
Psycho-Oncology - 2018 - Holland - Psycho Oncology Overview Obstacles and Opportunities
Psycho-Oncology - 2018 - Holland - Psycho Oncology Overview Obstacles and Opportunities
You might also like
- Kentucky Cabinet For Health and Family Services Inspector General Investigative Report 2007Document63 pagesKentucky Cabinet For Health and Family Services Inspector General Investigative Report 2007Beverly Tran100% (1)
- The Knowledge Foundation of Social WorkDocument4 pagesThe Knowledge Foundation of Social WorkIzzaNo ratings yet
- Antipsychotic-Induced Extrapyramidal Syndromes andDocument144 pagesAntipsychotic-Induced Extrapyramidal Syndromes andSeiska Mega100% (1)
- Mental RetardationDocument37 pagesMental RetardationaartiNo ratings yet
- ATPDDocument11 pagesATPDsagar189No ratings yet
- Seclusion and Physical Restraint: GeneralDocument6 pagesSeclusion and Physical Restraint: GeneralMegan ClearyNo ratings yet
- Unit 5 Family InfluencesDocument25 pagesUnit 5 Family Influencesshubhii1997No ratings yet
- ECT CompDocument23 pagesECT CompPinak DeNo ratings yet
- Artikel PTSS 10 QuestionnaireDocument17 pagesArtikel PTSS 10 QuestionnaireTELEPSIHIJATARNo ratings yet
- Psychiatry Sample Osce Exam eDocument4 pagesPsychiatry Sample Osce Exam ePNo ratings yet
- EpidemioDocument6 pagesEpidemioFlavian Costin NacladNo ratings yet
- Aversion TherapyDocument4 pagesAversion Therapyamagra993023100% (1)
- Alcohl DependenceDocument47 pagesAlcohl DependenceViky SinghNo ratings yet
- Icd 10 & 11 Comparison - My Ignou Case 1Document40 pagesIcd 10 & 11 Comparison - My Ignou Case 1AmiZade WorksheetsNo ratings yet
- PST 1Document18 pagesPST 1Gopika SNo ratings yet
- Mse - DepressionDocument6 pagesMse - DepressionKervin Jude D. ManahanNo ratings yet
- Case Presentation - Bpad GsDocument10 pagesCase Presentation - Bpad GsAarti GuptaNo ratings yet
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNo ratings yet
- Test AnxietyDocument23 pagesTest AnxietyClaire ZahraNo ratings yet
- I YearMSc Clinical PsychologyDocument11 pagesI YearMSc Clinical Psychologypruthvi dalawaiNo ratings yet
- Panic Disorders and Agoraphobia: Step-by-StepDocument4 pagesPanic Disorders and Agoraphobia: Step-by-StepDaniel R. Gaita, MA, LMSWNo ratings yet
- Psychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyDocument17 pagesPsychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyyashodharaNo ratings yet
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 pagesSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimNo ratings yet
- 21.cpsy.034 Icd-10&dsm-5Document8 pages21.cpsy.034 Icd-10&dsm-5Victor YanafNo ratings yet
- Psychiatry: A Case Analysis in Course IntegrationDocument40 pagesPsychiatry: A Case Analysis in Course IntegrationMcleo OaferinaNo ratings yet
- Internship Report (747) 5Document32 pagesInternship Report (747) 5indian meme templatesNo ratings yet
- Theory of Interpersonal Relations-PeplauDocument35 pagesTheory of Interpersonal Relations-Peplaumel_pusag100% (1)
- Schizophernia - Unit 1Document15 pagesSchizophernia - Unit 119PSY05 ATULYA VENKATESHNo ratings yet
- Coexistence of Folie Communique e and Folie SimultaneeDocument4 pagesCoexistence of Folie Communique e and Folie SimultaneeAna Rosa González Barroso0% (1)
- Bhopal (M.P.) : Assignment OnDocument9 pagesBhopal (M.P.) : Assignment OnamitNo ratings yet
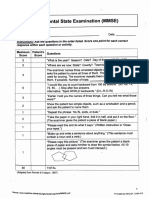
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)Prescilla San PedroNo ratings yet
- Memoryarticles: The Three Memory Storage SystemsDocument17 pagesMemoryarticles: The Three Memory Storage SystemsZein YusufNo ratings yet
- Concept of PsychobiologyDocument21 pagesConcept of Psychobiologydhivyaram100% (1)
- 300307814sherlin SapthicaDocument100 pages300307814sherlin SapthicaTitin PrihartiniNo ratings yet
- Stress and Coping NotesDocument10 pagesStress and Coping Notesrashi100% (1)
- Depression in Older AdultsDocument9 pagesDepression in Older Adultsapi-509881562No ratings yet
- Tolman Theory of LearningDocument4 pagesTolman Theory of LearningBigyan BasaulaNo ratings yet
- Overt Aggression Scale Modified MOASDocument1 pageOvert Aggression Scale Modified MOASVnaBronVizcondeNo ratings yet
- Neuropsyc Assessment Four LobesDocument12 pagesNeuropsyc Assessment Four LobesJulienne Rose Penaranda SaballaNo ratings yet
- Geriatric Psychiatry LectureDocument113 pagesGeriatric Psychiatry LectureabrihamNo ratings yet
- Brain Injury and Epilepsy: What Is An Epileptic Seizure?Document4 pagesBrain Injury and Epilepsy: What Is An Epileptic Seizure?kaninerNo ratings yet
- SuicideDocument33 pagesSuicidesreejithmk84No ratings yet
- Long Term ComplicationsDocument18 pagesLong Term Complicationsapi-3705046No ratings yet
- Lithium ToxicityDocument28 pagesLithium ToxicityReejan PaudelNo ratings yet
- ABG AnalysisDocument9 pagesABG AnalysisHoney PrasadNo ratings yet
- Clozapine Care GuideDocument16 pagesClozapine Care GuideERWIN SUMARDINo ratings yet
- Intellectual DisabilitiesDocument43 pagesIntellectual DisabilitiesrooqashaliNo ratings yet
- Occupational TherapyDocument6 pagesOccupational TherapyJayita Gayen DuttaNo ratings yet
- Technology Meets Tradition A Hybrid Model For Implementing Digital Tools in NeuropsychologyDocument13 pagesTechnology Meets Tradition A Hybrid Model For Implementing Digital Tools in NeuropsychologyRealidades InfinitasNo ratings yet
- Checklist MseDocument6 pagesChecklist MseHerlene Lyneth ZalamedaNo ratings yet
- Negative Symptoms EQZ Lancet ReviewDocument14 pagesNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNo ratings yet
- Master Rotation Plan Clinical Speciality PsychiatricDocument5 pagesMaster Rotation Plan Clinical Speciality Psychiatricaarti sahuNo ratings yet
- PBL 2Document16 pagesPBL 2alreemNo ratings yet
- Differences Between Icd 10 and DSM IV TRDocument2 pagesDifferences Between Icd 10 and DSM IV TRFareeha KhanNo ratings yet
- Mini Mental Status ReportDocument23 pagesMini Mental Status ReportAgnes MontalboNo ratings yet
- History of PsychiatryDocument8 pagesHistory of PsychiatryAngie MandeoyaNo ratings yet
- Social Psychology-1Document23 pagesSocial Psychology-1Zubair Mahmood KamalNo ratings yet
- 07 English Ocd BookletDocument27 pages07 English Ocd BookletJona JoyNo ratings yet
- Experimental Research Design: Mr. Jayesh PatidarDocument48 pagesExperimental Research Design: Mr. Jayesh PatidarKim NaNo ratings yet
- Psychiatry Notes For PGDocument8 pagesPsychiatry Notes For PGskycall28100% (1)
- Ethical Issues in Clinical Forensic PsychiatryFrom EverandEthical Issues in Clinical Forensic PsychiatryArtemis IgoumenouNo ratings yet
- Racism and Psychiatry: Contemporary Issues and InterventionsFrom EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockNo ratings yet
- 3.1. Emotional Facts of Life With Cancer - EnglishDocument32 pages3.1. Emotional Facts of Life With Cancer - EnglishReginaNo ratings yet
- The Dirty Dozen A Concise Measure of The Dark TriaDocument14 pagesThe Dirty Dozen A Concise Measure of The Dark TriaReginaNo ratings yet
- Manuscript HDocument43 pagesManuscript HReginaNo ratings yet
- HHS Public AccessDocument15 pagesHHS Public AccessReginaNo ratings yet
- Social WorkDocument2 pagesSocial Workdileep0% (1)
- Advocacy Practice For Social Justice 4Th Edition Richard Hoefer Full Chapter PDFDocument67 pagesAdvocacy Practice For Social Justice 4Th Edition Richard Hoefer Full Chapter PDFchesheleve100% (9)
- SUPERVISION SubibiDocument2 pagesSUPERVISION SubibiJiann AguilarNo ratings yet
- Welfare ModelDocument9 pagesWelfare ModelJananee Rajagopalan100% (4)
- Disciplines of Social WorkDocument20 pagesDisciplines of Social WorkMaria Lutgarda R. TumbagaNo ratings yet
- Wrap Thesis Shaffie 2006Document421 pagesWrap Thesis Shaffie 2006Najihah TarmiziNo ratings yet
- Residential Counselor ResumeDocument5 pagesResidential Counselor Resumebdg9hkj6100% (1)
- The Social Ecology of School Success. PDFDocument271 pagesThe Social Ecology of School Success. PDFOana X TodeNo ratings yet
- The Definition, Goals, Scope, CoreDocument10 pagesThe Definition, Goals, Scope, CoreCarmz PeraltaNo ratings yet
- PG New TanscheDocument14 pagesPG New TanscheSusiNo ratings yet
- Core Values of Social WorkDocument25 pagesCore Values of Social Workangie vibarNo ratings yet
- journalsImpactFactorsHIndex PDFDocument105 pagesjournalsImpactFactorsHIndex PDFcheahwaimunNo ratings yet
- Psychological ServicesDocument13 pagesPsychological Servicesapi-626136134No ratings yet
- ProfileDocument5 pagesProfileapi-537558791No ratings yet
- CNF ReviewerDocument4 pagesCNF ReviewerRose Anne Bautista100% (1)
- Lesson 4: Social Work Setting, Processes, and Services: Group 4 Humss 1 (ALLIANCE)Document40 pagesLesson 4: Social Work Setting, Processes, and Services: Group 4 Humss 1 (ALLIANCE)KaguraNo ratings yet
- 2 - The Professionals and Practitioners in Social WorkDocument7 pages2 - The Professionals and Practitioners in Social Workchewy chocoNo ratings yet
- Associate Marriage and Family Therapist Resume SampleDocument8 pagesAssociate Marriage and Family Therapist Resume Sampleebqlsqekg100% (1)
- Short Course in Social Work at UnisaDocument8 pagesShort Course in Social Work at Unisaafjwftijfbwmen100% (2)
- Diass SSLM Q1 W5Document10 pagesDiass SSLM Q1 W5Bonie ConjeNo ratings yet
- The Unionist November 2013Document8 pagesThe Unionist November 2013novvotikNo ratings yet
- Vietnam - Mental Health - CPIN - v1.0Document29 pagesVietnam - Mental Health - CPIN - v1.0Uyên ViNo ratings yet
- Bondhu ReportDocument47 pagesBondhu ReportMD. KHAIRUZZAMANNo ratings yet
- Crisis InterventionDocument12 pagesCrisis Interventiontatenda kosterNo ratings yet
- Residential Counselor: Job Description: I. Position SummaryDocument3 pagesResidential Counselor: Job Description: I. Position SummaryjackieeiesNo ratings yet
- Basic Concepts Related To Social Work Definition and InterrelationshipsDocument17 pagesBasic Concepts Related To Social Work Definition and Interrelationshipscarmina pagoy100% (3)
- Resume Mariyappa - AmarDocument2 pagesResume Mariyappa - AmarMariyappa Amara JyothyNo ratings yet
- Introduction To Group Work NOTES TODATE-3Document41 pagesIntroduction To Group Work NOTES TODATE-3catherine mutanuNo ratings yet




























































































Download as pdf or txt
You might also like
- Kentucky Cabinet For Health and Family Services Inspector General Investigative Report 2007Document63 pagesKentucky Cabinet For Health and Family Services Inspector General Investigative Report 2007Beverly Tran100% (1)
- The Knowledge Foundation of Social WorkDocument4 pagesThe Knowledge Foundation of Social WorkIzzaNo ratings yet
- Antipsychotic-Induced Extrapyramidal Syndromes andDocument144 pagesAntipsychotic-Induced Extrapyramidal Syndromes andSeiska Mega100% (1)
- Mental RetardationDocument37 pagesMental RetardationaartiNo ratings yet
- ATPDDocument11 pagesATPDsagar189No ratings yet
- Seclusion and Physical Restraint: GeneralDocument6 pagesSeclusion and Physical Restraint: GeneralMegan ClearyNo ratings yet
- Unit 5 Family InfluencesDocument25 pagesUnit 5 Family Influencesshubhii1997No ratings yet
- ECT CompDocument23 pagesECT CompPinak DeNo ratings yet
- Artikel PTSS 10 QuestionnaireDocument17 pagesArtikel PTSS 10 QuestionnaireTELEPSIHIJATARNo ratings yet
- Psychiatry Sample Osce Exam eDocument4 pagesPsychiatry Sample Osce Exam ePNo ratings yet
- EpidemioDocument6 pagesEpidemioFlavian Costin NacladNo ratings yet
- Aversion TherapyDocument4 pagesAversion Therapyamagra993023100% (1)
- Alcohl DependenceDocument47 pagesAlcohl DependenceViky SinghNo ratings yet
- Icd 10 & 11 Comparison - My Ignou Case 1Document40 pagesIcd 10 & 11 Comparison - My Ignou Case 1AmiZade WorksheetsNo ratings yet
- PST 1Document18 pagesPST 1Gopika SNo ratings yet
- Mse - DepressionDocument6 pagesMse - DepressionKervin Jude D. ManahanNo ratings yet
- Case Presentation - Bpad GsDocument10 pagesCase Presentation - Bpad GsAarti GuptaNo ratings yet
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNo ratings yet
- Test AnxietyDocument23 pagesTest AnxietyClaire ZahraNo ratings yet
- I YearMSc Clinical PsychologyDocument11 pagesI YearMSc Clinical Psychologypruthvi dalawaiNo ratings yet
- Panic Disorders and Agoraphobia: Step-by-StepDocument4 pagesPanic Disorders and Agoraphobia: Step-by-StepDaniel R. Gaita, MA, LMSWNo ratings yet
- Psychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyDocument17 pagesPsychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyyashodharaNo ratings yet
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 pagesSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimNo ratings yet
- 21.cpsy.034 Icd-10&dsm-5Document8 pages21.cpsy.034 Icd-10&dsm-5Victor YanafNo ratings yet
- Psychiatry: A Case Analysis in Course IntegrationDocument40 pagesPsychiatry: A Case Analysis in Course IntegrationMcleo OaferinaNo ratings yet
- Internship Report (747) 5Document32 pagesInternship Report (747) 5indian meme templatesNo ratings yet
- Theory of Interpersonal Relations-PeplauDocument35 pagesTheory of Interpersonal Relations-Peplaumel_pusag100% (1)
- Schizophernia - Unit 1Document15 pagesSchizophernia - Unit 119PSY05 ATULYA VENKATESHNo ratings yet
- Coexistence of Folie Communique e and Folie SimultaneeDocument4 pagesCoexistence of Folie Communique e and Folie SimultaneeAna Rosa González Barroso0% (1)
- Bhopal (M.P.) : Assignment OnDocument9 pagesBhopal (M.P.) : Assignment OnamitNo ratings yet
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)Prescilla San PedroNo ratings yet
- Memoryarticles: The Three Memory Storage SystemsDocument17 pagesMemoryarticles: The Three Memory Storage SystemsZein YusufNo ratings yet
- Concept of PsychobiologyDocument21 pagesConcept of Psychobiologydhivyaram100% (1)
- 300307814sherlin SapthicaDocument100 pages300307814sherlin SapthicaTitin PrihartiniNo ratings yet
- Stress and Coping NotesDocument10 pagesStress and Coping Notesrashi100% (1)
- Depression in Older AdultsDocument9 pagesDepression in Older Adultsapi-509881562No ratings yet
- Tolman Theory of LearningDocument4 pagesTolman Theory of LearningBigyan BasaulaNo ratings yet
- Overt Aggression Scale Modified MOASDocument1 pageOvert Aggression Scale Modified MOASVnaBronVizcondeNo ratings yet
- Neuropsyc Assessment Four LobesDocument12 pagesNeuropsyc Assessment Four LobesJulienne Rose Penaranda SaballaNo ratings yet
- Geriatric Psychiatry LectureDocument113 pagesGeriatric Psychiatry LectureabrihamNo ratings yet
- Brain Injury and Epilepsy: What Is An Epileptic Seizure?Document4 pagesBrain Injury and Epilepsy: What Is An Epileptic Seizure?kaninerNo ratings yet
- SuicideDocument33 pagesSuicidesreejithmk84No ratings yet
- Long Term ComplicationsDocument18 pagesLong Term Complicationsapi-3705046No ratings yet
- Lithium ToxicityDocument28 pagesLithium ToxicityReejan PaudelNo ratings yet
- ABG AnalysisDocument9 pagesABG AnalysisHoney PrasadNo ratings yet
- Clozapine Care GuideDocument16 pagesClozapine Care GuideERWIN SUMARDINo ratings yet
- Intellectual DisabilitiesDocument43 pagesIntellectual DisabilitiesrooqashaliNo ratings yet
- Occupational TherapyDocument6 pagesOccupational TherapyJayita Gayen DuttaNo ratings yet
- Technology Meets Tradition A Hybrid Model For Implementing Digital Tools in NeuropsychologyDocument13 pagesTechnology Meets Tradition A Hybrid Model For Implementing Digital Tools in NeuropsychologyRealidades InfinitasNo ratings yet
- Checklist MseDocument6 pagesChecklist MseHerlene Lyneth ZalamedaNo ratings yet
- Negative Symptoms EQZ Lancet ReviewDocument14 pagesNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNo ratings yet
- Master Rotation Plan Clinical Speciality PsychiatricDocument5 pagesMaster Rotation Plan Clinical Speciality Psychiatricaarti sahuNo ratings yet
- PBL 2Document16 pagesPBL 2alreemNo ratings yet
- Differences Between Icd 10 and DSM IV TRDocument2 pagesDifferences Between Icd 10 and DSM IV TRFareeha KhanNo ratings yet
- Mini Mental Status ReportDocument23 pagesMini Mental Status ReportAgnes MontalboNo ratings yet
- History of PsychiatryDocument8 pagesHistory of PsychiatryAngie MandeoyaNo ratings yet
- Social Psychology-1Document23 pagesSocial Psychology-1Zubair Mahmood KamalNo ratings yet
- 07 English Ocd BookletDocument27 pages07 English Ocd BookletJona JoyNo ratings yet
- Experimental Research Design: Mr. Jayesh PatidarDocument48 pagesExperimental Research Design: Mr. Jayesh PatidarKim NaNo ratings yet
- Psychiatry Notes For PGDocument8 pagesPsychiatry Notes For PGskycall28100% (1)
- Ethical Issues in Clinical Forensic PsychiatryFrom EverandEthical Issues in Clinical Forensic PsychiatryArtemis IgoumenouNo ratings yet
- Racism and Psychiatry: Contemporary Issues and InterventionsFrom EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockNo ratings yet
- 3.1. Emotional Facts of Life With Cancer - EnglishDocument32 pages3.1. Emotional Facts of Life With Cancer - EnglishReginaNo ratings yet
- The Dirty Dozen A Concise Measure of The Dark TriaDocument14 pagesThe Dirty Dozen A Concise Measure of The Dark TriaReginaNo ratings yet
- Manuscript HDocument43 pagesManuscript HReginaNo ratings yet
- HHS Public AccessDocument15 pagesHHS Public AccessReginaNo ratings yet
- Social WorkDocument2 pagesSocial Workdileep0% (1)
- Advocacy Practice For Social Justice 4Th Edition Richard Hoefer Full Chapter PDFDocument67 pagesAdvocacy Practice For Social Justice 4Th Edition Richard Hoefer Full Chapter PDFchesheleve100% (9)
- SUPERVISION SubibiDocument2 pagesSUPERVISION SubibiJiann AguilarNo ratings yet
- Welfare ModelDocument9 pagesWelfare ModelJananee Rajagopalan100% (4)
- Disciplines of Social WorkDocument20 pagesDisciplines of Social WorkMaria Lutgarda R. TumbagaNo ratings yet
- Wrap Thesis Shaffie 2006Document421 pagesWrap Thesis Shaffie 2006Najihah TarmiziNo ratings yet
- Residential Counselor ResumeDocument5 pagesResidential Counselor Resumebdg9hkj6100% (1)
- The Social Ecology of School Success. PDFDocument271 pagesThe Social Ecology of School Success. PDFOana X TodeNo ratings yet
- The Definition, Goals, Scope, CoreDocument10 pagesThe Definition, Goals, Scope, CoreCarmz PeraltaNo ratings yet
- PG New TanscheDocument14 pagesPG New TanscheSusiNo ratings yet
- Core Values of Social WorkDocument25 pagesCore Values of Social Workangie vibarNo ratings yet
- journalsImpactFactorsHIndex PDFDocument105 pagesjournalsImpactFactorsHIndex PDFcheahwaimunNo ratings yet
- Psychological ServicesDocument13 pagesPsychological Servicesapi-626136134No ratings yet
- ProfileDocument5 pagesProfileapi-537558791No ratings yet
- CNF ReviewerDocument4 pagesCNF ReviewerRose Anne Bautista100% (1)
- Lesson 4: Social Work Setting, Processes, and Services: Group 4 Humss 1 (ALLIANCE)Document40 pagesLesson 4: Social Work Setting, Processes, and Services: Group 4 Humss 1 (ALLIANCE)KaguraNo ratings yet
- 2 - The Professionals and Practitioners in Social WorkDocument7 pages2 - The Professionals and Practitioners in Social Workchewy chocoNo ratings yet
- Associate Marriage and Family Therapist Resume SampleDocument8 pagesAssociate Marriage and Family Therapist Resume Sampleebqlsqekg100% (1)
- Short Course in Social Work at UnisaDocument8 pagesShort Course in Social Work at Unisaafjwftijfbwmen100% (2)
- Diass SSLM Q1 W5Document10 pagesDiass SSLM Q1 W5Bonie ConjeNo ratings yet
- The Unionist November 2013Document8 pagesThe Unionist November 2013novvotikNo ratings yet
- Vietnam - Mental Health - CPIN - v1.0Document29 pagesVietnam - Mental Health - CPIN - v1.0Uyên ViNo ratings yet
- Bondhu ReportDocument47 pagesBondhu ReportMD. KHAIRUZZAMANNo ratings yet
- Crisis InterventionDocument12 pagesCrisis Interventiontatenda kosterNo ratings yet
- Residential Counselor: Job Description: I. Position SummaryDocument3 pagesResidential Counselor: Job Description: I. Position SummaryjackieeiesNo ratings yet
- Basic Concepts Related To Social Work Definition and InterrelationshipsDocument17 pagesBasic Concepts Related To Social Work Definition and Interrelationshipscarmina pagoy100% (3)
- Resume Mariyappa - AmarDocument2 pagesResume Mariyappa - AmarMariyappa Amara JyothyNo ratings yet
- Introduction To Group Work NOTES TODATE-3Document41 pagesIntroduction To Group Work NOTES TODATE-3catherine mutanuNo ratings yet