Download as pdf or txt
You might also like
- Community Health Nursing Practice Questions With RationaleDocument16 pagesCommunity Health Nursing Practice Questions With RationaleBe Nj90% (21)
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Pre Reg Pharmacists Last MinuteDocument9 pagesPre Reg Pharmacists Last MinuteBob BobNo ratings yet
- Guideline Watch 2021Document24 pagesGuideline Watch 2021Pedro NicolatoNo ratings yet
- Chapter 32. ConstipationDocument14 pagesChapter 32. ConstipationDiana F. MoscosoNo ratings yet
- The Effects of Alcohol Consumption On The Academic Performances of The Grade 12 Senior High School Students at Talisay City National High SchoolDocument5 pagesThe Effects of Alcohol Consumption On The Academic Performances of The Grade 12 Senior High School Students at Talisay City National High SchoolManarangJanine67% (6)
- Students Practical Training Report Project As Per PCI NormsDocument82 pagesStudents Practical Training Report Project As Per PCI NormsAakif Anjum100% (1)
- JudulDocument3 pagesJudulCacaNo ratings yet
- Iss Rts IndoDocument6 pagesIss Rts IndoPingkanNo ratings yet
- 7 Assessing The Motor Component of The Gcs Scoring SystemDocument11 pages7 Assessing The Motor Component of The Gcs Scoring Systemvishramki2009No ratings yet
- RTS 2011Document8 pagesRTS 2011Puspa AmandatyNo ratings yet
- Characteristicsandclinicaloutcomeoftraumaticbraininjuryin Lombok Indonesia 2019Document6 pagesCharacteristicsandclinicaloutcomeoftraumaticbraininjuryin Lombok Indonesia 2019Intan KarmilaNo ratings yet
- Trauma Geriatrico EstudioDocument6 pagesTrauma Geriatrico Estudioliz escalanteNo ratings yet
- Research JournalDocument22 pagesResearch JournalAnonymous vhVWBW1HSJNo ratings yet
- 164 321 1 SM PDFDocument11 pages164 321 1 SM PDFSasa KoropitNo ratings yet
- STROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Document7 pagesSTROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Ramona ManolitaNo ratings yet
- 1 s2.0 S2214139123000331 MainDocument6 pages1 s2.0 S2214139123000331 MainHailemariam MebratuNo ratings yet
- Assess The Traumatic Brain Injury Outcomes in Pakistani Emergency DepartmentDocument27 pagesAssess The Traumatic Brain Injury Outcomes in Pakistani Emergency DepartmentsanamaqsoodmalikNo ratings yet
- GJHS 8 152Document6 pagesGJHS 8 152Ika PuspitaNo ratings yet
- Trauma Score PDFDocument10 pagesTrauma Score PDFNdHy_Windhy_3403No ratings yet
- Profile of Trauma Patients in The Emergency DepartDocument6 pagesProfile of Trauma Patients in The Emergency DepartKhalil IbrahimNo ratings yet
- Bjs 11306Document11 pagesBjs 11306Carlos Perez RiveraNo ratings yet
- Prognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaDocument8 pagesPrognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaYeni PuspitasariNo ratings yet
- Acute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaDocument7 pagesAcute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaFidencio ParraNo ratings yet
- Body Temperature As A New Predictor of Mortality in Head Trauma PatientsDocument6 pagesBody Temperature As A New Predictor of Mortality in Head Trauma PatientsJuwita PuspaNo ratings yet
- Death After Head Injury: The 13 Year Outcome of A Case Control StudyDocument6 pagesDeath After Head Injury: The 13 Year Outcome of A Case Control StudyRegina SeptianiNo ratings yet
- Mortalidad HEMS PDFDocument7 pagesMortalidad HEMS PDFSebas GarciaNo ratings yet
- (10920684 - Neurosurgical Focus) The Estimated Cost of Surgically Managed Isolated Traumatic Head Injury Secondary To Road Traffic AccidentsDocument8 pages(10920684 - Neurosurgical Focus) The Estimated Cost of Surgically Managed Isolated Traumatic Head Injury Secondary To Road Traffic Accidentsnursyahiera aqilahNo ratings yet
- Big ScoreDocument7 pagesBig ScoredamonenNo ratings yet
- Review Jurnal Kelompok 1Document12 pagesReview Jurnal Kelompok 1Satria Yosi HernawanNo ratings yet
- Analisis Penilaian Triage Dan Revised Trauma Score Dalam Memprediksi Mortalitas Pada Pasien Trauma KepalaDocument11 pagesAnalisis Penilaian Triage Dan Revised Trauma Score Dalam Memprediksi Mortalitas Pada Pasien Trauma KepalaFarizalajiNo ratings yet
- Emerg 4 088 (9497)Document4 pagesEmerg 4 088 (9497)Taufik EffendyNo ratings yet
- Main 25Document6 pagesMain 25pokharelriwaj82No ratings yet
- Analisis Faktor Yang Mempengaruhi Outcome Pasien Cedera Kepala Berdasarkan Functional Independence Measure (Fim)Document7 pagesAnalisis Faktor Yang Mempengaruhi Outcome Pasien Cedera Kepala Berdasarkan Functional Independence Measure (Fim)rudimarwanNo ratings yet
- Recurrence Stroke of Ischemic Stroke Patients in Thailand:a Nationwide StudyDocument7 pagesRecurrence Stroke of Ischemic Stroke Patients in Thailand:a Nationwide StudyIJPHSNo ratings yet
- Clinical and Radiographic Predictors of Intracerebral Hemorrhage OutcomeDocument19 pagesClinical and Radiographic Predictors of Intracerebral Hemorrhage OutcomeAndre DharmawanNo ratings yet
- Using Machine Learning To Improve The Prediction of Functional Outcome in Ischemic Stroke PatientsDocument7 pagesUsing Machine Learning To Improve The Prediction of Functional Outcome in Ischemic Stroke PatientsdarNo ratings yet
- Plancikova2020 Article CharacteristicsAndOutcomeOfSevDocument7 pagesPlancikova2020 Article CharacteristicsAndOutcomeOfSevValéria MatosNo ratings yet
- Bet 10 59Document6 pagesBet 10 59Bhawna SaxenaNo ratings yet
- Pattern of Traumatic Head Injury in Makurdi, North Central Nigeria: Accident and Emergency ExperienceDocument9 pagesPattern of Traumatic Head Injury in Makurdi, North Central Nigeria: Accident and Emergency ExperienceMhmdzlkfli 12No ratings yet
- Defining Polytrauma by Abbreviated Injury Scale 3 For A Least Two Body Regions Is Insufficient in Terms of Short-Term Outcome (2018)Document7 pagesDefining Polytrauma by Abbreviated Injury Scale 3 For A Least Two Body Regions Is Insufficient in Terms of Short-Term Outcome (2018)Kenmaster WirelessNo ratings yet
- Catherine Tennick Final PHD Thesis PDFDocument10 pagesCatherine Tennick Final PHD Thesis PDFMelvri BisaiNo ratings yet
- Toracotomia en El Departamento de Emergencia PediáTricoDocument12 pagesToracotomia en El Departamento de Emergencia PediáTricoMartin Seminario AliagaNo ratings yet
- J Injury 2017 02 015Document5 pagesJ Injury 2017 02 015Ricky Rusydi SatriawanNo ratings yet
- 10 29252@beat-060208Document5 pages10 29252@beat-060208Khusnul KhotimahNo ratings yet
- 1 PBDocument9 pages1 PBJeon NianaNo ratings yet
- Comparison of The Modifed SMIR With GRACE For 1 Year AMI OutcomesDocument9 pagesComparison of The Modifed SMIR With GRACE For 1 Year AMI OutcomesJackNo ratings yet
- 479-Article Text-1740-1-10-20221114Document5 pages479-Article Text-1740-1-10-20221114Maryam AzamNo ratings yet
- Prevalence of Post Stroke Depression in Ambulatory PatientsDocument7 pagesPrevalence of Post Stroke Depression in Ambulatory PatientsSitti Rosdiana YahyaNo ratings yet
- Falls and TBiDocument0 pagesFalls and TBiMuhammad Abdul RahmanNo ratings yet
- Art 4Document6 pagesArt 4Hajji AhmedNo ratings yet
- Kana Afi Nabila-Jurnal 1 MataDocument11 pagesKana Afi Nabila-Jurnal 1 MataKanafie El NBilaNo ratings yet
- Sci 2Document7 pagesSci 2anna widiaNo ratings yet
- Degree of Injury On Visum Et Repertum: Upine PublishersDocument2 pagesDegree of Injury On Visum Et Repertum: Upine Publishersyunita sariNo ratings yet
- 1 SMDocument5 pages1 SMIntanPermataSyariNo ratings yet
- BR 57 1 20Document9 pagesBR 57 1 20Bui KienNo ratings yet
- Association Between Adherence To Guideline-Recommended Preventive Medications and In-Hospital Mortality in STEMIDocument10 pagesAssociation Between Adherence To Guideline-Recommended Preventive Medications and In-Hospital Mortality in STEMITheresia ledyNo ratings yet
- Relations With The Emergency Response Time: in Patients With Coronary Heart DiseaseDocument8 pagesRelations With The Emergency Response Time: in Patients With Coronary Heart DiseaseRizkyNo ratings yet
- Analisis Penilaian Triage Dan Revised Trauma Score Dalam Memprediksi Mortalitas Pada Pasien Trauma KepalaDocument11 pagesAnalisis Penilaian Triage Dan Revised Trauma Score Dalam Memprediksi Mortalitas Pada Pasien Trauma KepalaMaYola AkhriniNo ratings yet
- Pain Assessment and Management of Trauma Patients in An Emergency Department of A Tertiary Hospital in TanzaniaDocument6 pagesPain Assessment and Management of Trauma Patients in An Emergency Department of A Tertiary Hospital in TanzaniamandsximenesNo ratings yet
- Relations With The Emergency Response Time: in Patients With Coronary Heart DiseaseDocument7 pagesRelations With The Emergency Response Time: in Patients With Coronary Heart DiseaseRizkyNo ratings yet
- A Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurDocument9 pagesA Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurIJAR JOURNALNo ratings yet
- Stroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item GenerationDocument8 pagesStroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item Generationandi kurniawanNo ratings yet
- PrognosisDocument7 pagesPrognosisMuhammad Rafli AkbarNo ratings yet
- Journal of Orthopaedic Diseases and TraumatologyDocument5 pagesJournal of Orthopaedic Diseases and TraumatologySantosh KumarNo ratings yet
- Primary Management of PolytraumaFrom EverandPrimary Management of PolytraumaSuk-Kyung HongNo ratings yet
- Imaging Trauma and Polytrauma in Pediatric PatientsFrom EverandImaging Trauma and Polytrauma in Pediatric PatientsVittorio MieleNo ratings yet
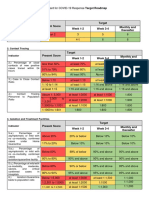
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Failure To Thrive JournalDocument13 pagesFailure To Thrive JournalApRil Anne BalanonNo ratings yet
- DGN Acedemic TranscriptDocument1 pageDGN Acedemic TranscriptFiftys Sabz KedewaNo ratings yet
- Guía de Práctica Clínica Europea ITUDocument7 pagesGuía de Práctica Clínica Europea ITUVICTORIA GONZALEZ VEGANo ratings yet
- Exercise Preparticipation and Health Screening Protocol (ContentDocument36 pagesExercise Preparticipation and Health Screening Protocol (ContentAndreuNo ratings yet
- Skills Checklist Blood AdminDocument3 pagesSkills Checklist Blood AdmingtsantosNo ratings yet
- Diabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?Document2 pagesDiabetic Foot Care Before and During The COVID-19 Epidemic: What Really Matters?SitiNo ratings yet
- Information For Persons With HOSPITA SEMI-PRIVATE/PRIVATE Supplementary Hospitalisation Insurance.Document4 pagesInformation For Persons With HOSPITA SEMI-PRIVATE/PRIVATE Supplementary Hospitalisation Insurance.docas123No ratings yet
- Bio Magnetic Therapy - DrJockersDocument20 pagesBio Magnetic Therapy - DrJockersIvica Putrić100% (1)
- MPU 3313 - V2 Kesihatan Dan Kesejahteraan 2Document13 pagesMPU 3313 - V2 Kesihatan Dan Kesejahteraan 2TAY JIUN HOANG MoeNo ratings yet
- 57d28ad03fcf8 - Nama Peserta Training PV 2016 - PESERTA UTAMADocument8 pages57d28ad03fcf8 - Nama Peserta Training PV 2016 - PESERTA UTAMASaepul BahriNo ratings yet
- Job DescriptionDocument2 pagesJob DescriptionVaughn Jovi GabrilloNo ratings yet
- Subject: of The of The F: Implementation CentralDocument1 pageSubject: of The of The F: Implementation CentralBhavagna SaiNo ratings yet
- Ra 11166Document33 pagesRa 11166Princess Melanie MelendezNo ratings yet
- Texas Health and Human Services Pink BookDocument266 pagesTexas Health and Human Services Pink BookTexas WatchdogNo ratings yet
- Medical AbbreviationsDocument31 pagesMedical AbbreviationsLailaNo ratings yet
- History Examination of Gynecology and Obstetrics PatientsDocument3 pagesHistory Examination of Gynecology and Obstetrics PatientsAgus WijayaNo ratings yet
- Glossopharyngeal NeuralgiaDocument36 pagesGlossopharyngeal NeuralgiaGeetha SoundaryaNo ratings yet
- Muslim Hands YEMENDocument3 pagesMuslim Hands YEMENreem esamNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- Sample Questions - True Learn Family MedicineDocument11 pagesSample Questions - True Learn Family MedicinelarazahabiNo ratings yet
- COVID-19 mRNA Vaccine BNT162b2 UKPAR PFIZER BIONTECH 15dec2020Document51 pagesCOVID-19 mRNA Vaccine BNT162b2 UKPAR PFIZER BIONTECH 15dec2020gio malicoNo ratings yet
- Tocovidj 1 191Document5 pagesTocovidj 1 191rithy khouyNo ratings yet