Download as pdf or txt
You might also like
- Bishop Coulston Roman Military Equipment From The Punic Wars To The Fall of RomeDocument345 pagesBishop Coulston Roman Military Equipment From The Punic Wars To The Fall of Romefevzisahin79100% (4)
- Agency AgreementDocument10 pagesAgency AgreementbinoyjmatNo ratings yet
- Fabrication Procrdure Metering SkidDocument11 pagesFabrication Procrdure Metering SkidgstketutNo ratings yet
- Analysis of Post Operative Systemic To Pulmonary Artery Shunt FailureDocument5 pagesAnalysis of Post Operative Systemic To Pulmonary Artery Shunt FailurePaul HartingNo ratings yet
- Sangre FrescaDocument9 pagesSangre FrescaRobinson Trujillo CabanillaNo ratings yet
- PSS en SarcomatosisDocument6 pagesPSS en SarcomatosisJuan Torres MeleroNo ratings yet
- Carson 2011Document10 pagesCarson 2011karine.ghiggiNo ratings yet
- Nihms 1676215Document23 pagesNihms 1676215nimaelhajjiNo ratings yet
- The Truths Behind The Statistics of Surgical Treatment For Hypertensive Brainstem Hemorrhage in China: A ReviewDocument10 pagesThe Truths Behind The Statistics of Surgical Treatment For Hypertensive Brainstem Hemorrhage in China: A ReviewAnonymous tG35SYROzENo ratings yet
- 1 s2.0 S1083879111002916 MainDocument8 pages1 s2.0 S1083879111002916 MainNunungTriwahyuniNo ratings yet
- 1749 8090 8 54 PDFDocument7 pages1749 8090 8 54 PDFInggriht Senny BondangNo ratings yet
- Neoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Document9 pagesNeoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Prodromos KoutoukoglouNo ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- Cha BH Clin Endosc. 2021 Survival Benefit of Intraductal Radiofrequency Ablation For Malignant Biliary Obstruction Meta Ce-2020-254Document7 pagesCha BH Clin Endosc. 2021 Survival Benefit of Intraductal Radiofrequency Ablation For Malignant Biliary Obstruction Meta Ce-2020-254Byung ChaNo ratings yet
- CMJ 128 826Document9 pagesCMJ 128 826nadya magfiraNo ratings yet
- Impact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationDocument12 pagesImpact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationsarahNo ratings yet
- Tirofiban Revision y MetanalisisDocument7 pagesTirofiban Revision y MetanalisisJorge Luis Plasencia CubaNo ratings yet
- Abdollah 2018Document4 pagesAbdollah 2018Neetumishti ChadhaNo ratings yet
- Jovin2017 PDFDocument12 pagesJovin2017 PDFdebby claudiNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- 2023 Article 4688Document13 pages2023 Article 4688Muhammad FakhrizalNo ratings yet
- Efficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Document8 pagesEfficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Rayhan OemarNo ratings yet
- Prognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDocument11 pagesPrognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDefriyan RamziNo ratings yet
- Choosing Between Enoxaparin and Fondaparinux For The Management of Patients With Acute Coronary Syndrome: A Systematic Review and Meta-AnalysisDocument13 pagesChoosing Between Enoxaparin and Fondaparinux For The Management of Patients With Acute Coronary Syndrome: A Systematic Review and Meta-Analysisfairuz syafira rahmahNo ratings yet
- 2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFDocument14 pages2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFClaudioLagosNo ratings yet
- Lectura 1Document13 pagesLectura 1Ricardo Huaman QuirozNo ratings yet
- Long-Term Recurrence Rates After Surgery in Primary HyperparathyroidismDocument9 pagesLong-Term Recurrence Rates After Surgery in Primary HyperparathyroidismTimothy supitNo ratings yet
- (2018) Aggresiveness of Solid Pseudopapillary Neoplasm Literature Review and MetanalysisDocument7 pages(2018) Aggresiveness of Solid Pseudopapillary Neoplasm Literature Review and MetanalysispengadaanNo ratings yet
- Criterio Nuevo para Transfusion 2014Document2 pagesCriterio Nuevo para Transfusion 2014Humberto Liu BejaranoNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptIntan Kartika NursyahbaniNo ratings yet
- Prediction of Mortality in Incident Hemodialysis PDocument13 pagesPrediction of Mortality in Incident Hemodialysis PiffaNo ratings yet
- Han 2018Document32 pagesHan 2018Isabella EspositoNo ratings yet
- Addition of The Fleischner Society Guidelines To Chest CT ExaminationDocument9 pagesAddition of The Fleischner Society Guidelines To Chest CT Examinationvictor ibarra romeroNo ratings yet
- J Ahj 2019 12 007Document29 pagesJ Ahj 2019 12 007Adriana MartinsNo ratings yet
- TP 0000000000001513Document5 pagesTP 0000000000001513Muhammad RiefkyNo ratings yet
- Safety of Low-Molecular-Weight Heparin Compared To Unfractionated Heparin in Hemodialysis: A Systematic Review and Meta-AnalysisDocument12 pagesSafety of Low-Molecular-Weight Heparin Compared To Unfractionated Heparin in Hemodialysis: A Systematic Review and Meta-AnalysisAaron GranadosNo ratings yet
- Heartfailure FixDocument10 pagesHeartfailure FixdhikaNo ratings yet
- Kemoterapi THT 5Document8 pagesKemoterapi THT 5Niko Nofian NugrohoNo ratings yet
- European Societyof CardiologyDocument26 pagesEuropean Societyof CardiologyKoncz AnnaNo ratings yet
- Routine Versus Selective Computed Tomography in Non-Traumatic Acute Abdominal Pain: Meta-Analysis of Randomised TrialsDocument9 pagesRoutine Versus Selective Computed Tomography in Non-Traumatic Acute Abdominal Pain: Meta-Analysis of Randomised TrialsJhosselyne Beatriz AliagaNo ratings yet
- Annonc mdw587.026Document1 pageAnnonc mdw587.026Aaron Paul BernasNo ratings yet
- Shiwei Yang, Xiaoli Yuan, Rongjun Ma, Li Jiang, Jianmin Guo, Yuzhu Zang, Jie Shi, Jing Yang, Pingchong Lei, Zhongwen Liu, Yin Zhang, Zunmin ZhuDocument6 pagesShiwei Yang, Xiaoli Yuan, Rongjun Ma, Li Jiang, Jianmin Guo, Yuzhu Zang, Jie Shi, Jing Yang, Pingchong Lei, Zhongwen Liu, Yin Zhang, Zunmin ZhuAbdurrahman HasanuddinNo ratings yet
- Eurheartj Ehu357 FullDocument8 pagesEurheartj Ehu357 FullagneselimNo ratings yet
- 2a.330-Removal of Humoral Mediators and The Effect On The Survival of Septic Patients by Hemoperfusion With Neutral Microporous Resin ColumnDocument7 pages2a.330-Removal of Humoral Mediators and The Effect On The Survival of Septic Patients by Hemoperfusion With Neutral Microporous Resin Columngmejiar5237No ratings yet
- Survival Benefit of Liver Resection For Hepatocellular Carcinoma Associated With Portal Vein InvasionDocument6 pagesSurvival Benefit of Liver Resection For Hepatocellular Carcinoma Associated With Portal Vein Invasion2rqcwwqdyfNo ratings yet
- s10147 020 01632 XDocument7 pagess10147 020 01632 X363331272No ratings yet
- Systematic-Review-of-a-Novel-Approach-to-Prevent-PDocument2 pagesSystematic-Review-of-a-Novel-Approach-to-Prevent-PJamie ElmawiehNo ratings yet
- High-Dose vs. Low-Dose Proton Pump Inhibitors Post-Endoscopic Hemostasis in Patients With Bleeding Peptic Ulcer. A Meta-Analysis and Meta-Regression AnalysisDocument10 pagesHigh-Dose vs. Low-Dose Proton Pump Inhibitors Post-Endoscopic Hemostasis in Patients With Bleeding Peptic Ulcer. A Meta-Analysis and Meta-Regression Analysis200742 Elya AmaliaNo ratings yet
- Factors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesDocument12 pagesFactors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesErinda SafitriNo ratings yet
- Vianen2022 Article PrehospitalTraumaticCardiacArrDocument16 pagesVianen2022 Article PrehospitalTraumaticCardiacArrMarco CulquiNo ratings yet
- Thrombectomy 6 To 24 Hours After Stroke With A Mismatch Between Deficit and InfarctDocument11 pagesThrombectomy 6 To 24 Hours After Stroke With A Mismatch Between Deficit and InfarctDaniela GuariniNo ratings yet
- Hep 49Document5 pagesHep 49Andreea NicoletaNo ratings yet
- 2023 AJTM Vol 7 Issue 1 Article 7Document9 pages2023 AJTM Vol 7 Issue 1 Article 7gzou2013No ratings yet
- Revista de RevistaDocument11 pagesRevista de RevistaMiguel Angel Tipiani MallmaNo ratings yet
- Characteristics, Treatment Patterns and Outcomes of Patients With Small Cell Lung Cancer-A Retrospective Single Institution AnalysisDocument4 pagesCharacteristics, Treatment Patterns and Outcomes of Patients With Small Cell Lung Cancer-A Retrospective Single Institution AnalysismaleticjNo ratings yet
- Does The UNOS Heart Transplant Allocation System Favor Men Over Women?Document9 pagesDoes The UNOS Heart Transplant Allocation System Favor Men Over Women?Thumper KatesNo ratings yet
- Characteristics of Chinese Herbal Medicine Usage and Its Effect On Survival ofDocument9 pagesCharacteristics of Chinese Herbal Medicine Usage and Its Effect On Survival ofu106023406No ratings yet
- Lung Cancer Current Therapies and New Targeted TreatmentsDocument13 pagesLung Cancer Current Therapies and New Targeted TreatmentsWlad PaCaNo ratings yet
- Metastase Cerebrale 3Document9 pagesMetastase Cerebrale 3Nouhad BenNo ratings yet
- Continuing High Mortality From Trauma Haemorrhage and Opportunities For Improvement in Transfusion Practice: A Observational StudyDocument21 pagesContinuing High Mortality From Trauma Haemorrhage and Opportunities For Improvement in Transfusion Practice: A Observational StudydanielNo ratings yet
- Shi 2017Document8 pagesShi 2017Claudia Ivette Villarreal OvalleNo ratings yet
- Berkhemer PDFDocument158 pagesBerkhemer PDFFariz Eka SetiawanNo ratings yet
- Best Practices of Apheresis in Hematopoietic Cell TransplantationFrom EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibNo ratings yet
- ASON SLA Classification of ServicesDocument6 pagesASON SLA Classification of ServicesWondale KebedeNo ratings yet
- Hendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Document930 pagesHendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Héctor RomeroNo ratings yet
- Semprof SweetinaDocument20 pagesSemprof SweetinaSweetina MerkusiNo ratings yet
- Unit-14 Maintenance BookDocument57 pagesUnit-14 Maintenance Bookrama_subbuNo ratings yet
- OGUNSOLA and RUFAI (2023) - Disaster Preparedness Strategies at The National Archives of Nigeria IbadanDocument17 pagesOGUNSOLA and RUFAI (2023) - Disaster Preparedness Strategies at The National Archives of Nigeria IbadanKKNo ratings yet
- A Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionDocument9 pagesA Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionIin Sakinah DewiNo ratings yet
- BSR455 - Group 9 - Building Inspection - 3aDocument22 pagesBSR455 - Group 9 - Building Inspection - 3aMuhammad IdzhamNo ratings yet
- The Problem of Increasing Human Energy - Nikola Tesla PDFDocument27 pagesThe Problem of Increasing Human Energy - Nikola Tesla PDFKarhys100% (2)
- 2-Design of HRISDocument34 pages2-Design of HRISRicha GargNo ratings yet
- Phrasal Verb LESSON FINAL 1701874327225Document67 pagesPhrasal Verb LESSON FINAL 1701874327225bgt dfgNo ratings yet
- HigginsBaumfieldHall07 - LearningSkills Tech OnlineDocument52 pagesHigginsBaumfieldHall07 - LearningSkills Tech OnlineattiqbakhtawarNo ratings yet
- PreviewpdfDocument136 pagesPreviewpdfDayana Suarez RamosNo ratings yet
- Safir 9 Tonearm ManualDocument14 pagesSafir 9 Tonearm Manualmoma52No ratings yet
- Time Value of Money: Compound InterestDocument28 pagesTime Value of Money: Compound InterestkateNo ratings yet
- Management Theories-1Document5 pagesManagement Theories-1veera kaurNo ratings yet
- Oct 1st Week Details (Eng) by ACDocument26 pagesOct 1st Week Details (Eng) by ACHema Sundar ReddyNo ratings yet
- Pollack Cells Gels Engines LifeDocument320 pagesPollack Cells Gels Engines LifeAlfonso Lema100% (3)
- 4.3 - Maintenance Processing V2.0Document14 pages4.3 - Maintenance Processing V2.0ఈశ్వర్ భరణి100% (1)
- Delcam - PowerINSPECT 2017 WhatsNew CNC RU - 2016Document40 pagesDelcam - PowerINSPECT 2017 WhatsNew CNC RU - 2016phạm minh hùngNo ratings yet
- Home Learning IB GR 12 June 4, 7 - 11Document6 pagesHome Learning IB GR 12 June 4, 7 - 11Arnel Ordas AvilaNo ratings yet
- Invenia ABUS 2.0 Release Notes - UM - 4700-0044-00 - 4Document24 pagesInvenia ABUS 2.0 Release Notes - UM - 4700-0044-00 - 4Jawad SandhuNo ratings yet
- CPA-Financial ReportingDocument158 pagesCPA-Financial Reportingjbah saimon baptisteNo ratings yet
- Amanpulo FactsheetDocument6 pagesAmanpulo FactsheetAlexNo ratings yet
- Sarah Tchoukaleff ResumeDocument1 pageSarah Tchoukaleff Resumeapi-261081956No ratings yet
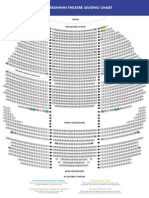
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- Workout ChartDocument1 pageWorkout ChartAsadullah JawaidNo ratings yet
- Lexical Semantic Problems in TranslationDocument13 pagesLexical Semantic Problems in Translationvargas199511100% (2)