Download as doc, pdf, or txt
You might also like
- Amputations and Ex ArticulationsDocument24 pagesAmputations and Ex ArticulationsTesmal FernandoNo ratings yet
- UW Ped Clerkship Final Exam From CLIPP CasesDocument4 pagesUW Ped Clerkship Final Exam From CLIPP CasesJoe ConeNo ratings yet
- 1 s2.0 S0891842207000249 Main PDFDocument14 pages1 s2.0 S0891842207000249 Main PDFAnonymous kdBDppigENo ratings yet
- Pi Is 2212628717302013Document5 pagesPi Is 2212628717302013DrManoj JagarlamudiNo ratings yet
- Lowe Limb AmputationDocument11 pagesLowe Limb AmputationNadya ZahraNo ratings yet
- Lower Limb AmputationDocument37 pagesLower Limb AmputationUhuebor David0% (1)
- Combat Foot and Ankle Trauma: LT Scott M. Tintle, MD, CDR John J. Keeling, MD, and LTC Scott B. Shawen, MDDocument7 pagesCombat Foot and Ankle Trauma: LT Scott M. Tintle, MD, CDR John J. Keeling, MD, and LTC Scott B. Shawen, MDbaljinderNo ratings yet
- Partial FootDocument15 pagesPartial FootpascallindaNo ratings yet
- DEFINATION: Amputation Is The Removal of ADocument22 pagesDEFINATION: Amputation Is The Removal of AsurchadNo ratings yet
- Surgical Management of Severe Lower Extremity Injury - UpToDate PDFDocument46 pagesSurgical Management of Severe Lower Extremity Injury - UpToDate PDFRáisa Camilo FerreiraNo ratings yet
- 24.amputations of The Foot and AnkleDocument29 pages24.amputations of The Foot and AnklesteoeviciNo ratings yet
- Amputation: DefinitionDocument9 pagesAmputation: DefinitionCharaNo ratings yet
- AmpitutionDocument21 pagesAmpitutionIqra ZulfiqarNo ratings yet
- P and o SelfDocument443 pagesP and o SelfDeepa SeiraNo ratings yet
- Closure of Major Diabetic Foot Wounds and Defects With External FixationDocument10 pagesClosure of Major Diabetic Foot Wounds and Defects With External FixationAnonymous kdBDppigENo ratings yet
- SymeDocument5 pagesSymepascallindaNo ratings yet
- Ch31 Amputación MSDocument34 pagesCh31 Amputación MSAstra LuzNo ratings yet
- Amputatii - GeneralitatiDocument23 pagesAmputatii - GeneralitatiBogdan BurcheciNo ratings yet
- AmputationDocument75 pagesAmputationFaith LoveNo ratings yet
- Amputation: Mangled Extremity Severity Score (MESS) I. Skeletal and Soft Tissue Injury PointsDocument4 pagesAmputation: Mangled Extremity Severity Score (MESS) I. Skeletal and Soft Tissue Injury PointsMalueth AnguiNo ratings yet
- Cuadricepsplastia MipiDocument5 pagesCuadricepsplastia MipiVictor HernandezNo ratings yet
- Amputation-Dr N K BeheraDocument8 pagesAmputation-Dr N K BeheraSheel GuptaNo ratings yet
- Anatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisDocument5 pagesAnatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisMoustafa MohamedNo ratings yet
- Selected Instructional Course LecturesDocument27 pagesSelected Instructional Course LecturesAhmad ShakirNo ratings yet
- Fractures of Thetibial PlafondDocument21 pagesFractures of Thetibial PlafondMario Esteban Muñoz RojasNo ratings yet
- Serletti 2001Document13 pagesSerletti 2001Phùng HiểnNo ratings yet
- Medialepıkondıl DırsekDocument6 pagesMedialepıkondıl DırsekMehmetali Seçil UysalNo ratings yet
- Clinicas de Endocrino. Pie Diabetico - Dic 2013Document15 pagesClinicas de Endocrino. Pie Diabetico - Dic 2013Betzabeth RodriguezNo ratings yet
- AMPUTATIONDocument73 pagesAMPUTATIONmohammad farhanNo ratings yet
- Percutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezDocument12 pagesPercutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezNuno Craveiro LopesNo ratings yet
- Amputation EngDocument6 pagesAmputation EngKholifa FitriaNo ratings yet
- Management of The Mangled ExtremityDocument10 pagesManagement of The Mangled ExtremityosteonectinNo ratings yet
- The Syme Amputation SX Technique and Prosthetic Management JFAS 1994Document14 pagesThe Syme Amputation SX Technique and Prosthetic Management JFAS 1994Evan BowlesNo ratings yet
- Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCDocument15 pagesMinimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCchhabraanNo ratings yet
- Diaphyseal Femur FracturesDocument9 pagesDiaphyseal Femur FracturesSoulmates1No ratings yet
- Fractures of The Tibial PlafondDocument21 pagesFractures of The Tibial PlafondCamila FontechaNo ratings yet
- Amputation and The Fitting of Artificial Limbs 1945Document67 pagesAmputation and The Fitting of Artificial Limbs 1945alex1973maNo ratings yet
- PIIS2212628721001900Document6 pagesPIIS2212628721001900ANDRES DURANNo ratings yet
- Fai 2011 0818Document4 pagesFai 2011 0818Mohamed GoudaNo ratings yet
- Surgicaltreatmentof Intra-Articularcalcaneal Fractures: John J. Stapleton,, Thomas ZgonisDocument8 pagesSurgicaltreatmentof Intra-Articularcalcaneal Fractures: John J. Stapleton,, Thomas Zgonisthzone1986No ratings yet
- Kneemliinjuries: Common Problems and SolutionsDocument11 pagesKneemliinjuries: Common Problems and SolutionsHenry CollazosNo ratings yet
- Clavicle Fracture: Signs and SymptomsDocument4 pagesClavicle Fracture: Signs and SymptomsbvlbvlNo ratings yet
- Acute Forefoot and Midfoot InjuriesDocument8 pagesAcute Forefoot and Midfoot InjuriesAJ CésarNo ratings yet
- Surgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDDocument9 pagesSurgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDGustavoBecerraNo ratings yet
- Acute Compartment Syndrome of The Lower Leg: Retrospective Study On Prevalence, Technique, and Outcome of FasciotomiesDocument5 pagesAcute Compartment Syndrome of The Lower Leg: Retrospective Study On Prevalence, Technique, and Outcome of FasciotomiesTHE.GUNNERSNo ratings yet
- Tibia Fractures Overview - StatPearls - NCBI BookshelfDocument6 pagesTibia Fractures Overview - StatPearls - NCBI BookshelfVivi DeviyanaNo ratings yet
- Surgical Guideline of Femur FracturesDocument13 pagesSurgical Guideline of Femur FractureswangNo ratings yet
- 25.lower Limb ProstheticsDocument24 pages25.lower Limb ProstheticsThomas Walker100% (1)
- 8 Ankle SprainDocument11 pages8 Ankle Sprainapi-241264935No ratings yet
- Rotational Flap Closure of 1st and 5nth Met HeadDocument8 pagesRotational Flap Closure of 1st and 5nth Met HeadleahbayNo ratings yet
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- Arthroscopic Arthrolysis of Stiff ElbowDocument5 pagesArthroscopic Arthrolysis of Stiff ElbowMoustafa MohamedNo ratings yet
- SVNIRTAR Module 1-24 - Compiled by Sanlap Kundu (MPT Neuro) PDFDocument626 pagesSVNIRTAR Module 1-24 - Compiled by Sanlap Kundu (MPT Neuro) PDFArchita AgarwalNo ratings yet
- AmputationDocument4 pagesAmputationFalah IsmailNo ratings yet
- Musculoskeletal TrumaDocument30 pagesMusculoskeletal TrumaadnanreshunNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic InjuriesvikramNo ratings yet
- The Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASDocument5 pagesThe Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASdamonenNo ratings yet
- Use of External Fixation in The Reconstruction of The Charcot Foot and AnkleDocument21 pagesUse of External Fixation in The Reconstruction of The Charcot Foot and AnkleAnonymous kdBDppigENo ratings yet
- Acetabular Fractures in Older Patients: Assessment and ManagementFrom EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Internal Fixation of Distal Fibula Fractures JFAS 1995Document9 pagesInternal Fixation of Distal Fibula Fractures JFAS 1995Evan BowlesNo ratings yet
- Symes Amputation - Yu JAPMADocument23 pagesSymes Amputation - Yu JAPMAEvan BowlesNo ratings yet
- The Syme Amputation SX Technique and Prosthetic Management JFAS 1994Document14 pagesThe Syme Amputation SX Technique and Prosthetic Management JFAS 1994Evan BowlesNo ratings yet
- Torsion of The Human Achilles Tendon JFAS 1996Document11 pagesTorsion of The Human Achilles Tendon JFAS 1996Evan BowlesNo ratings yet
- Repair of Neglected Achilles Tendon Ruptures JFAS 1994Document8 pagesRepair of Neglected Achilles Tendon Ruptures JFAS 1994Evan BowlesNo ratings yet
- Surgery For Chronic Achilles Tendon Problems JFAS 1995Document7 pagesSurgery For Chronic Achilles Tendon Problems JFAS 1995Evan BowlesNo ratings yet
- Reconstruction of An Achilles Tendon Defect Utilizing An Achilles Tendon Allograft JFAS 1996Document8 pagesReconstruction of An Achilles Tendon Defect Utilizing An Achilles Tendon Allograft JFAS 1996Evan BowlesNo ratings yet
- Multiple Ruptures of The Tendo Achillis JFAS 1992Document17 pagesMultiple Ruptures of The Tendo Achillis JFAS 1992Evan BowlesNo ratings yet
- Long Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Document5 pagesLong Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Evan BowlesNo ratings yet
- Pathologic Afflictions of The Achilles Tendon JFAS 1991Document8 pagesPathologic Afflictions of The Achilles Tendon JFAS 1991Evan BowlesNo ratings yet
- Critical Analysis of Tendo Achillis Repair Using Achilles Tendon Rupture Classification System and RepaiDocument8 pagesCritical Analysis of Tendo Achillis Repair Using Achilles Tendon Rupture Classification System and RepaiEvan BowlesNo ratings yet
- Old Testament: in The Beginning God Created..Document1 pageOld Testament: in The Beginning God Created..Evan BowlesNo ratings yet
- A Severe Acute Achilles Rupture and Repair JFAS 1995Document5 pagesA Severe Acute Achilles Rupture and Repair JFAS 1995Evan BowlesNo ratings yet
- Accessory Soleus Muscle Simulating A Soft Tissue Tumor of The Posteromedial Ankle Region JFAS 1991Document3 pagesAccessory Soleus Muscle Simulating A Soft Tissue Tumor of The Posteromedial Ankle Region JFAS 1991Evan BowlesNo ratings yet
- Achilles Tendon Rupture in Athletes Histochem of Triceps Surae JFAS 1991Document7 pagesAchilles Tendon Rupture in Athletes Histochem of Triceps Surae JFAS 1991Evan BowlesNo ratings yet
- Calcified Tendo Achillis Insertion New SX Approach JFAS 1991Document4 pagesCalcified Tendo Achillis Insertion New SX Approach JFAS 1991Evan BowlesNo ratings yet
- 8635 20240219210812 PrescriptionDocument2 pages8635 20240219210812 PrescriptionRana BiswasNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic HyperplasiajustmiitmiideeNo ratings yet
- Rcsi Mini Med ProgrammeDocument1 pageRcsi Mini Med Programmeapi-531313826No ratings yet
- Class1 and 2Document16 pagesClass1 and 2api-263590842No ratings yet
- Freezing in ParkinsonDocument14 pagesFreezing in ParkinsonGermaine Sperberg DuhartNo ratings yet
- Epistaxis 2019Document20 pagesEpistaxis 2019dr MohammedNo ratings yet
- SURG 32 1st PartDocument2 pagesSURG 32 1st PartTheeya QuigaoNo ratings yet
- Pertemuan 9 Arista PDFDocument12 pagesPertemuan 9 Arista PDFNi Putu aristaNo ratings yet
- NursingDocument98 pagesNursingLAWRENCE MARI SANTELLA0% (1)
- Pancreatic Cancer Early Detection, Diagnosis, and StagingDocument29 pagesPancreatic Cancer Early Detection, Diagnosis, and StagingDokter LinggauNo ratings yet
- Pucat Dan Anemia Pada AnakDocument21 pagesPucat Dan Anemia Pada AnakHerry WaraNo ratings yet
- Comparison Between Manual Procedure and Automated For Determinant of Wbcs and PCV in Maternity and Labor Hospital in Karbala CityDocument3 pagesComparison Between Manual Procedure and Automated For Determinant of Wbcs and PCV in Maternity and Labor Hospital in Karbala Cityyousrazeidan1979No ratings yet
- Clinical: Contact Allergy To Cinnamon: Case ReportDocument4 pagesClinical: Contact Allergy To Cinnamon: Case ReportGrace Victoria OctavianusNo ratings yet
- Complications of Post PartumDocument69 pagesComplications of Post PartumSN Tee100% (1)
- Skeptical Inquirer - November-December 2022-4Document5 pagesSkeptical Inquirer - November-December 2022-4matildaNo ratings yet
- Dental CertificateDocument2 pagesDental Certificatesherlyn de guzman100% (1)
- President Kaguta Museveni's Speech On Covid-19 As of 18 June 2021Document26 pagesPresident Kaguta Museveni's Speech On Covid-19 As of 18 June 2021The Campus TimesNo ratings yet
- FIX - Fracture and DislocationDocument80 pagesFIX - Fracture and DislocationWildan Hilmi AnsoriNo ratings yet
- Clinical Rotation Handbook 2021Document22 pagesClinical Rotation Handbook 2021Tony Allday0% (1)
- Antiviral and Healing Potential of Sambucus Nigra Extracts: Review / Artículo de RevisiónDocument7 pagesAntiviral and Healing Potential of Sambucus Nigra Extracts: Review / Artículo de RevisiónJuliana LondoñoNo ratings yet
- Sciencefairreserchpaper LogankushnerDocument5 pagesSciencefairreserchpaper Logankushnerapi-347582278No ratings yet
- Do You Have ADHD or OCD Amen Clinics PDFDocument1 pageDo You Have ADHD or OCD Amen Clinics PDFJessica Therese TranNo ratings yet
- Silodosin 1Document7 pagesSilodosin 1Akhmad MustafaNo ratings yet
- Shi 2021Document11 pagesShi 2021szt.stevensNo ratings yet
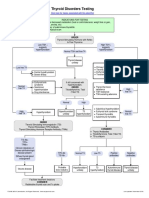
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Continuous EEG Monitoring in The Intensive Care UnDocument7 pagesContinuous EEG Monitoring in The Intensive Care UnSara MendesNo ratings yet
- Anderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinDocument4 pagesAnderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinОлександр БайдоNo ratings yet
- Q&ADocument45 pagesQ&AElba De Asis Manacob0% (1)
- Postoperative Care in MedicalDocument5 pagesPostoperative Care in MedicalMark Russel Sean LealNo ratings yet