNo ratings yet
- Drug Name Mechanism of Action Indication Side Effects Nursing Responsibilities Generic NameDocument2 pagesDrug Name Mechanism of Action Indication Side Effects Nursing Responsibilities Generic NamehahahaNo ratings yet
- Endocrino Unidad 2 Diabetes Cont.Document33 pagesEndocrino Unidad 2 Diabetes Cont.GenesisGissellPlazaQuesadaNo ratings yet
- Manajemen DM Tipe 2 - HBD Idi LabuselDocument40 pagesManajemen DM Tipe 2 - HBD Idi LabuselJunni EdyNo ratings yet
- More : Drug Class How It Works Generic Name Brand Name Cost Type 2 Oral Medications BiguanideDocument4 pagesMore : Drug Class How It Works Generic Name Brand Name Cost Type 2 Oral Medications BiguanideJoshua LewisNo ratings yet
- Drug StudyDocument1 pageDrug StudyGiselle TutorNo ratings yet
- Topiramate: May Decrease Glyburide Levels Colesevelam:decreases The Absorption of SulfonylureasDocument3 pagesTopiramate: May Decrease Glyburide Levels Colesevelam:decreases The Absorption of SulfonylureaserinNo ratings yet
- Non-Insulin Management of Diabetes MellitusDocument15 pagesNon-Insulin Management of Diabetes MellitusrogeracasusoNo ratings yet
- 23-5-2022 Presentation JentadeutoDocument52 pages23-5-2022 Presentation JentadeutofsvtqsNo ratings yet
- DiabetesDocument40 pagesDiabetesA RNo ratings yet
- NENC Regional SGLT2 Top Tips v1.2 NTAG Approved March 2023Document5 pagesNENC Regional SGLT2 Top Tips v1.2 NTAG Approved March 2023Nehal ElnagarNo ratings yet
- Summary Drugs Table - GERR BlockDocument2 pagesSummary Drugs Table - GERR BlockRiley WestwoodNo ratings yet
- Five Steps in Management of DMDocument62 pagesFive Steps in Management of DMarti tyagitaNo ratings yet
- New Dyslipidemia 2021 Naplex QuickDocument2 pagesNew Dyslipidemia 2021 Naplex Quickkaylakmills_1013586883% (6)
- Visual Summary Full Version Choosing Medicines For Firstline and Further Treatment PDF 10956472093Document5 pagesVisual Summary Full Version Choosing Medicines For Firstline and Further Treatment PDF 10956472093BiancaPancuNo ratings yet
- Diabetes MedicationDocument3 pagesDiabetes MedicationRuben Gutierrez-ArizacaNo ratings yet
- SGLT 2Document21 pagesSGLT 2Genix PharmaNo ratings yet
- DPP 4Document20 pagesDPP 4Genix PharmaNo ratings yet
- Step 3 - PharmacologyDocument10 pagesStep 3 - PharmacologyLauren LevyNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Dyslipidemia SummaryDocument6 pagesDyslipidemia SummaryJan Angela BaylonNo ratings yet
- Class Generic Brand MOA Indication: GetrylDocument6 pagesClass Generic Brand MOA Indication: GetrylDr. Sadaf khanNo ratings yet
- Diabetes DrugsDocument1 pageDiabetes Drugsmed testNo ratings yet
- Diabetes and Its Management: Rohit ThanageDocument10 pagesDiabetes and Its Management: Rohit ThanageRohit ThanageNo ratings yet
- The Metabolic Syndrome From Insulin Resistance To Obesity and DiabetesDocument44 pagesThe Metabolic Syndrome From Insulin Resistance To Obesity and DiabetesDwiPutriArlinaNo ratings yet
- Acs Review - Student VersionDocument3 pagesAcs Review - Student Versionapi-549451092No ratings yet
- Diabetes Treatment: PancreatitisDocument2 pagesDiabetes Treatment: PancreatitisSafiya JamesNo ratings yet
- SGLT2 IDocument24 pagesSGLT2 IFiErCeNo ratings yet
- Cardiovascular KBKDocument7 pagesCardiovascular KBKDavid SantosoNo ratings yet
- Diabetes in CKDDocument20 pagesDiabetes in CKDdr_iswahyudhiNo ratings yet
- Updates On Metformin JDM2019 DTDocument37 pagesUpdates On Metformin JDM2019 DTLaurentius JohanNo ratings yet
- Dyslipdiemia 2022Document75 pagesDyslipdiemia 2022LeeNo ratings yet
- Clinical Therapeutics: Case 1Document17 pagesClinical Therapeutics: Case 1NoreenNo ratings yet
- Crash Course 1 StudentDocument1 pageCrash Course 1 Studentapi-648595816No ratings yet
- Oral Antidiabetic DrugsDocument46 pagesOral Antidiabetic Drugscarms100% (1)
- 2020 - Diabetes PharmacotherapyDocument68 pages2020 - Diabetes PharmacotherapyAmal HijaziNo ratings yet
- Diabetes ManagementDocument2 pagesDiabetes ManagementronaldNo ratings yet
- نسخة abdullah alhajri final check 25Document16 pagesنسخة abdullah alhajri final check 25abdulrahman AlrashedNo ratings yet
- LIPIDS Guidance For The Management of Hypertriglyceridaemia July 2018Document2 pagesLIPIDS Guidance For The Management of Hypertriglyceridaemia July 2018siti munajaliahNo ratings yet
- Mounjaro MonographDocument13 pagesMounjaro Monographlu161513No ratings yet
- Communication Aids and Strategies Using Tools of TechnologyDocument14 pagesCommunication Aids and Strategies Using Tools of TechnologyJussel CataloNo ratings yet
- Vibration LectureDocument49 pagesVibration LectureMark Oliver BernardoNo ratings yet
- TITLE: Distillation and Hardness of Water AbstractDocument4 pagesTITLE: Distillation and Hardness of Water AbstractnotmeNo ratings yet
- FullereneDocument12 pagesFullereneapi-249970885No ratings yet
- Currency Detection For Blind PeopleDocument19 pagesCurrency Detection For Blind Peoplehaffah1245No ratings yet
- KPI FormulaDocument3 pagesKPI FormulaSrikant GuptaNo ratings yet
- Business Math AssignmentDocument4 pagesBusiness Math AssignmentiamshowrovNo ratings yet
- Fire Protection Valves: Effective March 18, 2013 - Supercedes FPP-0312 of March 26, 2012Document8 pagesFire Protection Valves: Effective March 18, 2013 - Supercedes FPP-0312 of March 26, 2012Jorge Alberto Martinez OrtizNo ratings yet
- Multi Evaporator System With Single Compressor and Individual Expansion ValveDocument4 pagesMulti Evaporator System With Single Compressor and Individual Expansion ValveALL THE GOOD STUFFNo ratings yet
- Assignment Management System: Project Report OnDocument68 pagesAssignment Management System: Project Report OnAnuj Kumar SinghNo ratings yet
- Timothy StainbrookDocument1 pageTimothy Stainbrookapi-548131304No ratings yet
- Fruits and Veg SCMDocument11 pagesFruits and Veg SCMamoldhawanNo ratings yet
- Adult PSG Guidelines 2014Document49 pagesAdult PSG Guidelines 2014mohanNo ratings yet
- Coralia AntenasDocument3 pagesCoralia AntenasALEX_125No ratings yet
- Cleanroom Design GOODDocument135 pagesCleanroom Design GOODtony manyookNo ratings yet
- BGBA Membership ProcedureDocument2 pagesBGBA Membership ProceduremizanacmaNo ratings yet
- Procedures For Reimbursement of Expenses Relating To Official TravelsDocument14 pagesProcedures For Reimbursement of Expenses Relating To Official TravelsNeringa Gudelevičiūtė - PolitienėNo ratings yet
- KaksbsjsusnsklsDocument244 pagesKaksbsjsusnsklskevin0% (1)
- Colors and Effects - PSG Pigment Preparations PolyolefinsDocument24 pagesColors and Effects - PSG Pigment Preparations PolyolefinsBoonyarit LurdgrienggraiyingNo ratings yet
- AbanDocument12 pagesAbanIsmar MorenoNo ratings yet
- XdealSkin Vitamins Tiktok ProposalDocument4 pagesXdealSkin Vitamins Tiktok ProposalElixia KiteNo ratings yet
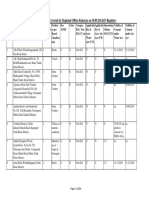
- List of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)Document284 pagesList of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)mutton moonswamiNo ratings yet
- Berklee Drum Notation FinaleDocument25 pagesBerklee Drum Notation Finalenbelane100% (2)
- Astm D 4258Document2 pagesAstm D 4258anthonybarnard100% (1)
- City Builder 10 - Governmental PlacesDocument30 pagesCity Builder 10 - Governmental Placesskypalae86% (7)
- Invaders Around The World in 2018Document18 pagesInvaders Around The World in 2018RVLEBNo ratings yet
- Evolution of Media PPT FinalDocument50 pagesEvolution of Media PPT FinalRoxette SantillanNo ratings yet
- Q2-COT-LP-Health7 - Wk4 (Malnutrition and Micronutrients Deficiency)Document4 pagesQ2-COT-LP-Health7 - Wk4 (Malnutrition and Micronutrients Deficiency)ivonneNo ratings yet