Disorders of the REVIEW ARTICLE
Cauda Equina C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
By Samantha LoRusso, MD
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo65TEub0G9tZtPaMachiqn on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: Cauda equina dysfunction (often referred to as cauda
equina syndrome) is caused by a diverse group of disorders that affect the
lumbosacral nerve roots. It is important to recognize dysfunction of the
cauda equina quickly to minimize diagnostic delay and lasting neurologic
symptoms. This article describes cauda equina anatomy and the clinical
features, differential diagnosis, and management of cauda equina
disorders.
RECENT FINDINGS: The diagnosis of disorders of the cauda equina continues to
be a challenge. If a compressive etiology is seen, urgent neurosurgical
intervention is recommended. However, many people with clinical
features of cauda equina dysfunction will have negative diagnostic studies.
If the MRI is negative, it is important to understand the diagnostic
evaluation and differential diagnosis so that less common etiologies
are not missed.
SUMMARY: Cauda equina dysfunction most often occurs due to lumbosacral
disk herniation. Nondiskogenic causes include vascular, infectious,
inflammatory, traumatic, and neoplastic etiologies. Urgent evaluation and
surgical intervention are recommended in most cases of compressive
cauda equina syndrome. Other types of treatment may also be indicated CITE AS:
depending on the etiology. CONTINUUM (MINNEAP MINN)
2021;27(1, SPINAL CORD DISORDERS):
205–224.
Address correspondence to
INTRODUCTION Dr Samantha LoRusso, 395 W
D
ysfunction of the lumbosacral nerve roots within the cauda equina 12th Ave, Columbus, OH 43210,
samantha.lorusso@osumc.edu.
can lead to symptoms of urinary retention and incontinence,
constipation, bowel incontinence, sexual dysfunction, sensory RELATIONSHIP DISCLOSURE:
changes (particularly saddle anesthesia), back pain, and lower Dr LoRusso receives
research/grant support from
extremity weakness; this is often referred to as cauda equina the National Institute of
syndrome. The first description of cauda equina syndrome in the literature is Neurological Disorders and
attributed to Mixter and Barr,1 who described a case due to disk herniation in Stroke NeuroNEXT.
1934. The exact incidence of cauda equina syndrome is not known, but it is UNLABELED USE OF
thought to be somewhere between 1 per 33,000 and 1 per 100,000,2 which is PRODUCTS/INVESTIGATIONAL
consistent with an estimate from the United Kingdom of 1.9 per 100,000.3 USE DISCLOSURE:
Dr LoRusso reports no
However, a study from Slovenia estimated an annual incidence of 3.4 per 1 million disclosure.
people.4 The variability in the epidemiologic data may be partly because of poor
consensus regarding the precise definition of cauda equina syndrome. As many © 2021 American Academy
as 17 different definitions were found in a literature review on the topic.5 Still, it of Neurology.
CONTINUUMJOURNAL.COM 205
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
is accepted that the most common cause is lumbar disk herniation, representing
about 45% of cases.5 Other etiologies include, but are not limited to,
nondiskogenic structural changes, neoplasm, trauma, infection, inflammatory
disorders, vascular disorders, and iatrogenic causes. Timely diagnosis is
important since delays may result in worse neurologic outcomes. This article
discusses the anatomy, clinical presentation, diagnosis, and management of
disorders of the cauda equina.
ANATOMY
The last segment of the spinal cord, termed the conus medullaris, ends around
vertebral level T12-L2. The nerve roots that exit via foramina below the conus
medullaris (L2 through L5, S1 through S5, and the coccygeal nerve roots) create
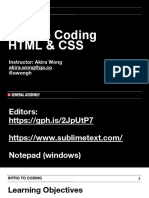
the cauda equina (FIGURE 9-16), which was named for its resemblance to a
horse’s tail by French anatomists Andre du Laurens and Andreas Lazarius in the
1600s.7 Damage to these nerve roots can cause symptoms of weakness,
numbness, sexual dysfunction, and changes in urinary and bowel function since
they control lower extremity movement and sensation (L2 through S3), external
genitalia and perineal sensation (S2 through S4), sensation overlying the coccyx
(S4-S5 and coccygeal nerve roots), bladder function (S2 through S4), and the
external anal sphincter (S2 through S4).8
The cauda equina is located in the thecal sac inside the spinal canal. Similar to
the spinal cord itself, it is surrounded by the vertebral bodies, intervertebral
disks, and posterior longitudinal ligament anteriorly and the ligamentum flavum
and spinous processes posteriorly.9 The blood supply is not as well defined as that
of the spinal cord.10 One study found that each nerve root obtains blood supply
from proximal and distal radicular arteries, with the ventral and dorsal proximal
radicular arteries receiving blood supply from the anterior and posterior spinal
arteries, respectively. This group also found the cauda equina to be an area of
relative hypovascularity, which may make it more likely to be damaged by
ischemia.10,11
CLINICAL PRESENTATION
Despite a lack of consensus
regarding the precise definition
of cauda equina syndrome, the
clinical features of bladder or
bowel disturbance, sexual
dysfunction, saddle anesthesia,
weakness or numbness in the
legs, and pain in the lower back
or legs are well recognized. An
individual patient with cauda
equina dysfunction may have
any of these symptoms to
varying degrees, so high clinical
suspicion is required. Symptoms
FIGURE 9-1 may come on suddenly or
Cauda equina anatomy. Lumbar, sacral, and
develop over days to weeks.12,13
coccygeal nerve roots of the cauda equina.
Reprinted with permission from Stewart JD.6 © 2010 JBJ Some patients even describe a
Publishing. more chronic course in which
206 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
back pain and sciatica are present with gradual progression of other symptoms KEY POINTS
over months.13 The variability in time course may be because of differences
● Cauda equina syndrome
in pathophysiology, with some patients having a sudden large disk herniation results from dysfunction of
and others with more slowly developing canal stenosis or neoplastic disease, lumbosacral nerve roots
for example. leading to symptoms of
Examination findings that suggest cauda equina dysfunction include reduced urinary retention and
incontinence, constipation,
or absent reflexes in the lower extremities, loss of perineal or lower extremity
bowel incontinence, sexual
sensation, reduced rectal tone, and lower extremity flaccid weakness. Classically, dysfunction, sensory
this is a syndrome that affects only lumbosacral nerve roots, so no upper motor changes (particularly saddle
neuron signs and no signs or symptoms in the upper extremities should be anesthesia), back pain, and
lower extremity weakness.
present (eg, if the cauda equina dysfunction is caused by lumbosacral disk
herniation). However, some disorders that affect the cauda equina may also ● Examination findings that
affect the spinal cord, leading to upper motor neuron signs, or may involve the suggest cauda equina
upper extremities if the specific pathologic process also causes dysfunction of dysfunction include reduced
cervical nerve roots. or absent reflexes in the
lower extremities, loss of
perineal or lower extremity
Pain sensation, reduced rectal
Low back pain and leg pain are very common in cauda equina syndrome, with tone, and lower extremity
sciatica reported in up to 97% of patients in one retrospective review.14 However, flaccid weakness.
within the larger population of those with low back pain (about 90% of the
● The sensory changes in
population will experience low back pain at some point in their lives),15 cauda cauda equina syndrome can
equina syndrome is rare, with an estimated prevalence of 4 per 10,000.16 Of be unilateral or bilateral,
those with cauda equina syndrome, unilateral sciatica may be more common with the most common areas
of involvement being the
than bilateral sciatica,8,13,14 and the pain may worsen in the supine position.8
posterior thighs, buttocks,
and perineum.
Sensory Changes
The sensory changes in cauda equina syndrome can be unilateral or bilateral,
with the most common areas of involvement being the posterior thighs,
buttocks, and perineum.5 Saddle anesthesia was noted to be present in 93% of
patients with cauda equina syndrome in one study.14 It is important to
specifically ask patients about perineal sensory deficits in a way that is
understood by everyone, including asking about sensation during toileting
activities such as wiping or defecation.17 Sensation in the extremities should be
assessed as part of the basic neurologic examination, but if cauda equina
syndrome is suspected, perineal sensation, particularly to pinprick, should also
be assessed.5
Urinary Symptoms
Symptoms of urinary dysfunction include decreased urethral sensation and
urinary stream, urinary retention, and incontinence. Urinary incontinence in
cauda equina syndrome is thought to be overflow incontinence that occurs
secondary to the retention.8,18 At least some of these symptoms occur in the
majority of patients with cauda equina syndrome.14 Careful history taking is
important since patients may not fully recognize their symptoms.19
Bowel Dysfunction
Bowel dysfunction in cauda equina syndrome can range from constipation to
incontinence, with the former usually preceding the latter.17 Overall, bowel
incontinence is not as commonly reported as urinary dysfunction.14 The reason
for this is not entirely clear but may be because of a reporting bias, or bowel
CONTINUUMJOURNAL.COM 207
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
problems may simply take longer to become apparent.12 It is still recommended
to test rectal tone,5 although testing may have limited utility since some studies
have noted poor physician accuracy in assessing rectal tone.20 Testing for the
presence of the bulbocavernosus reflex can also aid in the evaluation of anal
function. This reflex, which may be absent in cauda equina syndrome, is
elicited by squeezing the glans penis or clitoris and watching for contraction
of the anal sphincter. Examination elements such as assessing rectal tone and
the bulbocavernosus reflex should be elicited only when clinically indicated
and in the presence of an appropriate chaperone. Furthermore, given the
sensitive nature of these maneuvers, the clinician should explain the rationale and
mechanics of these examinations and obtain verbal consent before conducting these
assessments.
Sexual Dysfunction
Of patients with cauda equina syndrome, 12% to 96% will report sexual
dysfunction if asked.14,21 The symptoms of sexual dysfunction are variable and can
include erectile or ejaculatory impairment, impotence, priapism, dyspareunia,
and urination during intercourse.14,19 Asking specific questions about these
symptoms is important but often omitted or not documented by physicians.5,22
Weakness
Weakness in the lower extremities can occur in any distribution (proximal or
distal, symmetric or asymmetric) in cauda equina syndrome.5 However, it is not
necessary for weakness to be present since a process affecting only the lower
sacral and coccygeal roots will not cause weakness. On examination, motor
strength should be assessed in detail and reflexes evaluated since lower extremity
reflexes may be reduced.
DIAGNOSIS
The diagnosis of cauda equina syndrome can be challenging since many of the
symptoms are common in the general population and could be secondary to
other causes. For example, urinary retention and constipation are common side
effects of medications. Delays in diagnosis are not infrequent, with one study
citing a median of 11 days from the onset of symptoms to diagnosis and another
citing an average of 9 days until diagnosis.2,18 Furthermore, no single symptom or
sign has been found to have consistently high sensitivity and specificity in
diagnosing MRI-positive cauda equina syndrome.23-25 In one study, bowel
dysfunction, reduced perineal sensation, and abnormal rectal tone were the most
specific findings but had low sensitivity.17,26 That being said, measuring the
postvoid residual volume may be a helpful early step (and can be done as an
adjunct to the examination) in evaluating a patient with suspected cauda equina
syndrome. A postvoid residual of 200 mL or more was found to have a sensitivity
of 94% and specificity of 72% in predicting MRI-positive cauda equina syndrome
in one study.27
MRI and Other Imaging
In patients with possible cauda equina dysfunction, MRI of the lumbosacral spine
is the imaging modality of choice, with many studies using it as the standard for
diagnosis. It allows for optimal evaluation of soft tissue pathology and can help
evaluate for both diskogenic and nondiskogenic causes of cauda equina
208 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
dysfunction. If diskogenic disease is highly suspected, contrast administration KEY POINTS
can be withheld, but if the etiology is unclear, a contrast-enhanced scan can be
● No single symptom or sign
helpful. Neoplastic, infectious, and inflammatory disorders will often show has been found to have
nerve root enhancement. If MRI cannot be performed, CT of the lumbar spine consistently high sensitivity
should be done. In a study evaluating the sensitivity and specificity of CT and specificity in diagnosing
in cauda equina syndrome, it was found that CT was 98% sensitive and 86% MRI-positive cauda equina
syndrome.
specific for identifying significant spinal stenosis (using MRI as the standard).28
If the CT does not reveal a clear etiology, CT myelography should be performed ● If any question exists
as soon as possible to help rule out a compressive etiology. regarding the localization
to the cauda equina based
MRI-negative Cauda Equina Dysfunction on history and examination,
then imaging of the entire
Of patients with suspected cauda equina dysfunction, 14% to 48% will have the neuraxis (brain and spinal
diagnosis confirmed on MRI of the lumbosacral spine.23 The recommended cord) should be
evaluation for the other patients, those who are “scan negative,” is not well considered.
delineated. In these patients, less common causes of cauda equina dysfunction
should be considered. For example, patients with abdominal aortic disease may
have ischemia leading to cauda equina dysfunction, in which case imaging of the
aorta may be helpful. In other cases, magnetic resonance angiography (MRA) of
the spine may be needed to visualize vascular lesions causing cauda equina
dysfunction. In addition, further neurologic workup with CSF analysis and nerve
conduction studies and EMG is recommended unless a clear explanation is
already evident. CSF analysis is helpful in the evaluation of infectious,
inflammatory, or neoplastic disorders. Nerve conduction studies and EMG can
help to confirm a pathologic preganglionic process or help to diagnose disorders
such as Guillain-Barré syndrome (GBS) or chronic inflammatory demyelinating
polyradiculoneuropathy (CIDP) that can rarely present resembling cauda equina
syndrome. However, it is necessary to take the timing of the presentation into
consideration when performing nerve conduction studies and EMG, as some
findings may not be evident in the first 2 to 3 weeks.
In patients with symptoms of cauda equina dysfunction whose scan is
negative, consideration of other diagnoses that can have similar symptoms is also
important. If any question exists regarding the localization based on history and
examination, then imaging of the entire neuraxis (brain and spinal cord) should
be considered. This can help rule out other etiologies, such as spinal cord
compression, infarction, or myelitis, that may be missed by imaging only the
lumbosacral spine. Other potential mimickers of cauda equina dysfunction
include pudendal neuralgia (discussed in more detail below), side effects of
medications such as opiates and anticholinergics, neurodegenerative disorders
such as multiple system atrophy, and urologic disorders such as Fowler
syndrome (urinary retention in young women associated with polycystic ovaries
due to poor relaxation of the external urethral sphincter).22,29
In a 2018 series that reviewed 276 patients presenting with symptoms of cauda
equina dysfunction, 28% had positive scans, with 86% of those due to a herniated
disk; other causes included fracture, primary tumor, metastatic disease, and a
cyst.22 The study authors did not describe the full evaluation done on the patients
with negative MRIs but noted that these patients were more likely to have
comorbid psychiatric and functional disorders as well as chronic pain at
follow-up.22 In addition, only 1 out of 191 patients with negative MRIs was
found to have an explanatory neurologic disorder (transverse myelitis in that
case) at follow-up (mean follow-up time was 13 to 16 months).22
CONTINUUMJOURNAL.COM 209
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
NEUROSURGICAL INTERVENTION AND PROGNOSIS
Neurosurgery should be consulted immediately in a case of suspected cauda
equina dysfunction due to a compressive lesion. Early surgical intervention is
thought to be important in improving patient outcomes. In the literature, surgery
within 48 hours of symptom onset and after 48 hours is often compared. A large
meta-analysis found that surgery within 48 hours of symptom onset was
associated with improved outcomes, but no difference in outcomes was seen
in those who had surgery in less than 24 compared to within 48 hours.30
However, others have questioned this conclusion,31 and some studies have even
found that timing of surgery does not significantly alter outcomes.32,33 Because
of such mixed conclusions, surgical decompression is generally recommended
at the earliest time that it can be performed safely by an experienced
surgeon.33,34
The degree of neurologic dysfunction before surgery is the most consistent
prognostic factor in cauda equina syndrome.34 Most studies divide patients into
two categories based on presurgical symptoms: complete cauda equina syndrome
or incomplete cauda equina syndrome. Complete cauda equina syndrome is
defined as cauda equina syndrome with painless urinary retention and overflow
incontinence, whereas incomplete cauda equina syndrome is defined as cauda
equina syndrome with altered urinary sensation, poor stream, or a need to strain
during urination. Patients with incomplete cauda equina syndrome are often
cited as having a more favorable prognosis than those with complete cauda
equina syndrome.13,35 One large retrospective study (n = 136) found that all
patients had some recovery of bowel and bladder function postoperatively
independent of cauda equina syndrome type36; however, a smaller study (n = 22)
found that only pain improved after surgery in those with complete cauda equina
syndrome after a median follow-up of 75 months.37 Clinical improvement can
occur soon after surgery, but often improvement continues to occur slowly over
months to years.12,33 This is supported by the findings of Korse and colleagues,38
who noted that more dysfunction was reported in studies with a shorter
follow-up time. Although patients often have some improvement, persistent
deficits are common. Many patients (one study cited about 50%38) will still have
bowel, bladder, or sexual dysfunction at long-term follow-up.14,38,39
ETIOLOGIES OF CAUDA EQUINA DYSFUNCTION
The etiologies of cauda equina dysfunction are varied. The most common cause is
lumbar disk herniation. Other causes include nondiskogenic lumbar spinal
disease, vascular disorders, infectious or neoplastic disease, trauma, and
inflammatory or iatrogenic disorders (TABLE 9-1).
Diskogenic Cauda Equina Dysfunction
Disk herniations are the most common cause of cauda equina dysfunction,
occurring the majority of the time at the L4-L5 or L5-S1 level (CASE 9-1).17,18
However, only about 2% to 3% of all disk herniations requiring surgery result in
cauda equina syndrome.5,35 It is thought that a history of spinal disease, such as
spinal stenosis, is a risk factor for diskogenic cauda equina dysfunction since a
smaller disk herniation in this setting could lead to symptoms.8,17 Obesity is
another potential risk factor for cauda equina dysfunction due to disk
herniation.40,41 Cushnie and colleagues40 suggested an increase in epidural fat
(and thus reduced spinal canal diameter) in patients who are obese as a potential
210 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
mechanism. As discussed above, MRI should be obtained to confirm the KEY POINTS
diagnosis, and urgent neurosurgical intervention is recommended.
● Neurosurgery should be
consulted immediately in a
Lumbosacral Spinal Stenosis and Other Nondiskogenic Spine Disease case of suspected cauda
The onset of symptoms in cauda equina dysfunction from a herniated disk can be equina dysfunction due to a
sudden, but in cauda equina dysfunction secondary to lumbosacral spinal compressive lesion.
stenosis, the symptoms usually have an insidious onset because of degenerative
● The degree of neurologic
changes to the spinal canal over time. The degenerative changes result in loss of dysfunction before surgery
intervertebral disk height and hypertrophy of the ligamentum flavum, leading to is the most consistent
central stenosis and eventually compression of the cauda equina.42 Symptoms of prognostic factor in cauda
degenerative spinal stenosis commonly occur in the sixth or seventh decade but equina syndrome.
can occur earlier in those with a congenitally narrow spinal canal.42 Symptoms ● Disk herniations are the
usually start with pain that radiates from the low back and is made better by most common cause of
flexion of the low back. This can eventually progress and cause bladder dysfunction cauda equina dysfunction,
(and cauda equina syndrome), but this is rare.42,43 Similar to the way that occurring the majority of the
time at the L4-L5 or L5-S1
degenerative lumbar spinal stenosis can lead to cauda equina dysfunction, cases levels.
of spinal epidural lipomatosis directly causing cauda equina dysfunction have also
been reported.44,45 Spinal epidural lipomatosis may be idiopathic or secondary to
obesity, chronic corticosteroid use, or other endocrinopathies.44
Vascular Causes
People with aortic disease, especially abdominal aortic disease, can rarely present
with symptoms of cauda equina dysfunction, which is thought to be secondary to
nerve root ischemia from hypoperfusion or embolization.46 From these case
reports, it is not always entirely clear if the lumbosacral roots or the lumbosacral
spinal cord were actually affected. Still, in cases in which patients present with
symptoms of cauda equina dysfunction and MRI of the lumbosacral spine is
unrevealing, imaging of the abdominal aorta with MRA or CT angiography
should be considered. Symptoms similar to cauda equina dysfunction may also
be seen after a severe hypotensive event such as cardiac arrest. One study
evaluating pathology specimens from patients who died after a cardiac arrest or
severe hypotension found that neurons in the lumbosacral spinal cord were
actually much more susceptible to ischemic injury than those in other spinal cord
levels (even midthoracic), but the nerve roots were not examined.47
Spinal hematomas, either intradural or epidural, can cause compression of the
lumbosacral nerve roots and cauda equina dysfunction. In some cases, neurologic
symptoms may be preceded by hours or days of back pain.48 Spinal hematomas
can occur spontaneously; may be secondary to coagulopathy, trauma, or vascular
anomalies; or may occur after intervention from a surgery or procedure.
Asymptomatic spinal epidural hematomas are common after lumbosacral spine
surgery, occurring in 33% to 100% of people, whereas symptomatic postoperative
spinal epidural hematomas are rare, occurring in only 0.1% to 0.2% of cases.49
However, in one large retrospective study of 15,668 patients in whom the etiology
was known, 6.3% of cauda equina syndrome cases were listed as secondary to
postoperative hematoma.50 For this reason, clinicians should have a high index of
suspicion and patients should be rescanned after surgery if any concern exists.
One case report describes engorgement of the epidural venous plexus
occurring postoperatively, leading to dural sac shift and cauda equina
dysfunction.51 In this particular case, the dural sac shift was treated with
laminoplasty and had a good clinical outcome.51 Epidural venous plexus
CONTINUUMJOURNAL.COM 211
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
enlargement (seen as signal flow voids on MRI of the lumbosacral spine) leading
to cauda equina dysfunction can also occur secondary to occlusion of the inferior
vena cava.52 This most commonly occurs because of thrombosis in the inferior
vena cava but can occur secondary to occlusion from a mass or from pregnancy.
Occlusion of the inferior vena cava can be visualized on MRI of the lumbosacral
spine but is usually confirmed with Doppler ultrasound. In one case series, all
TABLE 9-1 Causes of Cauda Equina Dysfunction
Diskogenic and nondiskogenic structural spinal disease
◆ Lumbosacral disk herniation
◆ Lumbosacral spinal stenosis
◆ Spinal epidural lipomatosis
Vascular
◆ Spinal hematoma
◆ Aortic disease (eg, dissection, thrombosed aneurysm)
◆ Dural arteriovenous fistula
Neoplastic
◆ Myxopapillary ependymoma
◆ Leptomeningeal metastasis
◆ Skeletal metastases (eg, lung, breast, prostate cancer)
◆ Schwannoma
◆ Paraganglioma
◆ Neurofibroma
◆ Meningioma
◆ Non-Hodgkin lymphoma
◆ Chordoma
◆ Chondrosarcoma
◆ Ewing sarcoma
◆ Hemangioblastoma
◆ Dermoid tumor
◆ Glioma
◆ Drop metastasis from primary brain tumors
Inflammatory
◆ Sarcoidosis
◆ Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP)
◆ Chronic immune sensory polyradiculopathy
◆ Acute inflammatory demyelinating polyradiculoneuropathy (AIDP)
◆ Vasculitis
CONTINUED ON PAGE 213
212 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
patients had resolution of their neurologic symptoms after treatment of the vena
cava occlusion.51 Similarly, a spinal dural arteriovenous fistula can lead to or
mimic cauda equina syndrome. This disorder can be difficult to diagnose;
contrast-enhanced MRA of the spine can help localize the fistula, and digital
subtraction angiography is used to confirm the diagnosis.53 For more information
regarding spinal dural arteriovenous fistulas and other vascular disorders of the
CONTINUED FROM PAGE 212
◆ Ankylosing spondylitis
◆ Graft versus host disease
Infectious
◆ Spinal epidural abscess
◆ Lyme disease
◆ Elsberg syndrome (herpes simplex virus type 2)
◆ Cytomegalovirus
◆ Varicella-zoster virus
◆ Human immunodeficiency virus (HIV)
◆ Herpes simplex virus type 1
◆ Epstein-Barr virus
◆ Syphilis
◆ Tuberculosis
◆ Cysticercosis
◆ Schistosomiasis
◆ Hydatid cysts
◆ Cryptococcosis
◆ Nocardiosis
◆ Brucellosis
◆ Tick-borne encephalitis
Iatrogenic
◆ Radiation induced
◆ Arachnoiditis
◆ Epidural pneumorrhachis (entrapment of air/gas within spinal column)
◆ Intrathecal cytarabine or methotrexate
◆ Complication of spinal anesthesia
Other
◆ Trauma
◆ Extramedullary hematopoiesis
◆ Calcifying non-neoplastic pseudoneoplasm
CONTINUUMJOURNAL.COM 213
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
spinal cord, refer to the article “Vascular Myelopathies” by Nicholas L. Zalewski,
MD,54 in this issue of Continuum.
Infectious Causes
Constitutional symptoms, such as fevers, night sweats, and weight loss, should
lead to consideration of an infectious etiology of cauda equina dysfunction in the
appropriate clinical setting. Spinal epidural abscesses are a potential infectious
cause of cauda equina dysfunction. Back pain at the level of the abscess (present
in 75% of patients) and fever (present in 50% of patients) are the most common
symptoms.55 The symptoms may be present for days or up to 2 months in some
cases. Predisposing factors include, but are not limited to, diabetes, alcohol use
disorder, human immunodeficiency virus (HIV), spine abnormality or recent
intervention, sepsis or other current infection, and IV drug use.55 Two-thirds of
cases are caused by Staphylococcus aureus; other common pathogens include
Staphylococcus epidermidis, Escherichia coli, and Pseudomonas aeruginosa.55
Infection from other pathogens, such as tuberculosis, fungi, or parasites, is
rare.55-57 If infection is present, erythrocyte sedimentation rate and C-reactive
protein will be elevated, and blood cultures should be obtained. Diagnosis is
CASE 9-1 A 35-year-old man with a history of chronic back pain presented to the
emergency department with worsening back pain, lower extremity and
saddle paresthesia, urinary retention, and a feeling of weakness in his
feet. He said he had been playing basketball 4 days prior and “twisted”
his back, causing worsening of his typical back pain. He thought the pain
was improving, but shortly before coming to the emergency department,
he stood up and felt a sudden worsening of low back pain and developed
numbness and tingling in his legs and perineum. He felt the need to
urinate but had been unable to do so; he denied bowel symptoms. He had
no other significant past medical history except for morbid obesity.
Neurologic examination revealed normal strength, left greater than
right perianal numbness and patchy distal lower extremity numbness to
pinprick, a reduced left ankle reflex, and normal rectal tone. MRI of the
lumbosacral spine (FIGURE 9-2) revealed a large disk herniation at L5-S1
compressing the cauda equina. Underlying central spinal stenosis existed
secondary to significant ventral epidural fat.
Emergent L5-S1 microdiskectomy was performed within 24 hours of
symptom onset. At a follow-up visit 8 months later, he reported a
continued pins and needles sensation in his feet, saddle paresthesia, and
a feeling of weakness in his feet that was still gradually improving. He
denied any residual bladder dysfunction.
214 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
made with MRI with and without contrast or CT myelography if MRI cannot be
performed, as both are more than 90% sensitive.55 CSF evaluation is not
recommended (unless myelography is needed) since the culture yield is low and
a small risk exists of causing meningitis or a subdural infection from the lumbar
puncture. In most cases, emergency decompressive surgery and antibiotic
treatment are recommended.55
In a patient with HIV, usually with a CD4 count of less than 100 cells/mm3,
an infectious cause of cauda equina dysfunction must be considered. An acute
polyradiculopathy due to involvement of lumbosacral nerve roots occurs in
about 2% of patients with HIV.58 In this population, this is most frequently
caused by cytomegalovirus (CMV), herpes simplex virus type 1 (HSV-1) or
type 2 (HSV-2), varicella-zoster virus (VZV), or tuberculosis.59 HIV itself is
also a rare cause of polyradiculopathy or polyradiculoneuropathy, especially at
the time of seroconversion. This is more likely to present as GBS or pure motor
polyradiculopathy than as cauda equina syndrome.60
CMV (usually seen in patients with HIV or other patients who are
immunocompromised, as previously mentioned) can cause cauda equina
dysfunction through invasion of the lumbosacral nerve roots, with clinical signs
FIGURE 9-2
Imaging of the patient in CASE 9-1. Sagittal (A) and axial (B) T2-weighted MRIs of the
lumbosacral spine show a large extruded disk fragment (arrows) compressing the thecal
sac. The prominent epidural fat seen in this patient is not shown in these T2-weighted
images.
This case illustrates a typical case of cauda equina dysfunction secondary to COMMENT
lumbosacral disk herniation at the L5-S1 level. This patient had a risk factor of
obesity with central canal stenosis that was already present to some degree
because of epidural lipomatosis. None of the hospital notes for this patient
commented on sexual dysfunction, but this should be discussed with every
patient in whom cauda equina dysfunction is suspected. Surgery was
performed within 24 hours of symptom onset in this patient. At follow-up,
the patient reported improvement but still had some neurologic symptoms,
which is not uncommon.
CONTINUUMJOURNAL.COM 215
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
and symptoms of areflexia, weakness, sensory disturbance, and urinary
retention. In some patients, the infection can spread to affect the upper
extremities and cranial nerves as well. Often MRI of the spinal cord will show
contrast enhancement of the nerve roots and meninges and T2-hyperintense
lesions in the cord itself.61 CSF will often have a mixed pleocytosis, low glucose,
and protein elevation. CMV DNA found in the CSF is specific, and patients
should be treated with IV ganciclovir or foscarnet, or both.61
HSV-2 and VZV can cause a presentation similar to CMV. Elsberg syndrome is
an acute or subacute presentation of lumbosacral radiculitis, often with myelitis,
that is associated with HSV-2 infection. A retrospective review of patients from the
Mayo Clinic with Elsberg syndrome found that Elsberg syndrome likely accounts
for about 10% of patients with a clinical presentation of cauda equina syndrome
and myelitis.62 Out of 30 patients, only two had a preceding genital herpes infection.
Other clues to the diagnosis include an acute presentation (potentially distinguishing
it from neoplastic or inflammatory causes), smooth (rather than nodular) nerve
root enhancement on MRI, and, if present, spinal cord lesions that are multiple
and discontinuous. HSV can rapidly clear from the CSF, so a high clinical suspicion
should exist even in the absence of positive CSF polymerase chain reaction (PCR).
VZV may be more likely than HSV-2 when more lesions are present higher in the
spinal cord, in the presence of a longitudinally extensive lesion, or when
encephalitis is present. Both VZV and HSV-2 are treated with acyclovir, and
treatment should be considered even when CSF studies are nondiagnostic.62
Polyradiculopathy can be seen in half of patients with peripheral nerve
involvement due to Lyme disease. Pain and sensory loss are the most common
symptoms and typically have an acute onset within the first couple of months
of infection.63 This disorder may be underrecognized since the symptoms can be
self-limited and CSF may not be abnormal (although a lymphocytic pleocytosis
and elevated protein are commonly seen). On EMG, abnormalities may be seen
in paraspinal muscles; however, this should be true in most polyradiculopathies,
so this finding is not specific. Previous rash, arthralgia, facial palsy, or a known
environmental exposure can be helpful in making the diagnosis.63
Other potential infectious causes of cauda equina dysfunction include
tuberculosis,64 cryptococcosis,65 neurosyphilis,66 schistosomiasis,67
cysticercosis,68 Epstein-Barr virus,69 nocardiosis,70 brucellosis,71 and tick-borne
encephalitis.72 For more information on infectious causes, refer to the article
“Infectious Myelopathies” by Michel Toledano, MD,73 in this issue of Continuum.
Neoplastic Causes
In one large retrospective study, cauda equina syndrome was secondary to tumor
in 3.1% of patients (478 of 15,668 patients with a reported etiology).50 Neoplastic
disease can lead to cauda equina dysfunction by direct compression from
primary or metastatic lesions or secondary to nerve root invasion from
meningeal-based disease. It is more common for cauda equina dysfunction from
tumors to present in a subacute or chronic fashion compared to cauda equina
dysfunction resulting from other causes.
Ependymomas are the most common primary tumor of the spinal cord in adults
and the most common primary tumor to affect the cauda equina. Specifically,
myxopapillary ependymomas are more likely to occur below the conus medullaris
than other types of ependymomas.74 These tumors grow slowly, arising from
the ependymal cells in the central canal. On MRI, they typically enhance with
216 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
contrast and appear to be intradural-extramedullary when affecting the cauda equina. KEY POINTS
Other tumors that can rarely lead to cauda equina dysfunction or involve the
● Constitutional symptoms,
lumbosacral nerve roots include schwannomas, neurofibromas, meningiomas, such as fevers, night sweats,
hemangioblastomas, dermoid tumors, chordomas, and gliomas.74-76 Cauda equina and weight loss, should lead
dysfunction can also occur secondary to compression from metastatic disease, most to consideration of an
frequently from lung cancer, breast cancer, prostate cancer, or multiple myeloma.74,75 infectious etiology of cauda
equina dysfunction in the
Leptomeningeal disease can also lead to cauda equina dysfunction. This is often
appropriate clinical setting.
due to lung or breast cancer but has been reported from a large range of cancers.
Rarely, invasion of the lumbosacral nerve roots can occur with leukemia77 or ● Elsberg syndrome likely
lymphoma, most commonly related to diffuse large B-cell lymphoma.78 Drop accounts for about 10% of
metastases from brain tumors such as medulloblastomas, ependymomas, patients with a clinical
presentation of cauda equina
germinomas, choroid plexus carcinomas, and glioblastomas can also lead to syndrome and myelitis.
leptomeningeal disease.74 MRI of the spine with and without contrast may show
nodular enhancement along the nerve roots or meninges. At least 10.5 mL of CSF ● Myxopapillary
should be sent for cytology, and the test should be repeated if negative to minimize ependymomas are the most
common primary tumor to
false-negative results.79 Flow cytometry should also be conducted when affect the cauda equina.
hematologic malignancy is suspected to increase the sensitivity.80
● Sarcoidosis is likely the
Inflammatory Causes most common inflammatory
Sarcoidosis presenting with cauda equina dysfunction is rare, but it is still likely disorder that can present
with cauda equina
the most common inflammatory cause of cauda equina syndrome (CASE 9-2).75,82 dysfunction.
About 5% of patients with sarcoidosis will have nervous system involvement
(neurosarcoidosis), with only about one-fifth of these cases affecting the peripheral
nerves or spinal roots.83 Of those with neuropathy, polyradiculoneuropathy was
the most common pattern in one series, seen in 22 of 57 patients. The most
commonly reported symptoms were pain and sensory symptoms, and only 8 of the
57 patients reported bowel or bladder symptoms.83 Other symptoms commonly
seen in this case series that may serve as diagnostic clues included fatigue, fever,
unexplained weight loss, arthralgia, and skin and eye involvement. The disease
course was most commonly acute or subacute, but some patients had an insidious
onset.83 MRI of the lumbosacral spine in neurosarcoidosis may show nodular
thickening of the nerve roots and enhancement. CSF findings are nonspecific;
protein elevation is the most common finding, whereas a pleocytosis or reduced
glucose are less common. As in any case of suspected neurosarcoidosis, CT of the
chest is important to look for pulmonary involvement. Positron emission
tomography (PET)-CT may be more sensitive to detection of systemic sarcoid
and can be considered if CT of the chest is negative. If the diagnosis is still
unclear, biopsy is necessary (in cases of polyradiculoneuropathy, biopsy would
likely be of the leptomeninges or nerve and muscle).
Peripheral nerve vasculitis presenting with cauda equina dysfunction has been
described in association with systemic lupus erythematosus.84 Cauda equina
syndrome has also been reported in association with ankylosing spondylitis and
graft versus host disease.85,86 Other inflammatory disorders to consider include
GBS,87 CIDP,88 and chronic immune sensory polyradiculopathy (CISP), since
lumbosacral root involvement can predominate the clinical picture and bowel
and bladder dysfunction can rarely occur.
Iatrogenic Causes
As discussed above, spinal hematomas occurring after surgery may cause cauda
equina syndrome. Epidural injections of anesthetics and analgesics have also
CONTINUUMJOURNAL.COM 217
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
CASE 9-2 A 45-year-old man with no significant past medical history presented
with several weeks of worsening low back pain, progressive lower
extremity weakness and sensory changes, saddle anesthesia, and urinary
retention. He had also noticed shortness of breath and arthralgia over the
past 2 months.
Neurologic examination showed normal cranial nerves and upper
extremity strength, 4/5 strength diffusely in the lower extremities,
reduced lower extremity reflexes, and reduced sensation in the perineum
and in a length-dependent pattern in the lower extremities. MRI of the
lumbosacral spine showed nodular enhancement in the cauda equina and
in the vertebrae, similar to the MRI example in FIGURE 9-3.81 CSF
analysis showed a protein of 101 mg/dL, white blood cell count
of 50 cells/mm3, low glucose, and a normal angiotensin-converting
enzyme level. Cytology was negative for malignant cells, and all
infectious studies were
negative. Nerve conduction
study/EMG was also
performed and showed
abnormal spontaneous
activity in the lumbar
paraspinal muscles and a
length-dependent
sensorimotor axonal
neuropathy. CT of the
chest showed hilar
lymphadenopathy, which was
ultimately biopsied and
consistent with sarcoidosis.
He was treated with IV FIGURE 9-3
methylprednisolone followed Nodular enhancement of the cauda equina
and vertebrae.
by oral prednisone and started Reprinted from Hoyle JC, et al, Neurohospitalist.81 © 2014
on mycophenolate mofetil. SAGE Publications.
COMMENT The progression of symptoms over several weeks in this patient was
suspicious for an inflammatory process, and the symptoms of arthralgia
and shortness of breath were clues to the diagnosis. The possibility of
infection should be evaluated fully, especially since CSF findings in
sarcoidosis can appear similar to an infection, with a high white blood cell
count and low glucose. In addition, given the CSF findings and nodular
enhancement on MRI, it was also necessary to ensure that no signs of
malignancy were present in the CSF or elsewhere in this patient. The
diagnosis of sarcoidosis is made from tissue biopsy. If no lung involvement
had been found in this patient, then biopsy of the meninges would have
been considered.
218 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
been associated with cauda equina dysfunction. In some cases, a subarachnoid KEY POINTS
(rather than epidural) injection was performed, inadvertently leading to
● Trauma, especially from
lumbosacral polyradiculopathy.89 In other cases in which an epidural injection motor vehicle accidents,
was performed correctly, it is thought that patients who developed cauda equina falls, and gunshot wounds, is
dysfunction may have been at greater risk because of a history of spinal stenosis a potential cause of cauda
or adhesive arachnoiditis.89,90 A possible reason for this is that edema caused equina syndrome, often
because of a low lumbar or
by the injection may lead to compression of the lumbosacral nerve roots.89
transverse sacral fracture.
Adhesive arachnoiditis itself may also present with cauda equina dysfunction.91
In adhesive arachnoiditis, the arachnoid is thickened and scarred and may lead to ● Although not technically a
nerve ischemia.75 It is most commonly caused by myelographic contrast agents disorder of the cauda
or other intrathecal injections and spinal operations.91 The treatment of adhesive equina, pudendal
neuropathy can closely
arachnoiditis is usually conservative, with medications and physical therapy; mimic cauda equina
surgical treatment is sometimes used, depending on the specific case.92 syndrome since it originates
Radiation can also cause lumbosacral polyradiculopathy. This typically from the S2 through S4
occurs about 6 years after exposure but can occur as soon as several months nerve roots and innervates
the perineum.
after or as late as 25 years after radiation.75 This is mostly reported as a
pure motor syndrome, with less than one-third of patients reporting sensory
symptoms and many without pain. MRI may sometimes show nodular
nerve root enhancement, making it difficult to distinguish from a neoplastic
meningitis.75,93,94
Other Causes
Trauma, especially from motor vehicle accidents, falls, and gunshot wounds, is a
potential cause of cauda equina dysfunction. Often this is because of low lumbar
or transverse sacral fractures.95,96 No prospective trials have evaluated the best
treatment for such fractures. A 2018 meta-analysis of case reports and
retrospective case series that included a total of 521 patients with transverse sacral
fractures found that surgically treated and nonoperatively treated patients
showed no significant difference in neurologic recovery. In patients who were
surgically treated, fracture fixation in addition to decompression resulted in
greater neurologic recovery.97
Several case reports have described extramedullary hematopoiesis as a cause
of cauda equina dysfunction. Extramedullary hematopoiesis is hematopoiesis
that occurs outside of the bone marrow, which is normal during embryonic and
fetal development. However, it can occur as a pathologic process in people with
thalassemia and, less commonly, myelofibrosis, polycythemia, and sickle cell
disease. The spleen, liver, and lymph nodes are common sites of extramedullary
hematopoiesis, but rarely extramedullary hematopoiesis can occur in the spinal
canal, leading to neurologic symptoms.98 On MRI of the spine, this may appear as
multiple rounded masses or a single mass in the epidural space, typically contrast
enhancing with variable signal characteristics.98,99 No clear treatment of choice
has been identified, but surgical decompression, transfusion, hydroxyurea, and
radiation therapy have all been tried.98
Although not technically a disorder of the cauda equina, pudendal neuropathy
can closely mimic cauda equina dysfunction since the pudendal nerve originates
from the S2 through S4 nerve roots and innervates the perineum.100 It most
commonly presents as a neuralgia, with perineal pain that is worse with sitting
because of pressure on the perineum.75 Sensory symptoms of numbness can
occur, as can bowel, bladder, and sexual dysfunction if the neuropathy is
bilateral.75,101 A key difference between pudendal neuropathy and true cauda
CONTINUUMJOURNAL.COM 219
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
equina syndrome is that the pain in cauda equina syndrome is more commonly in
the lower back and legs and less often described as in the perineum. Pudendal
neuralgia occurs secondary to compression or entrapment from pelvic fractures,
bicycle seats, neoplasm, childbirth, or muscle or iatrogenic injury.101-103 The
diagnosis is challenging since objective findings can be difficult to demonstrate.
Nerve conduction studies of the pudendal nerve are not often performed and are
of unclear sensitivity and specificity for identifying a nerve injury.75 Denervation
of the external anal sphincter would be supportive of nerve injury; however,
external anal sphincter EMGs are technically challenging, and if the EMG is
normal, pudendal nerve dysfunction still cannot be ruled out (the same is true
when using these techniques to assess for cauda equina dysfunction in general).
MRI, especially MRI neurography, may be helpful in some cases.104 Symptoms of
pudendal neuropathy can be treated symptomatically with medications or
sometimes with pudendal nerve block.105 Surgery should generally not be
performed unless a clear etiology is identified or if the patient is severely
affected.75,106
CONCLUSION
Cauda equina syndrome is a neurologic emergency requiring timely diagnosis
and treatment. Important clinical characteristics include radiating low back pain,
perineal and lower extremity sensory disturbances, urinary and bowel
dysfunction, and lower extremity weakness. Although diskogenic causes account
for most cases, nondiskogenic etiologies must also be considered. An
understanding of cauda equina anatomy; clinical presentation; and the value of
diagnostic studies such as MRI, CSF evaluation, and nerve conduction studies
and EMG is necessary to provide the best chance for neurologic recovery.
REFERENCES
1 Mixter W, Barr J. Rupture of the intervertebral 6 Stewart JD. Focal peripheral neuropathies,
disc with involvement of the spinal canal. 4th ed. JBJ Publishing, 2010.
N Engl J Med 1934;211:210-215. doi:10.1056/
7 Ridley LJ, Han J, Ridley WE, Xiang H. Cauda
NEJM193408022110506
equina: normal anatomy. J Med Imaging
2 Fuso FAF, Dias ALN, Letaif OB, et al. Radiat Oncol 2018;62 Suppl 1:123.
Epidemiological study of cauda equina doi:10.1111/1754-9485.04_12786
syndrome. Acta Ortop Bras 2013;21(3):159-162.
8 Tarulli AW. Disorders of the cauda equina.
doi:10.1590/S1413-78522013000300006
Continuum (Minneap Minn) 2015;21(1 Spinal Cord
3 Woodfield J, Hoeritzauer I, Jamjoom AAB, et al. Disorders):146-158. doi:10.1212/01.
Understanding cauda equina syndrome: CON.0000461090.09736.45
protocol for a UK multicentre prospective
9 McNamee J, Flynn P, O'Leary S, et al. Imaging in
observational cohort study. BMJ Open 2018;8(12):
cauda equina syndrome—a pictorial review.
e025230. doi:10.1136/bmjopen-2018-025230
Ulster Med J 2013;82(2):100-108.
4 Podnar S. Epidemiology of cauda equina and
10 Spector LR, Madigan L, Rhyne A, et al.
conus medullaris lesions. Muscle Nerve 2007;
Cauda equina syndrome. J Am Acad Orthop Surg
35(4):529-531. doi:10.1002/mus.20696
2008;16(8):471-479. doi:10.5435/
5 Fraser S, Roberts L, Murphy E. Cauda equina 00124635-200808000-00006
syndrome: a literature review of its definition and
11 Parke WW, Gammell K, Rothman RH. Arterial
clinical presentation. Arch Phys Med Rehabil
vascularization of the cauda equina. J Bone Joint
2009;90(11):1964-1968. doi:10.1016/j.
Surg Am 1981;63(1):53-62.
apmr.2009.03.021
220 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
12 Kostuik JP, Harrington I, Alexander D, et al. Cauda 25 Bell DA, Collie D, Statham PF. Cauda equina
equina syndrome and lumbar disc herniation. syndrome: what is the correlation between
J Bone Joint Surg Am 1986;68(3):386-391. clinical assessment and MRI scanning? Br J
Neurosurg 2007;21(2):201-203.
13 Gardner A, Gardner E, Morley T. Cauda equina
doi:10.1080/02688690701317144
syndrome: a review of the current clinical and
medico-legal position. Eur Spine J 2011;20(5): 26 Dionne N, Adefolarin A, Kunzelman D, et al. What
690-697. doi:10.1007/s00586-010-1668-3 is the diagnostic accuracy of red flags related to
cauda equina syndrome (CES), when compared
14 Korse NS, Pijpers JA, van Zwet E, et al. Cauda
to magnetic resonance imaging (MRI)? A
equina syndrome: presentation, outcome, and
systematic review. Musculoskelet Sci Pract 2019;
predictors with focus on micturition, defecation,
42:125-133. doi:10.1016/j.msksp.2019.05.004
and sexual dysfunction. Eur Spine J 2017;26(3):
894-904. doi:10.1007/s00586-017-4943-8 27 Venkatesan M, Nasto L, Tsegaye M, Grevitt M.
Bladder scans and postvoid residual volume
15 Mazanec DJ. Back pain: medical evaluation and
measurement improve diagnostic accuracy of
therapy. Cleve Clin J Med 1995;62(3):163-168.
cauda equina syndrome. Spine (Phila Pa 1976)
doi:10.3949/ccjm.62.3.163
2019;44(18):1303-1308. doi:10.1097/
16 Deyo RA, Weinstein JN. Low back pain. N Engl J BRS.0000000000003152
Med 2001;344(5):363-370. doi:10.1056/
28 Peacock JG, Timpone VM. Doing more with less:
NEJM200102013440508
diagnostic accuracy of CT in suspected cauda
17 Long B, Koyfman A, Gottlieb M. Evaluation and equina syndrome. AJNR Am J Neuroradiol
management of cauda equina syndrome in the 2017;38(2):391-397. doi:10.3174/ajnr.A4974
emergency department. Am J Emerg Med 2020;
29 Swinn MJ, Fowler CJ. Isolated urinary retention in
38(1):143-148. doi:10.1016/j.ajem.2019.158402
young women, or Fowler's syndrome. Clin Auton
18 Shapiro S. Medical realities of cauda equina Res 2001;11(5):309-311. doi:10.1007/BF02332976
syndrome secondary to lumbar disc herniation.
30 Ahn UM, Ahn NU, Buchowski JM, et al. Cauda
Spine (Phila Pa 1976) 2000;25(3):348-351;
equina syndrome secondary to lumbar disc
discussion 352. doi:10.1097/
herniation: a meta-analysis of surgical outcomes.
00007632-200002010-00015
Spine (Phila Pa 1976) 2000;25(12):1515-1522.
19 Goodman BP. Disorders of the cauda equina.
31 Kohles SS, Kohles DA, Karp AP, et al.
Continuum (Minneap Minn) 2018;24(2, Spinal
Time-dependent surgical outcomes following
Cord Disorders):584-602. doi:10.1212/
cauda equina syndrome diagnosis: comments on
CON.0000000000000584
a meta-analysis. Spine (Phila Pa 1976) 2004;29(11):
20 Sherlock KE, Turner W, Elsayed S, et al. The 1281-1287.
evaluation of digital rectal examination for
32 Qureshi A, Sell P. Cauda equina syndrome
assessment of anal tone in suspected cauda
treated by surgical decompression: the influence
equina syndrome. Spine (Phila Pa 1976)
of timing on surgical outcome. Eur Spine J 2007;
2015;40(15):1213-1218. doi:10.1097/
16(12):2143-2151. doi:10.1007/s00586-007-0491-y
BRS.0000000000000902
33 Kaiser R, Nasto LA, Venkatesan M, et al. Time
21 Angus M, Horner D. BET 2: is sexual dysfunction a
factor and disc herniation size: are they really
recognised sign of cauda equina syndrome in the
predictive for outcome of urinary dysfunction in
ED? Emerg Med J 2019;36(8):508-510. doi:10.1136/
patients with cauda equina syndrome?
emermed-2019-208777.2
Neurosurgery 2018;83(6):1193-1200. doi:10.1093/
22 Hoeritzauer I, Pronin S, Carson A, et al. The neuros/nyx607
clinical features and outcome of scan-negative
34 Chau AM, Xu LL, Pelzer NR, Gragnaniello C.
and scan-positive cases in suspected cauda
Timing of surgical intervention in cauda equina
equina syndrome: a retrospective study of 276
syndrome: a systematic critical review. World
patients. J Neurol 2018;265(12):2916-2926.
Neurosurg 2014;81(3-4):640-650. doi:10.1016/
doi:10.1007/s00415-018-9078-2
j.wneu.2013.11.007
23 Fairbank J, Hashimoto R, Dailey A, et al. Does
35 Gleave JR, Macfarlane R. Cauda equina
patient history and physical examination predict
syndrome: what is the relationship between
MRI proven cauda equina syndrome? Evid Based
timing of surgery and outcome? Br J Neurosurg
Spine Care J 2011;2(4):27-33. doi:10.1055/
2002;16(4):325-328. doi:
s-0031-1274754
10.1080/0268869021000032887
24 Ahad A, Elsayed M, Tohid H. The accuracy of
36 Heyes G, Jones M, Verzin E, et al. Influence of
clinical symptoms in detecting cauda equina
timing of surgery on cauda equina syndrome:
syndrome in patients undergoing acute MRI of
outcomes at a national spinal centre. J Orthop
the spine. Neuroradiol J 2015;28(4):438-442.
2018;15(1):210-215. doi:10.1016/j.jor.2018.01.020
doi:10.1177/1971400915598074
37 Delgado-López PD, Martín-Alonso J,
Martín-Velasco V, et al. Cauda equina syndrome
due to disk herniation: long-term functional
prognosis. Neurocirugia (Astur) 2019;30(6):
278-287. doi:10.1016/j.neucir.2019.05.002
CONTINUUMJOURNAL.COM 221
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
38 Korse NS, Jacobs WCH, Elzevier HW, 51 Maki Y, Takayama M, Hayashi H, et al. Cauda
Vleggeert-Lankamp CL. Complaints of equina syndrome due to dural sac shift with
micturition, defecation and sexual function in engorgement of the epidural venous plexus: rare
cauda equina syndrome due to lumbar disk complication after lumbar microdiscectomy.
herniation: a systematic review. Eur Spine J 2013; World Neurosurg 2017;104:1048.e15-1048.e18.
22(5):1019-1029. doi:10.1007/s00586-012-2601-8 doi:10.1016/j.wneu.2017.05.078
39 Hazelwood JE, Hoeritzauer I, Pronin S, 52 Paksoy Y, Gormus N. Epidural venous plexus
Demetriades AK. An assessment of enlargements presenting with radiculopathy and
patient-reported long-term outcomes following back pain in patients with inferior vena cava
surgery for cauda equina syndrome. Acta obstruction or occlusion. Spine (Phila Pa 1976)
Neurochir (Wien) 2019;161(9):1887-1894. doi: 2004;29(21):2419-2424. doi:10.1097/01.
10.1007/s00701-019-03973-7 brs.0000144354.36449.2f
40 Cushnie D, Urquhart JC, Gurr KR, et al. Obesity 53 Mull M, Othman A, Dafotakis M, et al. Spinal
and spinal epidural lipomatosis in cauda equina epidural arteriovenous fistula with perimedullary
syndrome. Spine J 2018;18(3):407-413. doi:10.1016/ venous reflux: clinical and neuroradiologic
j.spinee.2017.07.177 features of an underestimated vascular disorder.
AJNR Am J Neuroradiol 2018;39(11):2095-2102.
41 Venkatesan M, Uzoigwe CE, Perianayagam G,
doi:10.3174/ajnr.A5854
et al. Is cauda equina syndrome linked with
obesity? J Bone Joint Surg Br 2012;94(11):1551-1556. 54 Zalewski NL. Vascular myelopathies. Continuum
doi:10.1302/0301-620X.94B11.29652 (Minneap Minn) 2021;27(1, Spinal Cord Disorders):
30-61.
42 Storm PB, Chou D, Tamargo RJ. Lumbar spinal
stenosis, cauda equina syndrome, and multiple 55 Darouiche RO. Spinal epidural abscess. N Engl J
lumbosacral radiculopathies. Phys Med Rehabil Med 2006;355(19):2012-2020. doi:10.1056/
Clin N Am 2002;13(3):713-733, ix. doi:10.1016/ NEJMra055111
s1047-9651(02)00013-x
56 Hasan GA, Kani SM, Alqatub A. Tuberculous
43 Sheehan JM, Shaffrey CI, Jane JA Sr. lumbar spinal epidural abscess in a young adult
Degenerative lumbar stenosis: the neurosurgical (case report). SICOT J 2018;4:5. doi:10.1051/
perspective. Clin Orthop Relat Res 2001(384): sicotj/2018005
61-74.
57 Shweikeh F, Zyck S, Sweiss F, et al. Aspergillus
44 Kim YS, Ju CI, Kim SW, Kim HS. Cauda equina spinal epidural abscess: case presentation and
syndrome caused by idiopathic epidural review of the literature. Spinal Cord Ser Cases
lipomatosis. Korean J Spine 2015;12(4):272-274. 2018;4:19. doi:10.1038/s41394-018-0046-y
doi:10.14245/kjs.2015.12.4.272
58 Corral I, Quereda C, Casado JL, et al. Acute
45 Wells AJ, McDonald MJ, Sandler SJ, Vrodos NJ. polyradiculopathies in HIV-infected patients.
Lumbosacral epidural lipomatosis causing rapid J Neurol 1997;244(8):499-504. doi:10.1007/
onset cauda equina syndrome. J Clin Neurosci s004150050132
2014;21(7):1262-1263. doi:10.1016/j.jocn.2013.
59 Panos G, Watson DC, Karydis I, et al. Differential
09.027
diagnosis and treatment of acute cauda equina
46 He F, Xing T, Yu F, et al. Cauda equina syndrome: syndrome in the human immunodeficiency virus
an uncommon symptom of aortic diseases. Int J positive patient: a case report and review of the
Clin Exp Med 2015;8(7):10760-10766. literature. J Med Case Rep 2016;10:165.
doi:10.1186/s13256-016-0902-y
47 Duggal N, Lach B. Selective vulnerability of the
lumbosacral spinal cord after cardiac arrest and 60 Benatar MG, Eastman RW. Human
hypotension. Stroke 2002;33(1):116-121. doi:10.1161/ immunodeficiency virus-associated pure motor
hs0102.101923 lumbosacral polyradiculopathy. Arch Neurol
2000;57(7):1034-1039. doi:10.1001/
48 Bhatt D, Bhatt D, Bhatt N. Cauda equina
archneur.57.7.1034
syndrome caused by a spontaneous spinal
haematoma. BMJ Case Rep 2015;2015: 61 Maschke M, Kastrup O, Diener HC. CNS
bcr2014208583. doi:10.1136/bcr-2014-208583 manifestations of cytomegalovirus infections:
diagnosis and treatment. CNS Drugs 2002;16(5):
49 Kaner T, Sasani M, Oktenoglu T, et al.
303-315. doi:10.2165/00023210-200216050-00003
Postoperative spinal epidural hematoma
resulting in cauda equina syndrome: a case 62 Savoldi F, Kaufmann TJ, Flanagan EP, et al.
report and review of the literature. Cases J 2009; Elsberg syndrome: a rarely recognized cause
2:8584. doi:10.4076/1757-1626-2-8584 of cauda equina syndrome and lower
thoracic myelitis. Neurol Neuroimmunol
50 Hogan WB, Kuris EO, Durand WM, et al. Timing of
Neuroinflamm 2017;4(4):e355. doi:10.1212/
surgical decompression for cauda equina
NXI.0000000000000355
syndrome. World Neurosurg 2019;132:e732-e738.
doi:10.1016/j.wneu.2019.08.030 63 Halperin JJ. Lyme disease and the peripheral
nervous system. Muscle Nerve 2003;28(2):
133-143. doi:10.1002/mus.10337
222 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
64 Pluemvitayaporn T, Jindahra S, Pongpinyopap W, 78 Sasaki R, Ohta Y, Yamada Y, et al.
et al. Concomitant mycotic abdominal aortic Neurolymphomatosis in the cauda equina
aneurysm and lumbar tuberculous spondylitis diagnosed by an open biopsy. Intern Med 2018;
with cauda equina syndrome: a rare condition—a 57(23):3463-3465. doi:10.2169/
case report and literature review. Spinal Cord Ser internalmedicine.1049-18
Cases 2018;4:13. doi:10.1038/s41394-018-0047-x
79 Glantz MJ, Cole BF, Glantz LK, et al.
65 Jongwutiwes U, Malathum K, Sungkanuparph S. Cerebrospinal fluid cytology in patients with
Cryptococcal meningoradiculitis: an atypical cancer: minimizing false-negative results. Cancer
presentation after initiation of antiretroviral 1998;82(4):733-739. doi:10.1002/(sici)1097-
therapy. J Med Assoc Thai 2007;90 Suppl 2: 0142(19980215)82:4<733::aid-cncr17>3.0.co;2-z
85-88.
80 Bromberg JE, Breems DA, Kraan J, et al. CSF flow
66 Lanska MJ, Lanska DJ, Schmidley JW. Syphilitic cytometry greatly improves diagnostic accuracy
polyradiculopathy in an HIV-positive man. in CNS hematologic malignancies. Neurology
Neurology 1988;38(8):1297-1301. doi:10.1212/ 2007;68(20):1674-1679. doi:10.1212/01.
wnl.38.8.1297 wnl.0000261909.28915.83
67 Carod Artal FJ, Vargas AP, Horan TA, et al. 81 Hoyle JC, Jablonski C, Newton HB.
Schistosoma mansoni myelopathy: clinical and Neurosarcoidosis: clinical review of a disorder
pathologic findings. Neurology 2004;63(2): with challenging inpatient presentations and
388-391. doi:10.1212/01.wnl.0000130190.67613.be diagnostic considerations. Neurohospitalist 2014;
4(2):94-101. doi:10.1177/1941874413519447
68 Ganesan S, Acharya S, Kalra KL, Chahal R.
Intradural neurocysticercosis of lumbar spine: a 82 Verma KK, Forman AD, Fuller GN, et al. Cauda
case report. Global Spine J 2015;5(4):e1-e4. equina syndrome as the isolated presentation of
doi:10.1055/s-0034-1394125 sarcoidosis. J Neurol 2000;247(7):573-574.
doi:10.1007/s004150070163
69 Majid A, Galetta SL, Sweeney CJ, et al.
Epstein-Barr virus myeloradiculitis and 83 Burns TM, Dyck PJ, Aksamit AJ, Dyck PJ. The
encephalomyeloradiculitis. Brain 2002;125(pt 1): natural history and long-term outcome of 57 limb
159-165. doi:10.1093/brain/awf010 sarcoidosis neuropathy cases. J Neurol Sci 2006;
244(1-2):77-87. doi:10.1016/j.jns.2006.01.014
70 Hisatsugu K, Shigeru H, Makoto M, et al. A case
report of nocardiosis at the cauda equina. 84 Molyneux PD, Barker R, Thomas PK, et al. Non-
J Orthop Sci 2015;20(2):434-438. doi:10.1007/ systemic vasculitic neuropathy presenting with a
s00776-013-0460-8 painful polyradiculopathy: a case report. J Neurol
2000;247(8):645-646. doi:10.1007/s004150070136
71 Hu T, Wu J, Zheng C, Wu D. Brucellar
spondylodiscitis with rapidly progressive spinal 85 Tang C, Moser FG, Reveille J, et al. Cauda equina
epidural abscess showing cauda equina syndrome in ankylosing spondylitis: challenges in
syndrome. Spinal Cord Ser Cases 2016;2:15030. diagnosis, management, and pathogenesis.
doi:10.1038/scsandc.2015.30 J Rheumatol 2019;46(12):1582-1588. doi:10.3899/
jrheum.181259
72 Pfefferkorn T, Feddersen B,
Schulte-Altedorneburg G, et al. Tick-borne 86 Terrettaz M, Verholen F, Passweg J, et al.
encephalitis with polyradiculitis documented by Steroid-responsive cauda equina syndrome
MRI. Neurology 2007;68(15):1232-1233. associated with GVHD after allogeneic
doi:10.1212/01.wnl.0000259065.58968.10 hematopoietic stem cell transplantation. Bone
Marrow Transplant 2008;41(3):315-316.
73 Toledano M. Infectious myelopathies.
doi:10.1038/sj.bmt.1705915
Continuum (Minneap Minn) 2021;27(1, Spinal Cord
Disorders):93-120. 87 Amatya B, Khan F, Whishaw M, Pallant JF.
Guillain-Barré syndrome: prevalence and
74 Bennett SJ, Katzman GL, Roos RP, et al.
long-term factors impacting bladder function in
Neoplastic cauda equina syndrome: a
an Australian community cohort. J Clin Neurol
neuroimaging-based review. Pract Neurol 2016;
2013;9(3):144-150. doi:10.3988/jcn.2013.9.3.144
16(1):35-41. doi:10.1136/practneurol-2015-001236
88 Ishii K, Tamaoka A, Fujita Y, Shoji S. Bladder and
75 Amato ARJ, editor. Neuromuscular disorders. 2nd
bowel dysfunction in chronic inflammatory
ed. New York: McGraw-Hill Education, 2016.
demyelinating polyradiculoneuropathy. Eur J
76 Chen X, Xu G, Bi Q, et al. Cauda equina syndrome Intern Med 2005;16(3):211-213. doi:10.1016/j.
as first manifestation of von Hippel-Lindau ejim.2004.10.021
disease. World Neurosurg 2019;125:316-319.
89 Yuen EC, Layzer RB, Weitz SR, Olney RK.
doi:10.1016/j.wneu.2019.01.269
Neurologic complications of lumbar epidural
77 Walton A, Mecklosky J, Carr C, et al. Cauda equina anesthesia and analgesia. Neurology 1995;45(10):
syndrome secondary to diffuse infiltration of the 1795-1801. doi:10.1212/wnl.45.10.1795
cauda equina by acute myeloid leukemia: case
90 Shields LBE, Iyer VG, Zhang YP, Shields CB. Acute
report and literature review. World Neurosurg
cauda equina syndrome following orthopedic
2019;134:439-442. doi:10.1016/j.wneu.2019.11.068
procedures as a result of epidural anesthesia.
Surg Neurol Int 2018;9:81. doi:10.4103/
sni.sni_492_17
CONTINUUMJOURNAL.COM 223
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DISORDERS OF THE CAUDA EQUINA
91 Bourne IH. Lumbo-sacral adhesive arachnoiditis: 99 Das D, Andi AC, van der Walt JD, Houghton R. MRI
a review. J R Soc Med 1990;83(4):262-265. appearances of extramedullary haematopoiesis
presenting with cauda equina syndrome in sickle
92 Khan MU, Devlin JAJ, Fraser A. Adhesive
cell disease. Clin Radiol 2011;66(12):1219-1222.
arachnoiditis in mixed connective tissue disease:
doi:10.1016/j.crad.2011.07.043
a rare neurological manifestation. BMJ Case Rep
2016;2016:bcr2016217418. doi:10.1136/ 100 Kaur J, Singh P. Pudendal nerve entrapment
bcr-2016-217418 syndrome. In: StatPearls. Treasure Island,
FL: StatPearls Publishing StatPearls Publishing
93 Bowen J, Gregory R, Squier M, Donaghy M. The
LLC, 2019.
post-irradiation lower motor neuron syndrome
neuronopathy or radiculopathy? Brain 1996; 101 Silbert PL, Dunne JW, Edis RH, Stewart-Wynne
119(pt 5):1429-1439. doi:10.1093/brain/119.5.1429 EG. Bicycling induced pudendal nerve pressure
neuropathy. Clin Exp Neurol 1991;28:191-196.
94 Feistner H, Weissenborn K, Münte TF, et al.
Post-irradiation lesions of the caudal roots. Acta 102 Insola A, Granata G, Padua L. Alcock canal
Neurol Scand 1989;80(4):277-281. doi:10.1111/ syndrome due to obturator internus muscle
j.1600-0404.1989.tb03878.x fibrosis. Muscle Nerve 2010;42(3):431-432.
doi:10.1002/mus.21735
95 Li P, Qiu D, Shi H, et al. Isolated decompression
for transverse sacral fractures with cauda equina 103 Andersen KV, Bovim G. Impotence and nerve
syndrome. Med Sci Monit 2019;25:3583-3590. entrapment in long distance amateur cyclists.
doi:10.12659/MSM.916483 Acta Neurol Scand 1997;95(4):233-240. doi:
10.1111/j.1600-0404.1997.tb00104.x
96 Thongtrangan I, Le H, Park J, Kim DH. Cauda
equina syndrome in patients with low lumbar 104 Wadhwa V, Hamid AS, Kumar Y, et al. Pudendal
fractures. Neurosurg Focus 2004;16(6):e6. nerve and branch neuropathy: magnetic
resonance neurography evaluation. Acta Radiol
97 Kempen DHR, Delawi D, Altena MC, et al.
2017;58(6):726-733. doi:10.1177/0284185116668213
Neurological outcome after traumatic transverse
sacral fractures: a systematic review of 521 105 Hough DM, Wittenberg KH, Pawlina W, et al.
patients reported in the literature. JBJS Rev 2018; Chronic perineal pain caused by pudendal nerve
6(6):e1. doi:10.2106/JBJS.RVW.17.00115 entrapment: anatomy and CT-guided perineural
injection technique. AJR Am J Roentgenol 2003;
98 Soman S, Tharadara GD, Chhatrala N, Jain S. A
181(2):561-567. doi:10.2214/ajr.181.2.1810561
case report of extramedullary haematopoeisis in
lumbosacral region presenting as cauda equina 106 Hruby S, Dellon L, Ebmer J, et al. Sensory
syndrome. Int J Spine Surg 2016;10:25. recovery after decompression of the distal
doi:10.14444/3025 pudendal nerve: anatomical review and
quantitative neurosensory data of a prospective
clinical study. Microsurgery 2009;29(4):270-274.
doi:10.1002/micr.20615
224 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Hereditary Myelopathies REVIEW ARTICLE
By John K. Fink, MD C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo/R1NuKT7SYsuBdzpo0ePV on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This article guides clinicians in the clinical recognition and
differential diagnosis of hereditary myelopathies.
RECENT FINDINGS: Rather than a disease, a disease process, or relating to
specific cellular vulnerability, the term hereditary myelopathy refers to
diverse inherited disorders in which major aspects of the clinical syndrome
reflect disturbance of elements within the spinal cord (specifically, the
dorsal columns and dorsal root ganglia, corticospinal tracts, and anterior
horn cells). It is important to note that the clinical features of almost all
hereditary myelopathies reflect not only disturbance of elements within
the spinal cord but also disturbance of extraspinal structures (particularly,
but not limited to, peripheral nerves and the cerebellum) and that these
extraspinal clinical features can be very helpful in recognizing specific
myelopathy syndromes. The value of classifying disorders as inherited
myelopathies lies primarily in facilitating their clinical recognition and
differential diagnosis. It is useful to recognize that many hereditary
myelopathies conform to one of four clinical paradigms: (1) spinocerebellar
ataxia, (2) motor neuron disorder, (3) leukodystrophy, or (4) distal
motor-sensory axonopathy predominantly affecting the central nervous
system. Although they are myelopathies, spinal dysraphisms such as spina CITE AS:
CONTINUUM (MINNEAP MINN)
bifida and myelomeningocele are not included in this context because they 2020;27(1, SPINAL CORD DISORDERS):
are not usually due to single-gene mutation and have low hereditability. 185–204.
SUMMARY: This article illustrates clinical paradigms of hereditary Address correspondence to
Dr John K. Fink, Michigan House,
myelopathy with clinical examples emphasizing the spectrum, clinical 2301 Commonwealth Blvd,
recognition, and differential diagnosis of hereditary myelopathies. Rm 1029, Ann Arbor, MI 48105,
jkfink@umich.edu.
RELATIONSHIP DISCLOSURE:
INTRODUCTION Dr Fink has served as a medical
H
advisor for the Spastic
ereditary myelopathies are diverse genetic disorders in which the Paraplegia Foundation and as a
major clinical features are due to disturbance of elements that occur consultant for Cure AP-4, Inc.
entirely within, emanate from, or traverse the spinal cord. Although Dr Fink receives research/grant
support from the Spastic
the word hereditary implies genetic causation as the disease Paraplegia Foundation and
mechanism, the term myelopathy is strictly a clinical syndromic patent royalties and has
designation describing particular signs and symptoms localizing to the spinal provided expert medicolegal
consultation.
cord and therefore does not imply common neuropathologic processes or
radiographic findings. As with most neurologic syndromes, correlation between UNLABELED USE OF
PRODUCTS/INVESTIGATIONAL
the distribution of neuropathology, radiographic findings, and nature of the USE DISCLOSURE:
clinical disorder is imperfect. For example, some forms of “pure” cerebellar Dr Fink reports no disclosure.
ataxia have postmortem evidence of more widespread neurodegeneration
involving dorsal columns. Conversely, not all inherited disorders that cause © 2021 American Academy
radiographic abnormalities involving the spinal cord in fact manifest as of Neurology.
CONTINUUMJOURNAL.COM 185
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
myelopathies.1 As used in this article, hereditary myelopathy is a clinical term
describing a pattern of signs and symptoms.
The term hereditary myelopathy does not imply that clinical features
exclusively relate to spinal cord disturbance: clinical neurologic involvement in
nearly all hereditary myelopathies reflects disturbance in structures outside the
spinal cord. In fact, the nature of these extraspinal neurologic signs is very
helpful in classifying and diagnosing hereditary myelopathies.
HEREDITARY MYELOPATHY CLINICAL PARADIGMS
Myelopathies are recognized by variable combinations of upper motor
neuron–pattern functional motor disturbance, impaired vibration or
proprioception, and lower motor neuron–pattern motor impairment that are not
attributable (by the remainder of neurologic symptoms and examination
findings) to another localization (ie, brain or peripheral nerve). The magnitude
of each of these elements is highly variable between and within different types of
inherited myelopathy. For example, in primary lateral sclerosis (PLS), upper
motor neuron–pattern motor impairment is severe and occurs in the absence of
significant dorsal column or lower motor neuron impairment. In the spinal
muscular atrophies, anterior horn cell degeneration causing lower motor
neuron–pattern motor impairment occurs in the absence of upper motor neuron
or dorsal column disturbance.
Variable presence and degree of these elements (upper motor neuron, lower
motor neuron, and dorsal column [or dorsal root ganglia] disturbance) cause
most inherited myelopathies to conform to one of four syndromes:
spinocerebellar degeneration, motor neuron disorder, leukodystrophy, and
central nervous system (CNS)–predominant distal motor-sensory axonopathy
(TABLE 8-12-19).
Spinocerebellar Degeneration
The prefix spino- of spinocerebellar degeneration indicates involvement of one or
more of the following: corticospinal tracts in the spinal cord, dorsal columns (or
dorsal root ganglia), or anterior horn cells. As clinical syndromes, spinocerebellar
disorders are contrasted with much less common “isolated” or “pure” cerebellar
ataxia syndromes (eg, spinocerebellar ataxia type 15 [SCA15, Mendelian
Inheritance in Man (MIM) 606658] and SCA41 [MIM 616410])20 and
distinguished from clinical olivopontocerebellar disorders that involve the
cerebellum and other brainstem structures (eg, multiple system atrophy,
cerebellar type) and disorders involving the cerebellum and other areas of the
nervous system that do not have clinical manifestations of spinal cord
involvement (eg, Niemann-Pick disease type C). Classifications of spastic ataxias
(in which ataxia is prominent)1 and complicated forms of hereditary spastic
paraplegia (HSP) associated with cerebellar involvement (in which spastic
paraparesis is prominent) overlap.15,16
Inherited spinocerebellar degenerations (eg, Friedreich ataxia, SCA3 [also
known as Machado-Joseph disease] [CASE 8-1], Bassen-Kornzweig syndrome,
and vitamin E deficiency [occasionally familial]) are recognized by a
combination of progressive cerebellar ataxia, peripheral neuropathy, dorsal
column impairment, and variable corticospinal tract involvement.
It is important to recognize that both between individuals who share the same
disorder and between individuals with genetically unrelated types of
186 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
spinocerebellar degeneration, these diagnostic elements (cerebellar ataxia, KEY POINTS
peripheral neuropathy, dorsal column impairment, and signs of upper motor
● In addition to symptoms
neuron disturbance) exist in variable proportions, that some of the diagnostic arising from disturbance
elements may be absent entirely, and that diagnostic elements may appear within the spinal cord,
asynchronously as the disorder evolves. neurologic involvement in
Friedreich ataxia is often associated with hypertrophic cardiomyopathy nearly all hereditary
myelopathies includes
(present in the patient in CASE 8-2 but absent in the patient in CASE 8-3). The
structures outside the spinal
significantly different, yet overlapping, neurologic and systemic involvement in cord.
the two patients presented in these cases illustrates the important clinical
variation in Friedreich ataxia. Each patient had evidence of marked impairment ● Many hereditary
of the dorsal columns, an important feature of Friedreich ataxia. These patients myelopathic syndromes
can be recognized as one of
differed, however, in the occurrence of cardiomyopathy, generalized areflexia, four clinical paradigms:
and prominent cerebellar deficits (present in the patient in CASE 8-2 but not in (1) spinocerebellar ataxia,
the patient in CASE 8-3) and the occurrence of corticospinal tract impairment (2) motor neuron disorder,
(hyperreflexia, in contrast to areflexia) in the patient in CASE 8-3 but not in the (3) leukodystrophy, or
(4) central nervous system–
patient in CASE 8-2. predominant distal motor-
Recognition that upper motor neuron signs ranging from simply extensor sensory axonopathy.
plantar responses to progressive lower extremity spasticity are common in
Friedreich ataxia represents an evolution of our understanding of this disorder. ● Spinocerebellar
degenerations (eg,
Prior to discovery of the causative gene mutation, Friedreich ataxia was
Friedreich ataxia,
diagnosed clinically as an autosomal recessive disorder (ie, ascertained either in spinocerebellar ataxia
sibships or as a single affected individual in a family without similarly affected type 3, Bassen-Kornzweig
parents or children) marked by ataxia (both cerebellar ataxia and sensory ataxia) syndrome, and vitamin E
deficiency) are recognized
and areflexia (owing to peripheral neuropathy and dorsal root ganglia
by a combination of
involvement). Following discovery of the FXN gene, mutation-based diagnosis progressive cerebellar
led to recognition that many individuals not only had preserved reflexes, but ataxia, often accompanied
some had lower extremity hyperreflexia and spasticity. Indeed, some individuals by peripheral neuropathy;
with Friedreich ataxia present with progressive spastic gait instead of progressive dorsal column (or dorsal
root ganglia) impairment
ataxia. Typically, severe dorsal column (and dorsal root ganglia) involvement in (which may cause sensory
Friedreich ataxia contrasts with the typically mild distal vibration impairment ataxia); and variable
that usually accompanies uncomplicated HSP. corticospinal tract
FXN encodes a mitochondrial protein. The vast majority of patients with involvement.
Friedreich ataxia have expanded trinucleotide repeats (GAA) on both FXN ● Spinocerebellar ataxia
alleles (CASE 8-2). The patient described in CASE 8-3 is not homozygous for this type 3 is caused by a
trinucleotide repeat and instead has compound heterozygosity with an expanded trinucleotide repeat (CAG)
GAA repeat on one FXN allele and a point mutation on the other allele. Point expansion that, like other
polyglutamine expansions,
mutations (rather than GAA expansion) are responsible for only 2% of patients
is thought to be pathogenic
with Friedreich ataxia. The frataxin trinucleotide repeat is GAA instead of the through protein misfolding.
more common polyglutamine expansion (CAG) repeat responsible for
Huntington chorea and many other spinocerebellar ataxias. Furthermore, the ● The vast majority of
frataxin GAA trinucleotide repeat occurs in an intron (frataxin intron 1) and does patients with Friedreich
ataxia are homozygous for
not alter the frataxin coding sequence. Nonetheless, this intronic mutation leads expanded trinucleotide
to reduced frataxin messenger RNA (possibly through locally increased DNA repeat in the FXN gene,
methylation leading to reduced transcription),24 iron accumulation in which encodes a
mitochondria, and an apparent increased vulnerability to oxidative stress. mitochondrial protein.
Rarely, individuals will have
an expanded trinucleotide
Motor Neuron Disorders repeat in one FXN allele and
Motor neuron disorders involve degeneration of the corticospinal tracts or a point mutation in the other
anterior horn cells, or both.2,4,8 Cortical motor neurons may also be involved, FXN allele.
although generally to a lesser extent. Various motor neuron disorder syndromes
CONTINUUMJOURNAL.COM 187
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
TABLE 8-1 Syndromic Classification of Hereditary Myelopathiesa
Major syndrome Representative examples Diagnostic testing
Spinocerebellar ataxias SCA 1 through 48 Genetic testing for specific SCA gene
(SCAs)3 mutation; neuroimaging to demonstrate
cerebellar atrophy
Machado-Joseph disease (SCA3) Genetic testing for specific SCA gene
mutation; neuroimaging to demonstrate
cerebellar atrophy
Friedreich ataxia FXN gene analysis
Familial vitamin E deficiency Serum vitamin E
Abetalipoproteinemia (Bassen-Kornzweig Lipoprotein electrophoresis
syndrome)
Autosomal recessive spastic ataxia of Genetic testing
Charlevoix-Saguenay (ARSACS)
Motor neuron disorders4-8 Spinal muscular atrophy Survival motor neuron (SMN1, SMN2) gene
analysis
Familial amyotrophic lateral sclerosis C9orf72, SOD1, and other gene analysis
Primary lateral sclerosis (rarely familial) ALSIN gene analysis (for juvenile familial
primary lateral sclerosis); FIG4, C9orf72,
SPG7 analysis
Hereditary spastic paraplegia (HSP) HSP gene analysis
Spinal bulbar muscular atrophy (Kennedy Androgen receptor gene mutation (CAG
disease) repeats)
Partial hexosaminidase deficiency Leukocyte hexosaminidase assay
Leukodystrophies9-11 Subacute combined degeneration (rarely Serum vitamin B12, methylmalonic acid
familial)
5-Methyltetrahydrofolate reductase deficiency Plasma homocysteine, methionine, vitamin
(MTHFR)12 B12, methylmalonic acid, folate; urine
homocysteine
Cobalamin C deficiency (MMACHC gene Plasma methylmalonic acid, homocysteine
mutation)13
Multiple sclerosis (occasionally familial) MRI of brain and spinal cord, CSF analysis,
clinical course
Adrenoleukodystrophy, Serum very long chain fatty acid analysis
adrenomyeloneuropathy
Krabbe disease Leukocyte β-galactosidase assay
Metachromatic leukodystrophy Leukocyte arylsulfatase assay
Pelizaeus-Merzbacher disease/SPG2 HSP due to Proteolipid protein gene analysis
PLP1 gene mutation
Cerebrotendinous xanthomatosis Serum cholestanol
Alexander disease14 MRI, GFAP gene analysis
CONTINUED ON PAGE 189
188 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
CONTINUED FROM PAGE 188
Major syndrome Representative examples Diagnostic testing
Central nervous system- Hereditary spastic paraplegia HSP gene analysis
predominant, distal motor-
sensory axonopathies15,16
Other Mitochondrial myelopathy17 Magnetic resonance spectroscopy (brain),
muscle biopsy for ragged red fibers and
histochemical evidence of oxidative
phosphorylation deficit; mitochondrial
gene analysis
Leukoencephalopathy with brainstem and spinal DARS2 gene analysis, spinal MRI
cord involvement and lactate elevation (DARS2
mutation) (FIGURE 8-1A)18
Autosomal dominant leukodystrophy (multiple Brain and spinal cord MRI, LMNB1 gene
sclerosis mimic)19 analysis (including copy number analysis);
LMNB1 quantification in white blood cells
Adult polyglucosan body disease due to GBE1 Brain and spinal cord MRI, nerve
gene mutation conduction studies and EMG, GBE1 gene
analysis
Variant Alzheimer disease with spastic PSEN1 gene analysis
paraplegia due to PSEN1 mutation
Hyperzincemia Serum zinc
Neurofibromatosis type 2 MRI scan
Hereditary exostosis with spinal cord CT and MRI scans
compression
Hereditary hemorrhagic telangiectasia MRI scan
Von Hippel-Lindau (hereditary hemangiomata) MRI scan and VHL gene analysis
Tropical spastic paraplegia (due to human T-cell HTLV-1 antibody testing
lymphotropic virus type 1 [HTLV-1] infection; may
occur in familial clusters)
Arginase deficiency Increased plasma arginine, reduced red
blood cell arginase
Biotinidase deficiency Reduced serum biotinidase
Syringomyelia (rarely familial) MRI scan
Sjögren-Larsson syndrome Clinical features of congenital ichthyosis,
mental deficiency, and spastic diplegia or
tetraplegia (typically accompanied by
additional features) and demonstrating
enzyme (fatty aldehyde dehydrogenase)
defect in cultured fibroblasts
CSF = cerebrospinal fluid; CT = computed tomography; EMG = electromyography; MRI = magnetic resonance imaging.
a
Updated from Fink JK, Continuum (Minneap Minn).2 © 2008 American Academy of Neurology.
CONTINUUMJOURNAL.COM 189
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
differ in the relative combination of upper motor neuron versus lower motor
neuron involvement and the variable occurrence of additional neurologic
disturbance. In PLS, for example, progressive spastic weakness, usually beginning
in the legs and later involving the arms, speech, and swallowing, reflects
corticospinal and corticobulbar tract involvement and, to a lesser extent, loss of
cortical motor neurons (CASE 8-4). In PLS, in contrast to amyotrophic lateral
sclerosis (ALS), there is either no evidence of lower motor neuron involvement
or, at most, minimal evidence on EMG of chronic denervation late in the disease.
Conversely, spinal muscular atrophy is characterized by muscular weakness and
atrophy due to anterior horn cell degeneration with relative preservation of
corticospinal tracts.
CASE 8-1 A 30-year-old woman presented for an initial neurologic evaluation for
difficulty with balance and handwriting. She first noted the insidious
onset of a very slowly progressive balance disturbance at approximately
age 26, followed several years later by mildly impaired handwriting.
Although she was fully able to ascend and descend stairs and walk long
distances independently, neurologic examination at age 30 showed
slightly wide-based gait and impaired ability to walk in tandem. Ocular
dysmetria and saccadic intrusions into pursuit eye movements were also
noted. The remainder of neurologic examination, including finger-to-
nose, heel-to-shin, sensory, and reflex testing, was normal.
Serial evaluations were performed over the next 20 years. During this
time, her balance impairment slowly worsened, her speech became
increasingly dysarthric, and she gradually lost the ability to stand and
walk (requiring a walker by age 48 and a wheelchair in her fifties). In
addition, progressive dystonia, axial rigidity, impaired distal sensation,
and generalized hyperreflexia gradually emerged.
By age 47, she had begun to experience involuntary movements of her
face, neck, and upper extremities. Examination at this time showed
prominent axial rigidity, particularly affecting neck movements; dystonia
affecting the neck, face, and bilateral upper extremities; and cogwheel
rigidity in her upper extremities. In addition to ataxic dysarthria and ataxia
affecting upper and lower extremities, she had grade 3 hyperreflexia
throughout except at the ankles, which were hyporeflexic, and
decreased sensation to pinprick and vibration in a stocking distribution
below the knees. She was able to stand with great difficulty and was
able to take a few steps but had marked balance impairment and
tendency to fall.
Neurologic examination at age 53 showed facial bradykinesia,
generally reduced movements of the extremities, marked ataxic
dysarthria, marked saccadic intrusions into smooth pursuit, very slow
ocular saccades, and generalized hyperreflexia (grade 3) except
absent ankle deep tendon reflexes. She required significant assistance
to stand, had a wide-based stance, and required maximum assistance
to take a couple of steps.
190 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Disorders collectively known as the amyotrophic lateral scleroses typically
involve degeneration of both anterior horn cells and corticospinal tracts and, to a
lesser degree, loss of cortical motor neurons. Although motor neuron,
corticospinal tract, and corticobulbar tract degeneration are the major features
and primary cause of death in ALS, neuropathology is often not limited to the
motor system. Many forms of ALS (eg, C9orf72 expansion-related ALS) also
involve other brain areas (particularly the frontal lobes) and manifest clinically
as frontal lobe dementia.
Approximately 10% of ALS is familial, in which affected individuals have
similarly affected first-degree relatives. The majority of familial ALS is dominantly
inherited, often due to SOD1 mutation or pathogenic expansion in the C9orf72
Family history was notable for similar symptoms in the patient’s
brother and mother, who also had progressive ataxia and dysarthria.
The brother had died at age 40 and the mother died at age 55. The
patient’s maternal aunt and several cousins were also similarly
affected. Postmortem examination of the patient’s mother had
showed degenerative changes in cerebellum and spinal cord.
Genetic testing revealed pathologic CAG repeat expansion ([CAG]75)
in ATXN3, and the patient was diagnosed with spinocerebellar ataxia
type 3 (SCA3).
Localization indicated deficits affecting the cerebellum midline (ocular COMMENT
dysmetria, saccadic intrusions, ataxic dysarthria) and cerebellar
hemispheres (upper extremity dysmetria), peripheral nerves (stocking
gradient to pinprick and vibration below the knees, absent ankle deep
tendon reflexes), corticospinal tracts (generalized hyperreflexia except at
the ankles), and extrapyramidal system (dystonia in the neck, face,
extremities, axial rigidity).
SCA3 is caused by a trinucleotide repeat (CAG) expansion that, like other
polyglutamine expansions, is thought to be pathogenic through protein
misfolding.21 SCA3 phenotypes vary from spastic paraparesis (which
dominated the first decade of this patient’s symptoms) to complex
syndromes involving elements of cerebellar ataxia, extrapyramidal
disturbance (eg, nigrostriatal pathway disturbance), and peripheral
neuropathy. Symptoms in SCA3, as in many degenerative neurologic
disorders, often evolve as the disorder progresses and other neurologic
regions become involved. This patient’s neurologic signs for the first
15 years were limited to disturbance of the cerebellum (ataxic speech and
ataxia of upper and lower extremities) and a minor degree of peripheral
neuropathy. These features are shared with many forms of spinocerebellar
ataxia. It was only after approximately 15 years that features that tend to
distinguish SCA3 from other spinocerebellar ataxias (ie, axial rigidity,
dystonia, and mild corticospinal tract impairment [hyperreflexia]) began
to appear.
CONTINUUMJOURNAL.COM 191
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
repeat. More than 50 other genes have been implicated in familial ALS.8 Genetic
factors also contribute to the disease in many individuals with apparently sporadic
ALS (ie, ALS ascertained in individuals who do not have ALS-affected first-degree
relatives). Specifically, among individuals with apparently sporadic ALS, 1% to 3%
have SOD1 mutations and approximately 5% have pathogenic C9orf72 expansions.
Additional genes (eg, TARDBP, FUS, HNRNPA1, SQSTM1, VCP, OPTN, and
PFN1) have also been implicated in apparently sporadic ALS.8
Overlap exists between the classifications of motor neuron disorder and distal
motor-sensory axonopathy affecting the CNS (eg, HSP). The primary differences
are the degree to which anterior horn cells are lost (a major aspect of spinal muscular
CASE 8-2 A 13-year-old girl presented with very slowly worsening gait and balance.
She reported some stumbling and occasionally dropping things. She had
a history of mild clumsiness in childhood that did not rise to the level of
medical concern. A heart murmur had been discovered at age 10.
Echocardiography identified hypertrophic cardiomyopathy.
Examination was notable for pes cavus, mild scoliosis, mild hypophonia
and dysarthria, mild nystagmus, mild weakness of intrinsic hand muscles
and tibialis anterior muscles, mildly ataxic heel-to-shin and finger-to-nose
movements, mild truncal titubation, and markedly impaired vibration
perception (absent below the knees and absent in her hands). Deep
tendon reflexes were absent throughout. Although she was able to
ambulate independently, her gait was mildly ataxic. Romberg sign was
present.
Her gait and balance slowly worsened, and she required the use of a
wheelchair at approximately age 17. Examination at age 21 showed mild
ataxic dysarthria; saccadic intrusions into smooth pursuit; and weakness of
hip flexion, foot dorsiflexion, and wrist extension. She had mild hypotonia
in the legs, generalized areflexia, ataxia in upper and lower extremities,
and pes cavus with hammer toe formation. She could stand with assistance
but was not able to walk even with support. Localization indicated deficits
referable to the cerebellar midline, cerebellar hemispheres, and dorsal
columns serving the upper and lower extremities.
Genetic analysis showed expansions in both FXN alleles (FXN [GAA]766
and [GAA] 533). The normal GAA repeat number is approximately 8 to 30,
with pathologic expansions measuring 170 to 1700 repeats.22 The patient
was diagnosed with Friedreich ataxia.
COMMENT This individual manifests classic symptoms of Friedreich ataxia: adolescent
onset, slowly progressive gait disturbance associated with areflexia, dorsal
column impairment, cerebellar ataxia, scoliosis, pes cavus, and
cardiomyopathy. Following the discovery of the FXN gene, the classic
clinical presentation of Friedreich ataxia was expanded with recognition
that some individuals with pathologic FXN gene mutations had late-onset
symptoms and retained deep tendon reflexes or even hyperreflexia and
spasticity (CASE 8-3).
192 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
A 24-year-old woman began to notice insidiously progressive difficulty CASE 8-3
with walking and balance beginning at approximately 12 years of age.
There was no previous illness and no family history of similar symptoms.
Although able to walk and run, she noted that she had to concentrate
on keeping her balance. Within the next 2 years she began noticing a tingling
sensation in both legs. Classmates began commenting that she walked as if
she were drunk. Gait disturbance continued to worsen slowly.
Her neurologic examination at age 24 revealed normal speech and
normal cranial nerves with the exception of saccadic intrusions into
smooth pursuit. Muscle bulk, tone, and strength were normal in the
upper extremities. In the lower extremities, however, muscle tone was
increased (particularly at the hamstrings and ankles and to a lesser
extent at the quadriceps), and she had marked weakness of tibialis
anterior, moderate weakness of iliopsoas, and mild weakness of
hamstring muscles. She had profound impairment of distal vibratory
sensation (she was able to perceive vibratory sensation applied to her
shins but not to her toes) and moderately impaired distal proprioception.
She had subjectively decreased pinprick sensation in the distal aspects
of the lower extremities. Deep tendon reflexes were 1 to 2+ at the
biceps, triceps, and brachioradialis; 3+ at the knees; and absent at the
ankles. Finger-to-nose testing was normal. Heel-to-shin testing was
minimally abnormal. Plantar responses were extensor bilaterally. Nerve
conduction studies and EMG were consistent with a sensorimotor
polyneuropathy. MRI of the brain was normal.
Localization indicated deficits referable to corticospinal tracts serving COMMENT
bilateral lower extremities (weakness, increased tone, extensor plantar
responses); dorsal columns and/or dorsal roots (marked vibration and
proprioception impairment, which were out of proportion to subtle
diminution in pinprick perception); and peripheral nerves (absent ankle
deep tendon reflexes and stocking distribution of subjectively decreased
pinprick sensation) and subtle midline cerebellar disturbance (saccadic
intrusions into smooth pursuit and mild heel-to-shin abnormality). Note that
the gradient of hyperreflexia (increased in the legs relative to the arms)
suggests length-dependent central axonopathy. Furthermore, reflexes
that are diminished distally (ie, 3+ at knees and absent at ankles), suggests
co-occurrence of length-dependent corticospinal tract and peripheral
nerve deficits in addition to severe dorsal column or dorsal root ganglia
disturbance.
Genetic analysis revealed compound heterozygous FXN mutations, with
one FXN allele with an expanded repeat ([GAA]962) and the other FXN allele
having a missense mutation resulting in amino acid substitution (G130V).The
patient was diagnosed with Friedreich ataxia, the most common form of
autosomal recessive spinocerebellar ataxia.23
Case updated from Fink JK, Continuum (Minneap Minn).2
CONTINUUMJOURNAL.COM 193
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
CASE 8-4 A 64-year-old man began experiencing initially subtle but slowly
worsening gait disturbance. Neurologic examination showed generalized
hyperreflexia (3+) and mild symmetric weakness and spasticity in his legs.
Speech articulation; swallowing ability; and upper extremity strength,
tone, and dexterity were normal. Sensation was normal throughout. Brain
MRI showed areas of T2 signal intensity in periventricular regions
consistent with chronic small vessel ischemia and age-related changes.
Cervical and thoracic spine MRI showed degenerative changes but no
evidence of spinal cord compression or spinal cord signal change.
One year later (approximately 6 years after symptom onset [age 70]),
he began to experience subtle difficulty speaking, slight impairment of
handwriting and hand dexterity, and emotional lability. Neurologic
examination at that time showed mild slowing of finger tapping, the
presence of Hoffman and Trömner signs, generalized hyperreflexia, and
continued weakness and spasticity in the legs. Worsening gait
disturbance required use of a walker.
By age 74 (approximately 10 years after symptom onset), the patient
reported dysphagia, emotional lability (suggestive of pseudobulbar
affect), and worsened ability to use his upper extremities. Examination
demonstrated marked spastic dysarthria and hypophonia, very slow hand
opening and closing, the emergence of spasticity in the upper
extremities, and worsening of spasticity to a marked degree in the legs.
Marked spastic gait required intermittent use of a wheelchair. There was
no family history of similar disorder.
EMG within approximately 1 year of symptom onset and again after
symptoms had progressed for at least 5 years showed only mild
sensory-motor neuropathy without evidence of amyotrophic lateral
sclerosis.
COMMENT Neurologic findings localized to the corticospinal tracts serving all
extremities (the legs initially and most severely) and corticobulbar tracts
serving speech.
In this patient, the absence of generalized white matter disturbance on
neuroimaging argued against a leukodystrophy, and the absence of lower
motor neuron involvement on EMG argued against amyotrophic lateral
sclerosis. Involvement of upper extremities and speech and the absence
of dorsal column involvement argued against a form of hereditary spastic
paraplegia. The onset after age 30, exclusion of other disorders, limitation
of neurologic symptoms to corticobulbar and corticospinal tracts, and
involvement of three body segments fulfill diagnostic criteria for primary
lateral sclerosis.25
194 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
atrophy, an important feature of ALS, and a minimal feature of PLS and which can KEY POINT
occur insidiously and symmetrically in some complicated forms of HSP) and the
● In primary lateral
degree of sensory (eg, dorsal column) involvement (a finding common in sclerosis, there is either no
hereditary spastic paraplegia but absent in ALS). In individuals with both upper and evidence of lower motor
lower motor neuron involvement, the occurrence of additional neurologic neuron involvement, or, at
disturbance such as peripheral neuropathy and cerebellar ataxia, features not most, minimal evidence of
chronic denervation is seen
associated with ALS or PLS, would suggest a complicated form of HSP.
on EMG late in the disease.
For most individuals, PLS is an “apparently sporadic” adult-onset disorder,25 At the other extreme, spinal
being diagnosed in individuals without similarly affected relatives. Rarely, PLS muscular atrophy is
begins in early childhood and occurs in families, where it appears to be an characterized by muscular
weakness and atrophy due
autosomal recessive disorder. Yang and colleagues26 identified mutations in the
to anterior horn cell
ALSIN gene in patients with autosomal recessive juvenile PLS. Depending on the degeneration with
precise location of the ALSIN gene mutation, patients either exhibit a phenotype preservation of
of pure upper motor neuron impairment (PLS phenotype) or also manifest lower corticospinal tracts.
motor neuron disturbance (consistent with a juvenile-onset, autosomal recessive
ALS phenotype).
The vast majority of adults with PLS do not have identified gene mutations.
However, with increasing analysis of large candidate gene panels and
whole-exome sequencing, gene mutations have been identified in approximately
5% of individuals with PLS. Interestingly, although rare, these mutations have
been in genes implicated in HSP (eg, SPG7) and ALS (eg, C9orf72 and FIG4). This
observation indicates that for some individuals, ALS, PLS, and HSP may share
similar underlying molecular processes and represent a clinical spectrum.
Although PLS is often regarded as an exclusively upper motor neuron
disorder, the variable occurrence of cognitive disturbance (usually in the
frontotemporal dementia pattern of deficits that also occurs in ALS)27 and
relatively common occurrence of pseudobulbar affect in PLS indicate
involvement in nonmotor brain areas. Pseudobulbar affect occurs in individuals
with a variety of disorders (eg, multiple sclerosis, stroke, ALS, PLS). Although it
occurs in individuals with upper motor neuron impairment, pseudobulbar affect
is unlikely to be caused by upper motor neuron impairment.
The precise neuroanatomic localization of pseudobulbar affect is uncertain28
and includes the dorsal globus pallidus as well as descending pathways from
frontal lobes to the brainstem, pontine nuclei, and cerebellum (corticopontine
cerebellar pathways). Regarding the localization and frequent occurrence of
pseudobulbar affect in patients with PLS, Floeter and colleagues29 wrote
“[Pseudobulbar affect] is common in PLS. Imaging findings showing disruption
of corticopontocerebellar pathways support the hypothesis that [pseudobulbar
affect] can be viewed as a ‘dysmetria’ of emotional expression resulting from
cerebellar dysmodulation.”
In other words, although pseudobulbar affect is common in individuals whose
neurologic syndrome includes upper motor neuron impairment (eg, ALS and
PLS), the present understanding is that pseudobulbar affect is not due to
disturbance in the upper motor neurons but reflects co-occurrence of
impairment in other brain areas (likely corticopontocerebellar pathways).
Leukodystrophies
Leukodystrophies are disorders in which the primary or major abnormality
involves myelin development (dysmyelination) or myelin degeneration
(demyelination) of central nerves occurring alone or in combination with
CONTINUUMJOURNAL.COM 195
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
demyelinating peripheral neuropathy.9,10 As discussed below, primary myelin
abnormality may cause degeneration of the long axons, manifesting clinically as
the syndrome of HSP (CNS-predominant distal motor sensory axonopathy)
instead of a leukodystrophy syndrome.
Leukodystrophies have extremely variable clinical presentations, including
progressive cognitive disturbance and signs of corticospinal and corticobulbar
tract deficits. Early corticobulbar tract involvement argues against disorders
causing distal motor-sensory axonopathy (ie, types of HSP). Although the
complete constellation of insidiously progressive cognitive impairment, spasticity,
optic neuropathy, and demyelinating peripheral neuropathy is suggestive of
generalized leukodystrophy (affecting both the CNS and peripheral nervous
system), often all elements of this constellation are not present. In particular,
demyelinating peripheral neuropathy, which typically accompanies childhood-onset
leukodystrophies (eg, Krabbe disease and metachromatic leukodystrophy), may
be absent in the rare adolescent- and adult-onset forms of these disorders.30
Whereas it is not uncommon for inherited leukodystrophies to eventually
cause spastic paraparesis or tetraparesis, it is much more common for inherited
leukodystrophies (eg, CADASIL [cerebral autosomal dominant arteriopathy
with subcortical infarcts and leukoencephalopathy], adrenoleukodystrophy,
Krabbe disease, metachromatic leukodystrophy, Pelizaeus-Merzbacher disease,
mitochondrial disorder [eg, DARS2 mutation (FIGURE 8-1)], and Alexander
disease) to manifest initially and predominantly with cerebral symptoms
(ie, cognitive impairment). Notable exceptions occur when the primary myelin
disturbance (eg, due to proteolipid protein [PLP1] mutation) results in
progressive axon degeneration involving corticospinal tracts.31 In these
individuals, primary myelin impairment (ie, leukodystrophy) manifests as a
myelopathy. When cognitive disturbance is minimal or absent, leukodystrophies
may be difficult to distinguish from hereditary CNS distal axonopathy (ie, HSP).
Certainly, demyelinating optic neuropathy and deafness, which are not
uncommon in leukodystrophies but quite atypical of HSP, would aid the
differential diagnosis. Brain and spinal cord MRI (FIGURE 8-1), brainstem and
visual evoked potentials, and nerve conduction studies are valuable in evaluating
individuals suspected of having leukodystrophy.
ADRENOLEUKODYSTROPHY AND ADRENOMYELONEUROPATHY. Childhood-onset
adrenoleukodystrophy and adolescent- and adult-onset adrenomyeloneuropathy
are X-linked disorders in which ABCD1 gene mutation leads to impaired
peroxisomal beta-oxidation and accumulation of very long chain fatty acids
systemically.32,33 Adrenoleukodystrophy/adrenomyeloneuropathy phenotypes
include rapidly progressive childhood, adolescent, and adult cerebral forms
(CASE 8-5); slowly progressive myelopathic forms (characterized by slowly
progressive spastic paraparesis and peripheral neuropathy, often with complete
sparing of the brain); and isolated adrenal insufficiency. The patient in CASE 8-5
had confluent leukodystrophy on brain MRI and conforms to the adult-onset
cerebral form of adrenoleukodystrophy/adrenomyeloneuropathy.
Potentially treatable leukodystrophies include multiple sclerosis,
cerebrotendinous xanthomatosis, vitamin B12 deficiency, folate deficiency,
5-methylenetetrahydrofolate reductase (MTHFR) deficiency,12 Wilson disease
(occasionally causes demyelination), and mitochondrial disorders (less
treatable). For this reason, serum vitamin B12, methylmalonic acid, folate, very
196 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
● Demyelinating peripheral
neuropathy, which may
accompany childhood-
onset leukodystrophies (eg,
Krabbe disease and
metachromatic
leukodystrophy), may be
absent in the rare
adolescent- and adult-onset
forms of these disorders.
● Childhood-onset
adrenoleukodystrophy and
adolescent- and adult-onset
adrenomyeloneuropathy are
X-linked disorders in which
ABCD1 gene mutation leads
to impaired peroxisomal
beta-oxidation and
accumulation of very long
chain fatty acids
systemically.
● Adrenoleukodystrophy/
adrenomyeloneuropathy
phenotypes include rapidly
progressive childhood,
adolescent, and adult
cerebral forms; slowly
progressive myelopathic
forms (characterized by
slowly progressive spastic
FIGURE 8-1 paraparesis and peripheral
MRI examples of hereditary myelopathies. Sagittal (A) and axial (B) T2-weighted images neuropathy, often with
of the cervical spine show spinal cord atrophy accompanied by dorsal T2 hyperintensity complete sparing of the
(A, B, arrows) in a patient with a leukoencephalopathy with brainstem and spinal cord brain); and isolated adrenal
involvement and high lactate associated with the DARS2 gene mutation. Sagittal (C) and insufficiency.
axial (D) T2-weighted images of the cervical spine show moderate cervical cord atrophy
in a young man with X-linked adrenomyeloneuropathy. Sagittal (E) and axial (F)
T2-weighted images of the thoracic spine show diffuse spinal cord atrophy in a patient
with hereditary spastic paraplegia accompanied by a mutation in the SPG7 gene.
Figure courtesy of Eoin Flanagan, MBBCh.
long chain fatty acids, lactate, pyruvate, serum copper, plasma amino acids
(including homocysteine and methionine), urine amino acids, and serum
cholestanol should be checked in all patients with unexplained spastic paraplegia
and those with leukodystrophy.
CNS-Predominant Distal Motor-Sensory Axonopathies
Distal axonopathy predominantly affecting long CNS fibers2,15,16 in the spinal
cord may be entirely motor (eg, PLS) or involve both long motor (corticospinal)
and sensory (dorsal column) fibers (eg, uncomplicated HSP). The term distal
refers to neuropathologic findings that show greater axonal degeneration in the
distal ends of these fibers. Postmortem studies (although limited to relatively few
of the nearly 100 genetic types of HSP) have shown axonal degeneration that is
maximal in corticospinal tracts in distal thoracic segments and only mild
CONTINUUMJOURNAL.COM 197
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
CASE 8-5 A 46-year-old man presented with a 13-year history of progressive gait
disturbance, urinary urgency, dementia, and dysphagia. He first noted
symptoms at age 33, when he noticed difficulty driving because his foot
would “jump” repetitively when pressing the gas and brake pedals. This was
followed by very slowly progressive gait impairment and urinary urgency.
Within the previous year, he had quit working (after age 46) because of
progressive inability to walk and stand and frequent urinary incontinence.
Over the 6 months before presentation, he developed new symptoms of
progressive dementia and dysphagia. These symptoms began at
approximately age 46 and became severe over the next 6 months.
His family history was significant for a brother who died at age 12 and a
maternal cousin (son of his mother’s sister) who died in childhood of a
neurodegenerative disorder.
Neurologic examination at age 46 demonstrated full alertness, markedly
impaired cognition with very slow verbal replies, and difficulty following
simple commands. Cranial nerves, including extraocular movements, were
normal. Muscle strength was preserved. He had mild spasticity in the arms
and moderate to marked spasticity in the legs. Sensory testing was
considered unreliable. Deep tendon reflexes were hyperactive (3+)
throughout his upper and lower extremities. He was able to stand and take
steps (consistent with mild spastic gait) but was quite unsteady and required
a wheelchair.
Brain MRI showed diffuse white matter abnormality, including areas of
contrast enhancement. Laboratory studies demonstrated increased plasma
very long chain fatty acids.
COMMENT In this patient, neurologic deficits involved corticospinal tracts (symmetric,
four-limb spastic weakness with hyperreflexia) and cerebral hemispheres,
particularly frontal lobes (subacutely progressive dementia).
Increased very long chain fatty acids indicate peroxisomal disease.
The 13-year course of insidiously progressive spastic gait is typical of
adrenomyeloneuropathy and is considered the “default pathway” or
typical neurologic presentation of individuals with an ABCD1 mutation. The
subsequent rapidly progressive dementia and dysphagia with MRI
indicating diffuse brain white matter abnormality are consistent with
transition to cerebral adrenoleukodystrophy, which occurs in a small
percentage of individuals with adrenomyeloneuropathy. Areas of contrast
enhancement in brain white matter are consistent with active inflammatory
demyelination, typical of cerebral adrenoleukodystrophy. As they are
X-linked disorders, individuals with adrenoleukodystrophy and
adrenomyeloneuropathy may have no family history of similarly affected
relatives, either because the disorder is transmitted through asymptomatic
or mildly symptomatic mothers or because the condition is due to de novo
ABCD1 gene mutation. In this case, the history of a neurodegenerative
disorder affecting the patient’s brother and maternal cousin was consistent
with transmission through unaffected mothers and therefore supportive of
an X-linked disorder.
198 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
corticospinal tract axonal degeneration in cervical spinal cord segments as well as
axonal degeneration of dorsal column fibers that is maximal at the distal ends (in
the cervicomedullary region) of the longest fibers (affecting fasciculus gracilis
fibers more than shorter fibers [fasciculus cuneatus]). Similar findings are noted
in phenotypically similar adrenomyeloneuropathy (FIGURE 8-1B). Clinically,
length-dependent axonopathy predominantly involving distal ends of
corticospinal tracts may be apparent as an upper-to-lower extremity gradient of
upper motor neuron signs; much greater (or much earlier onset) upper motor
neuron–pattern impairment is seen in the legs compared to the arms.
Distinguishing between leukodystrophies and CNS-predominant
motor-sensory axonopathies at the bedside may be difficult but is important in
formulating a differential diagnosis. Signs of corticospinal tract impairment (eg,
spastic weakness, hyperreflexia, extensor plantar responses, Hoffman and
Trömner signs) are typical of both leukodystrophies and axonopathies. Clinically
distinguishing leukodystrophies from CNS-predominant distal motor-sensory
axonopathies is based on the presence of additional neurologic findings,
particularly cognitive impairment and sensory disturbance. For example,
patients with generalized leukodystrophies (those affecting myelin of both the
CNS and peripheral nervous system) may also have (although not always)
progressive cognitive impairment and may have demyelinating peripheral
neuropathy, which usually manifests as stocking distribution of hypesthesia and
a gradient of deep tendon reflexes, being reduced in the ankles compared to the
A former college football player experienced insidious-onset progressive CASE 8-6
gait impairment beginning in his late twenties. There was no family history
of similar disorder and no parental consanguinity. Neurologic
examination demonstrated normal cranial nerves; normal upper
extremity muscle strength, tone, and dexterity; bilaterally symmetric
lower extremity spasticity (hamstrings, quadriceps, adductors) without
weakness; minimally reduced distal lower extremity vibration sensation
with normal light touch perception; lower extremity hyperreflexia; and a
marked spastic gait. Brain and spinal cord MRI were normal.
Examination showed neurologic deficits referable to corticospinal tracts COMMENT
serving bilateral lower extremities and, to a lesser extent, dorsal column
fibers serving bilateral lower extremities. Genetic testing demonstrated a
potentially pathogenic mutation in SPAST that was absent in his parents.
This suggests that the patient’s adult-onset apparently sporadic spastic
paraplegia was due to a de novo spastin gene mutation causing adult-onset
apparently sporadic uncomplicated spastic paraplegia.
SPAST hereditary spastic paraplegia is an autosomal dominant disorder.
Therefore, despite having no previous family history of spastic paraparesis,
this individual has an approximately 50% risk of transmitting this disorder to
each child. This emphasizes the need to consider genetic causes in
individuals with possible myelopathy even when there is no family history
of similar disorder.
CONTINUUMJOURNAL.COM 199
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
knees. On the other hand, sensory impairment in motor-sensory axonopathies
(eg, uncomplicated forms of HSP) is typically predominantly limited to dorsal
column impairment affecting longer fibers (fasciculus gracilis) and manifests as
mildly impaired vibration perception in the toes with preservation of other
sensory modalities. Note is made, however, that peripheral neuropathy may be a
complicating feature of many forms of HSP.
The HSPs are a group of nearly 100 disorders in which lower extremity spastic
weakness is a major clinical feature.15,16 There are autosomal dominant, autosomal
recessive, X-linked, and maternally inherited (mitochondrial) forms of HSP. When
CASE 8-7 A 13-year-old girl presented for evaluation of gait disturbance, upper
extremity tremor and declining hand dexterity. She had been born at
35 weeks gestation after an induced delivery because of premature
placental aging. Her speech and developmental milestones had been mildly
delayed, and she had mild cognitive impairment that required special
education. She was nonetheless fully ambulatory, social, and able to
perform self-care activities. By the age of 13 she was noted to have a gait
disturbance with incomplete extension of her knees and a tendency to keep
her arms flexed while walking. She also was noted to have upper extremity
tremors and slowed hand dexterity with impaired ability to write.
Initial neurologic examination at age 13 showed upper extremity tremor,
mild dysarthria, and increased tone in the upper and lower extremities, with
preserved strength, generalized hyperreflexia, and ankle clonus. Sensory
and cerebellar testing were normal. Her balance was impaired, and her gait
was slow, narrow-based, and associated with dystonic arm postures.
Slowly, over many years, her cognition, speech, swallowing, gait, and
functional use of the upper extremities progressively declined, ultimately
causing profound disability. Examination at age 22 showed marked cognitive
impairment, marked hypophonia, very slow arm movements, coarse tremor
in the hands, mild spasticity in the arms, and marked spasticity in the legs.
She had marked weakness in the legs and was unable to lift her legs against
gravity or bend her knees. She had generalized hyperreflexia, including a
hyperactive jaw jerk, and was nonambulatory. EMG and nerve conduction
studies showed only left median neuropathy. Brain MRI at age 23 showed a
thin corpus callosum (FIGURE 8-2A) and focal T2 signal hyperintensity anterior
to the anterior horns of the lateral ventricles consistent with the ears of the
lynx sign (FIGURE 8-2B).34 At age 31, she was nearly aphonic and was only able
to very slowly move her right arm, turn her head, and slowly partially open
and close her hands. She had dystonia in her hands and marked spasticity in
upper and lower extremities. Progressive dysphagia and weight loss
necessitated gastrostomy feeding. Repeat EMG and nerve conduction
studies showed length-dependent motor-predominant neuropathy.
The diagnosis of SPG11 autosomal recessive hereditary spastic paraplegia
was made. Genetic testing at age 28 revealed compound heterozygous
SPG11/spatacsin mutations each causing protein truncation (c.6299 T>A,
pLeu2100Stop and c.6598 A>T, p.Lys2200Stop).
200 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HSP symptoms begin in early childhood, gait disturbance may be nonprogressive
and resemble spastic diplegic cerebral palsy. HSP symptoms that begin after early
childhood typically progress slowly over a number of years. Neurologic examination
demonstrates signs of upper motor neuron impairment as various degrees of
hyperreflexia, spasticity, and weakness that are exclusively present or markedly
greater in the legs than the arms. For example, in the presence of spasticity,
weakness, and grade 3 to 4 reflexes in the legs, upper extremities are typically
entirely asymptomatic yet show mildly brisk deep tendon reflexes. This is often
accompanied by subtle decrease in vibration perception in the toes.
FIGURE 8-2
Imaging of the patient in CASE 8-7. A, Sagittal T1-weighted MRI shows a thin corpus callosum.
B, Axial fluid-attenuated inversion recovery (FLAIR) MRI shows the ears of the lynx sign.
This patient’s findings indicated neurologic deficits involving corticospinal COMMENT
tracts serving all extremities (with earlier-appearing and more severe deficits
affecting the legs compared to the arms), corticobulbar tracts,
extrapyramidal system (dystonia and tremor), and cerebral hemispheres
(serving cognition). In addition, EMG and nerve conduction studies provided
evidence of motor neuropathy.
SPG11 HSP, the diagnosis in this patient, is among the most common causes
of autosomal recessive HSP.35 Although some individuals have
uncomplicated spastic paraparesis, it is typical for patients with SPG11 HSP to
have complicated phenotypes in which progressive spastic paraplegia is
associated with other deficits, including cognitive impairment, a thin corpus
callosum, extrapyramidal features36 (which may resemble dopa-responsive
dystonia37 and dopa-unresponsive parkinsonism38), upper extremity and
bulbar muscle involvement, and peripheral motor neuropathy.39 Motor
neuron degeneration in SPG11 HSP may mimic ALS.40,41
CONTINUUMJOURNAL.COM 201
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
KEY POINTS HSP’s pattern of CNS-predominant motor and sensory axonopathy
particularly affecting the distal ends of very long CNS fibers (corticospinal
● Clinical distinction of
leukodystrophies from
tracts and dorsal columns, respectively) can be considered analogous to
axonopathies is based on Charcot-Marie-Tooth disease type 2, in which distal motor-sensory axonopathy is
the presence of additional limited to the peripheral nervous system.
neurologic findings, Numerous types of complicated HSP have neurologic involvement in addition
particularly cognitive
to corticospinal tract and dorsal column disturbance. These abnormalities
impairment, optic
neuropathy, deafness, and include, for example, peripheral neuropathy, cerebellar ataxia, cognitive
sensory disturbance. impairment, dementia, and distal muscle wasting.15,16
SPAST mutations are the single most common cause of dominantly inherited
● Sensory impairment in HSP, present in approximately 35% to 45% of such individuals with HSP.15,16
uncomplicated motor-
sensory axonopathies (eg, Individuals with SPAST HSP typically manifest with a slowly progressive
uncomplicated hereditary uncomplicated spastic paraparesis (CASE 8-6).
spastic paraplegia) typically Recognizing HSP is straightforward when the patient has similarly affected
results in mild dorsal column first-degree relatives, neurologic involvement is limited to progressive
impairment affecting longer
fibers and manifests as
corticospinal tract impairment (often accompanied by urinary urgency and
impaired vibration subtle impairment of vibration perception), and other disorders are excluded by
perception in the toes with laboratory testing and neuroimaging (FIGURE 8-1C). Recognizing HSP is more
preservation of other difficult when patients have no family history (which may be the case when HSP
sensory modalities.
is autosomal recessive, X-linked, or due to de novo mutation [CASE 8-6]) and
● ATL1/atlastin gene when diverse neurologic symptoms are (or eventually become) indicative of
mutation is the most more extensive CNS involvement (CASE 8-7).
common cause of
childhood-onset autosomal
GENETIC TESTING
dominant hereditary spastic
paraplegia. ATL1 hereditary Genetic testing is often able to establish a precise diagnosis for patients with
spastic paraplegia usually hereditary myelopathy. Depending on the clinical syndrome (ie, whether
causes nonprogressive cerebellar ataxia, spastic paraparesis, or cognitive impairment is the predominant
infantile-onset spastic gait symptom), the clinician may choose to either analyze a large panel of genes
and resembles spastic
diplegic cerebral palsy. implicated in spinocerebellar ataxias, HSPs, leukodystrophies, or motor neuron
disorders or proceed with whole-exome analysis. Next-generation sequencing
● Central nervous (either of gene panels or whole-exome analysis) may not sensitively detect gene
system–predominant distal copy number variation (deletion or duplication). Chromosome microarray
motor-sensory axonopathy
(eg, uncomplicated
analysis may be useful in this regard.
hereditary spastic In general, genetic testing has the highest likelihood of yielding unambiguous
paraplegia) can be information when a clinical diagnosis is made, and syndrome-specific candidate
considered analogous to genes are analyzed. It is often difficult to interpret the significance of gene
Charcot-Marie-Tooth
variations (such as those identified in whole-genome or whole-exome
disease type 2, in which
axonopathy affects sequencing) that have little or no known association with the specific syndrome.
predominantly the distal It is important to note that identifying a precise genetic cause of the syndrome
ends of long motor and often does not indicate the extent and severity of the individual’s symptoms.
sensory fibers in the
Each of these syndromes is highly variable. Significant variation may be seen
peripheral nervous system.
even between individuals who share exactly the same mutation. For most
● SPAST mutations are the conditions, little is known about genotype-phenotype correlation and the
most common cause of contribution of modifying genes and potentially modifying environmental
autosomal dominant factors. For this reason, a cautious approach to prognosis is advised.
hereditary spastic
paraplegia.
CONCLUSION
The clinical and genetic diversity of hereditary myelopathies limits useful
generalizations. Nonetheless, it is notable that in the patients described in the
202 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
cases in this article (SCA3, autosomal dominant HSP due to SPAST mutation,
autosomal recessive HSP due to SPG11 mutation, cerebral adrenoleukodystrophy,
Friedreich ataxia, and PLS), spastic gait disturbance was an early and prominent
symptom. Identifying associated features (eg, subtle dorsal column signs in HSP;
cognitive impairment in cerebral adrenoleukodystrophy; marked dorsal column
impairment in Friedreich ataxia; upper extremity and bulbar muscle
involvement in PLS; and cognitive, extrapyramidal, and peripheral motor
neuropathy in SPG11 HSP) is essential to clinical recognition of these disorders.
ACKNOWLEDGMENTS
The author would like to thank the Spastic Paraplegia Foundation, the Paul and
Lois Katzman family, and the Susan Parkinson Foundation, without whom his
investigations would not be possible.
REFERENCES
1 Marelli C, Salsano E, Politi LS, Labauge P. Spinal 12 Gales A, Masingue M, Millecamps S, et al.
cord involvement in adult-onset metabolic and Adolescence/adult onset MTHFR deficiency
genetic diseases. J Neurol Neurosurg Psychiatry may manifest as isolated and treatable distinct
2019;90(2):211-218. doi:10.1136/jnnp-2018-318666 neuro-psychiatric syndromes. Orphanet J Rare
Dis 2018;13:29. doi:10.1186/s13023-018-0767-9
2 Fink JK. Hereditary myelopathies. Continuum
(Minneap Minn) 2008;14(3):58-70. doi:10.1212/ 13 Cui J, Wang Y, Zhang H, et al. Isolated subacute
01.CON.0000324124.55065.09 combined degeneration in late-onset cobalamin
C deficiency in children: two case reports and
3 Klockgether T, Mariotti C, Paulson HL.
literature review. Medicine (Baltimore) 2019;
Spinocerebellar ataxia. Nat Rev Dis Primers 2019;
98(39):e17334. doi:10.1097/MD.0000000000017334
5(1):24. doi:10.1038/s41572-019-0074-3
14 Messing A. Alexander disease. Handb Clin Neurol
4 Garg N, Park SB, Vucic S, et al. Differentiating
2018;148:693-700. doi:10.1016/B978-0-444-
lower motor neuron syndromes. J Neurol
64076-5.00044-2
Neurosurg Psychiatry 2017;88(6):474-483.
doi:10.1136/jnnp-2016-313526 15 Fink JK. Upper motor neuron disorders:
hereditary spastic paraplegia and primary lateral
5 Tiryaki E, Horak HA. ALS and other motor neuron
sclerosis. In: Johnston MV, Adams HP, Fatemi A,
diseases. Continuum (Minneap Minn) 2014;
editors. Neurobiology of disease. 2nd ed. Oxford
20(5 Peripheral Nervous System Disorders):
University Press, 2016: 236-240.
1185-1207. doi:10.1212/01.CON.0000455886.
14298.a4 16 Fink JK. The hereditary spastic paraplegias. In:
Rosenberg RN, Pascual JM, editors. Rosenberg's
6 Verschueren A. Motor neuropathies and lower
molecular and genetic basis of neurologic and
motor neuron syndromes. Rev Neurol (Paris) 2017;
psychiatric disease. 6th ed. Academic Press,
173(5):320-325. doi:10.1016/j.neurol.2017.03.018
2020:891-902.
7 Peters OM, Ghasemi M, Brown RH Jr. Emerging
17 Scheper GC, van der Klok T, van Andel RJ, et al.
mechanisms of molecular pathology in ALS. J Clin
Mitochondrial aspartyl-tRNA synthetase
Invest 2015;125(5):1767-1779. doi:10.1172/JCI71601
deficiency causes leukoencephalopathy with
8 Taylor JP, Brown RH Jr, Cleveland DW. Decoding brain stem and spinal cord involvement and
ALS: from genes to mechanism. Nature 2016; lactate elevation. Nat Genet 2007;39(4):534-539.
539(7628):197-206. doi:10.1038/nature20413 doi:10.1038/ng2013
9 Raymond GV. Leukodystrophy: basic and clinical. 18 Isohanni P, Linnankivi T, Buzkova J, et al. DARS2
Adv Neurobiol 2017;15:365-382. doi:10.1007/ mutations in mitochondrial leucoencephalopathy
978-3-319-57193-5_14 and multiple sclerosis. J Med Genet 2010;47(1):
66-70. doi:10.1136/jmg.2009.068221
10 Köhler W, Curiel J, Vanderver A. Adulthood
leukodystrophies. Nat Rev Neurol 2018;14:94-105. 19 Padiath QS, Saigoh K, Schiffmann R, et al. Lamin
doi:10.1038/nrneurol.2017.175 B1 duplications cause autosomal dominant
leukodystrophy. Nat Genet 2006;38(10):1114-1123.
11 Lyon G, Fattal-Valevski A, Kolodny EH.
doi:10.1038/ng1872
Leukodystrophies: clinical and genetic aspects.
Top Magn Reson Imaging 2006;17(4):219-242.
doi:10.1097/RMR.0b013e31804c99d4
CONTINUUMJOURNAL.COM 203
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
HEREDITARY MYELOPATHIES
20 Bird TD. Hereditary ataxia overview. In: Adam 31 Garbern JY, Yool DA, Moore GJ, et al. Patients
MP, Ardinger HH, Pagon RA, et al, editors. lacking the major CNS myelin protein, proteolipid
GeneReviews. University of Washington, Seattle; protein 1, develop length-dependent axonal
1993-2020. Published October 28, 1998. Updated degeneration in the absence of demyelination
July 25, 2019. Accessed December 7, 2020. ncbi. and inflammation. Brain 2002;125(pt 3):551-561.
nlm.nih.gov/books/NBK1138/ doi:10.1093/brain/awf043
21 Paulson H. Machado-Joseph disease/ 32 Moser HW, Mahmood A, Raymond GV. X-linked
spinocerebellar ataxia type 3. Handb Clin Neurol adrenoleukodystrophy. Nat Clin Pract Neurol
2012;103:437-449. doi:10.1016/B978-0-444-51892- 2007;3(3):140-151. doi:10.1038/ncpneuro0421
7.00027-9
33 Engelen M, Kemp S, de Visser M, et al. X-linked
22 Cossée M, Schmitt M, Campuzano V, et al. adrenoleukodystrophy (X-ALD): clinical
Evolution of the Friedreich's ataxia trinucleotide presentation and guidelines for diagnosis,
repeat expansion: founder effect and follow-up and management. Orphanet J Rare Dis
premutations. Proc Natl Acad Sci U S A 1997; 2012;7:51. doi:10.1186/1750-1172-7-51
94(14):7452-7457. doi:10.1073/pnas.94.14.7452
34 Pascual B, de Bot ST, Daniels MR, et al. “Ears of
23 Cook A, Giunti P. Friedreich's ataxia: clinical the lynx” MRI sign is associated with SPG11 and
features, pathogenesis and management. SPG15 hereditary spastic paraplegia. AJNR Am J
Br Med Bull 2017;124(1):19-30. doi:10.1093/bmb/ Neuroradiol 2019;40(1):199-203. doi:10.3174/
ldx034 ajnr.A5935
24 Greene E, Mahishi L, Entezam A, et al. 35 Stevanin G. Spastic paraplegia 11. In: Adam MP,
Repeat-induced epigenetic changes in intron 1 of Ardinger HH, Pagon RA, et al, editors.
the frataxin gene and its consequences in GeneReviews. University of Washington, Seattle;
Friedreich ataxia. Nucleic Acids Res 2007;35(10): 1993-2020. Published March 27, 2008. Updated
3383-3390. doi:10.1093/nar/gkm271 December 19, 2019. Accessed December 7, 2020.
ncbi.nlm.nih.gov/books/NBK1210/
25 Turner MR, Barohn RJ, Corcia P, et al. Primary
lateral sclerosis: consensus diagnostic criteria. 36 Faber I, Martinez ARM, de Rezende TJR, et al.
J Neurol Neurosurg Psychiatry 2020;91(4): SPG11 mutations cause widespread white matter
373-377. doi:10.1136/jnnp-2019-322541 and basal ganglia abnormalities, but restricted
cortical damage. Neuroimage Clin 2018;19:
26 Yang Y, Hentati A, Deng HX, et al. The gene
848-857. doi:10.1016/j.nicl.2018.05.031
encoding alsin, a protein with three
guanine-nucleotide exchange factor domains, is 37 Wijemanne S, Shulman JM, Jimenez-Shahed J,
mutated in a form of recessive amyotrophic et al. SPG11 mutations associated with a complex
lateral sclerosis. Nat Genet 2001;29(2):160-165. phenotype resembling dopa-responsive
doi:10.1038/ng1001-160 dystonia. Mov Disord Clin Pract 2015;2(2):149-154.
doi:10.1002/mdc3.12144
27 de Vries BS, Spreij LA, Rustemeijer LMM, et al. A
neuropsychological and behavioral study of PLS. 38 Faber I, Martinez ARM, Martins CR Jr, et al.
Amyotroph Lateral Scler Frontotemporal SPG11-related parkinsonism: clinical profile,
Degener 2019;20(5-6):376-384. doi:10.1080/ molecular imaging and l-dopa response.
21678421.2019.1620284 Mov Disord 2018;33:1650-1656. doi:10.1002/
mds.27491
28 Lapchak PA. Neuronal dysregulation in
stroke-associated pseudobulbar affect (PBA): 39 Manole A, Chelban V, Haridy NA, et al. Severe
diagnostic scales and current treatment options. axonal neuropathy is a late manifestation of
J Neurol Neurophysiol 2015;6(5):323. doi:10.4172/ SPG11. J Neurol 2016;263(11):2278-2286. doi:
2155-9562.1000323 10.1007/s00415-016-8254-5
29 Floeter MK, Katipally R, Kim MP, et al. Impaired 40 Branchu J, Boutry M, Sourd L, et al. Loss of
corticopontocerebellar tracts underlie spatacsin function alters lysosomal lipid
pseudobulbar affect in motor neuron disorders. clearance leading to upper and lower motor
Neurology 2014;83(7):620-627. doi:10.1212/ neuron degeneration. Neurobiol Dis 2017;102:
WNL.0000000000000693 21-37. doi:10.1016/j.nbd.2017.02.007
30 Lyon G, Hagberg B, Evrard P, et al. 41 Daoud H, Zhou S, Noreau A, et al. Exome
Symptomatology of late onset Krabbe's sequencing reveals SPG11 mutations causing
leukodystrophy: the European experience. juvenile ALS. Neurobiol Aging 2012;33(4):839.
Dev Neurosci 1991;13(4–5):240-244. e5-839.e9. doi:10.1016/j.neurobiolaging.
doi:10.1159/000112167 2011.11.012
204 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Infectious Myelopathies REVIEW ARTICLE
By Michel Toledano, MD C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo65TEub0G9tZtPaMachiqn on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This
article reviews infectious etiologies of spinal cord
dysfunction, emphasizing the importance of recognizing common
clinicoradiographic syndromes and interpreting them in the context of
exposure risk and individual host susceptibilities.
RECENT FINDINGS: Thisarticle discusses the shifting spectrum of neurologic
infectious diseases, the growing population of patients who are
immunocompromised, and the emergence of effective antiretroviral
therapies. In addition, it discusses new molecular and serologic tests that
have the potential to enhance our ability to rapidly and accurately diagnose
infectious diseases of the spine.
SUMMARY: When evaluating patients with suspected infectious
myelopathies, it is imperative to narrow the range of pathogens under
consideration. The geography, seasonality, and clinicoradiographic
presentation and immunocompetence status of the patient define the
range of potential pathogens and should guide testing and initial
management.
INTRODUCTION CITE AS:
P
rompt and thorough investigation of spinal cord dysfunction is CONTINUUM (MINNEAP MINN)
2021;27(1, SPINAL CORD DISORDERS):
important as severe impairment may accrue rapidly without a clear 93–120.
diagnostic and treatment plan. Spinal cord dysfunction of any cause,
whether extrinsic or intrinsic, focal or diffuse, is referred to as Address correspondence to
Dr Michel Toledano, Mayo
myelopathy. Myelitis usually designates inflammation of the spinal cord
Clinic, 200 First St SW,
itself. The corollary terms for root pathology are radiculopathy and radiculitis. Rochester, MN 55905, toledano.
Infections can result in spine pathology through direct invasion of neural michel@mayo.edu.
structures, secondary inflammation, or compression, as with an epidural abscess. RELATIONSHIP DISCLOSURE:
Neuroinvasion can lead to downstream inflammatory changes, but inflammation Dr Toledano reports no
can also result from immune-mediated mechanisms triggered by systemic disclosure.
infection in the absence of direct nervous system involvement by the pathogen. UNLABELED USE OF
When this occurs contemporaneously with acute infection, the term PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
parainfectious is used, whereas the term postinfectious refers to cases in which
Dr Toledano discusses the
neurologic symptoms develop weeks after systemic infection. unlabeled/investigational use of
Once infection has been identified as a probable cause, it is imperative to corticosteroids and IV
immunoglobulin for the
narrow the range of potential pathogens under consideration. Knowing which treatment of infectious
microorganisms are likely and whether the presentation is primarily driven by myelopathies.
direct infection or secondary immune-mediated mechanisms can prevent
unnecessary testing, mitigate the risk of false-positive results, and guide © 2021 American Academy
appropriate empiric therapy. of Neurology.
CONTINUUMJOURNAL.COM 93
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
The traditional way of narrowing the differential diagnosis in neurology relies on
history, examination, and imaging. Certain pathogens cause primarily intramedullary
infection, whereas others are more likely to seed extramedullary sites. Some
pathogens cause isolated myelopathy, but others (such as herpes simplex virus type 2
[HSV-2]) are more likely to affect both the cord and roots, leading to myeloradiculitis.
Some infections preferentially involve anterior horn cells, leading to a syndrome of
acute flaccid myelitis, whereas others affect the cord more diffusely, leading to spastic
paresis and sensory dysfunction below the level of the lesion. Pyogenic bacteria are
more likely to be associated with fever and to seed structures adjacent to the cord,
resulting in compressive myelopathy. Both syphilis and varicella-zoster virus (VZV)
TABLE 4-1 Global Distribution of Select Microorganisms Associated With
Myelopathy and Radiculopathy
Microorganism Location of highest endemicity
Viruses
Human T-cell lymphotropic South America; the Caribbean; Japan; Papua New Guinea; the Melanesian islands; the
virus type 1 (HTLV-1) Middle East; and West, Central, and Southern Africa
Poliovirus Afghanistan and Pakistan
Rabies Lyssavirus Worldwide but most common in Africa, Central and South America, and Asia
Bacteria
Borrelia species Northeast, mid-Atlantic, and northern Midwest of the United States; Europe
Brucella species North Africa, the Mediterranean Basin, Middle East, Indian subcontinent, Mexico
Mycobacterium tuberculosis Central and South America, sub-Saharan and Northern Africa, Indian subcontinent,
Southeast Asia, Micronesia, China, Eastern Europe
Fungi
Blastomyces dermatitidis Areas of the United States and Canada surrounding the Ohio and Mississippi River Valleys
and the Great Lakes
Coccidioides species Southwestern United States, Mexico, and South America
Histoplasma capsulatum Most commonly reported in the United States, particularly areas around the Ohio and
Mississippi River Valleys; also in Central and South America, Africa, Asia, and Australia
Parasites
Angiostrongylus cantonensis Southeast Asia and the Pacific Basin
Echinococcus species South America, the Middle East, Eastern Mediterranean, Western China, and the former
Soviet Union
Gnathostoma spinigerum Southeast Asia
Schistosoma haematobium Sub-Saharan Africa and the Middle East
Schistosoma japonicum China, the Philippines, and Indonesia
Schistosoma mansoni Sub-Saharan Africa, South America, and some of the South Caribbean Islands
Taenia solium South and Central America, sub-Saharan Africa, India, and Southeast Asia
(neurocysticercosis)
94 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
can rarely be associated with spinal cord ischemia. Certain retroviruses result in KEY POINTS
slowly progressive myelopathies, whereas herpesviruses tend to be associated
● Infections can result in
with more rapid progression. Familiarity with these clinicoradiographic spine pathology through
presentations can help narrow the differential, although, admittedly, this direct invasion of neural
approach is limited as individual pathogens can have multiple manifestations. structures or by
Another important tool is microbiology. Exposure is a precondition to immune-mediated
mechanisms triggered by
infection, and certain host factors can predispose individuals to specific
systemic infection in the
microorganisms or increase their risk of developing manifestations of chronic absence of neuroinvasion.
infection. Age, geography (TABLE 4-1), seasonality, and psychosocial factors
define the range of potential pathogens. If a patient is immunocompromised, the ● Although considerable
nature of the immunodeficiency (whether cellular or humoral, for example) also overlap exists, recognizing
common clinicoradiographic
helps narrow the differential (TABLE 4-2) (CASE 4-1). All patients with suspected syndromes is critical when
central nervous system (CNS) infection should be tested for human generating a differential
immunodeficiency virus (HIV), which predisposes patients to opportunistic diagnosis for infectious
infection and can itself cause myelopathy. myelopathies.
The selection of microbiologic diagnostic tests should be guided by the
abovementioned considerations. Ignoring these can result in failure to test for the
offending pathogen. Conversely, overtesting increases the risk of false-positive
results and can result in unnecessary exposure to antimicrobials and delays in
establishing the correct diagnosis. CSF analysis can be useful for differentiating
between viral, bacterial, fungal, and parasitic etiologies (TABLE 4-3). Familiarity
with the role and accuracy of each test for identifying specific pathogens is crucial
for diagnosis and interpretation of results (TABLE 4-4). A variety of assays that
target multiple microorganisms are becoming increasingly available. Some rely on
nested multiplex nucleic acid amplification to simultaneously test for up to 14
pathogens. Others, such as 16s rRNA polymerase chain reaction (PCR) are used to
detect the presence of any bacteria in the sample. Metagenomic next-generation
sequencing of CSF or brain tissue samples can potentially detect the presence of
DNA or RNA sequences of all previously catalogued and sequenced pathogens
(TABLE 4-51). Utility, availability, and cost vary for these tests, but the tests are
likely to become incorporated into diagnostic algorithms in the near future.
INTRAMEDULLARY SPINAL CORD INFECTIONS
Most intramedullary cord infections are associated with some degree of
inflammation; thus, the term myelitis can be broadly applied. Rarely though, as
in the case of HIV-associated vacuolar myelopathy, inflammation appears to play
no pathogenic role. Many infections affect both cord and root, leading to
myeloradiculitis. Some infections preferentially affect the gray matter
(poliomyelitis), whereas others affect primarily the white matter
(leukomyelitis), sometimes even remaining confined to specific columns or
tracts. However, in many cases, the extent of inflammation or limitations in
imaging may render these distinctions obscure. The term transverse myelitis has
evolved to have multiple meanings and often mixes clinical and pathologic
entities, limiting its utility as a clinicoradiographic descriptor. Although rare,
some microorganisms can cause an intramedullary abscess.
Myelitis
Viruses are a common cause of infectious myelitis. Spinal cord injury can be
caused either by direct neural invasion or via immune-mediated parainfectious
or postinfectious mechanisms.
CONTINUUMJOURNAL.COM 95
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
HERPESVIRUSES. The herpesviruses are a family of DNA viruses that are ubiquitous
worldwide and include herpes simplex virus type 1 (HSV-1), HSV-2, VZV, Epstein-Barr
virus (EBV), and cytomegalovirus (CMV). Although they cause nervous system
disease in a minority of patients who are infected, their pervasiveness makes them one
of the more common infectious causes of myelitis and myeloradiculitis (TABLE 4-6).
VARICELLA-ZOSTER VIRUS. VZV causes a diverse spectrum of neurologic
complications. Primary infection causes chickenpox, after which the virus
establishes latent infection in the dorsal root ganglia. When reactivated, the
virus travels along the sensory nerve to the surface, leading to a vesicular rash, or
herpes zoster. Retrograde travel can lead to meningoencephalitis or myelitis,
particularly in immunocompromised hosts. The myelitis can be localized to the
same segment as the rash or can involve the cord more diffusely. Thoracic
involvement is most common.2 Patients usually present over days to weeks with
TABLE 4-2 Microorganisms Associated With Immunodeficiency
Immunodeficiency Microorganism
Cell-mediated dysfunction (eg, human immunodeficiency virus Viral: varicella-zoster virus (VZV) (herpes zoster and
[HIV], DiGeorge syndrome, Hodgkin lymphoma, disseminated infection), cytomegalovirus (CMV), JC virus
glucocorticoids, tacrolimus, methotrexate, mycophenolate
mofetil, cyclophosphamide) Bacterial: Staphylococcus aureus, Mycobacterium
tuberculosis, Nocardia species, Listeria monocytogenes;
coinfection with Treponema pallidum common in patients
with HIV
Fungal: Cryptococcus neoformans, Histoplasma capsulatum,
Blastomyces dermatitidis, Coccidioides species
Parasitic: Toxoplasma gondii (HIV)
Neutropenia (eg, intensive chemotherapy, hematopoietic cell Viral: herpes simplex virus types 1 and 2, VZV (herpes zoster
transplantation, solid organ transplantation) and disseminated infection), CMV, Epstein-Barr virus
Bacterial: Staphylococcus epidermidis, S. aureus,
Streptococcus species, Pseudomonas aeruginosa
Fungal: Aspergillus species, Candida species
Parasitic: T. gondii
Humoral immune dysfunction (eg, primary Viral: Enteroviruses, VZV (herpes zoster)
hypogammaglobulinemias, complement deficiency, multiple
myeloma, Waldenström macroglobulinemia, lymphoma, chronic Bacterial: encapsulated bacteria (Streptococcus
lymphocytic leukemia, B-cell–depleting therapies, splenectomy) pneumoniae, Neisseria meningitides, Haemophilus
influenzae)
Tumor necrosis factor-α inhibitors Viral: VZV (herpes zoster)
Bacterial: Mycobacterium tuberculosis, Nocardia species,
L. monocytogenes
Fungal: H. capsulatum, B. dermatitidis, Coccidioides
species, C. neoformans, Aspergillus species
Barrier disruption (eg, shunts/drains, neurosurgical Bacterial: Cutibacterium acnes, skin/gut-derived bacteria
intervention, lines)
Fungal: Candida species
96 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
progressive asymmetric paraparesis and sensory disturbances. MRI usually KEY POINTS
shows an expansile T2-hyperintense lesion with associated gadolinium
● The sensitivity of CSF
enhancement, which can be longitudinally extensive. Multifocal segmental varicella-zoster virus
lesions can also occur, although are less common. polymerase chain reaction
CSF commonly demonstrates a lymphocytic pleocytosis, and VZV PCR can be starts decreasing steadily
diagnostic, although sensitivity is variable and decreases steadily 1 week from the further away from
symptom onset. A low
symptom onset.3 CSF VZV serology, and in particular a low serum to CSF VZV IgG
serum to CSF IgG ratio
ratio confirming intrathecal production, has considerably higher sensitivity. A demonstrating intrathecal
presumptive diagnosis can be made in patients presenting with myelitis following a production of antibodies is
characteristic dermatomal rash even if PCR is negative. Conversely, VZV myelitis can more sensitive.
occur in the absence of antecedent herpes zoster.2 Additionally, it must be noted
● Varicella-zoster virus
that CSF pleocytosis and even VZV PCR positivity can occur in patients with herpes myelitis can occur in the
zoster without clinical meningoencephalomyelitis.4,5 Treatment is with IV acyclovir absence of a characteristic
and corticosteroids. Postinfectious aquaporin-4-IgG–seropositive neuromyelitis herpes zoster rash.
optica spectrum disorder (NMOSD) myelitis has been reported following herpes
zoster, and this should be considered in the appropriate clinical setting.6
EPSTEIN-BARR VIRUS. EBV establishes latency in lymphocytes and can become
reactivated in the setting of immune compromise. Primary infection in early adulthood
can be asymptomatic or present as mononucleosis, which is characterized by fever,
pharyngitis, fatigue, lymphadenopathy, and splenomegaly. Myelopathy is rare and
usually occurs in the setting of primary infection; it is frequently accompanied by
encephalopathy.7,8 It remains unclear whether the mechanism of injury is direct viral
invasion or an immune-mediated parainfectious process. Cases of acute disseminated
encephalomyelitis (ADEM) have been reported following primary infection, including
cases associated with anti–myelin oligodendrocyte glycoprotein (MOG) antibodies.9
Heterophile antibody positivity or the presence of viral capsid antigen IgM antibodies
is helpful in establishing acute systemic infection. Caution is needed when interpreting
CSF PCR results as EBV DNA detection does not necessarily indicate CNS infection.
CSF EBV DNA can be detected in the setting of CNS inflammation or infection by a
different pathogen, presumably because of trafficking of latently infected leukocytes
into the intrathecal space.10,11 CSF EBV PCR positivity can also occur in the setting of
CNS lymphoproliferative disorders. Treatment is supportive, but immunotherapies
such as corticosteroids and IV immunoglobulin (IVIg) are frequently used.
OTHER MICROORGANISMS. Other viruses, as well as some atypical bacteria, can also
cause isolated myelitis.
HUMAN IMMUNODEFICIENCY VIRUS. Although most HIV-associated myelopathies
occur late in the course of the disease, acute myelitis can rarely occur in the setting
of recent HIV infection and seroconversion.12 Rare cases of myelitis have also been
described in the setting of discordant HIV viral loads between CSF and plasma. This
phenomenon occurs because of the disparate effectiveness of combination
antiretroviral therapy between the CNS and blood compartments, leading to
unchecked infection in the CNS or CSF viral escape.13 Changing the antiretroviral
regimen to optimize CNS penetrance usually leads to improvement of symptoms.
SEVERE ACUTE RESPIRATORY SYNDROME CORONAVIRUS-2. Rare reports of myelitis,
including a case of necrotizing myelitis, have been reported in association with
severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the pathogen that
CONTINUUMJOURNAL.COM 97
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
causes COVID-19.14 Both parainfectious and postinfectious cases have been
reported, and the virus was not detected in CSF.15 Neural injury secondary to the
hypercytokinemia that is one of the hallmarks of COVID-19 has been postulated as a
potential mechanism, although the nature of the association remains to be elucidated.
MYCOPLASMA PNEUMONIAE. M. pneumoniae is an atypical bacterium commonly
associated with upper respiratory tract infections and acute bronchitis
(TABLE 4-7). CNS manifestations are rare and likely caused by parainfectious or
postinfectious immune-mediated mechanisms rather than direct infection.
Tellingly, the onset of neurologic symptoms is usually days to weeks following
respiratory infection. Most cases of myelitis occur in the setting of ADEM, but
isolated myelitis has been reported.16 MRI usually shows longitudinally extensive
CASE 4-1 A 34-year-old man with chronic myelogenous leukemia (status
post–day 60 after allogeneic hematopoietic stem cell transplantation on
tacrolimus for graft versus host disease prophylaxis) presented with a
3-week history of fevers, encephalopathy, right-sided greater than
left-sided weakness, and urinary retention. Antimicrobial prophylaxis
included valacyclovir, posaconazole, penicillin, and inhaled
pentamidine, with plans to transition to trimethoprim-sulfamethoxazole
following engraftment.
On neurologic examination, he was inattentive and oriented to person
and location only. He had a right homonymous hemianopia. Strength in the
right hemibody was 3/5, with an upper motor pattern of weakness. Strength
in the left hip flexor was 4/5. Deep tendon reflexes were hyperactive (3+)
on the right. Babinski sign was present bilaterally.
Brain MRI demonstrated a hemorrhagic lesion in the left occipital lobe
as well as several lesions with restricted diffusion, some with a ring pattern
but no enhancement (FIGURE 4-1). MRI of the cervical spine showed several
T2-hyperintense lesions (contrast was not given). CSF demonstrated
lymphocytic pleocytosis, and CSF Toxoplasma gondii polymerase chain
reaction (PCR) was positive. He was started on pyrimethamine and
sulfadiazine, with clinical and radiographic improvement seen over the
next few months.
COMMENT This case highlights the importance of reviewing antimicrobial prophylaxis in
patients who are immunocompromised. Toxoplasma encephalitis was
suspected despite atypical features (lack of enhancement, hemorrhagic lesion,
spinal cord involvement) as the patient was not on Toxoplasma gondii
prophylaxis. Toxoplasma encephalitis is rare in hematopoietic stem cell
transplantation but can occur in patients who have received allogeneic
hematopoietic stem cell transplantation and are seropositive, especially within
the first 100 days after transplantation. Because of its potential for
myelosuppression, trimethoprim-sulfamethoxazole prophylaxis for
Pneumocystis jiroveci pneumonia is usually avoided until engraftment. Delayed
engraftment (or intolerance to trimethoprim-sulfamethoxazole) can increase the
risk of Toxoplasma encephalitis.
98 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
T2 signal change with white or gray matter involvement. Not surprisingly,
detection of M. pneumoniae by CSF PCR is rare, as direct infection is not thought to
be the primary mechanism of CNS injury. Diagnosis of recent systemic infection
can be difficult given the lag between infection and onset of neurologic symptoms.
PCR is insensitive, and antibody titers may reflect past infection or cross-reactivity
with other pathogens.17,18 A fourfold rise in IgG titers when comparing acute and
convalescent serum is diagnostic, but this may not always be demonstrable by the
time neurologic symptoms develop. The role of antibiotics is unclear, and
symptoms are usually managed with corticosteroids or IVIg.
TREPONEMA PALLIDUM. Syphilitic meningomyelitis, although rare, is the most
common spinal cord manifestation of syphilis, a sexually transmitted disease caused
FIGURE 4-1
Imaging of the patient in CASE 4-1. A, Axial diffusion-
weighted imaging shows diffusion-restricting lesions
with a ring pattern (arrows). B, Axial gradient recalled
echo (GRE) sequence shows a hemorrhagic lesion in
the left occipital lobe (arrow). Sagittal (C) and axial
(D, E) T2-weighted images show intramedullary
lesions (C, D, E, arrows).
CONTINUUMJOURNAL.COM 99
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
by the spirochete T. pallidum. Neurosyphilis, particularly late forms (eg, tabes
dorsalis, general paresis), was common in the preantibiotic era. In the current era,
early forms (asymptomatic, meningitic, meningovascular) are more commonly
encountered, frequently in patients with HIV coinfection. Meningomyelitis presents,
on average, 6 years after infection, with progressive asymmetric spastic paresis, bladder
dysfunction, and sensory disturbances. Spinal cord MRI shows longitudinally extensive
T2 hyperintensity with pial gadolinium enhancement,19 although patchy parenchymal
enhancement has also been described and imaging findings are nonspecific.20
The first step in establishing the diagnosis of neurosyphilis is confirming infection
with T. pallidum with serum treponemal and nontreponemal testing. Nontreponemal
tests, such as rapid plasma reagin (RPR) or the Venereal Disease Research Laboratory
(VDRL) test are almost always reactive in early disease but may be nonreactive in late
neurosyphilis, particularly in tabes dorsalis. Treponemal tests detect antibodies to
T pallidum and remain positive for life. If serum treponemal tests are negative, the
diagnosis of syphilis is excluded. In the setting of positive serum tests, a reactive CSF
VDRL is diagnostic of neurosyphilis, but a nonreactive VDRL does not rule out the
diagnosis. CSF pleocytosis or an elevated protein in the correct clinical setting may be
diagnostic. Treatment is with 14 days of IV penicillin G.
Myeloradiculitis
Some microorganisms can preferentially affect the nerve roots. Root involvement
with or without associated myelitis can help narrow the differential diagnosis.
HERPES SIMPLEX VIRUS TYPE 2. HSV-2 lays dormant in the sacral dorsal root ganglia,
reactivating to cause recurrent genital lesions. Retrograde migration up the cauda
equina to the conus and lower spinal cord can cause myeloradiculitis. Symptoms
typically involve an anogenital vesicular rash followed by pain, paresthesia,
progressive flaccid paraparesis, and urinary retention. Upper motor neuron signs
may be present on examination and suggest lower thoracic spinal cord
TABLE 4-3 Characteristic CSF Profiles by Etiology
CSF to serum
Protein glucose ratio Nucleated cells (cell predominance) Lactate
3
Normal 15-45 mg/dL >0.6 <5 cells/mm <3.6 mmol/L
Pyogenic bacteriaa Increased Low Increased (neutrophilic)b Increased
c
Viral Normal to slightly increased Normal Increased (lymphocytic) Normal
Tuberculosis Increased Low Increased (lymphocytic) Can be increased
d
Fungal Increased Low Increased (lymphocytic) Can be increased
Parasitic Increased Normal Normal/increased (eosinophilic)e Unknown
a
Lumbar puncture is not recommended in patients with known or suspected epidural abscess both because it is low yield and because of
increased risk of introducing bacteria into CSF.
b
Partially treated meningitis/Listeria monocytogenes can be associated with lymphocytic pleocytosis.
c
Cytomegalovirus and West Nile virus may present with neutrophilic pleocytosis.
d
Coccidioides species can present with eosinophilic pleocytosis; Blastomyces, Candida, and Aspergillus species can cause neutrophilic pleocytosis.
e
Eosinophilic pleocytosis is not always present; lymphocytic and neutrophilic predominance is also seen.
100 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
involvement. CSF normally shows a lymphocytic pleocytosis, and MRI of the KEY POINTS
lumbosacral spine may show signal change and enlargement of the lower cord
● The myelitis associated
with nerve root enhancement. Diagnosis is usually established by demonstrating with Mycoplasma
the presence of HSV-2 DNA by PCR. Patients who are immunocompromised pneumoniae is likely caused
should receive IV acyclovir for 10 to 14 days. Oral antiviral therapy may be by parainfectious or
considered in those who are immunocompetent. Adjunctive corticosteroids are postinfectious immune-
mediated mechanisms.
frequently used. The clinical entity of rapidly progressive lumbosacral
myeloradiculitis is known as Elsberg syndrome. Although commonly associated ● Meningomyelitis is the
with HSV-2, other viruses (including VZV) can present as Elsberg syndrome, but most common spinal cord
an infectious agent is not always identified.21 manifestation of syphilis.
● Treponemal tests remain
CYTOMEGALOVIRUS. A painful ascending lumbosacral myeloradiculitis is also the positive for life following
most common manifestation of CMV spinal cord infection, although isolated infection. Negative
thoracolumbar myelitis has also been reported.22 CMV is a lymphocytic infection treponemal tests essentially
usually acquired in childhood or early adulthood. The virus then becomes latent rule out a diagnosis of
syphilis.
in mononuclear cells and can become reactivated later in life. Primary CMV
infection is usually asymptomatic, although a mononucleosislike syndrome can ● Elsberg syndrome is
occur. CMV nervous system infection occurs almost exclusively in patients who characterized by subacute
are immunocompromised in the setting of reactivation of latent disease, although onset of sacral
myeloradiculitis and is
postinfectious myelitis has been reported with primary infection.23 The CSF of commonly associated with
immunocompromised patients with myeloradiculitis or myelitis usually shows a herpes simplex virus type 2.
neutrophilic predominant pleocytosis with hypoglycorrhachia. Treatment is with
ganciclovir, but outcomes are variable. ● Meningoradiculitis is the
most common spinal
manifestation of Borrelia
LYME DISEASE. Painful meningoradiculitis with or without medullary burgdorferi.
involvement is the most common spinal manifestation of Lyme disease,
although frank myelitis is rare.24 Lyme disease is a tick-borne infection caused
by several species in the spirochete family Borreliaceae. In the United States,
neuroinvasive disease is caused almost exclusively by Borrelia burgdorferi
and is seen in the summer and fall months in the northeastern states and Great
Lakes region. The constellation of painful radiculitis accompanied by facial nerve
palsy and CSF pleocytosis is known as Bannwarth syndrome and appears to be more
common in Europe.25 Neurologic symptoms usually occur weeks after the initial tick
bite. Frequently, but not always, they follow the classic symptoms of fever and
characteristic target rash (erythema migrans). Lymphocytic or monocytic
pleocytosis without hypoglycorrhachia is common, although CSF parameters may
be normal. Diagnostic testing relies on detection of antibodies to B. burgdorferi using
the standard two-tiered testing algorithm, which starts with an initial enzyme
immunoassay.26 Positive samples require supplemental IgM or IgG immunoblot
testing. A newer algorithm involving two different sequential enzyme
immunoassays may be more sensitive for early disease but is not yet widely
available. Although CSF analysis is not required to establish neuroborreliosis in
symptomatic patients who are seropositive, demonstration of intrathecal
production of antibodies against B. burgdorferi with a serum to CSF IgG index can be
helpful in select clinical confounding cases.27 B. burgdorferi PCR is insensitive and
has low overall utility. Recommended treatment in the United States for CNS
involvement is IV ceftriaxone for 2 to 4 weeks.28
SCHISTOSOMIASIS. Parasiticinfections can also present with myeloradiculitis
(TABLE 4-8). Schistosomiasis is a disease caused by five species of parasitic
CONTINUUMJOURNAL.COM 101
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
trematode worms of the genus Schistosoma. Neuroschistosomiasis, characterized
by either myelopathy or encephalitis, is one of the most severe manifestations of
the disease. Schistosomiasis accounts for 1% to 4% of spinal cord lesions in
sub-Saharan Africa, although this is likely an underestimation.29 Myelopathy
occurs primarily with Schistosoma haematobium and Schistosoma mansoni, which
are endemic to sub-Saharan Africa and the Middle East; S. mansoni is also
endemic to parts of South America and some of the South Caribbean Islands.
TABLE 4-4 Laboratory Testing of Select Microorganisms Associated With Myelopathy
and Radiculopathy
Microorganism Laboratory tests (sample type) Comments
Viruses
Enteroviruses Polymerase chain reaction (PCR) (CSF, nasopharyngeal,
stool)
Epstein-Barr virus PCR (CSF, blood), serology (blood), heterophile CSF PCR can be positive in the setting
antibody test (blood) of central nervous system inflammation
or infection by another pathogen
Flaviviruses Serology (blood, CSF), PCR (CSF, blood) In general, serology more sensitive than
PCR, but PCR useful in patients with
congenital or acquired humoral
deficiency because of cross-reactivity
confirmatory testing can be done with
plaque reduction neutralization test
Cytomegalovirus PCR (CSF, blood), serology (blood), serum Serology: IgG appears within weeks
IgG avidity testing (blood) following primary infection and remains
positive for life; IgM is positive during
primary infection but can be
persistently positive or positive during
reactivation; serum IgG avidity assay
can disambiguate between primary and
past infection when both IgM and IgG
are positive
Herpes simplex virus CSF PCR
types 1 and 2
Varicella-zoster virus CSF PCR, serum to CSF IgG ratio CSF PCR sensitivity decreases >1 wk
from symptom onset
Bacteria
Borrelia burgdorferi Traditional algorithm is enzyme immunoassay followed Modified algorithm may be more
by Western blot; modified algorithm is two sequential sensitive for early disease but not yet
enzyme immunoassays; serum/CSF IgG index widely available; CSF PCR is insensitive
Brucella species Culture (blood, CSF, tissue), serology (blood) PCR not widely available
Mycobacterium Culture (blood, CSF, tissue), acid-fast bacilli stain, PCR Interferon gamma release assays can
tuberculosis (CSF, tissue), histopathology confirm exposure, but a negative test
does not rule out the diagnosis
CONTINUED ON PAGE 103
102 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Schistosoma japonicum, which is found in China, the Philippines, and Indonesia,
usually causes encephalitis but can rarely cause myelopathy. Infection is acquired
in freshwater ponds, lakes, and rivers contaminated by free-swimming parasite
larvae (cercariae) shed from snails. Cercariae penetrate the skin and develop into
worms that reside in blood vessels, mate, and produce eggs that travel through
the venous system and lodge in tissues. Myelopathy is thought to occur via
embolization of eggs through retrograde venous flow into the Batson venous
CONTINUED FROM PAGE 102
Microorganism Laboratory tests (sample type) Comments
Treponema pallidum Treponemal tests (fluorescent treponemal antibody A negative CSF Venereal Disease
absorption, treponema pallidum agglutination assay, Research Laboratory test does not rule
enzyme immunoassay), nontreponemal tests (rapid out neurosyphillis
plasma reagin [RPR], Venereal Disease Research
Laboratory test)
Fungi
Aspergillus species Antigen: galactomannan (CSF, blood, bronchoalveolar Galactomannan can be falsely positive
lavage [BAL]), (1,3)-β-D-glucan (CSF, blood, BAL), culture in patients receiving piperacillin-
(CSF, BAL, blood, tissue), PCR (CSF, BAL, tissue), tazobactam and IV immunoglobulin
histopathology (IVIg); (1,3)-β-D-glucan not specific for
Aspergillus; limited availability of PCR;
low sensitivity and specificity
Blastomyces Antigen (blood, urine, CSF), serology (blood, CSF), PCR Serology and antigen studies are more
dermatitidis and (CSF, BAL, tissue), culture (CSF, BAL), histopathology sensitive than PCR
Histoplasma
capsulatum
Coccidioides species Serology (CSF, blood), antigen (CSF, blood, urine), PCR
(CSF, tissue), culture (CSF, tissue), histopathology
Cryptococcus species Antigen (CSF, blood), culture (CSF, blood) Antigen most sensitive and specific test
Parasite
Taenia solium Serology enzyme-linked immunoelectrotransfer blot or Enzyme-linked immunoelectrotransfer
(neurocysticercosis) enzyme-linked immunosorbent assay (ELISA) (blood, blot test of choice; more sensitive in
CSF), histopathology serum; sensitivity reduced if single or
calcified lesion
Schistosoma species Microscopy (stool, urine), serology (blood, CSF),
histopathology
Toxoplasma gondii CSF PCR, histopathology CSF PCR is diagnostic but lacks
sensitivity; serology confirms past
exposure
CSF = cerebrospinal fluid; IgG = immunoglobulin G; IgM = immunoglobulin M.
CONTINUUMJOURNAL.COM 103
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
TABLE 4-5 Assays Targeting Multiple Microorganismsa
Assay Function Pros/cons
Meningitis/encephalitis panel Real-time multiplex polymerase chain Fast turnaround time with potential to
reaction (PCR) that can simultaneously decrease unnecessary antimicrobial
detect 14 pathogens: Escherichia coli exposure
K1, Haemophilus influenzae, Listeria
Sensitivities and specificities comparable
monocytogenes, Neisseria
to individual pathogens but low sensitivity
meningitidis, Streptococcus
for Cryptococcus species
pneumoniae, Streptococcus
agalactiae, cytomegalovirus, Standalone herpes simplex virus PCR has
varicella-zoster virus, herpes simplex higher sensitivity compared to panel
virus types 1 and 2, human herpesvirus 6,
No antibiotic susceptibilities
Enterovirus, human parechovirus, and
Cryptococcus neoformans/
Cryptococcus gattii
16S rRNA PCR with reflex sequencing Detection of 16S rRNA gene Useful for identifying bacteria in patients
(CSF or tissue sample) polymerase, which is highly preserved who have already received antibiotics
in bacteria (including mycobacteria), is
Can be run on paraffin-embedded tissue
followed by sequencing of the
amplified DNA, enabling a diagnosis No antibiotic susceptibilities
Fungal 18S and 28S rRNA/internal Detection of highly preserved fungal Fast turnaround time compared to fungal
transcribed spacer (ITS1 and ITS2) ribosomal genes is followed by cultures
PCR with reflex sequencing (CSF or sequencing of the amplified DNA,
Useful when fungal elements are seen on
tissue sample) enabling diagnosis
paraffin-embedded tissue but fresh tissue
sample no longer available
(1,3)-β-D-Glucan (serum or CSF) (1,3)-β-D-Glucan is a cell wall Sensitivity and specificity in serum varies
polysaccharide present in most fungi depending on population (highest among
(except Cryptococcus species, the patients with hematopoietic stem cell
Zygomycetes, and Blastomyces transplantation)
dermatitidis)
Few studies assessing utility in CSF
Not sufficient to rule out central nervous
system fungal infection if negative
Exposure to antibiotics such as
piperacillin-tazobactam and ampicillin can
cause false-positive results
Metagenomic next-generation All DNA and RNA in CSF or brain tissue Potential to detect any pathogen (bacteria,
sequencing (CSF or tissue sample) sample are sequenced without need virus, fungus, parasite) in a clinical sample,
for prior culturing; results can be including unsuspected pathogens
compared to databases of all known
Sensitivity likely low for pathogens for
microorganisms
which PCR is insensitive
A negative result does not rule out infection
CSF = cerebrospinal fluid; DNA = deoxyribonucleic acid; RNA = ribonucleic acid; rRNA = ribosomal ribonucleic acid.
a
Modified with permission from Yost MD, Toledano M.1 © 2020 Springer Nature.
104 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
plexus, a valveless paravertebral venous system that connects the deep pelvic
veins to the internal vertebral venous plexus. The eggs result in venous
congestion and granulomatous inflammation leading to myeloradiculitis.
Patients usually present with subacute lumbar pain, paraparesis, sensory loss,
and urinary retention. Symptoms can arise months to years after infection, so
eliciting a history of exposure may be challenging, particularly in nonendemic
regions.30 MRI often shows medullary expansion of the conus medullaris or
lower thoracic cord associated with intramedullary, meningeal, or root nodular
enhancement.31 Patients may demonstrate peripheral or CSF eosinophilia.
Definitive diagnosis is by visualization of the eggs on histopathology, but positive
serology, antigen detection, or demonstration of eggs in stool or urine by
microscopy can support the diagnosis in the correct clinical setting. Praziquantel
and corticosteroids are used for treatment, although decompressive surgery is
required in some cases. Neurologic sequelae are common.
FUNGI. Infiltrative meningoradiculitis and meningomyeloradiculitis can occur with
the endemic mycoses caused by the dimorphic fungi Histoplasma capsulatum and
Blastomyces dermatitidis, usually in the setting of chronic meningitis (CASE 4-2).32
Opportunistic fungi such as Cryptococcus can also rarely cause infiltrative
meningomyeloradiculitis (TABLE 4-9).33 MRI in these cases typically shows
leptomeningeal and root enhancement with or without cord signal change.
Similarly, atypical bacteria such as Mycobacterium tuberculosis, Brucella, and
T. pallidum can cause granulomatous myeloradiculitis in the setting of meningitis.
Leukomyelitis
Certain pathogens can preferentially affect the white matter of the spinal cord,
causing a leukomyelitis (leukos means white in Greek). Infections that primarily
affect the lateral columns result in spastic paraparesis, whereas those with
prominent dorsal column involvement result in sensory ataxia.
Herpesviruses Associated With Myelopathy and Radiculopathy TABLE 4-6
Herpesvirus Clinical characteristics Treatment
Herpes simplex virus Sacral myelopolyradiculitis; can be associated with vesicular rash Acyclovir or valacyclovir,
type 2 along sacral dermatomes; isolated myelitis (rare) adjunctive corticosteroids
Varicella-zoster virus Longitudinally extensive or multifocal myelitis, myeloradiculitis, or IV acyclovir with or without
spinal cord infarct; thoracic most common adjunctive corticosteroids
Cytomegalovirus Painful myeloradiculitis in patients who are immunocompromised Ganciclovir and/or foscarnet;
because of virus reactivation; postinfectious myelitis following immunomodulatory therapies
primary infection, can present as poliomyelitis for postinfectious cases
Epstein-Barr virus Probable parainfectious/postinfectious encephalomyelitis with or Supportive treatment;
without radiculopathy following primary infection immunomodulatory therapies
Herpes simplex virus Rare reports of myelitis, mostly in immunocompromised hosts IV acyclovir
type 1
Human herpesvirus 6 Few case reports in patients following allogeneic hematopoietic Ganciclovir, foscarnet,
stem cell transplantation cidofovir
CONTINUUMJOURNAL.COM 105
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
LATERAL COLUMN PREDOMINANT. Human T-cell lymphotropic virus type 1
(HTLV-1) is a retrovirus that infects 5 million to 20 million individuals worldwide.34,35
It is endemic to southern Japan, the Caribbean, South America, Papua New
Guinea, the Melanesian islands, and the Middle East as well as West, Central, and
Southern Africa. The virus is transmitted by breast-feeding, sharing of needles,
sexual intercourse (with male-to-female transmission being more efficient than
the reverse), and blood transfusions and, rarely, via transplanted organs.36
The two main diseases associated with HTLV-1 are adult T-cell leukemia and HTLV-
1–associated myelopathy (HAM), also known as tropical spastic paraparesis (TSP).
HAM/TSP affects between 0.25% and 4% of HTLV-1 carriers, depending on
the population studied, and is more common in females.37 The onset of
myelopathy ranges from 4 months to 30 years after infection, but it almost never
develops in children; the peak incidence is around the fifth decade of life.37 Virus
acquisition through blood transfusion or organ donation may be associated with
more severe disease.38 HAM/TSP has been described as a two-phase disease
consisting of an acute inflammatory phase and a chronic neurodegenerative
phase. The exact mechanism of injury is unknown, but the presence of
lymphocytic infiltrate in the CNS suggests that an aberrant immune response to
HTLV-1 is likely responsible, at least in the early inflammatory phase. Pathologic
studies show inflammation and demyelination of the lateral corticospinal,
spinocerebellar, and spinothalamic tracts, with relative sparing of the dorsal
columns.39 MRI of the spine may show T2-hyperintense lesions with or without
associated gadolinium enhancement, followed by spinal cord atrophy in later stages.
Unlike other parainfectious myelitis, HAM/TSP is characterized by the onset of
slowly progressive proximal greater than distal spastic paraparesis (upper limbs
are usually spared). Back pain and early bladder involvement are common.
Clinical diagnostic criteria have been proposed.40 Detection of HTLV-1 antibodies
is required for the diagnosis of HAM/TSP but lacks specificity. An elevated HTLV-1
proviral load in peripheral blood mononuclear cells can be supportive. CSF protein
concentration and lymphocyte count can be normal or mildly elevated, and
oligoclonal bands may be present. Elevated HTLV-1 proviral load in CSF
TABLE 4-7 Atypical Bacteria Associated With Myelopathy and Radiculopathy
Bacteria Spinal manifestation Treatment
Borrelia species Meningoradiculitis rarely with associated myelitis Ceftriaxone
Brucella species Spondylodiskitis, intramedullary and extramedullary abscess, Ceftriaxone plus rifampin and
granulomatous meningoradiculitis, arachnoiditis doxycycline
Mycobacterium Spondylodiskitis (Pott disease), intramedullary and Isoniazid, rifampin, pyrazinamide,
tuberculosis extramedullary tuberculoma, granulomatous myeloradiculitis, ethambutol for 2 months, followed
tuberous arachnoiditis causing myeloradiculopathy, spinal by isoniazid and rifampin for
artery vasculitis with spinal cord ischemia 7-10 months; corticosteroids
Mycoplasma Probable immune-mediated longitudinally extensive myelitis Corticosteroids, IV immunoglobulin
pneumoniae (IVIg)
Treponema pallidum Meningomyelitis, hypertrophic pachymeningitis with IV penicillin G
polyradiculopathy, meningovascular syphilis resulting in spinal
cord ischemia, spinal gummas
106 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
lymphocytes compared to matched peripheral blood mononuclear cells may be more
specific and help predict progression, but the assay is not widely available.41
Treatment is mainly supportive. Corticosteroids are often used as some studies
have shown that they slow progression and improve pain; however, no randomized
clinical trials have been conducted, and improvement may not be sustained.37
A phase 1–2a study of mogamulizumab, an anti-CCR4 (chemokine receptor
type 4) monoclonal antibody with efficacy in adult T-cell leukemia, was associated
with improvement in some clinical parameters as well as reduction in proviral
load, but larger studies are needed to establish efficacy.42 The general outcome is
progression to disability, but significant variation exists in the rate of progression.
LATERAL AND DORSAL COLUMN INVOLVEMENT. Vacuolar myelopathy is the best
characterized spinal cord abnormality associated with HIV infection, occurring
late in the course of the disease as an acute immunodeficiency syndrome
(AIDS)–defining illness.43 It is characterized pathologically by white matter
vacuolization of the posterior and lateral columns. HIV antigens and
inflammation are usually absent. Although it shares features with the subacute
combined degeneration seen with cobalamin deficiency, the pathophysiology
remains poorly understood. The disease is usually most prominent in the thoracic
cord and causes spastic paraparesis and profound sensory ataxia. MRI may be
normal or may show T2 hyperintensity in the affected tracts. Initiation of
combined antiretroviral therapy is the only effective treatment.
Tabes dorsalis, characterized by degeneration of the posterior column and
dorsal root ganglia, occurs in the setting of chronic untreated syphilis. Typically,
patients develop severe sensory ataxia and lancinating pain. Charcot joints and
Argyll Robertson pupils are often associated. Although common in the
preantibiotic era, tabes dorsalis is only rarely seen in contemporary practice.
Poliomyelitis and Acute Flaccid Myelitis
The word poliomyelitis specifies inflammation of the gray matter within the
spinal cord (poliós means gray in Greek).
Parasitic Infections Associated With Myelopathy and Radiculopathy TABLE 4-8
Parasite Spinal manifestation Treatment
Angiostrongylus Myeloradiculitis Albendazole, adjunctive corticosteroids
cantonensis
Echinococcus species Spondylodiskitis, epidural hydatid cysts Albendazole, surgery
Gnathostoma Eosinophilic myeloradiculitis Supportive care; use of antihelminthic agents
spinigerum remains controversial
Schistosoma species Sacral myeloradiculitis, intramedullary or Praziquantel
extramedullary granuloma
Taenia solium Subarachnoid lesions, intramedullary lesion Corticosteroids with or without surgery for
arachnoiditis; albendazole with or without
corticosteroids for intramedullary disease
Toxoplasma gondii Intramedullary lesion(s) Sulfadiazine plus pyrimethamine plus leucovorin
CONTINUUMJOURNAL.COM 107
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
POLIOVIRUS. Poliomyelitis is historically connected with the poliovirus, a
picornavirus of the genus Enterovirus that infects the anterior horn cells,
manifesting as acute flaccid paralysis. A worldwide vaccination program has
virtually eradicated wild-type virus, and as of 2019, poliomyelitis was endemic
only in Afghanistan and Pakistan. Outbreaks of vaccine-derived poliomyelitis
caused by circulating poliovirus derived from strains in the oral poliovirus vaccine
have occurred in locations with low population immunity.44 Vaccine-associated
paralytic poliomyelitis can also rarely occur in patients who are immunodeficient,
particularly those with B-cell depletion and hypogammaglobulinemia.45,46
Poliovirus infection occurs via the fecal/oral route. Only a small fraction of
those infected develop paralytic disease. The onset of weakness typically coincides
with signs and symptoms of viral meningitis and muscle pain. The distribution
and extent of weakness may vary, ranging from monoparesis to (usually
asymmetric) quadriparesis. Reflexes are decreased or absent, and the sensory
examination is normal. CSF may or may not demonstrate pleocytosis, and,
although CSF PCR rarely detects the virus, it can sometimes be detected in stool
or nasopharyngeal samples. MRI may show T2 hyperintensity primarily affecting
the gray matter of the affected spinal cord levels. Treatment is supportive.
ACUTE FLACCID MYELITIS. Other enteroviruses can also be associated with
poliomyelitis. Since 2012, the United States has experienced a biennial spike in cases
CASE 4-2 A 72-year-old man presented with a 4-month history of lumbar pain with
radicular features and urinary retention. He also reported headache,
fatigue, and myalgia. He had reportedly completed treatment for
pulmonary histoplasmosis 5 years earlier.
Neurologic examination was notable for bilateral proximal greater than
distal lower extremity weakness, which was 4/5 in affected muscles;
absent deep tendon reflexes; and decreased sensation to pinprick up to
the left thigh and right knee.
MRI of the thoracic and lumbar spine revealed leptomeningeal
enhancement around the thoracic cord and conus medullaris as well as
smooth enhancement of the roots without clumping (FIGURE 4-2). CSF
analysis revealed a protein of 127 mg/dL, lymphocytic pleocytosis with 94
cells/mm3, and a low glucose of 21 mg/dL. Urine Histoplasma antigen was
strongly positive. CSF Histoplasma serology, polymerase chain reaction
(PCR), and fungal cultures were negative, but Histoplasma antigen was
positive. CSF and blood (1,3)-β-D-glucan were positive. Imaging and
symptoms improved significantly after completing induction with IV
liposomal amphotericin B.
COMMENT Establishing the diagnosis of central nervous system histoplasmosis can be
difficult. Antigen testing in urine, blood, and CSF should be conducted,
along with serology in CSF and blood. Although specific, PCR is less
sensitive. (1,3)-β-D-Glucan is neither sensitive nor specific but can be
supportive. Some patients exhibit low-level antigenuria following
treatment of pulmonary or disseminated histoplasmosis, but a robustly
elevated antigen level is indicative of active infection.
108 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
of (mostly) pediatric acute flaccid paralysis, termed acute flaccid myelitis.47 These
have coincided temporally and geographically with outbreaks of the nonpolio
enterovirus D68. Both enterovirus D68 and enterovirus 71 have been associated
with cases of flaccid paresis elsewhere in the world, and enterovirus 71 has been
associated with cases of rhombencephalomyelitis in Southeast Asia.48,49 Despite the
strong epidemiologic link, the etiology of acute flaccid myelitis remains elusive.
CSF enterovirus PCR has only rarely been positive in these patients, and less than
half had enterovirus nucleic acid detected in respiratory or stool samples. Recently,
a study identified high levels of CSF enterovirus-specific antibodies in patients with
acute flaccid myelitis despite negative molecular testing, further supporting a causal
role for nonpolio enteroviruses.50 According to the 2020 consensus definition, a
patient presenting with acute flaccid paresis and MRI spine showing predominantly
gray matter involvement in one or more vertebral segments is considered a
confirmed case.47 CSF pleocytosis is not required. Currently no targeted therapies
have demonstrated efficacy, although IVIg is often used. Plasma exchange and
corticosteroids have also been suggested, but theoretical concerns exist about their
use in the setting of potentially active viral infection.51
52,53
OTHER VIRUSES. Adenoviruses have also been associated with poliomyelitis. In
addition, flaviviruses, a family of arthropod-borne RNA viruses more commonly
associated with meningoencephalitis, can also cause poliomyelitis (TABLE 4-10).
FIGURE 4-2
Imaging of the patient in CASE 4-2. Sagittal (A) and axial (B, C) postcontrast T1-weighted MRIs
show smooth leptomeningeal enhancement of the thoracic cord and conus medullaris (A, B,
arrows), as well as enhancement of the cauda equina roots (A, asterisks; C, arrow).
CONTINUUMJOURNAL.COM 109
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
WEST NILE VIRUS. West Nile virus is now endemic throughout the continental
United States. One percent of infections are neuroinvasive, including an acute
poliomyelitis or ventral root infection that manifests as acute flaccid paralysis.54
The latter commonly presents as acute flaccid monoparesis and fever with or
without associated meningoencephalitis and occurs in summer and early fall,
months in which the Culex mosquito thrives.
POWASSAN VIRUS. Powassan virus, which is carried by ticks and found in the
Northeast and Great Lakes regions of the United States, can also cause flaccid
paresis, usually between late spring and midfall, when ticks are most active
(CASE 4-3).55 Viremia is short-lived, and CSF PCR is an insensitive diagnostic
test unless performed early in the course of the disease.56 IgM-captured
enzyme-linked immunosorbent assay (ELISA) in either blood or CSF during the
acute phase is diagnostic. Although highly sensitive, the ELISA has poor
specificity given significant cross-reactivity with other flaviviruses.57
Confirmatory plaque reduction neutralization testing can be performed,
although the clinical utility may be limited in the absence of targeted antiviral
TABLE 4-9 Fungal Infections Associated With Myelopathy and Radiculopathy
Microorganism Spinal involvement Systemic involvement Treatment
Endemic fungi
Blastomyces Spondylodiskitis, intramedullary and Chronic pneumonia, verrucous lesions Liposomal
dermatitidis extramedullary abscess, with irregular borders, subcutaneous amphotericin B
myeloradiculitis nodules, prostatitis, osteomyelitis followed by an azole
Coccidioides Adhesive arachnoiditis, Pneumonia, fever, drenching night Oral fluconazole for life
species spondylodiskitis, intramedullary and sweats, weight loss, arthralgia,
extramedullary abscess erythema nodosum
Histoplasma Meningoradiculitis, meningomyelitis, In pulmonary disease: fever, chills, Liposomal
capsulatum spondylodiskitis, intramedullary and myalgia, anorexia, cough, chest pain, amphotericin B
extramedullary abscess chest x-ray showing mediastinal lymph followed by
nodes itraconazole
In disseminated disease: pancytopenia,
hepatosplenomegaly, endocarditis,
adrenal insufficiency, osteomyelitis
Opportunistic fungi
Aspergillus Necrotizing myelopathy, Pneumonia associated with single or Voriconazole or
species intramedullary and extramedullary multiple nodules surrounded by isavuconazole
mass lesions, spondylodiskitis ground-glass infiltrates (halo sign),
cavitations, rhinosinusitis,
endophthalmitis
Candida Spondylodiskitis, extramedullary Osteoarticular infections, endocarditis, Liposomal
species abscess endophthalmitis, peritonitis, amphotericin B with or
pneumonia, mediastinitis without flucytosine
Cryptococcus Meningomyeloradiculitis, Asymptomatic focal pneumonitis, rarely Liposomal
species intramedullary/extramedullary mass symptomatic pneumonia, fever, night amphotericin B
lesions (cryptococcoma) sweats followed by flucytosine
110 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
therapy. Serologic tests can be falsely negative in patients with congenital or
acquired humoral deficiency (eg, patients on B-cell–depleting therapies such as
rituximab), and PCR is usually needed to establish the diagnosis in these cases.58
RABIES. Paralytic rabies can also present with flaccid paresis. Rabies is caused by
a number of different species of viruses in the Rhabdoviridae family, genus
Lyssavirus, and usually transmitted to humans by bites from animal vectors. The
onset of clinical disease is between 20 and 90 days from exposure. Although a
majority of patients present with the more common encephalitic form, about
20% of patients develop paralytic rabies.59 These patients typically have early
progressive flaccid weakness that initially may affect only the bitten limb but
invariably spreads to other limbs and bulbar muscles. Sphincter dysfunction,
pain, piloerection, and sensory disturbances can occur, but hydrophobia is rare.
Several tests are required to confirm the diagnosis, including virus isolation
from saliva or skin via reverse transcriptase PCR or detection of antibodies in
serum and CSF.59 Once symptoms arise, no treatment has been found to be
effective and the disease is invariably fatal.60
Spinal Cord Infarct
Although relatively rare, some microorganisms can be associated with spinal
cord ischemic or hemorrhagic stroke.
Flaviviruses Associated With Myelopathy TABLE 4-10
Flavivirus Mechanism Area of involvement Vector Endemicity
West Nile virus Neuroinvasive Anterior horn cells and Culex species North America, the Caribbean, Africa,
roots mosquitoes the Middle East, parts of Europe and
the former Soviet Union
Powassan virus Neuroinvasive Anterior horn cells Ixodes Minnesota, Wisconsin, New York,
species ticks Massachusetts, Ontario, Manitoba,
Nova Scotia
St. Louis Neuroinvasive Anterior horn cells Culex species North and South America, but most
encephalitis mosquitoes cases reported in the eastern and
virus central United States
Tick-borne Probably Anterior horn cells Ixodes Baltic States, Russia, the Balkans,
encephalitis neuroinvasive species ticks Nordic countries
virus
Japanese Neuroinvasive Anterior horn cells Culex species Temperate regions of China, Japan,
encephalitis mosquitoes the Korean peninsula, the Indian
virus subcontinent, Southeast Asia
Dengue virus Neuroinvasive Longitudinally extensive Aedes species Central and South America, the
parainfectious/ or multifocal leukomyelitis mosquitoes Caribbean, Southeast Asia, the
postinfectious Pacific Islands; rarely, the southern
United States
Zika virus Neuroinvasive Longitudinally extensive Aedes species Outbreaks have occurred in Central,
parainfectious/ or multifocal mosquitoes North, and South America; the
postinfectious leukomyelitis, anterior Caribbean; Africa; Southeast Asia;
horn cells, roots and the Pacific Islands
CONTINUUMJOURNAL.COM 111
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
VARICELLA-ZOSTER VIRUS. Pathologic studies of VZV meningoencephalomyelitis
suggest the virus causes a necrotizing small vessel vasculitis with local
demyelination and neuronal inclusions. A postviral (days to months) vasculopathy
affecting larger caliber cerebral vessels has also been described.2 Spinal cord
ischemia, although rare, has been reported in association with VZV infection.61
TREPONEMA PALLIDUM. T. pallidum can cause an infection-associated inflammatory
arteriopathy of the leptomeninges known as meningovascular syphilis, which can
rarely result in spinal cord infarcts.62
BACTERIAL AND MYCOBACTERIAL MENINGITIS. Rarely, bacterial and mycobacterial
meningitis can be associated with anterior spinal artery infarction.63
ASPERGILLUS. Aspergillus can cause necrotizing myelitis with associated spinal
cord infarction, highlighting the angioinvasive nature of this opportunistic
mold.64 Typically, Aspergillus causes severe systemic infections in patients who
are immunocompromised, especially those with severe neutropenia. As with
most fungi, the route of infection is through inhalation into the lungs and
paranasal sinuses. Immune suppression allows dissemination to extrapulmonary
sites, including the CNS, where it more commonly presents with mass lesions.
Detection of galactomannan, a major constituent of Aspergillus cell wall, in
CASE 4-3 A 56-year-old woman from Minnesota presented to the hospital in
mid-October with new-onset fever, encephalopathy, and flaccid paresis
of her right arm. At admission, her temperature was 39.2 °C (102.6 °F).
On neurologic examination, she was sleepy but easily arousable and
oriented to person only. Strength in the right upper extremity was normal
with the exception of her deltoid, biceps, and triceps, which were 3/5.
Strength in the left arm and legs was normal. Deep tendon reflexes were
absent in the right upper extremity but present elsewhere. Sensation
appeared intact. Babinski sign was present on the right.
CSF revealed lymphocytic pleocytosis with normal glucose. Brain MRI
showed T2 hyperintensities in the deep gray matter nuclei on the left, but
MRI of the cervical spine was negative. Nerve conduction studies and EMG
were consistent with a disorder of the anterior horn cells affecting right
cervical myotomes (FIGURE 4-3). West Nile virus serology was negative.
Powassan virus was positive via CSF enzyme-linked immunosorbent assay
(ELISA) testing, later confirmed by plaque reduction neutralization testing.
COMMENT This case highlights the importance of recognizing characteristic clinical
patterns as well as the importance of paying attention to endemicity and
seasonality. The patient presented with encephalomyelitis, acute flaccid
monoparesis, and electrodiagnostic features suggestive of anterior horn cell
disease, all of which are suggestive of Flavivirus infection. Mid-October is
past mosquito season, making West Nile virus unlikely. Powassan virus,
however, is endemic to the Upper Midwest and northeastern states and
transmitted by ticks, which persist through early fall.
112 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
serum, bronchoalveolar lavage, or CSF can help establish the diagnosis.
(1,3)-β-D-Glucan, a cell wall component of many fungi, can also be detected but
is less specific. Histopathologic studies may be necessary for confirmation.
Intramedullary Abscess
Intramedullary abscess of the spinal cord is a rare clinical entity. This is partly
because normal spinal cord tissue appears to be remarkably resistant to
hematogenous spread from infection, which is a common cause of abscess
formation. When hematogenous spread does occur, a predisposing spinal cord
abnormality is common.65 Another mechanism is contiguous spread of infection
through a dermal sinus tract, more commonly in the lumbar region. In these
cases, pathogens reflect the microorganisms colonizing the skin surrounding the
sinus tract opening, including Staphylococcus species as well as gram-negative
rods and anaerobes. Most patients present with weakness, back pain with
radicular features, and bladder dysfunction. Fever occurs in less than 50% of
patients.65 MRI shows rim enhancement and surrounding edema and can be
associated with internal restricted diffusion.
Empiric antimicrobial therapy should be based on the presumed mechanism
of infection. Myelotomy and abscess drainage are usually required and help guide
antimicrobial therapy. Ampicillin should be initiated empirically in cryptogenic
cases to cover for Listeria monocytogenes.65 Mortality occurs in less than 10% of
cases, but residual neurologic deficits are common.65
FIGURE 4-3
Nerve conduction study and EMG results of the patient in CASE 4-3. A, Nerve conduction
studies show low-amplitude compound muscle action potentials (CMAPs) in the right arm
(box). B, Needle EMG demonstrates dense fibrillation potentials (box) and reduced motor
unit action potential recruitment in right upper extremity muscles.
CONTINUUMJOURNAL.COM 113
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
Microorganisms other than pyogenic bacteria that can cause intramedullary
rim-enhancing lesions include M. tuberculosis (tuberculomas), endemic and
opportunistic fungi, parasites, and CMV (TABLE 4-11).
EXTRAMEDULLARY INFECTION
Pyogenic bacteria are a common cause of extramedullary infection, but atypical
bacteria, fungi, and parasites can also seed extramedullary sites, leading to
compressive myelopathy and radiculopathy.
Spondylodiskitis and Spinal Epidural Abscess
Spondylitis (vertebral osteomyelitis) and infection of the adjacent intervertebral
space (diskitis) most often occur as a result of hematogenous seeding from a
distant focus of infection. Other routes of infection include direct inoculation
from trauma or surgical procedure or contiguous spread from an adjacent soft
tissue infection. Most cases occur in patients older than 50 years of age, and males
are affected twice as often as females. Important risk factors include injection
drug use, degenerative spine disease, prior spinal instrumentation, diabetes
mellitus, infective endocarditis, dialysis, corticosteroid therapy, or any
immunocompromised state.
Staphylococcus aureus accounts for more than 50% of cases in developed countries.
Other causes include enteric gram-negative bacilli as well as pyogenic and
nonpyogenic streptococci. Pseudomonas aeruginosa, coagulase-negative
Staphylococcus, and Candida species are seen in association with line infections and
injection drug use. M. tuberculosis still accounts for a substantial number of spinal
TABLE 4-11 Etiologies of Spinal Cord Intramedullary Ring-Enhancing Lesions
Viral
◆ Cytomegalovirus
Bacterial
◆ Pyogenic bacteria
◆ Mycobacterium tuberculosis (tuberculoma)
◆ Brucella species
Fungal
◆ Endemic fungi
◇ Blastomyces dermatitidis
◇ Coccidioides species
◇ Histoplasma capsulatum
◆ Opportunistic fungi
◇ Aspergillus species
◇ Cryptococcus species (cryptococcoma)
Parasitic
◆ Schistosoma species
◆ Taenia solium (neurocysticercosis)
◆ Toxoplasma gondii
114 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
cord infections worldwide, both in areas with high rates of disease (including KEY POINTS
sub-Saharan and North Africa, India, Southeast Asia, Micronesia, China, Eastern
● Neuroschistosomiasis
Europe, and Central and South America) and in countries with large populations from can present as an
endemic regions. Although spinal manifestations of tuberculosis (TB) are protean, insidious lumbosacral
tuberculous spondylitis (Pott disease) is by far the most common. In developed myeloradiculitis.
countries, TB usually presents as reactivation in adults from endemic regions. Brucella
● Human T-cell
and Echinococcus are rare causes of spondylodiskitis in endemic regions.66-68 Endemic
lymphotropic virus type
and opportunistic fungi are a rare but important cause of spondylodiskitis in those 1–associated myelopathy
who are immunocompromised. presents with slowly
The main clinical presentation of spondylodiskitis is insidious neck or back progressive proximal
pain, usually localized to the infected disk space. The pain is usually worse with greater than distal spastic
paraparesis and early
activity and can be reliably exacerbated with percussion over the involved urinary retention.
posterior spinous process. Fever is present in less than 50% of cases.69 Leukocytosis
is not always present, but elevations in erythrocyte sedimentation rate and ● Human immunodeficiency
C-reactive protein are observed in more than 80% of patients. Spondylodiskitis virus–associated vacuolar
myelopathy occurs most
associated with TB, Brucella, or fungi has a more indolent course and is generally commonly in advanced
less painful than pyogenic spondylodiskitis. Consequently, many patients exhibit infection, but the
signs of nervous system compromise by the time of diagnosis. pathophysiology does not
Blood and urine cultures should be obtained in all patients suspected of having seem to be caused by viral
cord infection or
spondylodiskitis and are positive in up to 50% of patients. If blood cultures are
inflammation.
positive for gram-positive organisms, evaluation for infective endocarditis
should be considered in those with a history of valvular disease or new-onset ● Although tabes dorsalis
heart failure. Although MRI cannot reliably distinguish between tuberculous and was common in the
pyogenic spondylodiskitis, features favoring TB infection include intervertebral preantibiotic era, it is only
rarely seen in contemporary
disk sparing, extensive paraspinal soft-tissue involvement, heterogeneous practice.
vertebral body enhancement, involvement of multiple vertebral bodies, and
subligamentous spread.70 Biopsy is warranted to establish a microbiologic ● The clinical presentation
diagnosis when blood and urine cultures are negative. If TB is suspected, tissue of poliomyelitis is usually
monoparesis with reflex
should be sent for acid-fast stain and mycobacterial culture. Existing molecular loss.
assays can simultaneously detect M. tuberculosis and rifampin resistance. Tissue
microscopy usually reveals necrotizing granulomas. ● Despite the strong
Spinal epidural abscesses frequently arise in the setting of spondylodiskitis; thus, epidemiologic link with
enterovirus D68, the
the two conditions share much of their epidemiology and microbiology.
etiology of epidemic acute
Hematogenous seeding of epidural fat, lymphatic spread from an oropharyngeal flaccid myelitis remains
abscess, or direct invasion of the epidural space in the setting of surgery or elusive.
penetrating trauma can also result in the formation of an epidural abscess.
Initial manifestations are similar to those of spondylodiskitis and ● Viremia is short-lived with
most flaviviruses, and
characterized by localized pain and fever, but patients eventually develop polymerase chain reaction is
radicular pain followed by frank myelopathic signs (CASE 4-4). Once weakness insensitive. Blood or CSF
develops, deficits may become irreversible without intervention within IgM in the acute setting
24 hours.71 When suspected, MRI should be obtained and empiric antibiotic establishes the diagnosis.
therapy initiated. Surgical decompression and drainage in addition to systemic
● Aspergillus can present
antibiotic therapy (guided by culture and susceptibilities) are the treatments of with spinal cord ischemia
choice in those with progressive neurologic deficits. and hemorrhage.
Treatment of spinal TB involves induction with a four-drug regimen
consisting of isoniazid, rifampin, pyrazinamide, and ethambutol for 2 months ● Ampicillin should be
initiated empirically in
followed by 7 to 10 months of isoniazid and rifampin. Medical management has cryptogenic spinal cord
been shown to be equal to combined medical and surgical management in abscess for Listeria
patients with tuberculous spondylitis (Pott disease) who are ambulatory at the coverage.
time of diagnosis.72
CONTINUUMJOURNAL.COM 115
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
Dural Disease and Arachnoiditis
Dural and arachnoid involvement by some pathogens can result in compressive
myelopathy and radiculopathy, either exclusively or in addition to parenchymal
inflammation caused by infiltrative disease.
TREPONEMA PALLIDUM. T. pallidum can cause hypertrophic pachymeningitis,
which can present as polyradiculopathy. Focal meningeal inflammation from T.
pallidum may lead to the formation of masslike lesions or gummas that can result
CASE 4-4 A 75-year-old man with a prosthetic mechanical aortic valve developed
severe lumbar back pain days after successful cardioversion for
incidentally discovered atrial
fibrillation. A week later,
he noted radicular features
followed by a right footdrop.
He denied fevers but
reported having chills.
On examination, he had
tenderness with percussion
of his lumbar spine. C-reactive
protein was elevated at
92 mg/L, and he had a mild
leukocytosis at 11.3 cells/mm3.
MRI of the lumbar spine
showed evidence of
spondylodiskitis at L5-S1 and
associated epidural abscess
extending from the distal
margin of the thecal sac to L1
(FIGURE 4-4). He was started
on empiric antimicrobials and
underwent lumbar
decompression and washout.
Blood and tissue cultures FIGURE 4-4
grew Enterococcus faecalis. Imaging of the patient in CASE 4-4. Sagittal
Given his cardiac history, he T2-weighted (A) and postcontrast T1-weighted (B)
MRIs of the lumbar spine show L5-S1 disk edema
underwent a transesophageal
with faint enhancement (A, B, arrows) as well as a
echocardiogram, which rim-enhancing epidural fluid collection extending
demonstrated endocarditis. from the thecal sac to L1 (A, B, asterisks).
COMMENT Focal spinal pain readily reproducible by percussion is suggestive of
spondylodiskitis even in the absence of fever. The emergence of
neurologic deficits is concerning for an evolving epidural abscess and
demands prompt evaluation with MRI as delays in management can result
in permanent disability. Cardiac history and detection of gram-positive
organisms are indicative of possible endocarditis, and a transesophageal
echocardiogram should be performed.
116 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
in compressive myelopathy or radiculopathy. MRI spine commonly reveals mass KEY POINTS
lesions that are hypointense on T1-weighted images and hyperintense on
● Tuberculous spondylitis
T2-weighted images, usually with adjacent parenchymal edema. The vast
(Pott disease) is the most
majority are associated with fairly homogeneous gadolinium enhancement, and common spinal
the appearance can mimic a meningioma.73 manifestation of
tuberculosis.
COCCIDIOIDOMYCOSIS. Coccidioidomycosis is a fungal infection endemic to the
● Fever is present in less
southwestern United States characteristically associated with pulmonary than 50% of patients with
infection. Meningitis is the most common CNS manifestation, but a compressive pyogenic spondylodiskitis or
myelopathy can be seen in association with spinal block. The altered CSF epidural abscess.
dynamics are caused by adhesive arachnoiditis that results from the thick
● Fungal and mycobacterial
gelatinous exudate characteristic of this and other fungal diseases.74
infection can cause adhesive
arachnoiditis, resulting in
MYCOBACTERIUM TUBERCULOSIS. M. tuberculosis can present in a similar fashion, spinal block and myelopathy
typically as a subacute myeloradiculopathy (tuberculous spinal arachnoiditis). In with or without
syringomyelia.
these cases, the inflammatory exudates surround but do not necessarily infiltrate the
spinal cord and nerve roots.75 MRI spine may demonstrate nodular meningeal ● Unlike intracerebral
enhancement, nerve root thickening, and intramedullary signal change, with or disease, which
without an associated syrinx.75 CSF typically reveals moderate lymphocytic pleocytosis, predominantly involves the
hypoglycorrhachia, and a markedly elevated protein indicative of spinal block. brain parenchyma, most
spinal neurocysticercosis
occurs in the subarachnoid
NEUROCYSTICERCOSIS. Unlike intracerebral disease, which predominantly involves space, resulting in
the brain parenchyma, most spinal neurocysticercosis occurs in the subarachnoid compressive myelopathy.
space, although intramedullary involvement occurs in about 20% of cases.76
Worldwide, cysticercosis remains the most common parasitic infection of the
central nervous system. Although predominantly intracranial, neurocysticercosis
can involve the spine in 1.5% to 3% of cases.76 Neurocysticercosis is caused by
infection by the eggs of the pork tapeworm Taenia solium, which is endemic to
Central America, South America, sub-Saharan Africa, India, and East Asia.77 Ingestion
of cysticercal eggs in food contaminated by human feces results in absorption
through the gut and migration to muscle, eye, or CNS.77 Dissemination to the
CNS occurs through small capillaries into the parenchyma or through the choroid
plexus into the ventricles and subsequently the subarachnoid space. The signs
and symptoms of neurocysticercosis are secondary to inflammation resulting
from the degenerating cyst and lead to edema, or, in extraparenchymal disease,
arachnoiditis or meningitis.
The signs and symptoms of spinal neurocysticercosis depend on a number of
factors, including location (subarachnoid versus intramedullary), spinal level, and
the presence or absence of inflammation and associated arachnoid scarring because
of cyst degeneration.76 Small intramedullary lesions often become symptomatic
early and rapidly, whereas extramedullary lesions may present late and insidiously
as the cyst grows large enough to compress the spinal cord or cauda equina roots.
Diagnosis is made by epidemiology and characteristic imaging features,
and serologic testing can help support the diagnosis. Enzyme-linked
immunoelectrotransfer blot is superior to the more widely available ELISA.
Serum is more sensitive than CSF, whereas CSF examination generally plays a
limited role in the diagnosis of neurocysticercosis. In cases of intramedullary
disease, CSF can be normal or associated with mild protein elevation and
pleocytosis. In the setting of arachnoiditis, marked protein elevation; monocytic,
neutrophilic, or eosinophilic pleocytosis; and hypoglycorrhachia may be observed.
CONTINUUMJOURNAL.COM 117
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
Intramedullary cysts are treated with either albendazole or a combination of
albendazole and praziquantel with adjunctive corticosteroids. Subarachnoid
cysts may require higher doses and more prolonged treatment or may require
surgical intervention. The inflammatory arachnoiditis resulting from cyst
degeneration may limit recovery despite treatment.76
CONCLUSION
When evaluating patients with suspected infectious myelopathies and
radiculopathies, it is important to narrow the range of pathogens under consideration.
Specific clinicoradiographic features and careful attention to exposure, travel history,
and immunocompetence can help narrow the differential. Direct infection is
responsible for the neural injury in many cases; however, in others a parainfectious or
postinfectious immune-mediated process is likely. Antimicrobial therapy is the
mainstay of treatment, although effective antiviral therapies are lacking. Given that
injury to the spinal cord usually involves both infectious and inflammatory
mechanisms, strategies targeting each separately are often justified.
REFERENCES
1 Yost MD, Toledano M. Severe infections of the 10 Davies NWS, Brown LJ, Gonde J, et al. Factors
central nervous system. In: Rabinstein AA, ed. influencing PCR detection of viruses in
Neurological emergencies: a practical approach. cerebrospinal fluid of patients with suspected
Springer; 2020:121-149. CNS infections. J Neurol Neurosurg Psychiatry
2 Gilden D, Nagel MA, Cohrs RJ. Varicella-zoster. 2005;76(1):82-87 doi:10.1136/jnnp.2004.045336
Handb Clin Neurol 2014;123:265-283. doi:10.1016/ 11 Martelius T, Lappalainen M, Palomäki M, Anttila
B978-0-444-53488-0.00012-2
VJ. Clinical characteristics of patients with
3 Nagel MA, Cohrs RJ, Mahalingam R, et al. The Epstein Barr virus in cerebrospinal fluid. BMC Infect
varicella zoster virus vasculopathies: clinical, CSF, Dis 2011;11:281. doi:10.1186/1471-2334-11-281
imaging, and virologic features. Neurology 2008;
70(11):853-860. doi:10.1212/01. 12 Andrade P, Figueiredo C, Carvalho C, et al.
wnl.0000304747.38502.e8 Transverse myelitis and acute HIV infection: a
case report. BMC Infect Dis 2014;14:149.
4 Haanpää M, Dastidar P, Weinberg A, et al. CSF
doi:10.1186/1471-2334-14-149
and MRI findings in patients with acute herpes
zoster. Neurology 1998;51(5):1405-1411. doi:10.1212/ 13 Canestri A, Lescure FX, Jaureguiberry S, et al.
wnl.51.5.1405 Discordance between cerebral spinal fluid and
plasma HIV replication in patients with
5 Ahmed SV, Hamada H, Jayawarna C, Chandra S.
Shingles with secondary asymptomatic CNS neurological symptoms who are receiving
involvement! BMJ Case Rep 2012;2012: suppressive antiretroviral therapy. Clin Infect Dis
bcr0320126041. doi:10.1136/bcr.03.2012.6041 2010;50(5):773-778. doi:10.1086/650538
6 Mathew T, Thomas K, Shivde S, et al. Post herpes 14 Sotoca J, Rodríguez-Álvarez Y. COVID-19-
zoster infection neuromyelitis optica spectrum associated acute necrotizing myelitis. Neurol
disorder. Mult Scler Relat Disord 2017;18:93-94. Neuroimmunol Neuroinflamm 2020;7(5):e803.
doi:10.1016/j.msard.2017.09.022 doi:10.1212/NXI.0000000000000803
7 Majid A, Galetta SL, Sweeney CJ, et al. 15 Zachariadis A, Tulbu A, Strambo D, et al.
Epstein-Barr virus myeloradiculitis and Transverse myelitis related to COVID-19
encephalomyeloradiculitis. Brain 2002; infection. J Neurol 2020:1-3.doi:10.1007/
125(Pt 1):159-165. doi:10.1093/brain/awf010 s00415-020-09997-9
8 Merelli E, Bedin R, Sola P, et al. 16 Tsiodras S, Kelesidis T, Kelesidis I, et al.
Encephalomyeloradiculopathy associated with Mycoplasma pneumoniae-associated myelitis: a
Epstein-Barr virus: primary infection or comprehensive review. Eur J Neurol 2006;13(2):
reactivation? Acta Neurol Scand 1997;96(6):
416-420. doi:10.1111/j.1600-0404.1997.tb00309.x 112-124. doi:10.1111/j.1468-1331.2006.01174.x
9 Nakamura Y, Nakajima H, Tani H, et al. Anti-MOG 17 Nir-Paz R, Michael-Gayego A, Ron M, Block C.
antibody-positive ADEM following infectious Evaluation of eight commercial tests for Mycoplasma
mononucleosis due to a primary EBV infection: pneumoniae antibodies in the absence of acute
a case report. BMC Neurol 2017;17(1):76. infection. Clin Microbiol Infect 2006;12(7):
doi:10.1186/s12883-017-0858-6 685-688. doi:10.1111/j.1469-0691.2006.01469.x
118 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
18 Lai CH, Chang LL, Lin JN, et al. High 32 Tan V, Wilkins P, Badve S, et al. Histoplasmosis of
seroprevalence of Mycoplasma pneumoniae IgM the central nervous system. J Neurol Neurosurg
in acute Q fever by enzyme-linked Psychiatry 1992;55(7):619-622. doi:10.1136/jnnp.55.7.619
immunosorbent assay (ELISA). PLoS One 2013;
33 Murai H, Tokunaga H, Kubo I, et al.
8(10):e77640. doi:10.1371/journal.pone.0077640
Myeloradiculitis caused by Cryptococcus
19 Kikuchi S, Shinpo K, Niino M, Tashiro K. Subacute neoformans infection in a patient with ulcerative
syphilitic meningomyelitis with characteristic colitis: a neuropathological study. J Neurol Sci 2006;
spinal MRI findings. J Neurol 2003;250(1):106-107. 247(2):236-238. doi:10.1016/j.jns.2006.05.050
doi:10.1007/s00415-003-0921-7 34 Gessain A, Cassar O. Epidemiological aspects and
20 Chilver-Stainer L, Fischer U, Hauf M, et al. world distribution of HTLV-1 infection. Front
Syphilitic myelitis: rare, nonspecific, but Microbiol 2012;3:388. doi:10.3389/fmicb.2012.00388
treatable. Neurology 2009;72(7):673-675. 35 de Thé G, Bomford R. An HTLV-I vaccine: why,
doi:10.1212/01.wnl.0000342460.07764.5c how, for whom? AIDS Res Hum Retroviruses 1993;
9(5):381-386. doi:10.1089/aid.1993.9.381
21 Savoldi F, Kaufmann TJ, Flanagan EP, et al.
Elsberg syndrome: A rarely recognized cause of 36 Tagaya Y, Matsuoka M, Gallo R. 40 years of the
cauda equina syndrome and lower thoracic human T-cell leukemia virus: past, present, and
myelitis. Neurol Neuroimmunol Neuroinflamm future. F1000Res 2019;8. doi:10.12688/
2017;4(4):e355. doi:10.1212/NXI.0000000000000355 f1000research.17479.1
22 Hénin D, Smith TW, De Girolami U, et al. 37 Bangham CR, Araujo A, Yamano Y, Taylor GP.
Neuropathology of the spinal cord in the HTLV-1-associated myelopathy/tropical spastic
acquired immunodeficiency syndrome. paraparesis. Nat Rev Dis Primers 2015;1:15012.
Hum Pathol 1992;23:1106-1114. doi:10.1016/ doi:10.1038/nrdp.2015.12
0046-8177(92)90028-2
38 Toro C, Rodés B, Poveda E, Soriano V. Rapid
23 Karacostas D, Christodoulou C, Drevelengas A, development of subacute myelopathy in three
et al. Cytomegalovirus-associated transverse organ transplant recipients after transmission of
myelitis in a non-immunocompromised patient. human T-cell lymphotropic virus type I from a
Spinal Cord 2002;40(3):145-149. doi:10.1038/ single donor. Transplantation 2003;75(1):102-104.
sj.sc.3101265 doi:10.1097/00007890-200301150-00019
24 Halperin JJ. Neuroborreliosis. Neurol Clin 2018; 39 Nagai M, Osame M. Human T-cell lymphotropic
36(6):821-830. doi:10.1007/s00415-016-8346-2 virus type I and neurological diseases. J Neurovirol
2003;9(2):228-235. doi:10.1080/13550280390194028
25 Stanek G, Strle F. Lyme disease: European
perspective. Infect Dis Clin North Am 2008;22(2): 40 De Castro-Costa CM, Araújo AQ, Barreto MM,
327-339, vii. doi:10.1016/j.idc.2008.01.001 et al. Proposal for diagnostic criteria of tropical
spastic paraparesis/HTLV-I-associated myelopathy
26 Centers for Disease Control and Prevention (TSP/HAM). AIDS Res Hum Retroviruses 2006;22
(CDC). Recommendations for test performance (10):931-935. doi:10.1089/aid.2006.22.931
and interpretation from the Second National
Conference on Serologic Diagnosis of Lyme 41 Enose-Akahata Y, Jacobson S. Immunovirological
Disease. MMWR Morb Mortal Wkly Rep 1995; markers in HTLV-1-associated myelopathy/tropical
44(31):590-591. spastic paraparesis (HAM/TSP). Retrovirology 2019;16
(1):35. doi:10.1186/s12977-019-0499-5
27 Blanc F, Jaulhac B, Fleury M, et al. Relevance
of the antibody index to diagnose Lyme 42 Sato T, Coler-Reilly ALG, Yagishita N, et al.
neuroborreliosis among seropositive patients. Mogamulizumab (Anti-CCR4) in HTLV-1-
Neurology 2007;69(10):953-958. doi:10.1212/ Associated Myelopathy. N Engl J Med 2018;
01.wnl.0000269672.17807.e0 378(6):529-538. doi:10.1056/NEJMoa1704827
28 Halperin JJ, Shapiro ED, Logigian E, et al. Practice 43 Di Rocco A. Diseases of the spinal cord in human
parameter: treatment of nervous system Lyme immunodeficiency virus infection. Semin Neurol
disease (an evidence-based review): report of 1999;19(2):151-155. doi:10.1055/s-2008-1040832
the Quality Standards Subcommittee of the
American Academy of Neurology. Neurology 44 Platt LR, Estívariz CF, Sutter RW. Vaccine-
2007;69(1):91-102. doi:10.1212/01. associated paralytic poliomyelitis: a review of
the epidemiology and estimation of the global
wnl.0000265517.66976.28
burden. J Infect Dis 2014;210 suppl 1:S380-S389.
29 Ferrari TCA, Moreira PRR. Neuroschistosomiasis: doi:10.1093/infdis/jiu184
clinical symptoms and pathogenesis. Lancet 45 Kew O, Morris-Glasgow V, Landaverde M, et al.
Neurol 2011;10(9):853-864. doi:10.1016/S1474- Outbreak of poliomyelitis in Hispaniola
4422(11)70170-3 associated with circulating type 1 vaccine-
derived poliovirus. Science 2002;296(5566):
30 Joshi TN, Yamazaki MK, Zhao H, Becker D. Spinal
356-359. doi:10.1126/science.1068284
schistosomiasis: differential diagnosis for acute
paraparesis in a U.S. resident. J Spinal Cord Med 46 Aylward RB, Alwan A. Polio in Syria. Lancet
2010;33(3):256-260. doi:10.1080/10790268. 2014;383(9916):489-491. doi:10.1016/S0140-
2010.11689703 6736(14)60132-X
31 Saleem S, Belal AI, El-Ghandour NM. Spinal cord 47 McLaren N, Lopez A, Kidd S, et al. Characteristics
schistosomiasis: MR imaging appearance with of patients with acute flaccid myelitis, United
surgical and pathologic correlation. AJNR Am J States, 2015-2018. Emerg Infect Dis 2020;26(2):
Neuroradiol 2005;26(7):1646-1654. 212-219. doi:10.3201/eid2602.191453
CONTINUUMJOURNAL.COM 119
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
INFECTIOUS MYELOPATHIES
48 Knoester M, Helfferich J, Poelman R, et al. 63 Ng KS, Abdul Halim S. Anterior spinal cord
Twenty-nine cases of enterovirus-D68-associated syndrome as a rare complication of acute bacterial
acute flaccid myelitis in Europe 2016: a case meningitis in an adult. BMJ Case Rep 2018;2018:
series and epidemiologic overview. Pediatr bcr2018226082. doi:10.1136/bcr-2018-226082
Infect Dis J 2019;38(1):16-21. doi:10.1097/
64 Kleinschmidt-DeMasters BK. Central nervous
INF.0000000000002188
system aspergillosis: a 20-year retrospective
49 Jang S, Suh SI, Ha SM, et al. Enterovirus 71-related series. Hum Pathol 2002;33(1):116-124. doi:10.1053/
encephalomyelitis: usual and unusual magnetic hupa.2002.30186
resonance imaging findings. Neuroradiology
2012;54(3):239-245. doi:10.1007/s00234-011-0921-8 65 Chan CT, Gold WL. Intramedullary abscess of the
spinal cord in the antibiotic era: clinical features,
50 Schubert RD, Hawes IA, Ramachandran PS, et al. microbial etiologies, trends in pathogenesis, and
Pan-viral serology implicates enteroviruses in outcomes. Clin Infect Dis 1998;27(3):619-626.
acute flaccid myelitis. Nat Med 2019;25(11): doi:10.1086/514699
1748-1752. doi:10.1038/s41591-019-0613-1
66 Ulu-Kilic A, Karakas A, Erdem H, et al. Update on
51 Murphy OC, Pardo CA. Acute flaccid myelitis: a treatment options for spinal brucellosis. Clin
clinical review. Semin Neurol 2020;40(2):211-218. Microbiol Infect 2014;20(2):O75-O82.
doi:10.1055/s-0040-1705123 doi:10.1111/1469-0691.12351
52 Ooi MH, Wong SC, Clear D, et al. Adenovirus type 67 Pappas G, Papadimitriou P, Akritidis N, et al. The new
21-associated acute flaccid paralysis during an global map of human brucellosis. Lancet Infect Dis
outbreak of hand-foot-and-mouth disease in 2006;6(2):91-99. doi:10.1016/S1473-3099(06)70382-6
Sarawak, Malaysia. Clin Infect Dis 2003;36(5): 68 Prabhakar MM, Acharya AJ, Modi DR, Jadav B.
550-559. doi:10.1086/367648 Spinal hydatid disease: a case series. J Spinal
Cord Med 2005;28(5):426-431. doi:10.1080/
53 Haddad-Boubaker S, Joffret ML, Pérot P, et al. 10790268.2005.11753843
Metagenomic analysis identifies human
adenovirus 31 in children with acute flaccid 69 Torda AJ, Gottlieb T, Bradbury R. Pyogenic
paralysis in Tunisia. Arch Virol 2019;164(3): vertebral osteomyelitis: analysis of 20 cases and
747-755. doi:10.1007/s00705-018-04141-5 review. Clin Infect Dis 1995;20(2):320-328.
doi:10.1093/clinids/20.2.320
54 Sejvar JJ. West Nile virus infection. Microbiol
Spectr 2016;4(3). doi:10.1128/microbiolspec. 70 Strauss SB, Gordon SR, Burns J, et al.
EI10-0021-2016 Differentiation between tuberculous and
pyogenic spondylodiscitis: the role of the
55 Picheca C, Yogendrakumar V, Brooks JI, et al. anterior meningovertebral ligament in patients
Polio-like manifestation of Powassan virus with anterior epidural abscess. AJNR Am J Neuroradiol
infection with anterior horn cell involvement, 2020;41(2):364-368. doi:10.3174/ajnr.A6370
Canada. Emerg Infect Dis 2019;25(8):1609-1611.
doi:10.3201/eid2508.190399 71 Khanna RK, Malik GM, Rock JP, Rosenblum ML.
Spinal epidural abscess: evaluation of factors
56 Lanciotti RS, Kerst AJ. Nucleic acid influencing outcome. Neurosurgery 1996;39(5):
sequence-based amplification assays for rapid 958-964. doi:10.1097/00006123-199611000-00016
detection of West Nile and St. Louis encephalitis
viruses. J Clin Microbiol 2001;39(12):4506-4513. 72 MRC Working Party on Tuberculosis of the Spine,
doi:10.1128/JCM.39.12.4506-4513.2001 Darbyshire J. Five-year assessment of controlled
trials of short-course chemotherapy regimens of
57 Shi PY, Wong SJ. Serologic diagnosis of West Nile 6, 9 or 18 months' duration for spinal tuberculosis
virus infection. Expert Rev Mol Diagn 2003;3(6): in patients ambulatory from the start or
733-741. doi:10.1586/14737159.3.6.733 undergoing radical surgery. Fourteenth report of
the Medical Research Council Working Party on
58 Goates C, Tsuha S, Working S, et al. Seronegative
Tuberculosis of the Spine. Int Orthop 1999;
West Nile virus infection in a patient treated with
23(2):73-81. doi:10.1007/s002640050311
rituximab for rheumatoid arthritis. Am J Med 2017;
130(6):e257-e258. doi:10.1016/j.amjmed.2017.01.014 73 Marra CM. Neurosyphilis. Continuum (Minneap
59 Jackson AC. Human rabies: a 2016 update. Curr Minn) 2015;21(6 Neuroinfectious Disease):
Infect Dis Rep 2016;18(11):38. doi:10.1007/s11908- 1714-1728. doi:10.1212/CON.0000000000000250
016-0540-y
74 Gavito-Higuera J, Mullins CB, Ramos-Duran L,
60 Zeiler FA, Jackson AC. Critical appraisal of the et al. Fungal infections of the central nervous
Milwaukee protocol for rabies: this failed system: a pictorial review. J Clin Imaging Sci 2016;
approach should be abandoned. Can J Neurol Sci 6:24. doi:10.4103/2156-7514.184244
2016;43(1):44-51. doi:10.1017/cjn.2015.331
75 Garg RK, Malhotra HS, Gupta R. Spinal cord
61 Orme HT, Smith AG, Nagel MA, et al. VZV spinal involvement in tuberculous meningitis. Spinal
cord infarction identified by diffusion-weighted Cord 2015;53(9):649-657. doi:10.1038/sc.2015.58
MRI (DWI). Neurology 2007;69(4):398-400.
doi:10.1212/01.wnl.0000266390.27177.7b 76 Alsina GA, Johnson JP, McBride DQ, et al. Spinal
neurocysticercosis. Neurosurg Focus 2002;12(6):
62 Terry PM, Glancy GR, Graham A. e8. doi:10.3171/foc.2002.12.6.9
Meningovascular syphilis of the spinal cord
presenting with incomplete Brown-Séquard 77 Del Brutto OH. Neurocysticercosis. Handb Clin
syndrome: case report. Genitourin Med 1989; Neurol 2014;121:1445-1459. doi:10.1016/B978-0-
65(3):189-191. doi:10.1136/sti.65.3.189 7020-4088-7.00097-3
120 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Metabolic and Toxic REVIEW ARTICLE
Myelopathies C O N T I N U UM AUDIO
INTERVIEW AVAILABLE
ONLINE
By Natalie Elizabeth Parks, MD
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNrnNdb1tgu/p0M6EMGzm2Aj on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This article describes the clinical presentation, relevant
diagnostic investigations, and treatment of metabolic and toxic myelopathies.
RECENT FINDINGS: Metabolic myelopathies, including those due to deficiency
of vitamin B12, folate, copper, or vitamin E, are preventable and typically
respond to supplementation. In metabolic myelopathy, early recognition
and treatment are important to reduce morbidity, particularly due to
subacute combined degeneration of the spinal cord. Toxic myelopathies,
including those due to medical interventions (eg, methotrexate, radiation),
dietary toxins (eg, lathyrism, konzo), and drugs of abuse (eg, heroin),
typically result in permanent neurologic deficits. Toxic myelopathy due to
CITE AS:
hepatic dysfunction may be reversible if patients receive early CONTINUUM (MINNEAP MINN)
intervention, whereas nitrous oxide myelopathy responds to vitamin B12 2021;27(1, SPINAL CORD DISORDERS):
143–162.
replacement and cessation of exposure. In toxic myelopathy, it is best to
avoid the provoking factor when possible or attempt to mitigate risk by
Address correspondence to
identifying risk factors for developing myelopathy. Dr Natalie Elizabeth Parks,
Division of Neurology, Rm 3832,
1796 Summer St, Halifax, NS,
SUMMARY: Metabolic and toxic myelopathies are important causes of
Canada B3H 3A7,
morbidity that require a high index of suspicion for diagnosis. nparks@dal.ca.
RELATIONSHIP DISCLOSURE:
Dr Parks has served as an
INTRODUCTION advisory board member/
I
t is important for clinicians to recognize metabolic and toxic myelopathies, as consultant for Biogen; EMD
Serono, Inc; F. Hoffmann-
almost all are preventable or treatable. Accurate diagnosis relies on a complete La Roche Ltd; Novartis AG;
neurologic history and neurologic examination accompanied by relevant and Sanofi Genzyme. Dr Parks
has received personal
diagnostic investigations, including MRI of the spinal cord. Metabolic compensation for speaking
myelopathies typically have an insidious onset and a chronic progressive engagements from Biogen and
course, whereas toxic myelopathies have a more variable time course. Accurate Bristol Myers Squibb and
research/grant support from
diagnosis relies on symptom recognition in the appropriate context, such as living Biogen, MedDay
in an endemic area, dietary habits, recreational drug use, and medical comorbidities. Pharmaceuticals, Novartis AG,
and Sanofi Genzyme.
METABOLIC MYELOPATHIES UNLABELED USE OF
PRODUCTS/INVESTIGATIONAL
Metabolic myelopathies, including those due to deficiency of vitamin B12, folate, USE DISCLOSURE:
copper, or vitamin E, are preventable and typically respond to supplementation Dr Parks discusses the
(TABLE 6-1). unlabeled/investigational use of
bevacizumab for the treatment
of radiation myelopathy.
Vitamin B12 Deficiency
The prevalence of vitamin B12 (cobalamin) deficiency varies by geographic © 2021 American Academy
location, with higher prevalence in socioeconomically disadvantaged regions.1 In of Neurology.
CONTINUUMJOURNAL.COM 143
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
high-income countries, an association is seen between vitamin B12 deficiency and
advanced age, with 6% of individuals 70 years of age or older in the United States
and 10% of individuals 75 years of age or older in the United Kingdom having
vitamin B12 deficiency. Among those with vitamin B12 deficiency and neurologic
symptoms, approximately 50% experience myelopathy symptoms either alone or
in combination with peripheral neuropathy (myeloneuropathy).2
The term subacute combined degeneration of the spinal cord is used to describe
the myelopathy accompanying vitamin B12 deficiency to emphasize the posterior
(dorsal) and lateral column damage encountered clinically and pathologically
(FIGURE 6-1).3,4 Initially, swelling of the myelin sheath is seen, followed by
myelin breakdown with infiltration of macrophages. Over time, gliosis with
axonal degeneration ensues.
Symptoms resulting from myelopathy due to vitamin B12 deficiency typically
begin with the insidious onset of paresthesia and gait difficulty because of dorsal
column dysfunction.2,5 Individuals often describe difficulty maintaining balance
TABLE 6-1 Metabolic Myelopathies
Nutrient
deficiency Etiologies Symptoms/signs MRI Diagnostic tests Treatment
Vitamin B12 Vegetarian diet, Subacute T2 Serum cobalamin: low Cyanocobalamin
pernicious anemia, combined hyperintensity 1000 mcg IM or
Plasma methylmalonic
stomach/small bowel degeneration of in posterior subcutaneous
acid: high
surgery, Crohn disease, spinal cord columns with daily for 5 days
gastritis, medications beginning with inverted V sign; Plasma homocysteine: followed by
(H2 blockers, proton paresthesia and may extend high 1000 mcg IM or
pump inhibitors, sensory ataxia over several subcutaneous
Complete blood cell
metformin, colchicine), (positive Romberg levels in monthly
count: macrocytic
tapeworm, nitrous sign, cervical or indefinitely;
anemia,
oxide pseudoathetosis) thoracic cord; 1000 mcg orally
hypersegmented
followed by rarely daily is a possible
neutrophils
pyramidal gadolinium alternative
symptoms and enhancement Intrinsic factor chronic regimen
signs; frequent antibodies: high
mixture of central specificity, low
and peripheral sensitivity for
sensory and motor pernicious anemia
signs due to among those with
coexisting vitamin B12 deficiency
peripheral axonal
neuropathy; may
be associated with
optic neuropathy
and cognitive
impairment
CONTINUED ON PAGE 145
144 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
when visual input is removed (eg, in darkness or when eyes are closed).
Neurologic examination reveals diminished vibration/proprioception that may
be accompanied by a wide-based unsteady gait from sensory ataxia and a positive
Romberg test. In addition, patients may have lower limb greater than upper limb
weakness that is often associated with upper motor neuron signs, including
spasticity, hyperreflexia, and upgoing plantar responses. Peripheral neuropathy
frequently occurs with myelopathy due to vitamin B12 deficiency, causing a
mixed picture of peripheral and central patterns of sensory and motor signs. In
addition, optic neuropathy and cognitive dysfunction are recognized
accompaniments. Patients may have an associated megaloblastic anemia,
although neurologic symptoms may occur before the development of
hematologic abnormalities.
Vitamin B12 is present in many animal proteins, such as meat, eggs, and milk,
but is not found in plants. Today, many foods are fortified with vitamin B12.
Vitamin B12 undergoes several steps in the digestive process to enable successful
CONTINUED FROM PAGE 144
Nutrient
deficiency Etiologies Symptoms/signs MRI Diagnostic tests Treatment
Folic acid Alcoholism, small Same as vitamin B12 Same as vitamin Serum folate: low Folic acid 3 mg
bowel surgery, celiac deficiency B12 deficiency; orally daily until
Red blood cell folate:
disease, inflammatory no reports of hematologic
low
bowel disease, gadolinium parameters
medications enhancement Plasma homocysteine: normalize and
(methotrexate, high then folic acid
pyrimethamine, 1 mg orally daily
Complete blood cell
trimethoprim,
count: macrocytic
sulfasalazine)
anemia,
hypersegmented
neutrophils
Copper Bariatric surgery, partial Same as vitamin B12 Same as vitamin Serum copper: low Copper 2-4 mg
gastrectomy, zinc deficiency B12 deficiency; orally daily with
Serum ceruloplasmin:
excess (supplements, no reports of repeat serum
low
denture cream), celiac gadolinium copper to adjust
disease, Menkes enhancement Complete blood cell dose; avoid zinc
disease count: anemia,
leukopenia
Assess serum zinc and
celiac serology
Vitamin E Cystic fibrosis, Sensory ataxia No Plasma α-tocopherol: Vitamin E
cholestatic liver with absent characteristic low 300-1000 mg
disease, small bowel reflexes and spinal cord orally daily
Consider genetic
surgery, upgoing plantar findings; MRI
testing (cystic fibrosis,
abetalipoproteinemia, responses, with or brain may
abetalipoproteinemia,
ataxia with vitamin E without demonstrate
ataxia with vitamin E
deficiency pigmentary mild cerebellar
deficiency)
retinopathy atrophy
IM = intramuscular; MRI = magnetic resonance imaging.
CONTINUUMJOURNAL.COM 145
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
absorption (FIGURE 6-2).6
Vitamin B12 is cleaved from
animal protein by gastric acid
secreted by gastric parietal cells
and becomes bound to intrinsic
factor secreted by gastric parietal
cells while both are passing
through the duodenum. Vitamin
B12 bound to intrinsic factor is
absorbed in the ileum. Only 1%
of vitamin B12 is absorbed as free
FIGURE 6-1 vitamin B12, independent of
Subacute combined degeneration with intrinsic factor. Absorbed
demyelination of the posterior and lateral
vitamin B12 becomes bound to
columns of the spinal cord.
Figure courtesy of Agamanolis DP, Neuropathology-web.org.3 transcobalamin II, which delivers
vitamin B12 to body tissues.
FIGURE 6-2
Vitamin B12 absorption. Vitamin B12 binds to intrinsic factor secreted by gastric parietal cells
while in the duodenum. Vitamin B12 bound to intrinsic factor is absorbed in the ileum.
Absorbed vitamin B12 binds to transcobalamin II for systemic transport.
Reprinted with permission from Oh R, Brown DL, Am Fam Physician.6 © 2003 American Academy of
Family Physicians.
146 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Vitamin B12 is an essential cofactor in the conversion of homocysteine to KEY POINTS
methionine, methylmalonic acid to succinyl-coenzyme A, and
● Vitamin B12 deficiency
methyltetrahydrofolate to tetrahydrofolate (FIGURE 6-3).7 These reactions are is common among
necessary for DNA synthesis, myelin synthesis, and the Krebs cycle, all of which older adults.
contribute to nervous system function.
Vitamin B12 deficiency may arise from reduced intake, inadequate absorption, ● Subacute combined
degeneration of the spinal
or abnormal metabolism.8 A diet low in vitamin B12 may result from eating
cord presents with posterior
exclusively plant-based food (ie, a vegan diet). A disruption in the absorption column dysfunction
process may also result in vitamin B12 deficiency. This disruption may be because (reduced vibration/
of surgery on the stomach or small bowel (eg, gastric bypass weight loss surgery). proprioception) along
Pernicious anemia is an autoimmune disease that affects parietal cells, which with variable severity of
lateral column dysfunction
secrete gastric acid and intrinsic factor needed for vitamin B12 absorption. Gastritis (upper motor neuron signs).
caused by Helicobacter pylori also reduces parietal cell secretions. Crohn disease
may preferentially affect the terminal ileum, reducing absorption. Medications
such as histamine-2 receptor antagonists and proton pump inhibitors result in more
alkaline gastric juices, reducing vitamin B12 breakdown by gastric acid. Additional
medications linked to vitamin B12 deficiency include metformin, colchicine, and
cholestyramine. Parasitic infection by the tapeworm Diphyllobothrium latum may
interfere with absorption of vitamin B12 in the terminal ileum. Nitrous oxide may
also affect vitamin B12 function, as discussed below.
The diagnosis of vitamin B12 deficiency is challenging because no gold
standard test has been established9; thus, it is important to interpret laboratory
FIGURE 6-3
Vitamin B12 biochemistry. Vitamin B12 is an essential cofactor in the conversion of
homocysteine to methionine, methylmalonic acid to succinyl-coenzyme A, and
methyltetrahydrofolate to tetrahydrofolate. These reactions are necessary for myelin
production, DNA synthesis, and the Krebs cycle, all of which contribute to nervous system
function. Nitrous oxide causes inactivation of vitamin B12, interfering with the ability of
methionine synthase to convert homocysteine to methionine or methyltetrahydrofolate
to tetrahydrofolate.
ATP = adenosine triphosphate; FADH2 = flavin adenine dinucleotide; NADH = nicotinamide adenine
dinucleotide.
CONTINUUMJOURNAL.COM 147
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
results in the context of clinical symptoms. Serum cobalamin is the standard
initial diagnostic test.9 In vitamin B12 deficiency, serum cobalamin may be low,
but it may also be in the borderline or normal range10,11; plasma methylmalonic
acid and homocysteine are particularly useful in this situation to help confirm
cellular vitamin B12 deficiency. Methylmalonic acid or homocysteine may be elevated
in vitamin B12 deficiency as vitamin B12 acts as a cofactor in the reaction needed to
metabolize these compounds. Elevation of methylmalonic acid is more specific than
elevation of homocysteine, which is also seen in other vitamin deficiencies,
including folate (vitamin B9) and pyridoxine (vitamin B6).9 Elevated methylmalonic
acid may also occur if a patient has renal insufficiency or methylmalonic acidemia.12
Elevated homocysteine may occur in renal insufficiency or homocystinuria.
MRI of the spinal cord in patients with vitamin B12 deficiency may
demonstrate T2 hyperintensity in the posterior or lateral columns (FIGURE 6-413).
Imaging changes typically occur contiguously over several segments in the
cervical or upper thoracic spinal cord. The appearance may resemble an
inverted V (or inverted rabbit ears) in the posterior columns on axial images
(FIGURE 6-4).5,13 The T2 signal change is only rarely accompanied by contrast
enhancement. Imaging findings often improve with adequate treatment.5,14
A number of additional investigations may be considered. Nerve conduction
studies and EMG may be performed to investigate for evidence of a peripheral
neuropathy, with a length-dependent axonal pattern typically encountered.
Visual evoked potentials may demonstrate evidence of optic neuropathy. A
complete blood cell count and peripheral blood smear may demonstrate
macrocytic anemia with hypersegmented neutrophils. Anti–intrinsic factor
antibody has high specificity but low sensitivity for identifying pernicious
FIGURE 6-4
Subacute combined degeneration due to vitamin B12 deficiency. Axial (A) and sagittal (B)
T2-weighted images of the spinal cord show hyperintensity in the posterior columns
affecting the thoracic spinal cord on sagittal image (B), with an inverted V appearance on
axial image (A, arrow).
Reprinted with permission from Matsuura H, Nakamura T, QJM.13 © 2017 Oxford University Press.
148 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
anemia among those with vitamin B12 deficiency,9 whereas anti–parietal cell KEY POINTS
antibody and elevated gastrin are not specific for pernicious anemia. The
● Vitamin B12 deficiency
Schilling test for pernicious anemia is no longer used in clinical practice.12 may be present despite
The treatment for vitamin B12 deficiency is vitamin B12 replacement, although serum cobalamin within the
no standard protocol has been established.12 Injected vitamin B12 is commonly normal range, although
cyanocobalamin in North America and hydroxocobalamin in Europe. British plasma methylmalonic acid
or plasma homocysteine, or
guidelines recommend that for cases of vitamin B12 deficiency with neurologic
both, may be elevated.
involvement, IM hydroxocobalamin 1000 mcg be given every 2 days
with reassessment after 3 weeks, followed by a maintenance dose of IM ● The treatment for
hydroxocobalamin 1000 mcg every 2 months.9 Another reasonable approach subacute combined
for vitamin B12 deficiency causing myelopathy is IM or subcutaneous degeneration of the spinal
cord due to vitamin B12
cyanocobalamin 1000 mcg/d for 5 days followed by a maintenance dose of IM or deficiency is IM or
subcutaneous cyanocobalamin 1000 mcg once per month.15 Replacement is subcutaneous
recommended indefinitely for subacute combined degeneration of the spinal cyanocobalamin 1000 mcg/d
cord.11 Low-quality evidence suggests that oral and IM vitamin B12 result in for 5 days followed by
1000 mcg once per month.
similar serum vitamin B12 levels.16 As a result, it may be reasonable to continue
maintenance therapy with 1000 mcg vitamin B12 given orally every day after ● Vitamin B12 replacement
initial parenteral replacement as an alternative. should be given indefinitely
Symptomatic and imaging improvement of subacute combined degeneration following subacute
combined degeneration of
of the spinal cord are often seen after supplementation, particularly if patients
the spinal cord due to
receive early diagnosis and treatment.14 vitamin B12 deficiency.
NITROUS OXIDE. Nitrous oxide (laughing gas) is an anesthetic gas used in surgical and ● Nitrous oxide causes
dental procedures. In addition, it is used in aerosol cans that dispense whipped inactivation of vitamin B12,
which may result in subacute
cream; inhaling nitrous oxide from these aerosol devices is called “doing whippets.”
combined degeneration of
Nitrous oxide has been exploited as a recreational drug as it causes euphoria. the spinal cord.
Nitrous oxide causes irreversible inactivation of vitamin B12, resulting in an
identical clinical presentation to that of vitamin B12 deficiency. Nitrous oxide ● Folate deficiency is
results in oxidation of the cobalt center of methylcobalamin from monovalent to uncommon since the
introduction of national
bivalent and trivalent forms.7 This inactivated form of vitamin B12 cannot be fortification programs aimed
used by methionine synthase to convert homocysteine to methionine or at improving folate levels
methyltetrahydrofolate to tetrahydrofolate (FIGURE 6-3), which results in among reproductive-age
interference with DNA and myelin synthesis. women to reduce neural
tube defects in their
The subacute combined degeneration of the spinal cord associated with offspring.
nitrous oxide toxicity is clinically and radiographically identical to vitamin B12
deficiency.17,18 Subacute combined degeneration of the spinal cord may result
from relatively brief exposure to nitrous oxide during routine surgical
procedures in as little as 30 minutes (CASE 6-1).19 Subacute combined
degeneration of the spinal cord may also be caused by habitual recreational
exposure to nitrous oxide from whippets.20
The diagnosis of nitrous oxide myelopathy requires a high index of suspicion
as no single diagnostic test has been established. Among those with nitrous oxide
toxicity, serum cobalamin level is low in approximately 70%, whereas plasma
methylmalonic acid or plasma homocysteine, or both, are elevated in more than
90%.17 Nitrous oxide toxicity is treated with vitamin B12 supplementation and
cessation of nitrous oxide use.20
Folate Deficiency
Folate deficiency is encountered much less frequently since national fortification
programs resulted in an increase in dietary folate.21 Folate fortification was
CONTINUUMJOURNAL.COM 149
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
introduced in many countries, including the United States and Canada, because
of a strong association between folate deficiency among reproductive-age women
and neural tube defects in their offspring. In adults, the neurologic complications
of folate (vitamin B9) deficiency include myelopathy, peripheral neuropathy,
optic neuropathy, and cognitive dysfunction.22,23 Neurologic manifestations of
folate deficiency (including myelopathy) are rare, and the myelopathy takes the
form of a subacute combined degeneration of the spinal cord.22,24,25
CASE 6-1 A 78-year-old woman underwent extraction of a painful broken tooth.
During the procedure, she received nitrous oxide anesthetic gas.
Approximately 2 days after the procedure, she began to note difficulty
walking in low lighting, with the need to hold on to the wall. Over the next
several weeks, she began to experience tingling in her feet and then her
hands. Her past medical history included hypertension and atrophic
gastritis due to Helicobacter pylori infection. She had lost 9 kg (20 lb)
over the previous 2 years because of reduced dietary intake since her
husband died and, more recently, because of dental pain.
Approximately 2 months after the dental procedure, neurologic
examination was remarkable for absent vibration distal to the tibial
tuberosity, diminished proprioception at the great toes, reduced ankle
jerks, bilateral extensor plantar responses, and positive Romberg sign.
MRI of her spinal cord demonstrated T2 hyperintensity in the posterior
columns extending from C2 to C6, with an inverted V configuration. MRI
of her brain demonstrated nonspecific T2 hyperintensities, most in
keeping with chronic small vessel ischemia. Nerve conduction studies
demonstrated a length-dependent axonal neuropathy affecting the
lower extremities to a greater extent than the upper extremities. A
complete blood cell count demonstrated macrocytic anemia, and her
serum cobalamin was 103 ng/L (lower limit of normal 150 ng/L) and plasma
methylmalonic acid was 0.7 nmol/mL (upper limit of normal 0.4 nmol/mL).
She was diagnosed with vitamin B12 deficiency unmasked following
exposure to nitrous oxide during a dental procedure and was treated with
IM cyanocobalamin 1000 mcg/d for 5 days followed by maintenance
therapy of IM cyanocobalamin 1000 mcg once per month. Over the next
2 months, she experienced improvement in paresthesia and improved
stability while walking. She was advised to continue with IM
cyanocobalamin 1000 mcg once per month indefinitely.
COMMENT The patient in this case had multiple risk factors for vitamin B12 deficiency,
including age older than 70 years, a diet low in animal protein, and atrophic
gastritis secondary to H. pylori. The neurologic examination features were
consistent with involvement of the dorsal and lateral columns (subacute
combined degeneration of the spinal cord). Parenteral (subcutaneous or
IM) cyanocobalamin is recommended to treat vitamin B12 deficiency with
neurologic manifestations.
150 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Folate is naturally found in dark green vegetables, legumes, and liver. In many KEY POINTS
countries, foods such as white flour are fortified with folate. Folate is absorbed
● Serum folate level
primarily in the jejunum.23 The active form of folate is tetrahydrofolate; folate reflects recent folate intake,
may be converted to dihydrofolate then tetrahydrofolate by dihydrofolate whereas red blood cell
reductase. In addition, 5-methyltetrahydrofolate, formed in the enterocyte, is folate level reflects intake
demethylated to tetrahydrofolate by methionine synthase. The methionine over approximately the past
3 months.
synthase reaction also uses cobalamin to convert homocysteine to methionine.
Tetrahydrofolate is required in nucleic acid synthesis for DNA (FIGURE 6-3).7 ● Copper deficiency is an
Folate deficiency may result from inadequate intake, inadequate absorption, underrecognized cause of
or abnormal metabolism.23 Low dietary intake may result from cooking food (as subacute combined
folate is destroyed by heat) or alcohol use disorder. Impaired absorption in the degeneration of the spinal
cord.
jejunum may be secondary to surgery, celiac disease, or inflammatory bowel
disease. Sulfasalazine impairs folate absorption by acting as a noncompetitive
inhibitor of the reduced folate carrier. A number of medications are
dihydrofolate reductase inhibitors, including methotrexate, pyrimethamine, and
trimethoprim, leading to impaired folate metabolism. The requirement for folate
is increased during pregnancy and in states with increased cell turnover,
including malignancy, hemolytic anemia, and psoriasis.
The diagnosis of folate deficiency should include serum folate level, which
reflects recent intake, as an initial test.9 Red blood cell folate, which reflects
intake over the past 3 months, may be performed if serum folate is normal.
Plasma homocysteine may also be tested, as folate is needed for the conversion of
homocysteine to methionine by methionine synthase. Elevated homocysteine
may be consistent with folate deficiency, although elevated homocysteine may
be seen in other conditions, including vitamin B12 deficiency. Abnormalities on
MRI, electrophysiology, and complete blood cell count are identical to those seen
in vitamin B12 deficiency discussed above.25
The treatment for folate deficiency is folate replacement, although no
standard treatment protocol has been established. British guidelines recommend
folic acid 5 mg/d for at least 4 months in the presence of megaloblastic anemia.9
Another reasonable approach for folate deficiency is folic acid 1 mg 3 times a day
until hematologic abnormalities normalize, followed by folic acid 1 mg/d.26 Folic
acid replacement is typically oral, although parenteral administration may be
considered in patients who are acutely ill.
Subacute combined degeneration of the spinal cord due to folate deficiency
often shows symptomatic improvement with folic acid replacement, particularly
with early diagnosis and treatment of the deficiency.22,24
Copper Deficiency
Copper deficiency is an underrecognized cause of myelopathy that mimics
vitamin B12 deficiency. The prevalence of copper deficiency is as high as 10% in
individuals having undergone bariatric surgery with a Roux-en-Y gastric
bypass.27 The best characterized neurologic complication is myelopathy with or
without neuropathy (CASE 6-2).
Copper deficiency myelopathy is almost identical to the subacute combined
degeneration of the spinal cord encountered with vitamin B12 deficiency, often
resulting in sensory ataxia and spasticity.28,29 An associated length-dependent
axonal peripheral neuropathy is frequently seen. Additional neurologic
manifestations that may be associated with copper deficiency are isolated
peripheral neuropathy, optic neuropathy, and cognitive dysfunction.
CONTINUUMJOURNAL.COM 151
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
Copper is absorbed in the stomach and proximal duodenum28,29 and is
transported into enterocytes by copper transporter protein-1 before transport
from enterocytes into the portal circulation by ATP7A. A number of enzymes use
copper as a cofactor, including cytochrome c oxidase in the mitochondrial
electron transport chain. Copper is transported out of the liver to systemic tissues
bound to ceruloplasmin.
Copper deficiency may be caused by inadequate intake or decreased
absorption. Copper is found in high amounts in shellfish, organ meat, nuts, and
beans. The most common cause of copper deficiency myelopathy is decreased
absorption following gastrointestinal surgery (eg, Roux-en-Y gastric bypass),
accounting for approximately 50% of cases, but celiac disease and excessive zinc
consumption as a supplement or in denture cream are other common
etiologies.28,29 Zinc upregulates metallothionein, a chelator in enterocytes that
has a higher affinity for copper than for zinc. Copper bound to the chelator
remains in the enterocytes until enterocytes are shed and excreted in feces.
Menkes disease is a genetic form of copper deficiency due to reduced copper
absorption from a mutation in ATP7A.
CASE 6-2 A 56-year-old man presented with a 3-year history of gradually increasing
difficulty with balance while walking and numbness that began in his feet
and gradually ascended to the knees. Over the previous year, he had
started to note paresthesia in his fingers. His past medical history was
remarkable for a Roux-en-Y gastric bypass at age 49 for medically
complicated obesity.
Neurologic examination was remarkable for absent vibration distal to
the tibial tuberosity, diminished proprioception at the great toes, brisk
reflexes, wide-based gait, and positive Romberg sign. MRI of the spinal
cord demonstrated T2 hyperintensity in the posterior columns extending
from C3 to C6, with an inverted V configuration. MRI of his brain was
normal. Nerve conduction studies were normal. A complete blood cell
count was also normal, as were serum cobalamin, serum folate, and
plasma methylmalonic acid levels. Serum copper was 8.7 µmol/L (lower
limit of normal 11.2 µmol/L), and serum ceruloplasmin was 54 mg/L (lower
limit of normal 232 mg/L); serum zinc was normal.
He was diagnosed with copper deficiency myelopathy resulting from
decreased copper absorption following bariatric surgery and was treated
with oral copper 2 mg/d for 3 months, with improvement in balance and
paresthesia. At 3 months, a repeat serum copper level was normal. He
was advised to continue with oral copper 2 mg/d indefinitely.
COMMENT Copper deficiency myelopathy mimics the subacute combined
degeneration of the spinal cord encountered with vitamin B12 deficiency
both clinically and radiologically. Gastric bypass surgery is a recognized risk
factor for both vitamin B12 deficiency–associated and copper deficiency–
associated myelopathies. Low serum copper can confirm the diagnosis,
and oral supplementation can lead to improvement in neurologic function.
152 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Measurement of serum copper is the diagnostic test of choice for copper KEY POINTS
deficiency; low copper levels may be accompanied by low ceruloplasmin.29
● Copper deficiency may
Evaluating serum zinc level may help identify the cause of copper deficiency, and be caused by bariatric
assessing for celiac disease is also useful. surgery, celiac disease, or
MRI of the spinal cord demonstrates features in keeping with subacute excessive zinc intake as a
combined degeneration of the spinal cord.28,29 Approximately 50% of cases of supplement or in denture
cream.
copper deficiency myelopathy demonstrate T2 hyperintensity in the posterior
region of the cervical or thoracic spinal cord, or both, without contrast ● Serum copper and serum
enhancement. ceruloplasmin levels are
Nerve conduction studies and EMG may demonstrate evidence of a typically low in copper
length-dependent axonal polyneuropathy.28 A complete blood cell count often deficiency.
reveals anemia or leukopenia, or both. ● Vitamin E deficiency that
The treatment for copper deficiency is copper replacement, although no results in spinocerebellar
standard treatment protocol has been established.28 Typically, copper deficiency ataxia is an increased risk
myelopathy is treated with the equivalent of elemental copper 2 mg/d to 4 mg/d, among those with impaired
fat absorption from
although higher doses are sometimes required.29 Copper is usually administered disorders such as cystic
orally but may be given intravenously. It may be necessary to administer copper fibrosis and rare genetic
indefinitely depending on the underlying cause of copper deficiency. In the case conditions, including ataxia
of copper deficiency due to zinc supplementation, it is important to avoid zinc with vitamin E deficiency
and abetalipoproteinemia.
consumption. Stabilization or partial improvement of symptoms due to copper
deficiency myelopathy often occurs following copper replacement.29
Vitamin E Deficiency
Vitamin E deficiency is rare in the general population of developed countries
such as the United States.30 Specific populations, including those with cystic
fibrosis, are at increased risk of vitamin E deficiency with a clinical phenotype
similar to Friedreich ataxia, including ataxia, reduced proprioception, absent
reflexes, and upgoing plantar responses.31 Pathology demonstrates degeneration
of the posterior columns with accumulation of lipofuscin in the dorsal root
ganglia.32
Vitamin E is a fat-soluble vitamin absorbed in the small intestine primarily as
α-tocopherol. Vitamin E is absorbed bound to bile salt, which is part of a micelle
composed of fatty acids. Fatty acids are formed from the breakdown of lipids by
pancreatic lipase. In the enterocyte, vitamin E is incorporated into a chylomicron
for transportation to the liver. Vitamin E is then transported from the liver in
very-low-density lipoprotein (VLDL) particles that become low-density
lipoprotein (LDL) particles that are absorbed by body tissues.
Vitamin E deficiency may be caused by inadequate intake, decreased
absorption, or impaired metabolism.30 Vitamin E is found in high amounts in
green vegetables and nuts. Decreased absorption occurs in cholestatic liver
disease, cystic fibrosis, and extensive resection of the small intestine. In
cholestatic liver disease, the production of bile salts that are needed for vitamin E
absorption is impaired. In cystic fibrosis, fat absorption is decreased because of
thickened pancreatic secretions interfering with pancreatic lipase function.
Genetic conditions, including ataxia with vitamin E deficiency (AVED) and
abetalipoproteinemia, interfere with vitamin E metabolism. AVED is the result of
a mutation in α-tocopherol transfer protein, which is needed to incorporate
vitamin E into VLDL for transport out of the liver.33 Abetalipoproteinemia is the
result of a mutation in microsomal triglyceride transfer protein, resulting in
impaired formation of chylomicra, VLDL, and LDL.
CONTINUUMJOURNAL.COM 153
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
The diagnosis of vitamin E deficiency should include obtaining the patient’s
plasma α-tocopherol level. Plasma vitamin E in the low range is supportive of
vitamin E deficiency. A lipid profile demonstrating absent or very low LDL is
supportive of abetalipoproteinemia. Genetic testing for inherited conditions
associated with vitamin E should be considered, including AVED,
abetalipoproteinemia, and cystic fibrosis.
CT or MRI of the brain may demonstrate mild cerebellar atrophy.31,33 No
imaging findings are characteristic of myelopathy secondary to vitamin E
deficiency, with MRI of the spinal cord reported as normal.31
Eye examination may reveal pigmentary retinopathy in genetic disorders such
as abetalipoproteinemia and AVED. Nerve conduction studies and EMG may
demonstrate mild axonal sensorimotor neuropathy.31
The treatment for vitamin E deficiency is vitamin E replacement. Vitamin E
replacement is typically provided by oral supplementation, although parenteral
forms are available. Vitamin E supplementation in some studies of AVED ranged
from 300 mg/d to 2400 mg/d, with some individuals experiencing symptom
stabilization, whereas others experienced ongoing neurologic deterioration.31,33
In cystic fibrosis, vitamin E 100 mg/d is sufficient to prevent vitamin E
deficiency in most individuals.34
TOXIC MYELOPATHIES
Toxic myelopathies often result in permanent neurologic deficits. If avoidance of
the provoking factor is not possible, identifying risk factors for developing
myelopathy may be helpful in creating a risk-mitigation strategy (TABLE 6-2).
Dietary Toxicity
Neurolathyrism is a toxic myelopathy that occurs in populations in which
diet consists largely of grass peas (Lathyrus sativus), red chickling vetch
(Lathyrus cicera), or purple Spanish vetchling (Lathyrus clymenum).35 Cases of
neurolathyrism have been reported in Europe, Asia, and Africa. Lathyrus species
are hearty plants that grow in conditions unfavorable to other crops, leading
to preferential consumption in socioeconomically disadvantaged populations,
particularly during famine. Risk factors for neurolathyrism include malnutrition,
male sex, and physical exertion.36 These plants contain the neurotoxin
β-N-oxalyl-L-α,β-diaminopropionic acid (ODAP). ODAP is a glutamate receptor
agonist, leading to glutamate toxicity in the central nervous system, particularly
in the longest axons in the corticospinal tract.36 Pathology demonstrates
degeneration of the lateral and ventral corticospinal tracts. Neurolathyrism
results in spastic paraparesis that develops over a variable period of time ranging
from acute (hours) to subacute (10 to 15 days) to chronic (months), with acute
onset being the most common.36,37 Typically, patients have upper motor neuron
findings with preserved sensation and sphincter function. The severity of
neurolathyrism is graded based on the patient’s ability to ambulate. Spasticity is
often out of proportion to weakness, and the upper extremities are rarely
affected. Diagnosis is based on history of exposure, clinical features, and
exclusion of alternative causes. MRIs of the brain and spinal cord of a limited
number of affected individuals were unremarkable.38 Treatment of
neurolathyrism includes discontinuing Lathyrus consumption. After the
discontinuation of Lathyrus consumption, symptoms typically stabilize, although
neurologic deficits are often permanent.
154 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Konzo is a toxic myelopathy that occurs in populations in which diet consists KEY POINTS
largely of bitter cassava (Manihot esculenta Crantz), which contains cyanogens
● Grass peas (Lathyrus
that result in cyanide toxicity.39 Cassava is a hearty plant that grows in sativus) contain a neurotoxin
sub-Saharan Africa in conditions that are unfavorable for other crops. Risk that may result in
factors for konzo include malnutrition and female sex. Detoxification through neurolathyrism manifesting
the wetting method (in which cassava flour is mixed with water then spread in a with acute-onset spastic
paraparesis.
thin layer to dry) reduces cyanogens by allowing the escape of hydrogen cyanide
gas.40 Konzo results in spastic paraparesis with acute or subacute (<1 week) ● Bitter cassava contains
onset, often following physical exertion.39 Typically, upper motor neuron cyanogens that may cause
findings are seen, with preserved sensation and sphincter function. The most konzo, manifesting with
spastic paraparesis, due to
prominent symptom is often a spastic gait. The severity of konzo is graded based
cyanide toxicity.
on the patient’s ability to ambulate. The upper extremities are rarely affected.
Sometimes, a bilateral optic neuropathy is seen. Diagnosis is based on history of ● Subacute combined
exposure, clinical features, and exclusion of alternative causes. Exposure to degeneration of the spinal
cyanogens may be estimated by measuring urine or plasma thiocyanate, a cord may occur with
intrathecal methotrexate,
cyanide metabolite.39 MRIs of the brain and spinal cord of a limited number of which is a folate antagonist.
affected individuals were unremarkable.41 Treatment includes limiting further
consumption of cyanogens by using the wetting method for cassava preparation ● Tumor necrosis factor-α
or discontinuing consumption of bitter cassava.40 Following avoidance of inhibitors and immune
checkpoint inhibitors are
cyanogens, symptoms stabilize, although neurologic deficits are typically
associated with transverse
permanent.39 myelitis.
Medication Toxicity
Methotrexate is a chemotherapy drug that acts as a folate antagonist by inhibiting
dihydrofolate reductase. Methotrexate administered intrathecally has been
associated with myelopathy presenting as subacute combined degeneration of
the spinal cord (CASE 6-3).42,43 Methotrexate toxicity is an increased risk among
individuals with C667T polymorphism in the gene for methylenetetrahydrofolate
reductase (MTHFR), which may also contribute to an increased risk of
methotrexate myelopathy.44 Additional risk factors include higher total
intrathecal methotrexate exposure, systemic methotrexate, radiation therapy,
and hematologic malignancy affecting the brain or spinal cord.42 Neurologic
examination demonstrates features in keeping with subacute combined
degeneration of the spinal cord.43 Diagnosis is based on exposure to intrathecal
methotrexate and may be supported by low serum folate and elevated plasma
homocysteine. MRI of the spinal cord demonstrates T2 signal abnormalities in
the dorsal and lateral columns consistent with subacute combined degeneration
of the spinal cord. Treatment of methotrexate myelopathy includes folate
supplementation and discontinuation of methotrexate.25 Methotrexate
myelopathy often results in permanent neurologic deficits with poor
prognosis.25,42,43
Tumor necrosis factor-α (TNF-α) inhibitors and immune checkpoint
inhibitors are associated with transverse myelitis.45-47 TNF-α inhibitors
(eg, adalimumab, etanercept, infliximab) bind to the cytokine TNF to inhibit
binding to TNF receptors for the treatment of rheumatologic conditions
(eg, rheumatoid arthritis) and inflammatory bowel disease (eg, Crohn disease).
TNF-α inhibitors are associated with demyelinating disease, including rare cases
of isolated myelitis.45 Immune checkpoint inhibitors upregulate the activity
of T cells by blocking targets such as anti–programmed cell death 1 (PD1)
(eg, nivolumab) and anti–cytotoxic T-lymphocyte associated protein 4 (CTLA4)
CONTINUUMJOURNAL.COM 155
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
TABLE 6-2 Toxic Myelopathies
Diagnostic
Toxin Etiology Symptoms/signs MRI tests Treatment
Nitrous oxide Inactivation of Subacute combined T2 Low serum IM or subcutaneous
vitamin B12 by degeneration of hyperintensity in cobalamin, cyanocobalamin
nitrous oxide used spinal cord beginning posterior high plasma 1000 mcg/d for
as anesthetic gas with sensory ataxia columns with methylmalonic 5 days followed by IM
or whippets (positive Romberg inverted V sign; acid, high or subcutaneous
(recreational use sign, pseudoathetosis) may extend over plasma 1000 mcg monthly
of aerosol used in followed by pyramidal several levels in homocysteine indefinitely;
dispensing symptoms and signs, cervical or 1000 mcg/d orally is a
whipped cream) with or without thoracic cord possible alternative
peripheral axonal chronic regimen;
neuropathy avoid nitrous oxide
Neurolathyrism Diet largely Spastic paraparesis MRI spinal cord, Diagnosis relies Improved nutrition;
caused by consisting of grass typically developing no specific on history of avoid consumption
neurotoxin β-N- pea (Lathyrus over hours findings exposure along of Lathyrus plants
oxalyl-L-α,β- sativus), red with exclusion
diaminopropionic chickling vetch of other causes
acid (Lathyrus cicera) or
purple Spanish
vetchling (Lathyrus
clymenum)
Konzo caused by Diet largely Spastic paraparesis MRI spinal cord, Diagnosis relies Improved nutrition,
cyanogens consisting of bitter typically developing no specific on history of wetting method for
cassava (Manihot over <1 week, with findings exposure along cassava preparation
esculenta Crantz) or without optic with exclusion or avoid
neuropathy of other causes; consumption of
estimate bitter cassava
cyanogen
exposure by
measuring
urine or plasma
thiocyanate
Methotrexate Chemotherapy Subacute combined T2 hyperintensity Exposure to Methotrexate
(intrathecal) drug acting as degeneration of the in posterior intrathecal cessation, folic acid
folate antagonist spinal cord, with or columns with methotrexate; supplementation
without peripheral inverted V sign; low serum
neuropathy may extend over folate, high
several levels in plasma
cervical or homocysteine
thoracic cord
Tumor necrosis Bind cytokine TNF Transverse myelitis Variable, Exposure to TNF-α inhibitor
factor-α (TNF-α) to inhibit binding short-segment TNF-α inhibitor, cessation, IV
inhibitors (eg, to TNF receptors, eccentric T2 with or without methylprednisolone
adalimumab, promoting hyperintensity or CSF oligoclonal 1000 mg/d for 5 days,
etanercept, neuroinflammation longitudinally banding with or without
infliximab) extensive plasma exchange
transverse
myelitis, with or
without
gadolinium
enhancement
CONTINUED ON PAGE 157
156 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
CONTINUED FROM PAGE 156
Diagnostic
Toxin Etiology Symptoms/signs MRI tests Treatment
Immune Upregulate T cells Transverse myelitis Variable, Exposure to Immune checkpoint
checkpoint by blocking anti– short-segment immune inhibitor cessation, IV
inhibitors (eg, programmed cell eccentric T2 checkpoint methylprednisolone
ipilimumab, death 1 (PD1)/ hyperintensity or inhibitor, with 1000 mg/d for 5 days,
nivolumab) programmed longitudinally or without CSF with or without
death ligand 1 extensive oligoclonal plasma exchange
(PD-L1) and anti– transverse banding
cytotoxic myelitis, with or
T-lymphocyte without
associated protein gadolinium
4 (CTLA4) enhancement
Heroin IV heroin Acute onset of T2 Exposure to IV Avoid heroin,
administered after complete spinal cord hyperintensity heroin after consider opiate
a period of syndrome, with involving the period of reversal agent (eg,
abstinence flaccid paralysis, complete abstinence naloxone), IV
sensory level, and cross section of methylprednisolone
sphincter dysfunction the spinal 1000 mg/d for 5 days
cord, typically
over several
levels with
predilection for
thoracic cord
Radiation Fractionated or Delayed onset of T2 Prior exposure Dexamethasone,
stereotactic myelopathy hyperintensity to radiation consideration of
radiation for 6-24 months within prior with exclusion bevacizumab, avoid
malignancy following radiation radiation field, of other further radiation
gadolinium causes
enhancement
Hepatic Chronic liver Spastic paraparesis MRI spinal cord Features in Liver transplant,
myelopathy due disease with no specific keeping with shunt-limiting
to accumulation portosystemic findings; MRI chronic liver surgery
of toxins, likely shunting brain T1 disease
nitrogen hyperintensity in
products globus pallidus
Decompression Diving for Flaccid paralysis, MRI spinal cord; Recent diving Hyperbaric
myelopathy likely prolonged sensory alteration, often no specific oxygen
due to nitrogen duration with rapid sphincter dysfunction findings
bubbles ascent within 1 hour of diving although T2
hyperintensity
may be seen in
posterior and
lateral columns
CSF = cerebrospinal fluid; IM = intramuscular; IV = intravenous; MRI = magnetic resonance imaging.
CONTINUUMJOURNAL.COM 157
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
(eg, ipilimumab) for the treatment of cancer (eg, melanoma, lung cancer).
Combination therapy with nivolumab and ipilimumab results in greater than 10%
risk of experiencing immune-related adverse events, including rare cases of
transverse myelitis.46,47 Treatment includes stopping the immunomodulatory
drug (TNF-α inhibitor or immune checkpoint inhibitor) along with administration
of high-dose IV steroids, typically IV methylprednisolone 1000 mg/d for 5 days. If
no improvement is seen with steroids, plasma exchange should be considered.
Clioquinol is a metal chelator that was developed as an antimicrobial.
Clioquinol has been associated with the syndrome of subacute myelo-optico-
neuropathy that occurred in Japan before 1970, when the medication was
removed from the market.48 Individuals with subacute myelo-optico-neuropathy
experienced primarily lower extremity sensory symptoms, gait instability, and
visual impairment. Neurologic examination demonstrates primarily lower
extremity reduced tactile sensation/vibration, lower extremity weakness with
spasticity, and visual impairment. Around the time of clioquinol exposure, green
deposits may be seen in the mouth (“green hairy tongue”) due to an iron
chelate.49 The mechanism of clioquinol toxicity is speculated to be because of
CASE 6-3 A 23-year-old man was diagnosed with acute lymphoblastic leukemia. He
was treated with cyclophosphamide, vincristine, doxorubicin, and
dexamethasone (hyper-CVAD) induction chemotherapy. In addition, he
received intrathecal methotrexate and cytarabine for prevention of
central nervous system involvement. After three rounds of intrathecal
methotrexate, he began to report numbness and weakness in his legs.
Neurologic examination demonstrated reduced pin sensation below
T10, reduced proprioception at the great toes, absent vibration distal to
the iliac crests, hyporeflexia, and upgoing plantar responses. MRI of his
spinal cord demonstrated T2 hyperintensity in the posterior columns
extending from T8 to the conus medullaris without contrast
enhancement. MRI of his brain was normal. CSF analysis demonstrated
no evidence of malignant cells, a white blood cell count of 2 cells/mm3
(normal 0 cells/mm3 to 5 cells/mm3), and elevated protein. Serum
cobalamin and plasma methylmalonic acid were normal. Serum folate
was 4.3 nmol/L (lower limit of normal 7.0 nmol/L).
He was diagnosed with methotrexate myelopathy secondary to
intrathecal methotrexate, which acts as a folate antagonist. Intrathecal
chemotherapy was discontinued, and he was treated with oral folic acid
3 mg/d. Despite folic acid replacement, he continued to experience
increasing leg weakness over several weeks, requiring the use of a
wheelchair.
COMMENT Intrathecal methotrexate can result in a toxic myelopathy indistinguishable
from that of vitamin B12 deficiency clinically and radiologically. Deficits are
often severe, and discontinuing methotrexate and folate supplementation
is the mainstay of treatment.
158 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
reduced copper availability.49 Diagnosis was based on clinical assessment and KEY POINTS
prior exposure to clioquinol with exclusion of other etiologies. Treatment
● Subacute myelo-optico-
included discontinuing clioquinol. Subacute myelo-optico-neuropathy resulted neuropathy was caused by
in long-term neurologic deficits, although greater symptomatic improvement of clioquinol, a metal chelator
myelopathic deficits than of visual impairment has been seen over time.48 that may cause copper
deficiency.
Heroin Toxicity
● Reintroduction of heroin
Heroin is an opiate used as a recreational drug. Administration of IV heroin after following a period of
a period of abstinence has been associated with the acute onset (within hours) of abstinence may cause
myelopathy.50 The mechanism for heroin myelopathy is unclear, although acute-onset complete
theories include immune-mediated and vascular causes.50,51 Patients with heroin myelopathy.
myelopathy have a complete spinal cord syndrome with flaccid paralysis, sensory ● Radiation myelopathy is a
level, and sphincter dysfunction. MRI of the spinal cord typically demonstrates delayed effect of radiation
T2 hyperintensity affecting the complete cross section of the spinal cord over occurring 6 to 24 months
several levels, with a predilection for the thoracic region. Diagnosis is based on after radiation exposure.
clinical assessment and prior exposure to heroin with exclusion of other causes.
● Hepatic myelopathy
Treatment is discontinuation of heroin, consideration of administering an opiate occurs in chronic liver
reversal agent, and steroids, including IV methylprednisolone 1000 mg/d for disease with portosystemic
5 days.50,51 Neurologic deficits are typically severe and largely permanent. shunting.
Iatrogenic Toxicity
Radiation myelopathy is a delayed complication of radiation therapy used in the
treatment of malignancy. The risk of permanent spinal cord injury is believed to
be less than 1%, provided the cumulative dose of fractionated radiation to which
the spinal cord is exposed does not exceed 45 Gy to 50 Gy administered in 1.8 Gy
to 2 Gy daily fractions.52 Stereotactic body radiation therapy has emerged as a
treatment for spinal and paraspinal tumors given very focused administration
of high-dose radiation. Lhermitte syndrome after radiation therapy refers to
transient spinal cord symptoms that may occur 2 to 4 months following
radiation, with paresthesia in the back and extremities with neck flexion that
resolves over months without permanent myelopathy. Radiation myelopathy
typically develops approximately 6 to 24 months following exposure.52,53 Clinical
symptoms range in severity, and patients may present with hemicord symptoms
consistent with Brown-Séquard syndrome. MRI of the spinal cord demonstrates
focal T2 hyperintensity associated with contrast enhancement.52 In radiation
myelopathy, reactive gliosis, demyelination, and necrosis of white matter are
seen, along with vascular injury.52,53 Treatment typically includes a course of a
steroid such as dexamethasone. The role of hyperbaric oxygen is controversial.
Bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor, may be
beneficial in the treatment of radiation myelopathy.53 Prognosis is variable, although
median survival following diagnosis of radiation myelopathy is 8 months.52
Hepatic myelopathy occurs in chronic liver disease with portosystemic shunting,
typically because of a transjugular intrahepatic portosystemic shunt (TIPS) used
to reduce portal hypertension.54 The mechanism of hepatic myelopathy is not
fully known, but nitrogen products bypassing the liver may have a toxic effect on
the spinal cord. Progressive spastic paraparesis is seen, without significant
sensory symptoms or sphincter dysfunction. Rarely, patients may have a spastic
quadriparesis. MRI of the spinal cord typically is normal, whereas MRI of the
brain may demonstrate T1 hyperintensity in the globus pallidus from manganese
deposition that accumulates with liver failure. Treatment includes liver
CONTINUUMJOURNAL.COM 159
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
KEY POINT transplantation or shunt-limiting surgery, which may be particularly effective if
performed within 6 months of onset of myelopathy symptoms.
● Decompression
myelopathy occurs within
1 hour of diving and is Decompression Sickness
treated with hyperbaric Decompression sickness occurs because of nitrogen gas coming out of solution
oxygen therapy, typically from body tissues as a diver ascends; the decompression myelopathy typically
with good recovery.
occurs within 1 hour of diving. The mechanism is not fully known but may be
because of venous occlusion or nitrogen bubbles in tissue.55 Decompression
myelopathy is included here as a toxic myelopathy given that it is triggered
by a toxic exposure despite a potential vascular etiology. Risk factors include
prolonged dives with rapid ascent and patent foramen ovale with right-to-left
shunting. Onset is acute (within hours), with symptoms including weakness
(typically flaccid), sensory alteration, and sphincter dysfunction. MRI of the
spinal cord may demonstrate T2 hyperintensity primarily in the dorsolateral
region, although up to 70% of individuals have normal imaging. Treatment is
hyperbaric oxygen therapy, which is continued until no further improvement
is seen for two consecutive treatments. Prognosis is typically good, with
expected improvement in neurologic deficits.
CONCLUSION
Metabolic myelopathies are important to recognize as they are preventable and
typically respond to supplementation, particularly if treatment is initiated soon
after symptom onset. Toxic myelopathies often lead to more fixed neurologic
impairment but are important to recognize for future risk mitigation.
REFERENCES
1 Allen LH. How common is vitamin B-12 7 Flippo TS, Holder WD Jr. Neurologic degeneration
deficiency? Am J Clin Nutr 2009;89(2):693S-696S. associated with nitrous oxide anesthesia in
doi:10.3945/ajcn.2008.26947A patients with vitamin B12 deficiency. Arch Surg
1993;128(12):1391-1395. doi:10.1001/
2 Healton EB, Savage DG, Brust JC, et al. Neurologic
archsurg.1993.01420240099018
aspects of cobalamin deficiency. Medicine
(Baltimore) 1991;70(4):229-245. 8 Hunt A, Harrington D, Robinson S. Vitamin B12
doi:10.1097/00005792-199107000-00001 deficiency. BMJ 2014;349:g5226. doi:10.1136/
bmj.g5226
3 Agamanolis DP. Nutritional CNS disorders. In:
Neuropathology: an illustrated interactive course 9 Devalia V, Hamilton MS, Molloy AM. Guidelines
for medical students and residents. Accessed for the diagnosis and treatment of cobalamin
December 3, 2020. neuropathology-web.org/ and folate disorders. Br J Haematol 2014;166(4):
chapter8/chapter8Nutritional.html#b12 496-513. doi:10.1111/bjh.12959
4 Pant SS, Asbury AK, Richardson EP Jr. The 10 Solomon LR. Cobalamin-responsive disorders in
myelopathy of pernicious anemia. A the ambulatory care setting: unreliability of
neuropathological reappraisal. Acta Neurol cobalamin, methylmalonic acid, and
Scand 1968;44(S35):7-36. homocysteine testing. Blood 2005;105(3):
978-985. doi:10.1182/blood-2004-04-1641
5 Hemmer B, Glocker FX, Schumacher M, et al.
Subacute combined degeneration: clinical, 11 Wolffenbuttel BHR, Wouters HJCM, Heiner-
electrophysiological, and magnetic resonance Fokkema MR, van der Klauw MM. The many faces
imaging findings. J Neurol Neurosurg Psychiatry of cobalamin (vitamin B12) deficiency. Mayo Clin
1998;65(6):822-827. doi:10.1136/jnnp.65.6.822 Proc Innov Qual Outcomes 2019;3(2):200-214.
doi:10.1016/j.mayocpiqo.2019.03.002
6 Oh R, Brown DL. Vitamin B12 deficiency. Am Fam
Physician 2003;67(5):979-986. 12 Stabler SP. Clinical practice. Vitamin B12
deficiency. N Engl J Med 2013;368(2):149-160.
doi:10.1056/NEJMcp1113996
160 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
13 Matsuura H, Nakamura T. Inverted V sign: 26 Goodman BP. Metabolic and toxic causes of
subacute combined degeneration of the spinal myelopathy. Continuum (Minneap Minn) 2015;
cord. QJM 2018;111(1):65-66. doi:10.1093/qjmed/ 21(1 Spinal Cord Disorders):84-99. doi:10.1212/01.
hcx189 CON.0000461086.79241.3b
14 Gürsoy AE, Kolukısa M, Babacan-Yıldız G, Celebi 27 Gletsu-Miller N, Broderius M, Frediani JK, et al.
A. Subacute combined degeneration of the Incidence and prevalence of copper deficiency
spinal cord due to different etiologies and following Roux-en-Y gastric bypass surgery. Int J
improvement of MRI findings. Case Rep Neurol Obes (Lond) 2012;36(3):328-335. doi:10.1038/
Med 2013;2013:159649. doi:10.1155/2013/159649 ijo.2011.159
15 Schwendimann RN. Metabolic and toxic 28 Kumar N. Copper deficiency myelopathy (human
myelopathies. Continuum (Minneap Minn) 2018; swayback). Mayo Clin Proc 2006;81(10):1371-1384.
24(2, Spinal Cord Disorders):427-440. doi:10.1212/ doi:10.4065/81.10.1371
CON.0000000000000596
29 Jaiser SR, Winston GP. Copper deficiency
16 Wang H, Li L, Qin LL, et al. Oral vitamin B12 versus myelopathy. J Neurol 2010;257(6):869-881.
intramuscular vitamin B12 for vitamin B12 doi:10.1007/s00415-010-5511-x
deficiency. Cochrane Database Syst Rev 2018;
30 Muller DPR. Vitamin E and neurological function.
3(3):CD004655. doi:10.1002/14651858.
Mol Nutr Food Res 2010;54(5):710-718.
CD004655.pub3
doi:10.1002/mnfr.200900460
17 Oussalah A, Julien M, Levy J, et al. Global burden
31 El Euch-Fayache G, Bouhlal Y, Amouri R, et al.
related to nitrous oxide exposure in medical and
Molecular, clinical and peripheral neuropathy
recreational settings: a systematic review and
study of Tunisian patients with ataxia with
individual patient data meta-analysis. J Clin Med
vitamin E deficiency. Brain 2014;137(pt 2):402-410.
2019;8(4):551. doi:10.3390/jcm8040551
doi:10.1093/brain/awt339
18 Yuan JL, Wang SK, Jiang T, Hu WL. Nitrous oxide
32 Yokota T, Uchihara T, Kumagai J, et al.
induced subacute combined degeneration
Postmortem study of ataxia with retinitis
with longitudinally extensive myelopathy with
pigmentosa by mutation of the alpha-tocopherol
inverted V-sign on spinal MRI: a case report and
transfer protein gene. J Neurol Neurosurg
literature review. BMC Neurol 2017;17(1):222.
Psychiatry 2000;68(4):521-525. doi:10.1136/
doi:10.1186/s12883-017-0990-3
jnnp.68.4.521
19 Patel KK, Mejia Munne JC, Gunness VRN, et al.
33 Mariotti C, Gellera C, Rimoldi M, et al. Ataxia with
Subacute combined degeneration of the spinal
isolated vitamin E deficiency: neurological
cord following nitrous oxide anesthesia: a
phenotype, clinical follow-up and novel
systematic review of cases. Clin Neurol
mutations in TTPA gene in Italian families. Neurol
Neurosurg 2018;173:163-168. doi:10.1016/
Sci 2004;25(3):130-137. doi:10.1007/s10072-004-
j.clineuro.2018.08.016
0246-z
20 Massey TH, Pickersgill TT, Peall KJ. Nitrous oxide
34 Peters SA, Kelly FJ. Vitamin E supplementation in
misuse and vitamin B12 deficiency. BMJ Case Rep
cystic fibrosis. J Pediatr Gastroenterol Nutr 1996;
2016;2016:bcr2016215728.
22(4):341-345. doi:10.1097/00005176-199605000-
21 Bailey RL, Dodd KW, Gahche JJ, et al. Total folate 00001
and folic acid intake from foods and dietary
35 Enneking D. The nutritive value of grasspea
supplements in the United States: 2003-2006.
(Lathyrus sativus) and allied species, their toxicity
Am J Clin Nutr 2010;91(1):231-237. doi:10.3945/
to animals and the role of malnutrition in
ajcn.2009.28427
neurolathyrism. Food Chem Toxicol 2011;49(3):
22 Okada A, Koike H, Nakamura T, et al. Slowly 694-709. doi:10.1016/j.fct.2010.11.029
progressive folate-deficiency myelopathy:
36 Woldeamanuel YW, Hassan A, Zenebe G.
report of a case. J Neurol Sci 2014;336(1-2):
Neurolathyrism: two Ethiopian case reports and
273-275. doi:10.1016/j.jns.2013.10.032
review of the literature. J Neurol 2012;259(7):
23 Wickramasinghe SN. Diagnosis of megaloblastic 1263-1268. doi:10.1007/s00415-011-6306-4
anaemias. Blood Rev 2006;20(6):299-318.
37 Misra UK, Sharma VP, Singh VP. Clinical aspects
doi:10.1016/j.blre.2006.02.002
of neurolathyrism in Unnao, India. Spinal Cord
24 Pincus JH, Reynolds EH, Glaser GH. Subacute 1993;31(4):249-254.
combined system degeneration with folate
38 Bick AS, Meiner Z, Gotkine M, Levin M. Using
deficiency. JAMA 1972;221(5):496-497.
advanced imaging methods to study
doi:10.1001/jama.1972.03200180038010
neurolathyrism. Isr Med Assoc J 2016;18(6):
25 Nakamura T, Nishi M, Rikitake M, et al. A case of 341-345.
subacute combined degeneration of the spinal
39 Kashala-Abotnes E, Okitundu D, Mumba D, et al.
cord due to folic acid and copper deficiency.
Konzo: a distinct neurological disease associated
Brain Dev 2019;41(1):111-115. doi:10.1016/j.
with food (cassava) cyanogenic poisoning. Brain
braindev.2018.07.006
Res Bull 2019;145:87-91. doi:10.1016/j.brainresbull.
2018.07.001
CONTINUUMJOURNAL.COM 161
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METABOLIC AND TOXIC MYELOPATHIES
40 Nhassico D, Bradbury JH, Cliff J, et al. Use of the 48 Konagaya M, Matsumoto A, Takase S, et al.
wetting method on cassava flour in three konzo Clinical analysis of longstanding subacute myelo-
villages in Mozambique reduces cyanide intake optico-neuropathy: sequelae of clioquinol at 32
and may prevent konzo in future droughts. Food years after its ban. J Neurol Sci 2004;218(1-2):
Sci Nutr 2016;4(4):555-561. doi:10.1002/fsn3.317 85-90. doi:10.1016/j.jns.2003.11.007
41 Tylleskar T, Howlett WP, Rwiza HT, et al. Konzo: a 49 Schaumburg H, Herskovitz S. Copper deficiency
distinct disease entity with selective upper myeloneuropathy: a clue to clioquinol-induced
motor neuron damage. J Neurol Neurosurg subacute myelo-optic neuropathy? Neurology
Psychiatry 1993;56(6):638-643. doi:10.1136/ 2008;71(9):622-623. doi:10.1212/01.
jnnp.56.6.638 wnl.0000324620.86645.c1
42 Gosavi T, Diong CP, Lim SH. Methotrexate- 50 Ivanovski T, Espino Ibañez AM, Barcelo Martin B,
induced myelopathy mimicking subacute Gomila Muñiz I. Acute extensive myelopathy
combined degeneration of the spinal cord. J Clin after single heroin and cocaine exposure in a
Neurosci 2013;20(7):1025-1026. patient with toxicological evidence of long-term
doi:10.1016/j.jocn.2012.06.018 drug abstinence. BMJ Case Rep 2019;12(3):
e228335. doi:10.1136/bcr-2018-228335
43 Pinnix CC, Chi L, Jabbour EJ, et al. Dorsal column
myelopathy after intrathecal chemotherapy for 51 Mahoney KW, Romba M, Gailloud P, et al. Acute
leukemia. Am J Hematol 2017;92(2):155-160. progressive paraplegia in heroin-associated
doi:10.1002/ajh.24611 myelopathy. J Clin Neurosci 2018;51:69-71.
doi:10.1016/j.jocn.2018.02.005
44 Juster-Switlyk K, Smith AG, Kovacsovics T, et al.
MTHFR C677T polymorphism is associated with 52 Wong CS, Fehlings MG, Sahgal A. Pathobiology of
methotrexate-induced myelopathy risk. radiation myelopathy and strategies to mitigate
Neurology 2017;88(6):603-604. doi:10.1212/ injury. Spinal Cord 2015;53(8):574-580.
WNL.0000000000003590 doi:10.1038/sc.2015.43
45 Barreras P, Mealy MA, Pardo CA. TNF-alpha 53 Cañedo G, Solis I, González-San Segundo C, et al.
inhibitor associated myelopathies: a neurological Treatment of radiation-induced myelopathy with
complication in patients with rheumatologic bevacizumab. Clin Transl Oncol 2020;22(6):
disorders. J Neurol Sci 2017;373:303-306. 957-960. doi:10.1007/s12094-019-02209-5
doi:10.1016/j.jns.2017.01.023
54 Zhao H, Yue Z, Wang L, et al. Benefits of early
46 Spain L, Tippu Z, Larkin JM, et al. How we treat treatment for patients with hepatic myelopathy
neurological toxicity from immune checkpoint secondary to TIPS: a retrospective study in
inhibitors. ESMO Open 2019;4(suppl 4):e000540. Northern China. Sci Rep 2018;8(1):15184.
doi:10.1136/esmoopen-2019-000540 doi:10.1038/s41598-018-33216-1
47 Liao B, Shroff S, Kamiya-Matsuoka C, Tummala S. 55 Saadi A, Ferenczi EA, Reda H. Spinal
Atypical neurological complications of decompression sickness in an experienced
ipilimumab therapy in patients with metastatic scuba diver: a case report and review of
melanoma. Neuro Oncol 2014;16(4):589-593. literature. Neurohospitalist 2019;9(4):235-238.
doi:10.1093/neuonc/nou001 doi:10.1177/1941874419828895
162 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
REVIEW ARTICLE
Myelitis and Other
C O N T I N UU M A U D I O
INTERVIEW AVAILABLE
ONLINE
Autoimmune
Myelopathies
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo65TEub0G9tZtPaMachiqn on 04/28/2022
By Sebastian Lopez Chiriboga, MD; Eoin P. Flanagan, MBBCh
ABSTRACT
PURPOSE OF REVIEW: This article provides an update on the clinical diagnosis
and management of immune-mediated myelopathies, including the
relevance of imaging, ancillary testing with an emphasis on autoantibody
biomarkers, recognition of myelitis mimics, and therapeutic approach.
RECENT FINDINGS: The imaging characterization of immune-mediated
myelopathies and the discovery of neural autoantibodies have been crucial
in improving our ability to accurately diagnose myelitis. The identification
of autoantibodies directed against specific central nervous system targets
has led to major improvements in our understanding of the mechanisms
underlying inflammation in myelitis. It has also allowed distinction of these
CITE AS: myelopathy etiologies from noninflammatory etiologies of myelopathy and
CONTINUUM (MINNEAP MINN) from multiple sclerosis and provided insight into their risk of recurrence,
2021;27(1, SPINAL CORD DISORDERS):
62–92.
treatment response, and long-term clinical outcomes. Prompt recognition
and appropriate testing in the setting of acute and subacute myelopathies
Address correspondence to is critical as timely administration of immunotherapy can help improve
Dr Eoin P. Flanagan, 200 First symptoms and prevent permanent neurologic disability. A patient should
Street SW, Rochester,
Minnesota 55905, not be classified as having “idiopathic transverse myelitis” without a
flanagan.eoin@mayo.edu. comprehensive evaluation for a more specific etiology. Achieving the
correct diagnosis and learning to recognize noninflammatory myelitis
RELATIONSHIP DISCLOSURE:
Dr Lopez Chiriboga reports mimics is crucial as they have therapeutic and prognostic implications.
no disclosure. Dr Flanagan
has received research/
grant support from
SUMMARY: Identifying the clinical and radiographic features of
MedImmune/VielaBio. immune-mediated myelitis and recognizing mimics and pitfalls will help
clinicians treat confirmed autoimmune myelitis appropriately.
UNLABELED USE OF
PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
Drs Lopez Chiriboga and
Flanagan discuss the INTRODUCTION
T
unlabeled/investigational use of he differential diagnosis of immune-mediated myelopathies is broad
azathioprine, corticosteroids,
and includes noninflammatory myelopathies from compressive,
cyclophosphamide, IV
immunoglobulin, methotrexate, vascular, neoplastic, metabolic, nutritional, infectious, toxic, and
mycophenolate mofetil, plasma inherited causes.1 Age, sex, ethnicity, risk factors, and comorbidities
exchange, and rituximab for the
treatment of myelitis and other
can help narrow the differential diagnosis, but careful attention
autoimmune myelopathies. to the clinical history with focus on the temporal profile of symptom onset,
neuroimaging features, and comprehensive serologic and CSF evaluation is
© 2021 American Academy necessary to distinguish immune-mediated myelopathies from other causes and
of Neurology. achieve a definitive diagnosis.2,3 This article focuses on recent advances
62 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
regarding the clinical, imaging, and serologic features and contemporary KEY POINTS
treatment of immune-mediated myelopathies.
● The differential diagnosis
of immune-mediated
TRANSVERSE MYELITIS DEFINITION AND TERMINOLOGY myelopathies is broad and
Myelitis refers to inflammation of the spinal cord; the inflammation can result includes noninflammatory
from infectious, immune-mediated, or other causes. The term transverse myelopathies from
compressive, vascular,
myelitis has become synonymous with immune-mediated myelitis; however,
neoplastic, metabolic,
“transverse” myelitis implies inflammation across the entire transverse section of nutritional, infectious, toxic,
the spinal cord, and many causes of myelitis (eg, multiple sclerosis [MS]– and inherited causes.
associated myelitis) cause inflammation of only a segment of the spinal cord on
cross section. Although such cases are often termed partial transverse myelitis ● The length of the
T2-hyperintense lesion seen
and those with inflammation across the entire cross section of the cord are on sagittal spinal cord
referred to as complete transverse myelitis, the clinical accompaniments of imaging is a very useful
partial and complete transverse myelitis can overlap. The presence of bilateral discriminator between
symptoms and signs is often used to distinguish complete from partial transverse multiple sclerosis (less than
three vertebral segments)
myelitis, but involvement of just the hemicord may still result in bilateral and aquaporin-4 (AQP4)
symptoms and signs (eg, as in Brown-Séquard syndrome). IgG–seropositive
Whereas clinical definitions have been problematic, radiologic discriminators neuromyelitis optica
have proved more useful. The length of the T2-hyperintense lesion seen on spectrum disorder (NMOSD)
(three or more vertebral
sagittal spinal cord imaging is a very useful discriminator between MS (less than segments).
three vertebral segments) and aquaporin-4 (AQP4) IgG–seropositive
neuromyelitis optica spectrum disorder (NMOSD) (three or more vertebral ● Idiopathic transverse
segments). Transverse myelitis is generally classified into disease-associated (ie, myelitis should be
considered a diagnosis of
related to a specific infectious or immune-mediated etiology) and idiopathic
exclusion, with a
forms. Diagnostic criteria for idiopathic transverse myelitis were established in comprehensive evaluation
2002 in an effort to identify homogeneous groups of patients for clinical studies. for both inflammatory and
The criteria define idiopathic transverse myelitis as bilateral (although not noninflammatory etiologies
necessarily symmetric) symptoms/signs of spinal cord dysfunction (sensory, before assigning that
diagnosis.
motor, or autonomic) evolving over 4 hours to 21 days, a sensory level on the
trunk, and evidence of inflammation (MRI gadolinium enhancement or CSF ● Significant advances in
pleocytosis/elevated IgG index) with appropriate exclusion of alternative the field of autoimmune
etiologies.4 Thus, idiopathic transverse myelitis should be considered a diagnosis neurology, including the
discovery of neural
of exclusion, with a comprehensive evaluation for both specific inflammatory autoantibodies, have
and noninflammatory etiologies before assigning the diagnosis. This is further assisted in identifying a
emphasized by recent studies highlighting that up to 70% of patients with a specific cause for patients
suspected diagnosis of idiopathic transverse myelitis have an alternative specific previously classified as
having idiopathic transverse
cause of myelopathy found.2,3 Significant advances in the field of autoimmune
myelitis.
neurology, including the discovery of neural autoantibodies (eg, AQP4-IgG and
myelin oligodendrocyte glycoprotein [MOG] IgG), have assisted in identifying a ● Better radiographic
specific cause for patients previously classified as having idiopathic transverse characterization of
myelitis.2,5 Better radiographic characterization of immune-mediated immune-mediated
myelopathies and their
myelopathies and their mimics has improved our ability to diagnose patients mimics has improved our
with myelopathies of uncertain etiology.6 These advances highlight the need for ability to diagnose patients
updated diagnostic criteria for myelitis and for potentially removing transverse with myelopathies of
from the terminology as it often leads to confusion and fails to capture the uncertain etiology.
frequently encountered focal spinal cord inflammation.
DEMOGRAPHICS AND EPIDEMIOLOGY
Immune-mediated myelopathies are more commonly encountered in females
and can affect all ages. MOG-IgG–associated disorders and myelitis occurring as
CONTINUUMJOURNAL.COM 63
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
a component of acute disseminated encephalomyelitis (ADEM), up to 50% of
which is MOG-IgG seropositive, are more common in children; acute flaccid
myelitis associated with outbreaks of enterovirus also occurs predominantly in
children.7 A paraneoplastic myelopathy is more common in older adults, in
whom the cancers (breast and lung) most associated with this disorder more
commonly occur.8,9 Dural arteriovenous fistulas predominantly affect older
males and should be strongly considered as a myelitis mimic when thoracic
myelopathy occurs in this demographic.
Race is important to consider when evaluating patients with immune-
mediated myelopathies. Neurosarcoidosis is more common in African
Americans,10 and the prevalence of AQP4-IgG–seropositive NMO/NMOSD
appears to be higher in Asians, Hispanics, Native Americans, and Africans.11
MS is more frequent in Whites and in regions farther from the equator.
Few studies exist on the incidence and prevalence of idiopathic transverse
myelitis, but a 2019 population-based US study (Olmsted County, Minnesota)
showed that the incidence of idiopathic transverse myelitis was 8.6 per million
person-years and the prevalence was 7.9 per 100,000.5
CLINICAL FEATURES
When evaluating patients with suspected myelitis, a detailed clinical history with
focus on the temporal evolution is one of the most important aspects that can
help narrow the differential diagnosis.
Time to Nadir
The time from onset to maximal neurologic deficit is the most important feature
to determine when evaluating a myelopathy as it helps narrow the differential
diagnosis (TABLE 3-1).2,3
The time to nadir can be classified as hyperacute (<12 hours), acute/subacute
(1 to 21 days), or chronic progressive (progression beyond 21 days). In spinal cord
infarction, the rapid onset of severe deficits reaching nadir within a few hours
(up to 12 hours) is typical and occurs in approximately 80% of patients with
spinal cord infarction.12 Most patients with idiopathic or disease-associated
myelitis reach nadir in 1 to 21 days. Symptoms that progress beyond 21 days are
more suggestive of an alternative etiology, such as spondylotic myelopathy, dural
arteriovenous fistula, metabolic myelopathy, paraneoplastic myelopathy,
neoplasms, or primary progressive MS.
Presenting Features
The classic clinical feature of myelitis is the development of sensorimotor deficits
in one or more extremities. Ascending numbness, often accompanied by a
sensory level across the trunk, is a characteristic presentation. Autonomic
dysfunction is frequent, with a combination of neurogenic bladder (usually
urinary retention), neurogenic bowel, and sexual dysfunction potentially
encountered; these features are particularly common with MOG-IgG–associated
disorder, perhaps reflecting conus involvement radiologically. Clinical features
supportive of a demyelinating etiology include the Lhermitte phenomenon
(an electrical sensation that radiates down the spine and to the extremities on
neck flexion) and the Uhthoff phenomenon (transient worsening of neurologic
symptoms from excessive heat). Tonic spasms (recurrent short-lived episodes of
involuntary painful flexor contractions lasting 30 seconds to a few minutes) are
64 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
another clinical feature. They can appear dystonic-like, usually follow a myelitis KEY POINTS
episode, and can be triggered by movement or hyperventilation. Ephaptic
● The time from onset to
transmission is thought to be the mechanism underlying tonic spasms. The maximal neurologic deficit is
spasms often respond well to carbamazepine. Tonic spasms are particularly the most important feature
frequent in AQP4-IgG–seropositive NMOSD. Neuropathic pruritus can be the to determine when
initial manifestation of myelitis with AQP4-IgG–seropositive NMOSD. evaluating a myelopathy as it
helps narrow the differential
The clinical severity of myelitis at nadir is usually mild with MS and moderate
diagnosis.
to severe with AQP4-IgG–seropositive NMOSD and MOG-IgG–associated
disorder (often requiring a gait aid); however, recovery is better with ● The time to nadir in
MOG-IgG–associated disorder than AQP4-IgG–seropositive NMOSD. Rarely, myelopathy can be
respiratory failure requiring mechanical ventilation may ensue from a severe classified as hyperacute
(<12 hours), acute/subacute
cervical myelitis accompanying MOG-IgG–associated disorder or AQP4-IgG– (1 to 21 days), or chronic
seropositive NMOSD. The natural evolution of attacks of myelitis associated with progressive (progression
central nervous system (CNS) inflammatory demyelinating diseases (MS, beyond 21 days).
AQP4-IgG–seropositive NMOSD, MOG-IgG–associated disorder) is subacute
● In spinal cord infarction,
development reaching nadir within 21 days with potential plateau, followed by the rapid onset of severe
subsequent improvement that may be sped up by intervening with treatment. deficits reaching nadir
Back-to-back attacks may occur, particularly with AQP4-IgG–seropositive within a few hours (up to
NMOSD. Primary progressive MS has a more insidious onset and slow 12 hours) is typical and
occurs in approximately
progression beyond 1 year and usually manifests as a progressive myelopathy.
80% of patients.
Rarely, patients may have a single MS lesion and develop insidious motor
progression from that lesion if located in an eloquent location (eg, spinal cord ● Most patients with
lateral columns). These patients are classified as having progressive solitary idiopathic or
sclerosis as they follow a course similar to primary progressive MS but lack the disease-associated
transverse myelitis reach
dissemination in space required to fulfill MS criteria.13 It is also recognized that a nadir in 1 to 21 days.
subset of patients with progressive MS fulfilling MS diagnostic criteria may have
isolated unilateral motor progression despite having bilateral demyelinating ● The natural evolution of
lesions in many CNS regions. The worsening in such cases is often attributable to attacks of myelitis
associated with central
a single severe lesion located along the lateral columns of the spinal cord (usually nervous system
accompanied by atrophy). This highlights the potential important contribution inflammatory demyelinating
of focal lesions in eloquent locations to motor disability in MS.14 diseases is subacute
An encephalomyelitis accompanied by glial fibrillary acidic protein development reaching nadir
within 21 days with potential
(GFAP) antibodies or glycine receptor antibodies may develop subacutely or
plateau, followed by
insidiously and often progresses beyond 21 days. Autoimmune GFAP subsequent improvement
astrocytopathy rarely manifests as isolated myelitis, and cerebral involvement at that may be sped up by
the time of myelitis is almost universal.15 Paraneoplastic myelopathy can be intervening with treatment.
necrotizing with a fulminant or slowly progressive course.9,16 Asking about a
prior history or assessing for the concurrent presence of CNS demyelinating
episodes (eg, optic neuritis) is useful to indicate a CNS inflammatory
demyelinating disease as the cause. A preceding vaccination or a viral-like
prodrome may suggest MOG-IgG–associated disorder or GFAP antibody–
associated encephalomyelitis.17 An area postrema syndrome manifested by
intractable nausea and vomiting with or without hiccups should raise the
suspicion for AQP4-IgG–seropositive NMOSD and may occur in isolation or
immediately precede an episode of myelitis.17 A smoking history, unintended
weight loss, or known cancer should raise concern for a paraneoplastic
myelopathy, which often manifests before the detection of cancer.18 Asking
about symptoms suggestive of systemic autoimmune disorders (eg, oral or
genital ulcers in Behçet disease) or sicca symptoms and looking for the presence
of arthritis or skin changes that may suggest systemic sarcoid involvement are
CONTINUUMJOURNAL.COM 65
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
TABLE 3-1 Differential Diagnosis of Myelopathies
Onset and etiologies Clinical/MRI clues
Acute
Vascular
Spinal cord infarct (anterior or posterior spinal artery) Vascular risk factors
Fibrocartilaginous embolism Valsalva, disk adjacent to lesion
Hematoma (hematomyelia, epidural hematoma) Bleeding diathesis, trauma
Structural/trauma
Surfer’s myelopathy Novice surfer
Spinal cord contusion Recent trauma
Subacute
Inflammatory demyelinating disease
Multiple sclerosis Short peripheral T2 lesions in dorsal/lateral columns
Aquaporin-4 antibody–seropositive neuromyelitis Longitudinally extensive T2 lesion
optica spectrum disorder (NMOSD)
Myelin oligodendrocyte glycoprotein (MOG) Long or short T2 lesion; conus involvement; nonenhancing
antibody–associated disorder
Acute disseminated encephalomyelitis (ADEM) Coexisting deep gray brain lesions
Inflammatory, confirmed etiology
Spinal cord sarcoidosis Milder deficit despite large lesion, linear dorsal subpial/trident
enhancement
Connective tissue disease associated (Behçet Systemic features of connective tissue disease
disease, lupus, Sjögren syndrome)
Paraneoplastic Known cancer; cancer risk factors; tract-specific lesion, especially
gadolinium enhancing
Immune checkpoint inhibitor associated Recent use of checkpoint inhibitor
Infectious
Bacterial (Lyme disease, syphilis, tuberculosis) Recent tick bite/rash; high-risk behavior
Viral (varicella-zoster virus, herpes simplex virus Zoster rash, genital herpes, endemic region for enterovirus/
type 1, herpes simplex virus type 2 [may be associated West Nile virus; high-risk behavior
with lumbar myeloradiculitis, Elsberg syndrome],
cytomegalovirus, West Nile virus,
enterovirus-associated acute flaccid myelitis; human
immunodeficiency virus [HIV])
Parasitic (schistosomiasis) Endemic region
Idiopathic Extensive investigations should be undertaken to assess for specific
cause before assigning this diagnosis
CONTINUED ON PAGE 67
66 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
CONTINUED FROM PAGE 66
Onset and etiologies Clinical/MRI clues
Chronic progressive (may have subacute onset/worsening)
Vascular
Dural arteriovenous fistula Clinical worsening after exertion or steroids, thoracic longitudinally
extensive lesion, flow voids
Cavernous malformation/arteriovenous malformation Popcorn appearance for cavernous malformationa
Inflammatory or demyelinating
Progressive solitary sclerosis Single multiple sclerosis lesion in lateral columns or pyramids of medulla
Primary progressive multiple sclerosis Multiple short T2 lesions in cord
Spinal cord sarcoidosis Milder deficit despite large lesion, linear dorsal subpial/trident
enhancement
Paraneoplastic Known cancer, smoking
Infectious
Bacterial (syphilis, tuberculosis); epidural abscess High-risk behavior, endemic region, IV drug use
Viral (HIV, human T-cell lymphotropic virus High-risk behavior, endemic region, dorsal/lateral column signal
type 1 [HTLV-1]) abnormality
Neoplastic
Primary spinal cord gliomas (astrocytoma, ependymoma) Prior radiation, expansile, mass effect, cap signb
Primary intramedullary spinal cord lymphoma Expansile lesion; persistent enhancement (>3 months), steroid
responsive, immunosuppressed
Metastatic disease (intramedullary, extramedullary Known solid organ cancer
compressive)
Structural
Spondylotic myelopathy History of trauma, neck osteoarthritis
Hereditary
Adrenomyeloneuropathy Neuropathy, progressive cord atrophy, adrenal involvement
Hereditary spastic paraplegia Spasticity disproportionate to weakness; progressive spinal cord atrophy
Mitochondrial disorders (eg, DARS2 gene) Dorsal/lateral signal abnormality; elevated lactate
Other genetic
Toxic/metabolic
Nutritional deficiency (vitamin B12, copper, vitamin E) Gastric bypass, zinc supplements, malabsorption
Toxic (intrathecal methotrexate, heroin, vitamin B6) Toxic exposure
Iatrogenic
Radiation Prior radiation exposure
IV = intravenous.
a
Popcorn appearance: mixed intensity at the center of the lesion from vascular components with a T2 hypointense rim from blood products.
b
A cap of T2 hypointensity secondary to hemosiderin is present at the top or bottom of the lesion.
CONTINUUMJOURNAL.COM 67
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
useful; such symptoms can suggest a myelopathy associated with a connective
tissue disorder. It is important to recognize that AQP4-IgG–seropositive NMOSD
can coexist with systemic autoimmune disorders, including systemic lupus
erythematosus, Sjögren syndrome, and antiphospholipid syndrome, and testing
for AQP4-IgG in such cases is prudent as a seropositive result confirms a
coexisting autoimmune neurologic disorder rather than a neurologic
manifestation of a systemic connective tissue disease (refer to the discussion on
autoantibodies below).
In the authors’ experience, patients with spinal cord sarcoidosis often present
with a myelopathy before they are diagnosed with systemic sarcoidosis; the
presentation may be subacute in onset (mimicking transverse myelitis) or
chronic and progressive, reaching nadir after 21 days.19 Systemic or primary CNS
vasculitis involving the spinal cord has been reported.20 Inflammatory
myelopathies have been described in patients with rheumatoid arthritis,
scleroderma, mixed connective tissue disease, and IgG4-related disease.21
It is also helpful to assess for clues to nonimmune myelopathies that
commonly cause or mimic transverse myelitis. The absence of sensory symptoms
with flaccid muscle tone in a child is strongly suggestive of the acute flaccid
myelitis associated with enterovirus D68, whereas the presence of genital herpes
(Elsberg syndrome) or vesicular rash (varicella-zoster virus) may suggest an
infectious-related myelitis. For more information on infectious myelopathies,
refer to the article “Infectious Myelopathies” by Michel Toledano, MD,22 in this
issue of Continuum. Worsening with exercise, Valsalva maneuver, or
corticosteroids is suggestive of dural arteriovenous fistula, and onset after
Valsalva maneuver is also seen with fibrocartilaginous embolism. For more
information on vascular myelopathies, refer to the article “Vascular
Myelopathies” by Nicholas L. Zalewski, MD,23 in this issue of Continuum. The
presence of constitutional symptoms (eg, fevers, chills, night sweats) suggests
epidural abscess, whereas a history of cancer should raise suspicion of metastatic
spinal cord compression. MRI will usually readily distinguish these conditions
from an immune-mediated myelopathy.
Typical findings of myelitis on neurologic examination include a sensory level
across the trunk and an upper motor neuron pattern of weakness, hyperreflexia,
spasticity, and extensor plantar responses, but these may take time to develop.1,4,24
The McArdle sign (rapidly reversible pyramidal weakness induced by
neck flexion) is suggestive of MS myelitis.25 The presence of an inverted
brachioradialis, triceps, or biceps jerk is suggestive of a myeloradiculopathy
(most commonly cervical spondylosis). For more information on spinal cord
localization, refer to the article “Spinal Cord Anatomy and Localization” by Todd
A. Hardy, PhD, MBBS, FRACP,26 in this issue of Continuum. Acute spinal cord
syndromes can present with spinal shock (flaccid limb weakness with areflexia
and mute plantar reflexes) mimicking lower motor neuron disorders, such as
Guillain-Barré syndrome.
NEUROIMAGING IN MYELITIS
MRI with and without gadolinium is the imaging modality of choice in the
evaluation of myelopathies; in those with contraindications for MRI, CT
myelography can be considered to exclude extrinsic compression.
Diffusion-weighted images should be requested in hyperacute and acute
myelopathy, which are not part of the usual MRI spine protocol. Confirmation of
68 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
lesions on multiple planes can improve specificity to avoid false-positive findings KEY POINTS
due to artifacts and false-negative results. Detailed evaluation of the gadolinium
● AQP4-IgG–seropositive
enhancement pattern is critical as it can provide clues to determine specific NMOSD can coexist with
etiologies (TABLE 3-2). Persistent enhancement beyond 3 months should prompt systemic autoimmune
strong consideration of noninflammatory etiologies, including neoplastic causes disorders, including
or dural arteriovenous fistula. Once extrinsic compression is excluded and if an systemic lupus
erythematosus, Sjögren
inflammatory myelopathy is suspected, imaging the entire spine (cervical and
syndrome, and
thoracic spine) and brain is often useful to assess for other lesions (eg, MS or antiphospholipid syndrome.
ADEM) that can help narrow the differential diagnosis. Repeat imaging can be Testing for AQP4-IgG in such
considered in patients with a severe definitive myelopathy as the initial MRI may cases is prudent as a
seropositive result confirms
be negative and subsequent MRIs may detect the lesion in spinal cord infarct and
a coexisting autoimmune
MOG-IgG–associated disorder myelitis.12,27 neurologic disorder rather
than a neurologic
Length of the T2-Hyperintense Lesion on Sagittal Images manifestation of a systemic
connective tissue disease.
The length and location of lesions are helpful in the differential diagnosis of
myelitis as they can provide clues to the specific etiology. ● Typical findings of
myelitis on neurologic
SHORT LESIONS (LESS THAN THREE VERTEBRAL SEGMENTS). A lesion extending less examination include a
than three vertebral segments (a short lesion) is most suggestive of MS sensory level across the
trunk and an upper motor
(FIGURE 3-1), and multiple peripheral short T2 hyperintensities within the spinal neuron pattern of weakness,
cord with or without typical brain lesions is strongly suggestive of MS. Indeed, hyperreflexia, spasticity,
it is not uncommon for primary progressive MS to have predominantly or and extensor plantar
exclusively spinal cord lesions. Lesions are usually wedge-shaped on axial images responses, but these may
take time to develop.
and involve the periphery of the cord in either the lateral or dorsal columns
(FIGURE 3-1B), although, less frequently, the central gray and anterior white ● Detailed evaluation of the
matter can also be affected. When imaged with higher field strengths, lesions gadolinium enhancement
are hypointense on T1-weighted sequences.28 Spinal cord edema is typically pattern on MRI is critical in
seen in the acute phase of MS myelitis, potentially mimicking neoplastic the evaluation of
myelopathies as it can
myelopathies; as edema resolves, chronic MS T2-hyperintense spinal cord lesions provide clues to determine
may appear smaller but typically do not resolve completely. Enhancement is specific etiologies.
present in most acute lesions; the pattern is variable, usually homogeneous or
patchy, but ring enhancement29 is seen in about one-third of enhancing cord ● A lesion extending less
than three vertebral
lesions in MS (FIGURES 3-1C and 3-1D)30 and the enhancement usually resolves segments (a short lesion) is
within 8 weeks.31 On sagittal imaging in patients with chronic MS, the coalescence most suggestive of multiple
of multiple short lesions can mimic longitudinally extensive transverse myelitis sclerosis, and multiple
(LETM),32 but true LETM is a red flag in MS and should prompt evaluation for an peripheral short T2
hyperintensities within the
alternative etiology.30 In some patents with unilateral progression or progression
spinal cord with or without
in the setting of a single lesion (ie, progressive solitary sclerosis), focal lesional typical brain lesions is
atrophy may develop over time and is usually located in the eloquent spinal strongly suggestive of
cord lateral columns (FIGURE 3-2) or in the medullary pyramids/anterior multiple sclerosis.
cervicomedullary junction.13 These critical lesions likely have an important role in
● Multiple sclerosis lesions
the development of motor progression in patients with MS. Short lesions are less are usually wedge-shaped
common with AQP4-IgG–seropositive NMOSD, occurring in about 15%; African on axial images and involve
American ethnicity, tonic spasms, coexisting systemic autoimmunity, central the periphery of the cord in
lesions and lesions extending two or more vertebral segments, absence of MS brain either the lateral or dorsal
columns.
lesions, and lack of oligoclonal bands are factors that help identify those at highest
risk, in whom AQP4-IgG should be tested.33 One or more short lesions occur in
one-third to one-half of cases of myelitis with MOG-IgG–associated disorder, and
the presence of a coexisting longitudinally extensive lesion and the central location
of lesions help distinguish it from MS.34 Spinal cord sarcoidosis may also be
CONTINUUMJOURNAL.COM 69
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
associated with short T2-hyperintense lesions, but longitudinally extensive lesions
are more typical.20,35
LONGITUDINALLY EXTENSIVE T2-HYPERINTENSE LESIONS (THREE OR MORE VERTEBRAL
SEGMENTS). A myelitis episode accompanied by an isolated longitudinally
extensive T2-hyperintense lesion that extends over three or more vertebral
segments is typical of AQP4-IgG–seropositive NMOSD (FIGURES 3-1E and 3-1F)
TABLE 3-2 MRI Findings in Autoimmune Myelopathies and Mimics
Length on Appearance on
Typical sagittal axial
spinal Number of T2-weighted T2-weighted Postcontrast
location T2 lesions imagesa images pattern Other feature(s)
Inflammatory/autoimmune
Multiple sclerosis Cervical or Multiple Short Peripheral Ringlike,
thoracic (dorsal or lateral homogeneous
columns)
Aquaporin-4-IgG– Cervical or Single Long 85%; Central (gray and Ringlike, patchy Bright spotty
seropositive thoracic short 15% white matter) T2b, prominent
neuromyelitis swelling
optica spectrum
disorder (NMOSD)
Myelin Cervical or Multiple Long 70%; Central (30% gray Faint or no Conus
oligodendrocyte thoracic short 30% matter enhancement
glycoprotein–IgG- restricted/H
associated disorder signc)
Sarcoidosis Cervical or Single or, Usually long Central Almost universal: Swelling, may
thoracic less often, dorsal subpiald see enlarged
multifocal or axial tridente lymph nodes in
carina or hilum
on thoracic MRI
Paraneoplastic Cervical or Single Long Tract-specific Tract-specific MRI normal in up
thoracic signal (dorsal/ enhancement to 50%
lateral column) (usually lateral
columns)
CONTINUED ON PAGE 71
70 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
and supports this diagnosis over MS; AQP4-IgG–seropositive NMOSD is the
most common cause of both monophasic (50%) and recurrent (93%) LETM.36
AQP4-IgG–seropositive NMOSD myelitis lesions may also have pockets of signal
intensity similar to the CSF, which are called bright spotty lesions. Contrast
enhancement is detected in the vast majority of myelitis associated with AQP4-
IgG–seropositive NMOSD and is usually patchy, although ringlike lesions are
found in one-third, often forming a ring around the bright spotty T2
CONTINUED FROM PAGE 70
Length on Appearance on
Typical sagittal axial
spinal Number of T2-weighted T2-weighted Postcontrast
location T2 lesions imagesa images pattern Other feature(s)
Most common mimics of inflammatory/autoimmune myelopathy
Spondylosis Cervical Single Long or short Central owl eyef Sagittal: Cervical canal
pancakelikeg; stenosis, other
axial: spondylotic
circumferential changes; slow
sparing gray resolution of
matter enhancement
after surgery
(1-2 years)
Spinal cord infarct Cervical or Single Long or short Owl eyef Linear striph; Diffusion
thoracic owl eyef restriction;
vertebral body
infarct; adjacent
artery dissection
Dural arteriovenous Thoracic Single Long Central Patchy, missing Flow voids
fistula piece,i dorsal to cord
enhancing large
veins; 40% no
enhancement
Nutritional (vitamin Cervical or Single Long Tracts (dorsal/ None
B12 deficiency, thoracic lateral columns)
copper deficiency)
Intramedullary Cervical or Single or Long or short Central or Rim and flame or
metastases thoracic multiple peripheral dot signj
MRI = magnetic resonance imaging.
a
Short: less than three vertebral segments; long: three or more vertebral segments.
b
Very bright T2 hyperintensity similar in consistency to CSF (syrinxlike) spotted within less bright T2-hyperintense lesion.
c
T2 signal abnormality restricted to gray matter on axial image forming an H shape.
d
Parenchymal enhancement extending inward from the dorsal surface of the cord.
e
Dorsal subpial enhancement combined with central canal enhancement creates a three-pronged appearance on axial sequences resembling a
trident.
f
Bilateral anterior horn cell involvement with the appearance of owl eyes (or snake eyes).
g
Transverse band of enhancement in which the width is equal to or greater than the height that appears squashed like a pancake.
h
A linear strip of enhancement in the anterior cord on sagittal images.
i
Area of absent enhancement within a long segment of homogeneous enhancement appearing as if the enhancement has a missing piece.
j
A rim of enhancement around a less enhancing central region of milder enhancement with a flame appearance at the top or the bottom of the
lesion; may have an accompanying dot of enhancement in the center on axial or sagittal images.
CONTINUUMJOURNAL.COM 71
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
FIGURE 3-1
Comparison of acute myelitis MRI findings in multiple sclerosis, aquaporin-4 (AQP4) IgG–
seropositive neuromyelitis optica spectrum disorder (NMOSD), and myelin oligodendrocyte
glycoprotein autoantibody (MOG-IgG)–associated disorder. Sagittal MRI of an adult patient
with multiple sclerosis shows a short T2 hyperintensity at C2 extending 1.5 vertebral
segments in length (A, arrow). Axial image shows the lesion is located peripherally in the
right lateral column (B, arrow). Sagittal (C) and axial (D) images show accompanying ring
enhancement of the spinal cord lesion (C, D, arrows) on postcontrast T1-weighted images.
Sagittal (E) and axial (F) images of AQP4-IgG–seropositive NMOSD–associated myelitis
show a longitudinally extensive T2 hyperintense lesion extending more than three vertebral
segments (E, F, arrows). Accompanying ring enhancement of the cord lesion is seen on
sagittal (G, lower arrow) and axial (H, arrow) postcontrast T1-weighted images along with
more homogeneous enhancement (G, upper arrow). In myelitis accompanying MOG-IgG–
associated disorder, a longitudinally extensive T2-hyperintense lesion extending more than
three vertebral segments is seen on sagittal imaging (I, arrows). On axial images, the lesion
involves predominantly gray matter, forming an H sign (J, arrow). No postcontrast
enhancement is seen on postcontrast T1-weighted images (K, L).
hyperintensity.37 Long segments of atrophy extending over more than three
vertebral segments may also be encountered as the sequelae of one or more
myelitis attacks (FIGURES 3-2C and 3-2D).6 MOG-IgG–associated disorder
myelitis can occur in isolation but is more commonly seen with concomitant
involvement of the brain and brainstem as part of ADEM or concurrently with an
episode of optic neuritis. Myelitis is considered a core clinical feature of MOG-
IgG–associated disorder.38,39
72 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 3-2
Comparison of chronic myelitis MRI findings in multiple sclerosis, aquaporin-4-IgG
(AQP4-IgG)–seropositive neuromyelitis optica spectrum disorder (NMOSD), and myelin
oligodendrocyte glycoprotein antibody (MOG-IgG)–associated disorder. Sagittal
T2-weighted cervical spine MRI of a patient with multiple sclerosis with progressive left
hemiparesis attributable to a severe critical demyelinating lesion showing evidence of
prominent “apple-core” atrophy on sagittal images (A, arrow) and focal left lateral cord
atrophy on axial image (B, arrow). Sagittal T2-weighted cervical spine MRI of a patient with
multiple prior episodes of myelitis from AQP4-IgG–seropositive NMOSD who has a residual
paraplegia, showing a long segment of atrophy (C, arrows) extending over more than three
vertebral segments, with residual T2 hyperintensity centrally on axial image (D, arrow;
corresponding to level of upper arrow in panel C). Sagittal T2-weighted cervical spine MRI of
a patient in remission after multiple episodes of MOG-IgG–associated disorder myelitis,
without residual motor deficits, showing no residual T2 hyperintensity and minimal atrophy
on sagittal (E) and axial (F) images.
CONTINUUMJOURNAL.COM 73
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
Similar to AQP4-IgG–seropositive NMOSD, MOG-IgG–associated disorder
myelitis is frequently associated with LETM (lesions extending for three or more
vertebral segments) (FIGURE 3-1I), although often multifocal cord lesions are
seen rather than the solitary lesion typical of AQP4-IgG–seropositive NMOSD.40
Patients with MOG-IgG–associated disorder often have conus involvement.40,41
On axial sequences, lesions are usually central; in about one-third of patients,
they are restricted to the gray matter in an H pattern and accompanied by a
sagittal T2-hyperintense line (FIGURE 3-1J) (CASE 3-1). Recurrent isolated LETM
is rare with MOG-IgG–associated disorder.36 Gadolinium enhancement is less
frequent (<50% of cases) than in AQP4-IgG–seropositive NMOSD or MS
(FIGURE 3-1K and 3-1L).30,34,40 In MOG-IgG–associated disorder, T2 lesions often
resolve completely (FIGURES 3-2E and 3-2F). In AQP4-IgG–seropositive NMOSD,
T2 lesions markedly reduce in size with mild residual T2 hyperintensity in
most (FIGURE 3-2C), whereas in MS, lesions lead to a persistent residual T2
hyperintensity that is only mildly reduced from the acute lesion (FIGURES 3-2A
and 3-2B).
Gadolinium Enhancement Pattern
MS lesions may have homogeneous enhancement or ring enhancement or may
not enhance.29 AQP4-IgG–seropositive NMOSD can have ring enhancement that
may be elongated or ellipsoid in appearance, extending over multiple segments
(FIGURE 3-1G and 3-1H),37 although patchy nonspecific enhancement is most
common. With MOG-IgG–associated disorder, mild patchy enhancement or no
enhancement is typical, and ring enhancement is not usually encountered.
Paraneoplastic autoimmune myelopathies may reveal a characteristic
tract-specific enhancement along the lateral columns (or, less commonly, the
dorsal columns) (FIGURE 3-4) but can also be normal. Linear dorsal subpial
enhancement extending inward from the posterior aspect of the cord and
spanning over multiple vertebral segments is seen in approximately 60% of
cases of spinal cord sarcoidosis and can distinguish it from AQP4-IgG–
seropositive NMOSD or other causes of LETM.10,19,42 When this dorsal
subpial enhancement is accompanied by central canal enhancement, an axial
trident sign42 can be seen, which is very suggestive of spinal cord sarcoidosis
(CASE 3-2). Despite a longitudinally extensive T2 hyperintense lesion with
prominent swelling, the accompanying neurologic deficit is often mild in
neurosarcoidosis (mild weakness or sensory deficit), unlike in other etiologies
(eg, AQP4-IgG–seropositive NMOSD) in which a longitudinally extensive
T2-hyperintense lesion is typically accompanied by a severe deficit (eg,
paraplegia).10 Ventral subpial enhancement can also be encountered in a braid
pattern.43 Sarcoid myelitis lesions may occur around sites of mechanical stress
from spondylosis, potentially implicating the breakdown of the blood–spinal
cord barrier in its pathogenesis.10 Leptomeningeal enhancement may coexist
with dorsal subpial enhancement, but the dominant pattern in spinal cord
sarcoidosis is a parenchymal dorsal subpial enhancement. In Behçet disease,
myelitis lesions seen on MRI can be longitudinally extensive, short, or a
combination of both and may show a T2 lesion with a hypointense core and
hyperintense rim with or without enhancement of the rim in a bagel-like
pattern.44 The gadolinium enhancement pattern can also assist with identifying
noninflammatory myelopathies that are associated with enhancement
(TABLE 3-2).
74 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Other MRI features KEY POINTS
Patients with glycine and glutamic acid decarboxylase 65 (GAD 65)
● Short lesions are less
autoantibodies may present with a myelopathy as a component of common with AQP4-
encephalomyelitis or stiff person syndrome; in such cases, MRI of the spine is IgG–seropositive NMOSD,
often normal. With GFAP-antibody–associated encephalomyelitis, MRI shows occurring in about 15% of
poorly demarcated longitudinally extensive T2-hyperintense lesions with central patients.
canal enhancement in approximately 20% of cases, and meningeal involvement
● An isolated longitudinally
can be encountered, including along the cauda equina.45 extensive T2-hyperintense
lesion that extends over
MRI BRAIN. Obtaining an MRI of the brain is standard in the evaluation of three or more vertebral
autoimmune myelopathy, and the features of the lesions detected can help segments is typical of AQP4-
IgG–seropositive NMOSD
suggest the underlying diagnosis (FIGURE 3-6). The presence of characteristic MS and supports this diagnosis
lesions (peripheral brainstem, inferior temporal pole, ovoid periventricular, over MS.
ring/open-ring enhancement [FIGURES 3-6D, 3-6G, and 3-6J]) may allow patients
to meet MS diagnostic criteria, whereas the absence of brain lesions predicts a ● Similar to AQP4-
IgG–seropositive NMOSD,
low risk of MS over the next 15 years (<20%). With MS optic neuritis, optic nerve MOG-IgG–associated
enhancement tends to be short, involving less than 50% of the length of the optic disorder myelitis is
nerve (FIGURE 3-6A) versus AQP4-IgG–seropositive NMOSD or MOG- frequently associated with
antibody–associated disorder, in which enhancing lesions tend to extend more longitudinally extensive
transverse myelitis,
than half the length of the nerve. With AQP4-IgG–seropositive NMOSD, the
although often multifocal
presence of brain lesions adjacent to the third (FIGURE 3-6H) or fourth ventricle cord lesions are seen rather
(area postrema region [FIGURE 3-6E]), internal capsule, and splenium of the than the solitary lesion
corpus callosum (in a bridge arch pattern) and linear ependymal enhancement typical of AQP4-
IgG–seropositive NMOSD.
have all been reported as suggestive (FIGURE 3-6K), although in the majority, a
normal MRI head is found. Optic nerve lesions frequently involve the chiasm ● Patients with MOG-
(FIGURE 3-6B). With MOG-IgG–associated disorder, cerebral manifestations can IgG–associated disorder
reveal ADEM-like lesions, including multifocal white matter lesions, deep gray often have conus
matter lesions, and large fluffy brainstem lesions, and leptomeningeal involvement.
enhancement may be encountered (FIGURES 3-6F, 3-6I, and 3-6L). Parenchymal ● Linear dorsal subpial
lesions may or may not enhance, and a novel syndrome with unilateral cortical enhancement extending
encephalitis accompanied by fluid-attenuated inversion recovery (FLAIR)– inward from the posterior
hyperintense lesions in MOG-associated encephalitis with seizures (FLAMES) aspect of the cord and
spanning over multiple
has been reported with MOG-IgG–associated disorder.46,47 Optic nerve lesions
vertebral segments is seen
with MOG-IgG–associated disorder tend to be longitudinally extensive and often in approximately 60% of
involve the anterior optic pathway, sparing the chiasm (FIGURE 3-6C).48 ADEM cases of spinal cord
can be associated with lesions similar to those mentioned with MOG-IgG– sarcoidosis. When this
dorsal subpial enhancement
associated disorder, and up to 50% of patients with ADEM are MOG-IgG
is accompanied by central
seropositive. With GFAP antibody–associated encephalomyelitis, a characteristic canal enhancement, an axial
radial enhancement extending out from the ventricles has been reported. The trident sign can be seen,
presence of basilar leptomeningeal enhancement may suggest sarcoidosis, which is very suggestive of
although often brain MRI is normal with spinal cord sarcoidosis. With Behçet spinal cord sarcoidosis.
disease, brainstem and internal capsule lesions can be encountered, as can ● Obtaining an MRI of the
cerebral venous sinus thrombosis. brain is standard in the
evaluation of autoimmune
NEURAL AND NON-NEURAL AUTOANTIBODIES myelopathy, and the
features of the lesions
Serum and CSF biomarkers of myelitis discovered in the past 2 decades have detected can help suggest
aided in the diagnosis and understanding of the pathogenesis of myelitis. the underlying diagnosis.
AQP4-IgG is an antibody that binds to a water channel on the end feet of
astrocytes, whereas MOG-IgG binds the MOG protein on the surface of
oligodendrocytes. AQP4-IgG and MOG-IgG are two important antibody
CONTINUUMJOURNAL.COM 75
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
CASE 3-1 A 20-year old right-handed woman developed a sore throat, rhinorrhea,
and headache 5 days after receiving the injectable influenza vaccine.
Over the subsequent 3 to 4 days, she developed ascending numbness and
weakness in her lower extremities with difficulty urinating and the
Lhermitte phenomenon. At her neurologic nadir 7 days from onset, she
had weakness in both legs (resulting in wheelchair dependence), bilateral
numbness from her knees to toes, and urinary retention that required an
indwelling urinary catheter.
Neurologic examination at that time revealed a moderately severe
paraparesis with brisk reflexes in the lower extremities but downgoing
plantar responses. MRI of her spine revealed a multifocal T2 hyperintensity
within the cervical and thoracic spine (FIGURE 3-3) predominantly involving
the gray matter and forming a sagittal line (FIGURE 3-3A) and H sign (FIGURES 3-3B
and 3-3F) with minimal enhancement (FIGURES 3-3C, 3-3D, 3-3G, and 3-3H). Brain
MRI revealed some mild hazy central brainstem T2 hyperintensity without
enhancement (not shown) and was otherwise normal. CSF analysis revealed
an elevated white blood cell count of 101 cells/mm3, elevated protein of
68 mg/dL, normal glucose, and negative oligoclonal bands. Serum
aquaporin-4 (AQP4)-IgG was negative, but serum myelin oligodendrocyte
glycoprotein (MOG)-IgG was positive at high titer of 1:1000 (normal <1:20).
She was diagnosed with MOG-IgG–associated disorder and treated with
1 g IV methylprednisolone once daily for 5 days followed by an oral
prednisone taper over 3 weeks. She had an excellent recovery over the
subsequent 2 months and returned to running, although she had mild
residual bladder dysfunction. A watchful waiting approach was taken
without empiric attack-prevention immunosuppressant treatment.
COMMENT In this patient, the subacute onset of myelopathy reaching its nadir
between 1 and 21 days is suggestive of transverse myelitis, and the positive
MOG-IgG confirmed MOG-IgG–associated disorder, which can follow
vaccination. The MRI findings were very suggestive of MOG-IgG–
associated disorder, with a longitudinally extensive T2 hyperintensity with
mild swelling (FIGURE 3-3A), multifocal T2 hyperintensity in the cord
(FIGURES 3-3A and 3-3E), conus involvement (FIGURE 3-3E), predominantly gray
matter T2 hyperintensity (FIGURES 3-3A, 3-3B, and 3-3F), and minimal
gadolinium enhancement (FIGURES 3-3C, 3-3D, 3-3G and 3-3H), compared to
AQP4-IgG–seropositive neuromyelitis optica spectrum disorder (NMOSD),
which usually has a solitary longitudinally extensive T2 hyperintensity, more
severe swelling, and more avid enhancement. The severity of the episode
at nadir (requiring a wheelchair), longitudinally extensive T2 hyperintensity,
absence of oligoclonal bands, and elevated white blood cell count
(>50 cells/mm3) favored MOG-IgG–associated disorder over multiple
sclerosis. The excellent recovery with acute treatment is typical of MOG-
IgG–associated disorder, which responds to treatment better than AQP4-
IgG–seropositive NMOSD. As the disease can be monophasic, empiric
attack-prevention immunosuppression is typically reserved for cases that
relapse.
76 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 3-3
Imaging of the patient in CASE 3-1. Sagittal T2-weighted cervical spine MRI shows a
longitudinally extensive T2 hyperintensity that forms a sagittal line (A, lower two arrows)
with additional T2 hyperintensity above (A, upper arrow). Axial T2-weighted image shows
predominantly gray matter T2 hyperintensity that forms an H sign (B, arrow). No gadolinium
enhancement is appreciable on sagittal postcontrast T1-weighted image (C), and minimal
gadolinium enhancement is seen on axial postcontrast T1-weighted image (D, arrow).
Sagittal T2-weighted MRI of the thoracic spine reveals a short T2 hyperintensity in the upper
thoracic/lower cervical cord (E, upper arrow) and a separate T2 hyperintensity in the conus
(E, lower arrow). Axial T2-weighted image shows the lesion to be central, forming an H sign
(F, arrow); no definitive accompanying enhancement is seen on sagittal (G) or axial (H)
postcontrast T1-weighted images.
CONTINUUMJOURNAL.COM 77
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
FIGURE 3-4
MRI findings in paraneoplastic myelopathy. Sagittal T2-weighted thoracic spine image shows
longitudinally extensive T2 signal abnormality (A, arrows) extending over seven spinal
segments with associated gadolinium enhancement (B, arrows) on sagittal postcontrast
T1-weighted image. Axial T2-weighted image shows symmetric tract-specific T2 signal
abnormality (lateral columns) (C, arrows) that enhances after gadolinium administration on
axial post contrast T1-weighted image (D, arrows).
Modified with permission from Flanagan EP, et al, Neurology.9 © 2011 American Academy of Neurology.
biomarkers of transverse myelitis that should be tested in patients in whom
the clinical and paraclinical findings are not suggestive of MS (eg, LETM).
AQP4-IgG–seropositive NMOSD is found in up to 50% of patients with LETM
and 90% of patients with recurrent LETM, and it may occur in conjunction with
or be preceded by optic neuritis or area postrema syndrome.36 The myelitis of
MOG-IgG–associated disorder may occur in isolation, as a component of ADEM,
or in conjunction with optic neuritis and accounts for 20% to 30% of NMOSD
syndromes negative for AQP4-IgG.40 For detection of AQP4-IgG and MOG-IgG,
serum yields the optimal sensitivity (more so than CSF) and cell-based assays
are the most reliable; CSF can be considered in highly suspicious cases if serum is
negative. Rare cases of isolated MOG-IgG CSF positivity have been reported.49
Testing before immunotherapy (eg, plasma exchange) is important to reduce
the risk of false negatives. Low-positive MOG-IgG results should be viewed
with caution as false positives can occur, particularly when ordered in
low-probability situations (eg, patients with classic clinical, radiologic, and
CSF features of MS), and the positive MOG-IgG test result should not replace
clinical judgment. With AQP4-IgG cell-based assays, false positives are
extremely rare, although with older-generation techniques (eg, enzyme-linked
immunosorbent assay [ELISA]), false positives at low titer can be found.50
Detection of AQP4-IgG in a patient with transverse myelitis predicts substantial
risk of further relapses (>90%) and warrants lifelong immunotherapy; repeat
AQP4-IgG titers are generally not useful. Repeating MOG-IgG serology may
help predict the risk of recurrence as transient seropositivity is more associated
with a monophasic course.39,40 AQP4-IgG may coexist with other neural
autoantibodies (or their respective syndromes), including N-methyl-D-aspartate
(NMDA) receptor-IgG (anti-NMDA receptor encephalitis) and GFAP-IgG
(meningoencephalomyelitis), often with an accompanying teratoma. Muscle
78 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
acetylcholine receptor–binding antibodies and a clinical syndrome of KEY POINTS
myasthenia gravis may also occur.17 However, AQP4-IgG coexisting with
● AQP4-IgG and MOG-IgG
MOG-IgG is exceedingly rare (0.06%).51 MOG-IgG and NMDA receptor–IgG are two important antibody
also coexist more frequently than expected. Several neural autoantibodies biomarkers of transverse
are associated with paraneoplastic myelopathies, and the most commonly myelitis that should be
encountered are amphiphysin52 and collapsin response mediator protein-5 tested in patients with
transverse myelitis in whom
(CRMP-5)-IgG/anti-CV2.
the clinical and paraclinical
GFAP-IgG appears to be a marker of a meningoencephalomyelitis, and findings are not suggestive
CSF analysis yields optimal sensitivity and specificity. Glycine receptor of MS.
α1 subunit (GlyRα1)-IgG, GAD 65–IgG (neurologic disease is usually associated
with high titers and detection in CSF), and adaptor protein-3B2(AP3B2)–IgG are ● For AQP4-IgG and
MOG-IgG, serum yields the
also associated with autoimmune or paraneoplastic myelopathies.53,54 optimal sensitivity (more so
Myelitis has been recently described accompanying a cerebellitis and than CSF) and cell-based
brainstem encephalitis in a patient with neurochondrin-IgG.55 Myelitis has assays are the most reliable.
also been reported in patients with autoantibodies specific for the neuronal
● Care is needed with
(type 1) isoform of the ubiquitously expressed inositol trisphosphate receptor low-positive MOG-IgG
(ITPR1),56 typically accompanying cerebellitis and neuropathy and rarely in results as false positives can
isolation. Myelopathy has also been reported coexisting with encephalopathy occur, particularly when
and cerebellar ataxia in patients with neuronal intermediate filament ordered in low-probability
situations, and the positive
NfL-IgG.57
MOG-IgG test result should
Testing serum for antinuclear antibody, double-stranded DNA antibodies, not replace clinical
Sjögren syndrome A (SSA)/Sjögren syndrome B (SSB), cytoplasmic judgment.
antineutrophil cytoplasmic antibody (c-ANCA) and perinuclear antineutrophil
cytoplasmic antibody (p-ANCA), other antibodies to the extractable nuclear ● With AQP4-IgG
cell-based assays, false
antigen, C3/C4 complement, antiphospholipid antibodies, β2 glycoprotein-1 positives are extremely rare,
autoantibodies, and lupus anticoagulant should be considered as part of although with older-
laboratory testing in a patient with suspected myelitis. Although inflammatory generation techniques, false
myelitis has been reported in patients with systemic lupus erythematosus and positives at low titer can be
found.
Sjögren syndrome or with serologic markers of those disorders, it is crucial to test
such patients for AQP4-IgG. It is now recognized that AQP4-IgG–seropositive ● Several neural
NMOSD may coexist with these disorders, and seropositivity for AQP4-IgG autoantibodies are
confirms the NMOSD diagnosis rather than the myelitis being a manifestation of associated with
paraneoplastic
the connective tissue disease; such patients require specific treatment for
myelopathies, and the most
NMOSD.58 Indeed, antiphospholipid antibodies frequently coexist with commonly encountered are
AQP4-IgG–seropositive NMOSD, and patients may be at higher risk of deep amphiphysin and collapsin
venous thrombosis.58 response mediator protein-5
(CRMP-5)/anti-CV2.
CSF ANALYSIS ● The majority of
The basic parameters of CSF (white and red blood cell counts, protein, autoimmune/inflammatory
glucose, and oligoclonal bands/IgG index) are helpful to show evidence of myelitis episodes will be
inflammation. The majority of autoimmune/inflammatory myelitis episodes accompanied by an elevated
CSF white blood cell count,
will be accompanied by an elevated CSF white blood cell count, and its and its absence should at
absence should at least raise consideration of alternative etiologies (eg, least raise consideration of
vascular myelopathies). A normal cell count with a markedly elevated CSF alternative etiologies (eg,
protein may suggest a spinal block, which can occur with spondylosis or tumor vascular myelopathies).
but should also lead to reconsideration of a peripheral cause (eg, Guillain-Barré
syndrome). With MS myelitis, the CSF white blood cell count is usually
less than 50 cells/mm3 and 85% of patients will have elevated oligoclonal bands or
IgG index. With MOG-IgG–associated disorder, AQP4-IgG–seropositive
NMOSD, and GFAP antibody–associated encephalomyelitis, the range in CSF
CONTINUUMJOURNAL.COM 79
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
CASE 3-2 A previously healthy 38-year-old man presented with numbness affecting
the trunk and painful dysesthesia involving both upper extremities, which
were followed by urinary retention, with symptoms worsening over the
course of 6 weeks. He had no other systemic symptoms.
Neurologic examination revealed a mild upper motor neuron pattern of
weakness affecting both upper extremities and abnormal proprioception
in the hands bilaterally but was otherwise normal. MRI of the cervical
spine showed a longitudinally extensive T2-hyperintense abnormality in
the cervical spine from C3 through T1 (FIGURES 3-5A and 3-5B), with dorsal
subpial (FIGURE 3-5C) and central canal (FIGURE 3-5C) gadolinium
enhancement forming a trident pattern on axial sequences, suggestive of
spinal cord sarcoidosis (FIGURE 3-5D). CSF analysis showed 67 total
nucleated cells/mm3 (normal 0 cells/mm3 to 5 cells/mm3) of which 89%
were lymphocytes, a mildly elevated protein at 50 mg/dL, a normal
glucose, and no oligoclonal bands. Testing for aquaporin-4 (AQP4)-IgG,
myelin oligodendrocyte glycoprotein (MOG)-IgG, antinuclear antibodies,
angiotensin-converting enzyme, vitamin B12, copper, and syphilis and
Lyme serologies were negative. CT of the chest was reported as negative
for malignancy or other abnormalities but fludeoxyglucose positron
emission tomography (FDG-PET) with CT showed increased glucose
uptake in the subcarinal, precarinal, and bilateral hilar nodes (FIGURE 3-5E),
and biopsy revealed non-necrotizing granulomatous inflammation.
Extensive testing for fungal and bacterial etiologies, including
tuberculosis, were negative.
The patient was treated with IV methylprednisolone (1 g/d for 5 days)
and transitioned to a prolonged oral steroid taper for 12 weeks. After
36 months of follow-up, no recurrence of enhancing lesions was seen and
the patient’s urinary retention had resolved, but he continued to have
residual allodynia in the upper limbs that responded poorly to multiple
neuropathic pain medications.
COMMENT The yield of PET-CT imaging may be higher than CT alone and should be
considered in the evaluation for neurosarcoidosis as it can help identify
potential sites for biopsy. The presence of gadolinium enhancement
involving the central canal and the dorsal subpial region forming a trident
pattern on axial images should raise suspicion for neurosarcoidosis.
Chronic neuropathic pain may be refractory to neuropathic medications
and is a common residuum of spinal cord sarcoidosis.
80 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 3-5
Imaging of the patient in CASE 3-2. A, Sagittal
T2-weighted cervical spine MRI shows a
longitudinally extensive T2 hyperintensity
(arrows). B, Axial T2-weighted image shows T2
hyperintensity in the central aspect of the cord
with edema (arrow). C, Sagittal postcontrast
T1-weighted image shows central (arrowhead )
and dorsal (arrows) subpial enhancement. D,
Axial postcontrast T1-weighted image shows a
characteristic trident sign (arrow). E, Increased
fludeoxyglucose positron emission tomography
(FDG-PET)/CT shows uptake in the subcarinal
nodes, precarinal nodes, and bilateral hilar
nodes (arrows).
CONTINUUMJOURNAL.COM 81
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
FIGURE 3-6
Comparison of brain MRI in multiple sclerosis (MS), aquaporin-4–IgG (AQP4-IgG)–seropositive
neuromyelitis optica spectrum disorder (NMOSD), and myelin oligodendrocyte glycoprotein
antibody (MOG-IgG)–associated disorder. Axial postcontrast T1-weighted MRIs show optic nerve
enhancement extending less than half the length of the nerve in a patient with MS (A, arrow),
whereas AQP4-IgG–seropositive NMOSD has a predilection for the optic chiasm (B, arrows) and
MOG-IgG–associated disorder is typically associated with bilateral anterior optic nerve pathway
enhancement extending more than half the length of the optic nerve (C, arrows). Axial
fluid-attenuated inversion recovery (FLAIR) images reveal peripheral small T2-hyperintense
lesions in the dorsal pons typical of MS (D, arrow); an additional characteristic inferior temporal
pole lesion of MS is also noted (D, arrowhead); a peri–fourth ventricle/area postrema
T2-hyperintense lesion is seen in the patient with AQP4-IgG–seropositive NMOSD (E, arrow),
whereas bilateral fluffy middle cerebellar peduncle T2-hyperintense lesions are typical of
MOG-IgG–associated disorder (F, arrows). Axial FLAIR MRIs reveal typical ovoid periventricular
lesions in MS (G, arrows), a peri–third ventricle hyperintense lesion in AQP4-IgG–seropositive
NMOSD (H, arrow), and characteristic deep gray matter (bithalamic) hyperintense lesions in
MOG-IgG–associated disorder (I, arrows). Axial postcontrast T1-weighted images show multiple
enhancing lesions typical of MS (J), linear ependymal enhancement occasionally encountered
with AQP4-IgG-seropositive NMOSD (K, arrow), and prominent enhancing vessels in MOG-
IgG–associated disorder (L, arrows).
82 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
white cell count is wider and can be between 0 cells/mm3 and 1000 cells/mm3.
Most inflammatory/autoimmune myelitis episodes are accompanied by a
lymphocytic predominance. AQP4-IgG–seropositive NMOSD can be
associated with a neutrophilic or eosinophilic predominance, whereas
neutrophilic predominance is associated with Behçet disease. Oligoclonal
bands are uncommon with AQP4-IgG–seropositive NMOSD (<30% of
patients) and very rare with MOG-IgG–associated disorder (<10% of
patients). Spinal cord sarcoidosis is almost always associated with an
elevated white blood cell count, although low glucose is rare; if present,
low glucose suggests a coexisting sarcoid meningitis. Experimental studies
have shown that CSF GFAP is elevated (reflective of astrocytic damage) in
AQP4-IgG–seropositive NMOSD, whereas elevated myelin basic protein
(reflective of oligodendrocyte damage) is recognized with MOG-
IgG–associated disorder.59,60 A lymphocytic pleocytosis is encountered in
approximately two-thirds of paraneoplastic myelitis.9 CSF angiotensin-
converting enzyme lacks sensitivity and specificity for sarcoidosis diagnosis
and is of limited use.
Occasionally, mild elevations in white blood cell count may be encountered
in noninflammatory/autoimmune myelopathies (eg, spinal cord infarct),
perhaps from secondary inflammation or breakdown of the blood–spinal
cord barrier, and should not dissuade from those diagnoses in the correct
clinical context.
CSF testing is also useful to assess for mimics of autoimmune myelitis.
Testing with polymerase chain reaction (PCR) in CSF for herpes simplex
virus type 1, herpes simplex virus type 2 (associated with the lumbar
myeloradiculitis of Elsberg syndrome), varicella-zoster virus,
cytomegalovirus, and JC virus (rarely associated with myelopathy) or
next-generation sequencing can be considered. CSF cytology and flow
cytometry, and MYD88 L265P mutation (L265P is a missense mutation changing
leucine at position 265 to proline in MYD88, identified in approximately 90%
of cases of Waldenström macroglobulinemia and in significant proportions of
cases of activated diffuse large B-cell lymphomas and IgM monoclonal gammopathy
of undetermined significance) are helpful in the evaluation of suspected
lymphoproliferative disorders.61
OTHER TESTING
In cases of suspected neurosarcoidosis, chest x-ray is insensitive and CT chest
is 73% sensitive; however, FDG-PET/CT has higher sensitivity (88%) and is
useful in selected cases (CASE 3-2; FIGURE 3-5E).1,8,19 CT body is considered
first line in assessing for malignancy accompanying a paraneoplastic
myelopathy, but PET-CT offers better sensitivity if suspicion is high;
mammogram is also useful.62 Searching for cancer is also recommended in older
patients (≥50 years) with AQP4-IgG–seropositive NMOSD as it is recognized to
occur occasionally in a paraneoplastic context.63 Somatosensory evoked
potentials may be helpful for patients who cannot undergo MRI. In patients with
clinical and radiologic progression despite immunotherapy, the diagnosis of an
autoimmune myelitis should be reconsidered. Spinal cord biopsy is considered a
last resort; however, in one study at a tertiary referral center it helped guide
specific treatment in 26% of patients with a morbidity of 21%, although
permanent deficits were rare (<5%).64
CONTINUUMJOURNAL.COM 83
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
FIGURE 3-7
Mimics of inflammatory/autoimmune myelitis. Sagittal T2-weighted cervical spine MRI shows
T2 hyperintensity extending from C5 through C7 in the anterior aspect of the cord (A, arrows);
axial T2-weighted MRI shows involvement of the anterior horn cells in a snake-eye pattern
(B, arrows), consistent with spinal cord infarct. Sagittal T2-weighted cervical spine MRI
shows T2 hyperintensity in the dorsal cord extending from C2 through C4 (C, arrows); axial
T2-weighted image shows involvement of the dorsal cord (D, arrow), consistent with
vitamin B12 deficiency. Sagittal T2-weighted thoracic spine MRI shows a longitudinally
extensive T2 hyperintensity extending from the upper thoracic cord to the conus (E, arrows);
axial T2-weighted image shows involvement of the central cord (F, arrow) that was
eventually confirmed to be a dural arteriovenous fistula despite the lack of evident flow
voids. Sagittal T2-weighted thoracic spine MRI shows a longitudinally extensive T2 hyperintensity
in the thoracic cord (G, arrows); axial T2-weighted image shows that the lesion is central
(H, arrow). Sagittal (I) and axial (J) postcontrast T1-weighted images show a rim of
enhancement (I, J, arrowheads) around a less enhancing center with a flame pattern at the
top and bottom of the lesion (I, arrow), a pattern that is highly characteristic of spinal
cord intramedullary metastasis.
Panels A and B modified with permission from Flanagan EP, Pittock SJ, Handb Clin Neurol.24 © 2017 Elsevier BV.
84 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
DIFFERENTIAL DIAGNOSIS KEY POINTS
Understanding the differential diagnosis of autoimmune/inflammatory myelopathy
● Understanding the
is crucial as many diagnostic pitfalls can lead the clinician to the wrong diagnosis. As differential diagnosis of
outlined previously, the time to nadir and speed of onset are crucial in narrowing the autoimmune/inflammatory
differential diagnosis. MRI attributes, particularly the gadolinium enhancement myelopathy is crucial as
patterns, are also extremely useful in determining the cause of the myelopathy many diagnostic pitfalls can
lead the clinician to the
(TABLE 3-1, TABLE 3-2, and FIGURE 3-7). An example of a noninflammatory
wrong diagnosis.
myelopathy mimicking an inflammatory myelopathy is outlined in CASE 3-3 and
illustrated in the accompanying FIGURE 3-8. FIGURE 3-9 is a pictorial summary of ● For most
the useful T2 signal and enhancement patterns accompanying myelopathies with autoimmune/inflammatory
longitudinally extensive lesions clinicians should be aware of. myelopathies, after
reasonable exclusion of
alternative etiologies such
ACUTE TREATMENT as extrinsic compression,
For most autoimmune/inflammatory myelopathies, after reasonable spinal cord infarction, and
exclusion of alternative etiologies such as extrinsic compression, spinal cord infections, expert
consensus recommends
infarction, and infections, expert consensus recommends prompt prompt administration of
administration of high-dose IV corticosteroids with 1 g IV methylprednisolone high-dose IV corticosteroids
once daily for 5 days. Treatment should not be withheld while waiting for with 1 g IV
results of antibody testing. In patients with myelitis as a manifestation of CNS methylprednisolone once
daily for 5 days.
inflammatory demyelinating disease (eg, MS, AQP4-IgG–seropositive
NMOSD, MOG-IgG–associated disorder, ADEM, idiopathic transverse ● In patients with myelitis
myelitis) with severe neurologic deficits despite steroids, plasma exchange as a manifestation of central
should be considered, as a randomized sham-controlled trial showed benefit nervous system
inflammatory demyelinating
of plasma exchange in patients with inflammatory CNS demyelinating disease
disease with severe
with ongoing impairment after high-dose corticosteroids.67-69 In children with neurologic deficits despite
MOG-IgG–associated disorder, IV immunoglobulin (IVIg) has been used in steroids, plasma exchange
the acute setting with good success, and a steroid taper over the course of 6 to should be considered.
12 weeks may be considered after an acute MOG-IgG–associated disorder
attack to prevent early relapse. Supportive care is focused on preventing
complications, with early implementation of frequent bladder scans,
intermittent catheterization or temporary indwelling catheter placement, and
prevention of deep venous thrombosis and decubitus ulcers. Depending on
the etiology of the myelopathy, chronic maintenance treatments may be
implemented to prevent future relapses.
MAINTENANCE AND ATTACK-PREVENTION IMMUNOTHERAPY
A comprehensive review of all the medications used as maintenance therapies
for autoimmune and inflammatory myelopathies, dosing, and side effects is
beyond the scope of this article, but a brief summary is provided here. Several
disease-modifying therapies are approved for relapsing-remitting and
progressive forms of MS.70 Long-term immunosuppression is recommended
in all patients with AQP4-IgG–seropositive NMOSD, as attacks can be very
severe. Historically, treatments included azathioprine and mycophenolate
mofetil, but these lacked clinical trial evidence. Recently, four randomized
controlled phase 3 clinical trials for relapse prevention in NMOSD (which
included predominantly AQP4-IgG–seropositive cases) showed efficacy for
four novel treatments in preventing attacks. The treatments tested included
eculizumab, which targets the terminal complement component C571;
inebilizumab, which antagonizes CD19, depleting B cells and plasmablasts72;
rituximab, which blocks CD20, depleting B cells73; and satralizumab, which
CONTINUUMJOURNAL.COM 85
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
CASE 3-3 A 35-year-old man presented with subacute paresthesia initially affecting
the right arm, which had spread over the course of 5 weeks to include the
left arm symmetrically up to the midforearm. He had progressed despite
treatment for presumed bilateral carpal tunnel syndrome. Six months
later, he was involved in a motor vehicle accident and subsequently
developed a progressive gait disorder, with right leg weakness and
frequent falls. MRI of his cervical spine was abnormal, showing a
longitudinally extensive T2 hyperintensity (FIGURE 3-8A) centrally located
on axial imaging (FIGURE 3-8B), associated with a pancakelike transverse
band of enhancement in which the width was equal to the height at C5-C6
(FIGURE 3-8C). On axial images, the enhancement involved the white matter
and spared the gray matter (FIGURE 3-8D). Moderate to severe
degenerative disk disease was also noted. CSF showed a normal white
blood cell count, red blood cell count, and glucose; a mildly elevated
protein of 66 mg/dL; and negative oligoclonal bands and IgG index.
Extensive serologic testing for infectious and autoimmune causes of
myelopathy were negative, including aquaporin-4 (AQP4)–IgG and myelin
oligodendrocyte glycoprotein (MOG)–IgG. Brain MRI and optical
coherence tomography were normal. The patient was diagnosed with
seronegative neuromyelitis optica spectrum disorder (NMOSD) and
received treatment with IV methylprednisolone daily for 5 days, but his
sensory symptoms progressed, gait dysfunction worsened, and urinary
frequency and erectile dysfunction ensued.
A second neurologic opinion was sought. Neurologic examination
showed an upper motor neuron pattern of weakness affecting the right
upper extremity and diffuse hyperreflexia, a positive Hoffman sign on the
right, and bilateral extensor plantar responses. His gait was broad based,
and a positive Romberg sign was noted. A diagnosis of cervical
spondylotic myelopathy was established based on the characteristic
presentation and imaging findings. The patient underwent cervical
decompression surgery, after which his symptoms improved.
COMMENT Spondylotic myelopathy can be associated with gadolinium enhancement
in 7% of patients, and its presence often leads to diagnostic confusion
and suspicion for a primary inflammatory or neoplastic etiology. The
progressive myelopathy following trauma and absence of CSF
inflammation were atypical for inflammatory myelopathy. The pattern of
gadolinium enhancement characterized by a pancakelike transverse band
of enhancement on sagittal images and sparing of the gray matter on
axial images is highly suggestive of spondylotic myelopathy.65 The
accompanying stenosis may appear only moderate in the neutral position,
and dynamic flexion-extension MRI views may help in selected cases as
compression often becomes more apparent during extension.66
86 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 3-8
Imaging of the patient in CASE 3-3. Sagittal
T2-weighted cervical spine MRI shows a
longitudinally extensive hyperintensity in the
cervical cord (A, arrows), which on axial
T2-weighted images is central (B, arrow). Sagittal
postcontrast T1-weighted image (C) reveals
evidence of a pancakelike transverse band of
enhancement at the C5-C6 interspace where the
width is equal to the height. Axial postcontrast
T1-weighted image shows enhancement of the
white matter sparing the gray matter (D, arrows),
highly consistent with the specific pattern of
enhancement seen with cervical spondylotic
myelopathy.
CONTINUUMJOURNAL.COM 87
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
FIGURE 3-9
Distinctive imaging features and patterns of enhancement with myelopathies accompanied by
longitudinally extensive T2 lesions. The sagittal and axial images depict the typical lesion patterns
on T2-weighted images (shown in light red) and postcontrast T1-weighted images (enhancement
after contrast is shown in dark red). For each panel, the T2 sequences are shown on the left and
postcontrast T1 sequences are shown on the right. A, Aquaporin-4 (AQP4)-IgG–seropositive
neuromyelitis optica spectrum disorder (NMOSD) myelitis on sagittal cervical spine images typically
reveals a solitary T2-hyperintense lesion that is central on axial sequences and extends over three
or more vertebral segments, with contrast enhancement sometimes having a ringlike appearance.
B, Myelin oligodendrocyte glycoprotein (MOG)-IgG–associated disorder myelitis on cervicothoracic
cord images typically shows multifocal T2-hyperintense lesions with one or more longitudinally
extensive T2 lesions and a predilection for the conus. The T2 lesions are generally central on axial
sequences and in about one-third of patients will be restricted to the gray matter, forming an H
pattern. Contrast enhancement is infrequent; if present, it is usually faint. C, Neurosarcoidosis myelitis
in the cervical spine shows a typical nonspecific longitudinally extensive T2-hyperintense lesion that is
central on axial images. Postcontrast images show hallmark linear dorsal subpial enhancement with
some accompanying central canal enhancement, with the combination forming an axial trident sign.
D, Paraneoplastic myelopathy in the cervical spine shows the typical longitudinally extensive T2 signal
abnormality with a tractopathy on axial images confirmed by the presence of symmetric tract-specific
T2 hyperintensity and enhancement restricted to the dorsal columns or lateral columns, or both. E,
Spinal cord infarction in anterior spinal artery territory reveals the typical pencillike linear anterior cord
longitudinally extensive T2 hyperintensity with a partial linear strip of enhancement with contrast. On
axial T2 and postcontrast images, the anterior horn cells are preferentially affected in an owl-eye
or snake-eye pattern; occasionally (in approximately 10%), a vertebral body infarct can ensue, as
shown here. F, Cervical spondylotic myelopathy with sagittal imaging showing spondylosis and a
spindle-shaped T2 hyperintensity extending more than three vertebral segments, with a characteristic
flat pancakelike transverse band of enhancement just below the site of maximum stenosis on
postcontrast images. On axial images, the enhancement typically involves the white matter but spares
the gray matter. G, Intramedullary spinal cord metastasis reveals a longitudinally extensive T2
hyperintensity with an enhancing intramedullary mass with the hallmark thin rim of more intense
enhancement (the rim sign) accompanied by an ill-defined flame-shaped region of enhancement at its
superior and inferior margins with a central dot (the dot sign) occasionally noted on postcontrast
images, as shown here. H, Spinal dural arteriovenous fistula reveals the typical thoracic longitudinally
extensive T2 hyperintensity extending to the conus with prominent flow voids and contrast
enhancement and a characteristic “missing piece” of enhancement sometimes noted, as shown here.
88 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
targets interleukin-6, involved in the plasmablast pathway.74 Transitional
low-dose prednisone (10 mg to 20 mg orally daily) for up to 1 month is often
used while the B-cell–depleting treatment takes effect. No randomized
controlled trials have been conducted for MOG-IgG–associated disorder, and
the role of immunotherapy after an initial episode of transverse myelitis
related to MOG-IgG–associated disorder remains to be determined. As
MOG-IgG–associated disorder may be monophasic, the current approach is
generally not to treat after a single attack and generally to restrict maintenance
immunotherapy to patients who relapse. Although the long-term outcome
is generally favorable in MOG-IgG–associated disorder, the accumulation of
mild disability with each attack supports the need for maintenance
immunotherapies in this disease.75 In the absence of clinical trial evidence in
MOG-IgG–associated disorder, consideration can be given to empiric
mycophenolate mofetil, azathioprine, rituximab, and intermittent IVIg.76 For
GFAP antibody–associated encephalomyelitis, a brisk response to steroids is
characteristic, but relapses can occur, and prolonged administration of steroids
or additional immunotherapy such as mycophenolate mofetil may be required in
some cases.45
Spinal cord sarcoidosis is usually treated with high-dose IV steroids
followed by prolonged high-dose oral corticosteroids (eg, prednisone
1 mg/kg/d for 3 months followed by a prolonged taper over the subsequent
6 to 12 months); steroid prophylaxis with trimethoprim-sulfamethoxazole
(one single-strength tablet daily or one double-strength tablet 3 times
a week) is recommended in any patients on more than 20 mg/d prednisone
for more than 5 weeks. In addition, calcium and vitamin D supplementation
and monitoring of bone density are recommended and gastrointestinal
prophylaxis should be considered. Administration of other medications,
such as infliximab, may be considered in those with severe disease or those
who are intolerant to steroids. Steroid-sparing medications, including
methotrexate, azathioprine, and mycophenolate mofetil, have been used in
patients with spinal cord sarcoidosis who relapse or develop recurrence on
weaning off steroids but may also be considered from onset to reduce the
risk of relapse.77
CONCLUSION
Autoimmune myelopathies are a heterogeneous group of spinal cord disorders
unified by their immune-mediated mechanism and potential for response to
immunotherapy. The time course of development of neurologic symptoms is
crucial in determining the likely etiology of a myelopathy, and autoimmune
myelopathies are usually subacute in onset. Immune-mediated myelopathies
may be monophasic or the initial manifestation of a relapsing disorder (eg, MS,
NMOSD); ancillary testing, particularly MRI, serologic antibody biomarkers, and
CSF analysis, can help determine a specific diagnosis and the correct treatment
approach and assist with prognosis. Idiopathic transverse myelitis should be
considered a diagnosis of exclusion and should only be assigned once a
comprehensive search for alternative etiologies has been completed. Timely
administration of acute treatment is critical to help stabilize and improve
symptoms while maintenance immunotherapy decisions are based on the
underlying etiology found.
CONTINUUMJOURNAL.COM 89
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
REFERENCES
1 Flanagan EP. Autoimmune myelopathies. Handb 14 Sechi E, Keegan BM, Kaufmann TJ, et al. Unilateral
Clin Neurol 2016;133:327-351. doi:10.1016/B978-0- motor progression in MS: association with a
444-63432-0.00019-0 critical corticospinal tract lesion. Neurology
2019;93(7):e628-e634. doi:10.1212/WNL.
2 Zalewski NL, Flanagan EP, Keegan BM. Evaluation
0000000000007944
of idiopathic transverse myelitis revealing
specific myelopathy diagnoses. Neurology 15 Flanagan EP, Hinson SR, Lennon VA, et al. Glial
2018;90(2):e96-e102. doi:10.1212/ fibrillary acidic protein immunoglobulin G as
WNL.0000000000004796 biomarker of autoimmune astrocytopathy:
analysis of 102 patients. Ann Neurol 2017;81(2):
3 Barreras P, Fitzgerald KC, Mealy MA, et al. Clinical
298-309. doi:10.1002/ana.24881
biomarkers differentiate myelitis from vascular
and other causes of myelopathy. Neurology 16 Lee CH, Bharwani L, Sullivan T. Paraneoplastic
2018;90(1):e12-e21. doi:10.1212/WNL. necrotizing myelopathy in a patient with newly
0000000000004765 diagnosed diffuse large B cell lymphoma. World J
4 Barnes G, Benjamin S, Bowen JD, et al. Proposed Oncol 2011;2:195-198. doi:10.4021/wjon279w
diagnostic criteria and nosology of acute 17 Flanagan EP. Neuromyelitis optica spectrum
transverse myelitis. Neurology 2002;59(4): disorder and other non–multiple sclerosis central
499-505. doi:10.1212/wnl.59.4.499 nervous system inflammatory diseases.
5 Sechi E, Shosha E, Williams JP, et al. Aquaporin-4 Continuum (Minneap Minn) 2019;25(3):815-844.
and MOG autoantibody discovery in idiopathic doi:10.1212/CON.0000000000000742
transverse myelitis epidemiology. Neurology 18 Flanagan EP, Keegan BM. Paraneoplastic
2019;93(4):e414-e420 doi:10.1212/WNL. myelopathy. Neurol Clin 2013;31(1):307-318.
0000000000007828 doi:10.1016/j.ncl.2012.09.001
6 Geraldes R, Ciccarelli O, Barkhof F, et al. The 19 Flanagan EP, Kaufmann TJ, Krecke KN, et al.
current role of MRI in differentiating multiple Discriminating long myelitis of neuromyelitis
sclerosis from its imaging mimics. Nat Rev Neurol optica from sarcoidosis. Ann Neurol 2016;79(3):
2018;14(4):199-213. doi:10.1038/nrneurol.2018.14 437-447. doi:10.1002/ana.24582
7 Reindl M, Waters P. Myelin oligodendrocyte 20 Salvarani C, Brown RD, Calamia KT, et al. Primary
glycoprotein antibodies in neurological disease. CNS vasculitis with spinal cord involvement.
Nat Rev Neurol 2019;15(2):89-102. doi:10.1038/ Neurology 2008;70(24 pt 2):2394-2400.
s41582-018-0112-x doi:10.1212/01.wnl.0000314687.69681.24
8 Zalewski NL, Flanagan EP. Autoimmune and 21 Dimberg EL. Rheumatology and neurology.
paraneoplastic myelopathies. Semin Neurol 2018; Continuum (Minneap Minn) 2017;23(3, Neurology
38:278-289. doi:10.1055/s-0038-1660856 of Systemic Disease):691-721. doi:10.1212/
9 Flanagan EP, McKeon A, Lennon VA, et al. CON.0000000000000474
Paraneoplastic isolated myelopathy: clinical course 22 Toledano M. Infectious myelopathies.
and neuroimaging clues. Neurology 2011;76(24): Continuum (Minneap Minn) 2021;27(1, Spinal Cord
2089-2095. doi:10.1212/WNL.0b013e31821f468f Disorders):93-120.
10 Murphy OC, Salazar-Camelo A, Jimenez JA, et al. 23 Zalewski NL. Vascular myelopathies. Continuum
Clinical and MRI phenotypes of sarcoidosis- (Minneap Minn) 2021;27(1, Spinal Cord Disorders):
associated myelopathy. Neurol Neuroimmunol 30-61.
Neuroinflamm 2020;7(4):e722. doi:10.1212/
NXI.0000000000000722 24 Flanagan EP, Pittock SJ. Diagnosis and
management of spinal cord emergencies. Handb
11 Flanagan EP, Cabre P, Weinshenker BG, et al. Clin Neurol 2017;140:319-335. doi:10.1016/B978-0-
Epidemiology of aquaporin-4 autoimmunity and 444-63600-3.00017-9
neuromyelitis optica spectrum. Ann Neurol 2016;
79(5):775-783. doi:10.1002/ana.24617 25 Savoldi F, Nasr Z, Hu W, et al. McArdle sign: a
specific sign of multiple sclerosis. Mayo Clin
12 Zalewski NL, Rabinstein AA, Krecke KN, et al. Proc 2019;94(8):1427-1435. doi:10.1016/j.
Characteristics of spontaneous spinal cord mayocp.2019.01.047
infarction and proposed diagnostic criteria.
JAMA Neurol 2019;76(1):56-63. doi:10.1001/ 26 Hardy TA. Spinal cord anatomy and localization.
jamaneurol.2018.2734 Continuum (Minneap Minn) 2021;27(1, Spinal Cord
Disorders):12-29.
13 Keegan BM, Kaufmann TJ, Weinshenker BG, et al.
Progressive solitary sclerosis: gradual motor 27 Sechi E, Krecke KN, Pittock SJ, et al. Frequency
impairment from a single CNS demyelinating and characteristics of MRI-negative myelitis
lesion. Neurology 2016;87(16):1713-1719. associated with MOG autoantibodies. Mult Scler
doi:10.1212/WNL.0000000000003235 2020;1352458520907900. doi:10.1177/
1352458520907900
90 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
28 Filippi M, Preziosa P, Banwell BL, et al. 41 Kitley J, Woodhall M, Waters P, et al. Myelin-
Assessment of lesions on magnetic resonance oligodendrocyte glycoprotein antibodies in
imaging in multiple sclerosis: practical guidelines. adults with a neuromyelitis optica phenotype.
Brain 2019;142(7):1858-1875. doi:10.1093/brain/awz144 Neurology 2012;79(12):1273-1277. doi:10.1212/
WNL.0b013e31826aac4e
29 Klawiter EC, Benzinger T, Roy A, et al. Spinal cord
ring enhancement in multiple sclerosis. Arch 42 Zalewski NL, Krecke KN, Weinshenker BG, et al.
Neurol 2010;67(11):1395-1398. doi:10.1001/ Central canal enhancement and the trident sign
archneurol.2010.271 in spinal cord sarcoidosis. Neurology 2016;87(7):
743-744. doi:10.1212/WNL.0000000000002992
30 Ciccarelli O, Cohen JA, Reingold SC, et al. Spinal
cord involvement in multiple sclerosis and 43 Boban J, Thurnher MM. Ventral-subpial enhancement
neuromyelitis optica spectrum disorders. Lancet in spinal cord sarcoidosis: a braid-like sign. Neurology
Neurol 2019:18(2):185-197. doi:10.1016/S1474- 2018;10.1212/WNL.0000000000006857. doi:10.1212/
4422(18)30460-5 WNL.0000000000006857
31 Filippi M, Rossi P, Campi A, et al. Serial 44 Uygunoglu U, Zeydan B, Ozguler Y, et al.
contrast-enhanced MR in patients with multiple Myelopathy in Behçet's disease: the Bagel sign.
sclerosis and varying levels of disability. AJNR Am Ann Neurol 2017;82(2):288-298. doi:10.1002/
J Neuroradiol 1997;18(8):1549-1556. ana.25004
32 Asnafi S, Morris PP, Sechi E, et al. The frequency 45 Sechi E, Morris PP, McKeon A, et al. Glial fibrillary
of longitudinally extensive transverse myelitis in acidic protein IgG related myelitis:
MS: a population-based study. Mult Scler Relat characterisation and comparison with
Disord 2020;37:101487. doi:10.1016/j.msard. aquaporin-4-IgG myelitis. J Neurol Neurosurg
2019.101487 Psychiatry 2019;90(4):488-490. doi:10.1136/
jnnp-2018-318004
33 Flanagan EP, Weinshenker BG, Krecke KN, et al.
Short myelitis lesions in aquaporin-4-IgG– 46 Ogawa R, Nakashima I, Takahashi T, et al. MOG
positive neuromyelitis optica spectrum antibody-positive, benign, unilateral, cerebral
disorders. JAMA Neurol 2015;72(1):81-87. cortical encephalitis with epilepsy. Neurol
doi:10.1001/jamaneurol.2014.2137 Neuroimmunol NeuroInflamm 2017;4(2):e322.
doi:10.1212/NXI.0000000000000322
34 Ciron J, Cobo-Calvo A, Audoin B, et al. Frequency
and characteristics of short versus longitudinally 47 Budhram A, Mirian A, Le C, et al. Unilateral
extensive myelitis in adults with MOG antibodies: cortical FLAIR-hyperintense lesions in anti-MOG-
a retrospective multicentric study. Mult Scler associated encephalitis with seizures (FLAMES):
2019;1352458519849511. doi:10.1177/1352458519849511 characterization of a distinct clinico-radiographic
syndrome. J Neurol 2019;266(10):2481-2487.
35 Kumar N, Frohman EM. Spinal neurosarcoidosis doi:10.1007/s00415-019-09440-8
mimicking an idiopathic inflammatory
demyelinating syndrome. Arch Neurol 2004;61(4): 48 Dutra BG, José da Rocha A, Nunes RH, Martins
Maia Júnior C. Neuromyelitis optica spectrum
586-589. doi:10.1001/archneur.61.4.586
disorders: spectrum of MR imaging findings and
36 Jitprapaikulsan J, Lopez Chiriboga AS, Flanagan their differential diagnosis–erratum. Radiographics
EP, et al. Novel glial targets and recurrent 2018;38(2):662. doi:10.1148/rg.2018184002
longitudinally extensive transverse myelitis.
49 Mariotto S, Gajofatto A, Batzu L, et al. Relevance
JAMA Neurol 2018:e180805. doi:10.1001/
of antibodies to myelin oligodendrocyte
jamaneurol.2018.0805
glycoprotein in CSF of seronegative cases.
37 Zalewski NL, Morris PP, Weinshenker BG, et al. Neurology 2019;93(20):e1867-e1872. doi:10.1212/
Ring-enhancing spinal cord lesions in WNL.0000000000008479
neuromyelitis optica spectrum disorders.
50 Waters PJ, Komorowski L, Woodhall M, et al. A
J Neurol Neurosurg Psychiatry 2017;88(3):218-225.
multicenter comparison of MOG-IgG cell-based
doi:10.1136/jnnp-2016-314738
assays. Neurology 2019;92(11):e1250-e1255.
38 Jarius S, Paul F, Aktas O, et al. MOG doi:10.1212/WNL.0000000000007096
encephalomyelitis: international
51 Kunchok A, Chen JJ, McKeon A, et al.
recommendations on diagnosis and antibody Coexistence of myelin oligodendrocyte
testing. J Neuroinflammation 2018;15(1):134. glycoprotein and aquaporin-4 antibodies in adult
doi:10.1186/s12974-018-1144-2 and pediatric patients. JAMA Neurol 2019;77(2):
39 López-Chiriboga AS, Majed M, Fryer J, et al. 257-259. doi:10.1001/jamaneurol.2019.3656
Association of MOG-IgG serostatus with relapse 52 Faissner S, Lukas C, Reinacher-Schick A, et al.
after acute disseminated encephalomyelitis and Amphiphysin-positive paraneoplastic myelitis
proposed diagnostic criteria for MOG-IgG– and stiff-person syndrome. Neurol
associated disorders. JAMA Neurol 2018;75(11): Neuroimmunol Neuroinflamm 2016;3(6):e285.
1355-1363. doi:10.1001/jamaneurol.2018.1814 doi:10.1212/NXI.0000000000000285
40 Dubey D, Pittock SJ, Krecke KN, et al. Clinical, 53 Honorat JA, Sebastian Lopez-Chiriboga A, Kryzer
radiologic, and prognostic features of myelitis TJ, et al. Autoimmune gait disturbance
associated with myelin oligodendrocyte accompanying adaptor protein-3B2-IgG.
glycoprotein autoantibody. JAMA Neurol 2019; Neurology 2019;93(10):954-963. doi:10.1212/
76(3):301-309. doi:10.1001/jamaneurol.2018.4053 WNL.0000000000008061
CONTINUUMJOURNAL.COM 91
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELITIS AND OTHER AUTOIMMUNE MYELOPATHIES
54 Hinson SR, Lopez-Chiriboga AS, Bower JH, et al. 67 Weinshenker BG, O'Brien PC, Petterson TM, et al.
Glycine receptor modulating antibody predicting A randomized trial of plasma exchange in acute
treatable stiff-person spectrum disorders. central nervous system inflammatory
Neurol Neuroimmunol Neuroinflamm 2018;5(2): demyelinating disease. Ann Neurol 1999;46(6):
e438. doi:10.1212/NXI.0000000000000438 878-886. doi:10.1002/1531-8249(199912)46:6<878::
aid-ana10>3.0.co;2-q
55 Shelly S, Kryzer TJ, Komorowski L, et al.
Neurochondrin neurological autoimmunity. 68 Abboud H, Petrak A, Mealy M, et al. Treatment of
Neurol Neuroimmunol Neuroinflamm 2019;6(6): acute relapses in neuromyelitis optica: steroids
e612. doi:10.1212/NXI.0000000000000612 alone versus steroids plus plasma exchange.
Mult Scler J 2016;22(2):185-192. doi:10.1177/
56 Alfugham N, Gadoth A, Lennon VA, et al. ITPR1
1352458515581438
autoimmunity: frequency, neurologic phenotype,
and cancer association. Neurol Neuroimmunol 69 Bonnan M, Valentino R, Debeugny S, et al. Short
Neuroinflamm 2018;5(1):e418. doi:10.1212/ delay to initiate plasma exchange is the strongest
NXI.0000000000000418 predictor of outcome in severe attacks of
NMO spectrum disorders. J Neurol Neurosurg
57 Basal E, Zalewski N, Kryzer TJ, et al.
Psychiatry 2018;89(4):346-351. doi:10.1136/
Paraneoplastic neuronal intermediate filament
jnnp-2017-316286
autoimmunity. Neurology 2018;91(18):e1677-e1689.
doi:10.1212/WNL.0000000000006435 70 Gross RH, Corboy JR. Monitoring, switching, and
stopping multiple sclerosis disease-modifying
58 Guerra H, Pittock SJ, Moder KG, et al. Frequency
therapies. Continuum (Minneap Minn) 2019;25(3):
of aquaporin-4 immunoglobulin g in longitudinally
715-735. doi:10.1212/CON.0000000000000738
extensive transverse myelitis with
antiphospholipid antibodies. Mayo Clin Proc 71 Pittock SJ, Berthele A, Fujihara K, et al.
2018;93(9):1299-1304. doi:10.1016/j.mayocp. Eculizumab in aquaporin-4-positive
2018.02.006 neuromyelitis optica spectrum disorder. N Engl J
Med 2019;381(7):614-625. doi:10.1056/
59 Takano R, Misu T, Takahashi T, et al. Astrocytic
NEJMoa1900866
damage is far more severe than demyelination in
NMO: a clinical CSF biomarker study. Neurology 72 Cree BAC, Bennett JL, Kim HJ, et al. Inebilizumab
2010;75(3):208-216. doi:10.1212/WNL. for the treatment of neuromyelitis optica
0b013e3181e2414b spectrum disorder (N-MOmentum): a
double-blind, randomised placebo-controlled
60 Ikeda K, Kiyota N, Kuroda H, et al. Severe
phase 2/3 trial. Lancet 2019;394(10206):1352-1363.
demyelination but no astrocytopathy in clinically
doi:10.1016/S0140-6736(19)31817-3
definite neuromyelitis optica with
anti-myelin-oligodendrocyte glycoprotein 73 Tahara M, Oeda T, Okada K, et al. Safety and
antibody. Mult Scler 2015;21(5):656-659. doi: efficacy of rituximab in neuromyelitis optica
10.1177/1352458514551455 spectrum disorders (RIN-1 study): a multicentre,
randomised, double-blind, placebo-controlled
61 Yu X, Li W, Deng Q, et al. MYD88 L265P mutation
trial. Lancet Neurol 2020;19:298-306. doi:10.1016/
in lymphoid malignancies. Cancer Res 2018;78(10):
S1474-4422(20)30066-1
2457-2462. doi:10.1158/0008-5472.CAN-18-0215
74 Yamamura T, Kleiter I, Fujihara K, et al. Trial of
62 McKeon A, Apiwattanakul M, Lachance DH, et al.
satralizumab in neuromyelitis optica spectrum
Positron emission tomography-computed
disorder. N Engl J Med 2019;381(22):2114-2124.
tomography in paraneoplastic neurologic
doi:10.1056/NEJMoa1901747
disorders: systematic analysis and review. Arch
Neurol 2010;67(3):322-329. doi:10.1001/ 75 Lopez-Chiriboga S, Sechi E, Buciuc M, et al.
archneurol.2009.336 Long-term outcomes in patients with myelin
oligodendrocyte glycoprotein immunoglobulin
63 Pittock SJ, Lennon VA. Aquaporin-4
G-associated disorder. JAMA Neurol 2020;31:
autoantibodies in a paraneoplastic context. Arch
e203115. doi:10.1001/jamaneurol.2020.3115
Neurol 2008;65(5):629-632. doi:10.1001/
archneur.65.5.629 76 Chen JJ, Flanagan EP, Bhatti MT, et al.
Steroid-sparing maintenance immunotherapy
64 Cohen-Gadol AA, Zikel OM, Miller GM, et al.
for MOG-IgG associated disorder. Neurology
Spinal cord biopsy: a review of 38 cases.
2020;95(2):e111-e120. doi:10.1212/
Neurosurgery 2003;52(4):806-815; discussion
WNL.0000000000009758
815-816. doi:10.1227/01.neu.0000053223.77641.5e
77 Gelfand JM, Bradshaw MJ, Stern BJ, et al.
65 Flanagan EP, Krecke KN, Marsh RW, et al. Specific
Infliximab for the treatment of CNS sarcoidosis:
pattern of gadolinium enhancement in
a multi-institutional series. Neurology 2017;
spondylotic myelopathy. Ann Neurol 2014;76(1):
89(20):2092-2100. doi:10.1212/
54-65. doi:10.1002/ana.24184
WNL.0000000000004644
66 Conway BL, Clarke MJ, Kaufmann TJ, Flanagan EP.
Utility of extension views in spondylotic
myelopathy mimicking transverse myelitis. Mult
Scler Relat Disord 2017;11:62-64. doi:10.1016/
j.msard.2016.12.004
92 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Neoplastic Myelopathies REVIEW ARTICLE
By Amy A. Pruitt, MD, FAAN C O N T I N U UM AUDIO
I NT E R V I E W A V A I L AB L E
ONLINE
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo/R1NuKT7SYsuBdzpo0ePV on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This article reviews the current classification system of
primary spinal cord tumors and explores evolving diagnostic and
therapeutic strategies for both primary tumors and metastatic tumors to
various compartments of the spinal cord.
RECENT FINDINGS: The 2016 World Health Organization classification system
allows for more precise prognostication of and therapy for spinal cord tumors
and has identified new entities, such as the diffuse midline glioma, H3 K27M
mutant. Whole-exome sequencing reveals that the genetic background of
primary glial spinal cord neoplasms differs from that of their intracranial
histologic counterparts in ways that can potentially influence therapy.
Targeted and immune checkpoint therapies have improved survival for patients
with melanoma and lung cancer and have simultaneously produced novel
complications by enhancing radiation toxicity in some cases and by facilitating
the emergence of novel autoimmune and paraneoplastic syndromes involving
the spinal cord, such as neuromyelitis optica spectrum disorder and
syndromes associated with anti-Hu and collapsin response mediator protein-5
(CRMP-5) antibodies. These conditions must be distinguished from tumor
or infection. Epidural spinal cord compression treatment paradigms have
changed with the advent of robotic surgery and advances in radiation therapy.
SUMMARY: Neoplastic myelopathies subsume a wide spectrum of
pathologies. Neoplastic cord involvement may be primary or secondary and
may be approached diagnostically by the particular spinal cord compartment
localization. Primary spinal cord tumors account for only 2% to 4% of primary
CITE AS:
central nervous system tumors, ranging from low-grade glial neoplasms to
CONTINUUM (MINNEAP MINN)
malignant tumors. Metastatic malignancy to the epidural or leptomeningeal 2021;27(1, SPINAL CORD DISORDERS):
spaces is more common than primary cord tumors. Differential diagnoses 121–142.
arising in the course of evaluation for cord tumors include myelopathies
Address correspondence to
related to radiation or chemotherapy and paraneoplastic syndromes, all of Dr Amy A. Pruitt, 3400 Spruce St,
which are sources of significant morbidity. Knowledge of genetic syndromes Philadelphia, PA 19104,
and the biologic behavior of diverse histologies together with selective pruitt@pennmedicine.upenn.edu.
application of surgery, radiation, and targeted therapies can facilitate RELATIONSHIP DISCLOSURE:
diagnosis, minimize surgical morbidity, and prolong quality of life. Dr Pruitt serves on the editorial
boards of Neurology Clinical
Practice and Neurology Today.
INTRODUCTION UNLABELED USE OF
A
PRODUCTS/INVESTIGATIONAL
lthough spinal cord tumors represent only 2% to 4% of all primary USE DISCLOSURE:
central nervous system (CNS) tumors, they cause significant Dr Pruitt reports no disclosure.
morbidity and are often confused clinically and radiographically
with non-neoplastic processes.1 Early identification of these © 2021 American Academy
neoplasms guides appropriate management and can minimize of Neurology.
CONTINUUMJOURNAL.COM 121
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
symptoms. Difficult decisions regarding when and if to consider biopsy or to
perform major surgery accompany a diagnosis of spinal cord neoplasm, and
neurologists can provide a guided workup that can lead to a diagnosis of
neoplastic or other disease process without hazardous invasive procedures.
Neoplastic myelopathies are classified by the compartment affected as
intramedullary, intradural-extramedullary, and extradural tumors. Differential
diagnostic considerations and workup are dictated by the particular
neuroanatomic compartment involved (FIGURE 5-1).1
Overall, metastatic tumors, which are usually in the epidural space, account
for many more cases of adult spinal cord tumors than do primary spinal tumors,
whereas in children (in whom primary tumors are more common), the
intramedullary compartment is the most common tumor site. Absolute numbers
of tumors show that 1322 children and adolescents were diagnosed with spinal
cord tumors between 2012 and 2016, whereas adults aged 20 and older accounted
for 18,184 cases.2 Among children, the most common primary tumors are
ependymomas (20.6%) followed by nerve sheath tumors, neuroepithelial
tumors, astrocytoma, oligodendroglioma, glioblastoma, meningeal tumors, and
pilocytic astrocytomas. Other aggressive high-grade glial spinal neoplasms
include the H3 K27M-mutant diffuse midline gliomas of pediatric and younger
adult populations. Ependymomas are the most common primary intramedullary
spinal tumors in adults (17.6%), but the most common primary spinal tumor
overall in adults is meningioma (38.8%) followed by nerve sheath tumors
(20.5%).2 Metastatic tumors most frequently are extradural, but systemic cancer
can involve the leptomeningeal and, less commonly, intramedullary
FIGURE 5-1
Algorithm for diagnosis and management of spinal mass on MRI.
a
Whole-neuraxis imaging usually indicated to delineate other levels of pathology.
b
Benign: bone cyst, angiolipoma, hemangioma, Langerhans cell histiocytosis, osteochondroma, osteoma.
Malignant: angiosarcoma, chondrosarcoma, chordoma, Ewing sarcoma, lymphoma, myeloma,
plasmacytoma.
122 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
compartments. Lung, breast, prostate, thyroid, and renal cell cancers represent KEY POINTS
the majority of spinal metastatic tumors, the vast majority of which are
● Although spinal cord
extradural. Leptomeningeal dissemination is seen most frequently with tumors represent only 2% to
adenocarcinoma of the breast, lung carcinoma, non-Hodgkin lymphoma, 4% of all primary central
melanoma, and gastrointestinal tumors. Several paraneoplastic syndromes nervous system tumors, they
involve the spinal cord and can occur before a cancer diagnosis or emerge in the cause significant morbidity
and are often confused
setting of immune checkpoint inhibitor therapy.
clinically and
radiographically with
PRIMARY SPINAL CORD TUMORS non-neoplastic processes.
Primary spinal cord tumors arise in the cord, spinal nerve roots, or dura. Between
900 and 1800 new adult cases of primary spinal cord tumors are diagnosed ● Neoplastic myelopathies
are classified by the
annually in the United States.2 Intramedullary spinal tumors represent about 10% compartment affected as
of all primary spinal cord tumors.2 In adults, meningeal and nerve sheath tumors intramedullary, intradural-
are the most common diagnoses, whereas in children and adolescents, extramedullary, and
ependymomas and astrocytomas are the most common histologies. extradural tumors.
Differential diagnostic
Ependymomas are the most common intramedullary primary spinal cord tumor considerations and workup
in all age groups. Other histologies include astrocytoma, oligodendroglioma, are dictated by the
hemangioblastoma, ganglioglioma, germinoma, and primary CNS lymphoma. particular neuroanatomic
Histiocytic tumors, such as in Erdheim-Chester disease, occasionally involve the compartment involved.
spinal cord and can be mistaken for meningiomas. The major histologies by
● Overall, metastatic
compartment are listed in TABLE 5-1.3-6 Spinal cord tumors differ clinically, tumors, which are usually in
histologically, and genetically from their primary intracranial counterparts in the epidural space, account
several ways: for many more cases of
adult spinal cord tumors
than do primary spinal
u Back, radicular, or central pain, often asymmetric and without motor involvement, is the tumors, whereas in children
most common symptom preceding the diagnosis of an intramedullary neoplasm (CASE 5-1 (in whom primary tumors are
and CASE 5-2). more common), the
u Neuroimaging cannot precisely pinpoint histology, but some general patterns are intramedullary
evident. Astrocytomas are commonly found in an eccentric location within the cord. compartment is the most
Ependymomas, usually more central, can have an associated cyst or syrinx (CASE 5-1). common tumor site.
Ependymomas and hemangioblastomas are often hypointense on susceptibility-weighted
images (SWI), suggesting prior hemorrhage. CNS lymphomas are hyperintense on ● Ependymomas are the
diffusion-weighted images, consistent with their marked cellularity. most common primary
intramedullary spinal tumors
u Spinal glial tumors show no association between increasing grade of malignancy and in adults, but the most
patient age at diagnosis. common primary spinal
u The majority of intracranial low-grade astrocytomas harbor IDH1/IDH2 mutations; however, tumors overall in adults are
in one series, 0 of 13 spinal cord cases had this mutation.7 Aggressive high-grade astrocytic meningiomas.
tumors may harbor H3 K27M mutations.8-10 BRAF V600E mutations found in pediatric and
adult pilocytic astrocytomas occur much less frequently in spinal astrocytomas.11-13 ● Lung, breast, prostate,
thyroid, and renal cell
cancers represent the
Ependymoma majority of spinal metastatic
The World Health Organization (WHO) 2016 classification system reclassified tumors, the vast majority of
which are extradural.
ependymomas to better reflect their biological behavior.14 Nine molecular Leptomeningeal
subgroups are now recognized, three each arising in the supratentorial region, dissemination is seen most
posterior fossa, and spine. Cellular ependymomas may be WHO grade II or grade frequently with
III and arise from the intraspinal canal, usually in the cervical and thoracic adenocarcinoma of the
breast and lung,
regions; myxopapillary ependymoma, a WHO grade I tumor, is most frequently non-Hodgkin lymphoma,
seen in the conus medullaris arising from the filum terminale, where they melanoma, and
comprise 90% of tumors.14 Subependymomas are rarely found in the spine; gastrointestinal tumors.
if present, they are usually cervical, eccentric, and T2-hyperintense and
T1-hypointense lesions that infrequently enhance with gadolinium.15 In children,
CONTINUUMJOURNAL.COM 123
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
ependymomas are frequently in the posterior fossa; however, in adults,
ependymomas are most common in the spine. Neurofibromatosis type 2 (NF2)
mutations are found in some ependymomas.7
Several radiographic features distinguish ependymomas from astrocytomas.
Ependymomas are often well-demarcated isointense lesions that enhance with
gadolinium. They may have a cyst and syrinx, and hemorrhage may be seen on
SWI sequences. Some have a rim of extreme hypointensity called the
hemosiderin cap sign, visible on T2 and SWI sequences. Patients present with
low back pain, leg weakness, and bladder dysfunction and are more likely to have
a central cord syndrome than a Brown-Séquard syndrome pattern.
Distinguishing ependymomas from astrocytomas radiographically is
important in preoperative planning as gross total resection of astrocytomas is
unlikely, but ependymomas, which are often encapsulated, are more amenable to
TABLE 5-1 Primary Spinal Cord Tumors
Intramedullary
◆ Ependymoma
◇ Ependymoma (World Health Organization [WHO] grade II)
◇ Anaplastic ependymoma (WHO grade III)
◇ Myxopapillary ependymoma (WHO grade I)
◇ Subependymoma (WHO grade I)
◆ Astrocytoma
◇ Pilocytic astrocytoma (WHO Grade I)
◇ Diffuse astrocytoma (WHO grade II)
◇ Anaplastic astrocytoma (WHO Grade III)
◇ Glioblastoma (WHO Grade IV)
→ Midline glioma (H3 K27M mutation)
◆ Oligodendroglioma
◇ Oligodendroglioma (WHO grade II)
◇ Anaplastic oligodendroglioma (WHO grade III)
◆ Atypical teratoid/rhabdoid tumors
◆ Mixed neuronal/glial tumors
◇ Ganglioglioma (WHO grade I)
◆ Mesenchymal tumors
◇ Hemangioblastoma (WHO grade I)
◇ Lipoma
◇ Melanocytoma
◆ Hematopoietic tumors
◇ Primary central nervous system lymphoma
◇ Leukemia (myelocytic sarcoma)
CONTINUED ON PAGE 125
124 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
total resection. Intraoperative monitoring can be used to assist with complete
resection. However, if on surgical resection the ependymoma capsule is entered,
these tumors can seed the neuraxis and frequently recur. Adjuvant radiation
therapy is suggested for incompletely resected tumors, and long-term
surveillance of the neuraxis is important (CASE 5-1). No chemotherapy regimen
has been established for incompletely resected ependymomas, but intracranial
ependymoma may respond to bevacizumab or lapatinib.16,17
Astrocytoma
Intramedullary astrocytomas represent about 7% of all primary spinal cord
tumors.2 Most are low grade, but their location and infiltrative behavior preclude
effective resection. They are often lateralized to one side of the cord, and patients
may present with local pain or a Brown-Séquard syndrome. Many patients will
CONTINUED FROM PAGE 124
Intradural-extramedullary
◆ Meningioma
◆ Schwannoma
◆ Neurofibroma
◆ Hemangioblastoma
◆ Myxopapillary ependymoma
◆ Paraganglioma
◆ Lipoma
◆ Sarcoma
Extradural
◆ Meningioma
◆ En plaque meningioma
◆ Schwannoma
◆ Myxopapillary ependymoma
◆ Histiocytic tumors
◇ Erdheim-Chester disease
Primary brain tumors that disseminate to spinal canala
◆ Medulloblastoma
◆ Central nervous system neuroblastoma
◆ Ependymoma
◆ Primary central nervous system lymphoma
◆ High-grade gliomab
◆ Primary dural lymphoma (low-grade B-cell marginal zone lymphoma)
a
Drop metastases or leptomeningeal metastases.
b
These complications usually occur late in the disease course, after multiple surgical interventions.
CONTINUUMJOURNAL.COM 125
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
CASE 5-1 A 53-year-old man with type 2 diabetes developed right arm pain. A
cervical MRI with contrast was obtained, and he was found to have a
cervical spinal cord neoplasm (FIGURE 5-2). After being followed for 4
years, during which there was slow tumor growth with concomitant
increase in arm paresthesia, he underwent surgery with partial excision of
a World Health Organization grade II cellular ependymoma. He remained
numb from the cervical level down, with whole-body hyperalgesia “like a
tight wetsuit.” Proprioceptive problems produced balance difficulties
that were a limiting factor in his functional abilities such as driving. Three
years after the original surgery, he underwent radiation for a new tumor
2 cm caudal to the original side (3600 cGy in 20 fractions with an
additional radiation boost of 50.4 Gy to the area of greatest contrast
enhancement). Five years after radiation, he developed urinary retention,
left calf pain, and left footdrop and was found to have a conus
medullaris/cauda equina lesion.
FIGURE 5-2
Imaging of the patient in CASE 5-1 with ependymoma. Intramedullary tumor with cystic
component at first diagnosis of ependymoma on sagittal T2-weighted (A) and postcontrast
T1-weighted (B) MRIs. Sagittal T2-weighted (C) and postcontrast T1-weighted (D) MRIs
reveal tumor recurrence 7 years later and with progressive symptoms 2 years later not
attributable to tumor but to tethering of the atrophic cord at C5 on sagittal T2-weighted
MRI following radiation therapy (E).
COMMENT This case illustrates the typical MRI findings of cyst and syrinx in a spinal
cord ependymoma as well as the role of surgery at clinical progression and
the resultant considerable disability, in this case proprioceptive
dysfunction and pain. It also illustrates the propensity of ependymoma for
local recurrence and subsequent spread through the neuraxis. This patient
sustained surgical and radiation morbidities, with cord atrophy and a
tethered cord. Although the indolent behavior over more than a decade is
typical, recurrence is common both locally and through drop metastases.
Diabetes complicated this patient’s functional status as he likely had a
superimposed distal sensory neuropathy.
126 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
enjoy long periods of minimal symptoms without surgical intervention (CASE 5-2,
FIGURE 5-3). Specialized imaging of the spine, including diffusion-weighted
imaging, diffusion tensor imaging, and fractional anisotropy, can be useful to
map the extent of spinal lesions and to predict the outcome of surgical
intervention, tracking fibers to visualize the integrity of white matter tracts.18
Intraoperative monitoring adds to the safety of the surgical intervention.19
Prognostic factors for astrocytoma have been identified. In one series of
131 adults from the Surveillance, Epidemiology, and End Results Program
A 30-year-old woman first noted bandlike dysesthesia and occasional CASE 5-2
sharp neuralgic pains in the midthoracic region when she was 13 years of
age, and a nonenhancing intraaxial mass in the thoracic spinal cord was
first seen on imaging when she was 19 years of age. She was followed with
stable MRI scans for more than 10 years (FIGURE 5-3), and her examination
remained stable with mild hyperreflexia and allodynia over the T9
through T11 levels. In view of her clinicoradiographic stability, continued
annual imaging was elected. She had no family history of neurofibromatosis
type 1, neurofibromatosis type 2, or von Hippel-Lindau syndrome.
FIGURE 5-3
Imaging of the patient in CASE 5-2 with a nonenhancing intramedullary tumor. Sagittal
T2-weighted images of the same tumor with a 14-year interval between panel A and
panels B and C. Axial T2-weighted MRI shows the typical asymmetric location of this
slow-growing astrocytic neoplasm.
Low-grade intramedullary spinal tumors account for 10% to 20% of all spinal COMMENT
tumors.7 These tumors do not harbor the classic mutations associated with
their intracranial counterparts; thus, for this patient, targeted therapeutic
options are limited. Typical for astrocytomas, this tumor is nonenhancing
and appears as a T2 hyperintensity on sagittal views (FIGURES 5-3A and 5-3B)
that involve one-half of the cord (FIGURE 5-3C). MRI characteristically shows
no enhancement in over 50% of low-grade astrocytomas, in contrast to
high-grade glial neoplasms of the spine.8
CONTINUUMJOURNAL.COM 127
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
CASE 5-3 A 28-year-old man presented with shortness of breath and was found
to have a cardiac ejection fraction of 15%. Coronary angiography was
normal, but MRI done because of dysphagia and right facial numbness
showed a nonenhancing medullary lesion. Because of hemodynamic
instability and tumor location, no biopsy was done, and he was
treated empirically
with proton therapy. He
did well, with no dysphagia
or hemodynamic instability
for 9 months before
presenting again with
numbness below the
nipples, urinary retention,
and recurrent facial
numbness. Repeat MRI
showed a relatively stable
brainstem tumor but also a
T6 intramedullary lesion
(FIGURE 5-4A). Within a
month, dramatic spread FIGURE 5-4
of leptomeningeal Imaging of the patient in CASE 5-3 with H3
enhancement was seen K27M-mutant midline glioma presenting with
medullary symptoms. A, Axial fluid-attenuated
(FIGURE 5-4B). This area inversion recovery (FLAIR) MRI shows diffuse
was biopsied, and H3 K27M expansion of the right side of the medulla by a
astrocytoma was diagnosed. nonenhancing intramedullary lesion. One year
The patient’s disease later, the patient had developed paraparesis from
this aggressive tumor. B, Sagittal postcontrast
progressed too rapidly to T1-weighted MRI obtained 1 year after the initial
permit enrollment in a imaging shows diffuse contrast-enhancing
clinical trial. metastases throughout the thoracic spine.
COMMENT This tumor in the medulla, which presented unusually as takotsubo
syndrome, did not behave like a low-grade brainstem glioma. Repeat
imaging showed an enhancing intramedullary lesion in the thoracic region,
and the patient rapidly developed paraplegia. The suspicion was that the
biological behavior was that of a high-grade H3 K27M glial neoplasm. The
cord lesion also was deemed inaccessible to safe biopsy, so diagnosis was
made by biopsy of the cauda equina; treatment was radiation to a wide
field of the spinal cord. The patient died before having access to
developing targeted therapy, such as imipridone ONC201. The prognosis
for these high-grade cord tumors is poor; this patient died 15 months after
onset of symptoms.
128 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
(SEER) database, overall survival was 85.5% at 1 year, 71% at 3 years, 64.1% at KEY POINTS
5 years, and 55% at 10 years.20 Younger age at diagnosis, tumor grade, and larger
● Ependymomas are the
extent of resection were each associated with worse long-term prognosis. This most common
study is consistent with prior literature that also noted better survival with intramedullary primary
thoracic astrocytomas compared to cervical region tumors.21 spinal cord tumor in all age
Primary spinal high-grade gliomas (WHO grade IV, glioblastoma) account for groups.
only 7.5% of all intramedullary spinal cord gliomas.22 The mean age at diagnosis is
● Back, radicular, or central
39 years, with males outnumbering females by more than 3 to 1.22 Median overall pain, often asymmetric and
survival of patients with high-grade glial spinal neoplasms is 10 to 13 months. without motor involvement,
Recognized for the first time in the 2016 WHO classification of tumors is the is the most common
WHO grade IV diffuse midline glioma, H3 K27M mutant, previously called symptom preceding the
diagnosis of intramedullary
diffuse intrinsic pontine glioma. Median survival was 48.5 months for H3 neoplasm.
K27M–positive cases, compared to 1 month for those with TERT promoter
mutation and 77 months for those harboring neither.7 Median survival for cases ● Spinal glial tumors show
with TP53 mutations was 11.5 months and for those with PPM1D mutations was no association between
increasing grade of
84 months. These statistics suggest that high-grade infiltrating gliomas of the malignancy and patient age
spinal cord in adults represent a heterogeneous group of tumors, the prognosis of at diagnosis.
which can be predicted by genetic profiling.
The H3 K27M mutation and EGFR or genetic alterations offering a better ● Cellular ependymomas
may be World Health
prognosis are mutually exclusive. Mutations conferring a better prognosis
Organization (WHO) grade II
include the IDH1, IDH2, 1p/19q codeletion, and BRAF mutations seen in or grade III and arise from
oligodendrogliomas and low-grade astrocytomas. the intraspinal canal, usually
Like high-grade gliomas elsewhere in the nervous system, the H3 K27M in the cervical and thoracic
mutation is associated with TP53 expression, ATRX loss, and monosomy 10. In regions; myxopapillary
ependymoma, a WHO grade
one series, the tumors of six of 13 patients with high-grade spinal cord gliomas I tumor, is most frequently
harbored this mutation.7 Most H3 K27M-mutant diffuse midline gliomas occur in seen in the conus medullaris
the thalamus and brainstem, but brainstem cases can extend to the spinal cord arising from the filum
and show a propensity for intramedullary drop metastases and leptomeningeal terminale, where they
comprise 90% of tumors.
dissemination (CASE 5-3).19,23,24 Although making the diagnosis through biopsy is
hazardous because of location, it is important to attempt definitive diagnosis. In a ● Ependymomas are often
2017 phase 2 trial of patients with glioblastoma, treatment with imipridone ONC201, well-demarcated isointense
a selective antagonist of the G protein–coupled dopamine receptor D2/D3, lesions that enhance with
gadolinium.
produced a dramatic response in one patient with a H3 K27M mutation.25-27
Based on this response, an expanded access program was initiated.28 A 2019 ● Gross total resection of
report described 18 patients who received imipridone ONC201 after initial astrocytomas is unlikely, but
radiation therapy and at or before recurrence without leptomeningeal ependymomas, which are
dissemination. Three adults among the 14 recurrent patients remained on often encapsulated, are
more amenable to total
treatment, with progression-free status at a median of 49.6 weeks (versus resection.
14 weeks before the use of ONC201).29 Referral to an ongoing open-label trial
should be considered for patients with biopsy-proven H3 K27M mutations. ● Recognized for the first
Better understanding of the molecular underpinnings of astrocytic tumors time in the 2016 WHO
classification of tumors is
has led to some improvement in survival for another subset of patients. The the WHO grade IV diffuse
BRAF V600E mutation has been infrequently reported in spinal cord tumors, midline glioma, H3 K27M
although it is of prognostic and therapeutic significance in several types of mutant, previously called
low-grade intracranial gliomas such as pleomorphic xanthoastrocytomas, diffuse intrinsic pontine
glioma.
gangliogliomas, and pilocytic astrocytomas. Occasionally, this mutation is seen
with higher-grade gliomas in both cord and brain.10 Sustained responses to BRAF
inhibitors have been reported in isolated instances.8,11,30 For most symptomatic
and incompletely resected primary spinal cord tumors, radiation therapy of
5040 cGy to 5400 cGy, depending on the grade of the tumor, is recommended.
CONTINUUMJOURNAL.COM 129
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
Proton therapy is assuming a larger role in the radiation oncologic management
of these tumors.31
Pilocytic astrocytomas of the spinal cord account for about 11% of pediatric
spinal cord tumors.2 These often are associated with neurofibromatosis type 1.
Most are well circumscribed and WHO grade I. The majority have a fusion gene
between the BRAF gene and KIAA1549. BRAF V600E also can be found. The
most common location is the cervical spinal cord followed by thoracic spinal
cord, but the tumor may be distributed throughout the cord. A limited role for
radiation exists only in cases with definite radiographic or clinical progression.
Atypical Teratoid/Rhabdoid Tumor
Atypical teratoid/rhabdoid tumor (ATRT) is another WHO Grade I tumor that
is seen primarily in children. The peak incidence is in children younger than
CASE 5-4 A 66-year-old man noted gradually progressive leg weakness over a
12-month period, during which he also experienced weight loss,
fevers, and night sweats. MRI showed a single enhancing expansile
abnormality in the cervical and thoracic cord (FIGURE 5-5), and brain MRI
showed worsening confluent
signal change in the corpus
callosum and brainstem.
Lumbar puncture showed
protein of 169 mg/dL and a
CD19-positive monoclonal
B-cell population consistent
with non-Hodgkin B-cell
lymphoma. He was human
immunodeficiency virus (HIV)
negative, and Epstein-Barr
virus was negative in the CSF.
His CD4+ count was 293.
He received rituximab,
methotrexate, and
temozolomide followed by
hematopoietic stem cell FIGURE 5-5
transplantation nearly 2 years Imaging of the patient in CASE 5-4 with
after onset of symptoms. intramedullary lymphoma. A, Sagittal T2-weighted
MRI shows an extensive area of intramedullary T2
Leg function returned, but signal abnormality. B, Sagittal postcontrast
he developed a persistent T1-weighted MRI shows diffuse homogeneous
need to self-catheterize. enhancement.
COMMENT This patient had primary central nervous system lymphoma involving both
brain and spinal cord, with the latter causing the predominant symptoms.
He also had B (systemic) symptoms, although this is not typical of primary
central nervous system lymphoma.
130 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
2 years of age, and ATRT is the most common CNS tumor in this age group. KEY POINTS
Localization of the primary tumor is nearly equally distributed between the
● Most H3 K27M-mutant
supratentorial and infratentorial compartments. Data on spinal cord ATRT are diffuse midline gliomas occur
limited to small numbers of patients included in series reporting on cerebral in the thalamus and
ATRT or published as isolated case reports. Recently, DNA methylation and brainstem, but brainstem
gene-expression profiles disclosed three distinct epigenetic subgroups of ATRT cases can extend to the
spinal cord and show a
(ATRT-MYC, ATRT-SHH, and ATRT-TYR), with distinguishing clinical
propensity for intramedullary
features. In one series of 13 patients, long-term survival was achieved in some drop metastases and
spinal cord ATRT patients with multimodality therapy (postoperative radiation leptomeningeal
and chemotherapy).32 dissemination.
● Pilocytic astrocytomas of
Hemangioblastoma the spinal cord account for
Hemangioblastoma, a WHO grade I tumor, is rare except in von Hippel-Lindau about 11% of pediatric spinal
syndrome, an autosomal dominant disorder characterized by chromosome cord tumors. These often
3p deletion; von Hippel-Lindau syndrome accounts for up to 30% of cases are associated with
neurofibromatosis type 1.
of hemangioblastoma.33 Retinal hemangiomas, renal and pancreatic cysts, Most are well circumscribed
renal cell carcinoma, and pheochromocytoma are associated pathologies. and WHO grade I.
Hemangioblastomas have a male predominance. Clinically, hemangioblastomas
of the spinal cord are characterized by slowly progressive proprioceptive deficits. ● Hemangioblastoma, a
WHO grade I tumor, is rare
The location is more frequently cervical than thoracic, and neuroimaging shows
except in von Hippel-Lindau
a homogeneously enhancing mural nodule; cysts and a syrinx are additional syndrome, an autosomal
common features. Hemangioblastomas are more vascular than ependymomas, dominant disorder
and early draining veins may cause diagnostic confusion with a vascular characterized by
malformation. The presence of a syrinx, uncommon with vascular malformations, chromosome 3p deletion;
von Hippel-Lindau
is seen in up to one-half of hemangioblastomas.3 Surgical resection may be syndrome accounts for up to
curative. Tumor recurrence is common in patients with von Hippel-Lindau 30% of cases of
syndrome and case reports exist of tumor regression with treatment with hemangioblastoma.
bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor.33,34
Primary Central Nervous System Lymphoma
Primary CNS lymphoma in the intramedullary or leptomeningeal compartments
is rare. The majority of tumors arise from large B cells and comprise no more than
2% of all primary CNS lymphoma cases.35 The tumors are often multifocal.
Patients who are immunocompetent have a median age of 62 years, and patients
with human immunodeficiency virus (HIV), who are organ transplant
recipients, or who are otherwise immunocompromised are usually younger.
Progressive myelopathy and radiculopathy are the most common presentations,
and the clinical setting often raises the differential diagnosis of neuromyelitis
optica spectrum disorder (NMOSD), multiple sclerosis, neurosarcoidosis, or
another immune-mediated myelopathy syndrome (CASE 5-4).35 Fludeoxyglucose
positron emission tomography (FDG-PET) may show hypermetabolism in the
lesion. Various systemic regimens based on rituximab, methotrexate,
temozolomide, or combinations of drugs have been employed.
INTRADURAL-EXTRAMEDULLARY PRIMARY SPINAL CORD TUMORS
Intradural-extramedullary primary spinal cord tumors represent a diverse and
important group of neoplasms, the treatment of which differs from intramedullary
tumors in that these extramedullary neoplasms often are amenable to surgical resection.
Many are associated with genetic syndromes, the identification and workup of which
falls to the neurologic consultant (TABLE 5-2).
CONTINUUMJOURNAL.COM 131
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
Meningioma
Meningiomas are the most common primary spinal cord neoplasm in adults,
accounting for one-fourth of all primary spinal cord tumors. Eighty percent
of patients with spinal cord meningioma are female, and 80% of the cases in
females occur in the thoracic region, whereas spinal cord meningiomas in
males are equally distributed between the cervical and thoracic cord.36 The
majority of spinal cord meningiomas are WHO grade I slow-growing tumors.
Genetic predisposition (eg, in patients with NF2) and prior radiation are risk
factors. Over 90% of spinal cord meningiomas are located in the intradural-
extramedullary space, and only 6% are extradural.36 On T1-weighted MRI, the
tumors are isointense to hypointense and exhibit intense solid homogeneous
enhancement postgadolinium; an accompanying dural tail may be seen.
Radiosurgery is used for incomplete resection or recurrence, and protons are
gaining a larger role in the treatment of spinal cord meningioma. No role for
chemotherapy has been established, but intracranial meningiomas have been
reported to respond to everolimus (a mammalian target of rapamycin [mTOR]
inhibitor), sunitinib (a multi–tyrosine kinase inhibitor), and bevacizumab
(a VEGF inhibitor). By extension of this experience, although without evidence
from prospective trials, some of these agents may be considered for select
patients with refractory spinal cord meningiomas (CASE 5-5).36
Patients with asymptomatic spinal cord meningiomas can be followed with
serial MRIs. Surgery is the primary modality and can be curative. Conventional
fractionated radiation therapy or proton therapy is a consideration at progression.
NERVE SHEATH TUMORS
Nerve sheath tumors include schwannomas and neurofibromas associated with
genetic syndromes that also involve other neurologic abnormalities (TABLE 5-2).
CASE 5-6 illustrates some of the management considerations for patients with
neurofibromas.
TABLE 5-2 Spinal Cord Tumors Related to Genetic Syndromesa
Syndrome (genetic mutation) Intracranial and systemic tumors Spinal tumor
Neurofibromatosis type 1 (NFI gene on Malignant nerve sheath tumors, optic gliomas, Neurofibroma, meningioma,
chromosome 17), autosomal dominant hamartomas schwannoma, ependymoma,
glioma
Neurofibromatosis type 2 (NF2 gene on Cranial nerve schwannomas Meningioma, schwannoma,
chromosome 22), bilateral vestibular ependymoma, glioma
schwannomas
Schwannomatosis (SMARCB1 gene on Schwannomas, meningiomas Meningioma, schwannoma
chromosome 22, LZTR1 gene on
chromosome 22, somatic NFR mutation)
Von Hippel-Lindau syndrome (VHL gene Renal cell carcinomas, retinal angiomas, Hemangioblastoma
on chromosome 3) pheochromocytomas, hemangioblastomas of
the central nervous system, endolymphatic
sac tumors of middle ear, pancreatic tumors
a
Modified with permission from Wu J, Ranjan S, Continuum (Minneap Minn).4 © 2018 American Academy of Neurology.
132 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Schwannoma
Schwannomas are benign nerve sheath tumors, the majority of which are
WHO grade I. They represent nearly 30% of spinal root tumors, and multiple
schwannomas can be found in patients with NF2 or schwannomatosis.4 Patients
with schwannomatosis typically present in their forties, usually with radicular
pain and little motor involvement as the schwannomas develop primarily on
spinal sensory roots. On MRI, the tumors often appear as heterogeneously
enhancing paraspinous dumbbell-shaped masses. The tumors are considered
cured after effective resection.
TRENDS
A word about spinal cord tumors resulting from “stem cell tourism” is in order.
Berkowitz and colleagues38 reported a case of a mixed spinal cord tumor arising
An 80-year old woman CASE 5-5
presented with a 6-month
history of unsteadiness and
leaning to the right. She
reported that she sometimes
felt that “food stays in my
throat and goes down the
wrong way.” She worried
that if she got any worse,
she would not be able to be
independent.
Her examination was
notable for slight
hyperreflexia in the lower
limbs and minimal ataxia of
the right arm. Her palate
elevated midline, and her FIGURE 5-6
Imaging of the patient in CASE 5-5 with meningioma.
tongue was strong. Gag Sagittal postcontrast T1-weighted MRI shows a
reflex was intact. large contrast-enhancing extramedullary lesion at
MRI showed a large, avidly the foramen magnum impinging on the upper
enhancing extradural mass at cervical cord and lower brainstem.
the foramen magnum
impinging on the cord
(FIGURE 5-6).
This patient’s MRI looked considerably worse than the patient’s COMMENT
examination demonstrated, suggesting that the process had been slow.
She had a foramen magnum meningioma, which is often heralded by lower
cranial nerve findings. Her symptoms could not be improved, and some
hazard existed in surgery. Systemic therapy options for unresectable
meningioma are limited to investigational agents. For this older patient with
stable symptoms, no systemic therapy would be recommended.
CONTINUUMJOURNAL.COM 133
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
in a patient who underwent intrathecal infusions of what was represented to the
patient as mesenchymal, embryonic, and fetal neural stem cells in commercial
clinics in China, Argentina, and Mexico for treatment of deficits related to an
ischemic stroke. When he subsequently developed back pain, paraplegia, and
urinary incontinence, he had an MRI that revealed a lesion of the thoracic
spinal cord. On neuropathologic review, it was shown to be a cellular highly
proliferative primitive tumor with glial differentiation. This should represent a
cautionary tale about such unsubstantiated treatments.
EXTRADURAL TUMORS
Numerically, extradural tumors represent the largest number of adult spinal cord
neoplasms and are usually metastases from a systemic neoplasm.
CASE 5-6 A 28-year old woman with neurofibromatosis type 1 (NF1) presented with
progressive neck pain, dysphagia, and evolving leg weakness. Multiple
surgeries and tipifarnib systemic therapy for NF1-associated
neurofibromas had failed. Cervical MRI was performed and showed
enlarging neurofibromas at multiple cervical levels (FIGURE 5-7).
She also had multiple neurofibromas caudal to the displayed level.
FIGURE 5-7
Imaging of the patient in CASE 5-6 with neurofibromatosis type 1. A, Sagittal postcontrast
T1-weighted MRI shows multiple lesions throughout the extramedullary cervical spine. B,
Axial postcontrast MRI shows the lesions more prominently. C, Sagittal postcontrast
T1-weighted MRI of the thoracic spine shows additional lesions.
COMMENT Surgery was not feasible for the patient in this case with multiple spinal
neurofibromas. If possible, she should be offered a trial of systemic
therapy. She is a candidate for selumetinib, which is a new development
for the treatment of plexiform neurofibromas that has shown significant
activity in large surgically hazardous tumors.37
134 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Spinal Cord Metastases KEY POINTS
Spinal intramedullary and leptomeningeal metastases are rare compared to their
● Meningiomas are the
intracranial counterparts, but their effect on survival and quality of life is great. most common primary
Tumors most frequently spreading to these compartments include some histologies spinal cord neoplasm in
for which new systemically administered targeted therapies are available (eg, lung adults, accounting for
cancer, breast cancer, melanoma). For example, second-generation (eg, ceritinib, one-fourth of all primary
spinal cord tumors. The
alectinib) and third-generation(eg, brigatinib, lorlatinib) anaplastic lymphoma
majority of meningiomas are
kinase (ALK) inhibitors have effected sustained remissions in non–small cell lung WHO grade I slow-growing
cancer.39 Extradural metastases are most likely to occur from lung, breast, prostate, tumors. Genetic
thyroid, and renal cancers, whereas leptomeningeal dissemination of solid tumors is predisposition
(neurofibromatosis type 2)
most commonly seen from breast and lung cancers, melanoma, non-Hodgkin
and prior radiation are risk
lymphoma, and gastrointestinal tumors. factors.
Treatment of epidural cord compression is palliative, with the principle goals
of pain relief, preservation of neurologic function, maintenance of spinal ● Radiosurgery is used for
stability, and improvement in quality of life while avoiding the toxic incomplete resection or
recurrence of spinal
consequences of radiation and chemotherapy. For selected patients, aggressive meningioma, and protons
management can improve local control with two relatively new technologies that are gaining a larger role in
improve outcomes over simple laminectomy. The first, called separation surgery, the treatment of spinal
involves dissecting the anterior sulcus in the spinal canal from the posterior edge meningioma. No role for
chemotherapy has been
of the vertebral body without affecting the vertebral body.40-42 This causes dural established, but intracranial
decompression and restores the thecal sac circumferentially. It is coupled with meningiomas have been
the second technology, stereotactic body radiation therapy, also known as spinal reported to respond to
stereotactic radiosurgery, as the physical separation of tumor from cord now everolimus, sunitinib, and
bevacizumab.
improves spine stereotactic body radiation therapy dosimetry. High-dose radiation
then ablates the remaining vertebral segment tumor, and vertebroplasty can be ● Schwannomas are benign
used to stabilize the bone. Integration of stereotactic body radiation therapy has nerve sheath tumors, the
fundamentally changed the indications and type of surgery performed for majority of which are WHO
metastatic spine tumors. Protons can be used as well, but large-scale studies of grade I. They represent
nearly 30% of spinal root
outcomes are lacking. As these treatment decisions become more complex, a tumors, and multiple
multidisciplinary approach involving neurologists, medical oncologists, radiation schwannomas can be found
oncologists, spine surgeons, interventionalists, and pain specialists is required.43 in patients with
neurofibromatosis type 2 or
schwannomatosis.
Leptomeningeal Disease
Leptomeningeal carcinomatosis or neoplastic meningitis occurs when malignant ● Extradural metastases are
cells gain access to the CNS either through hematogenous dissemination or by most likely to occur from
direct extension from parenchymal or bone metastases. This usually occurs at a lung, breast, prostate,
thyroid, and renal cancers,
time of advanced cancer dissemination. The most common cell types are breast,
whereas leptomeningeal
lung, and gastrointestinal cancers; melanoma; and non-Hodgkin lymphoma. dissemination of solid
Paresthesia, back pain, lower motor neuron weakness, and sphincter dysfunction tumors is most commonly
are the most common symptoms. The cauda equina is typically involved, but the seen from breast and lung
cancers, melanoma,
entire neuraxis should be scanned. Diagnosis is made by MRI or cytology, or
non–Hodgkin lymphoma,
both; MRI is better at visualizing solid tumors than lymphoma.44 Epidural, brain and gastrointestinal tumors.
parenchymal, and leptomeningeal involvement can coexist.
Progressive hydrocephalus may require repetitive lumbar punctures or
shunting, and acetazolamide can be used to control intracranial pressure.
Primary brain tumors can also spread to the spinal canal, usually late in the
course, in which case they can have both intramedullary and leptomeningeal
involvement (TABLE 5-1).
Intramedullary spinal cord metastases are much less common than epidural
metastatic disease. More than half are from lung cancer, followed by breast
CONTINUUMJOURNAL.COM 135
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
cancer and renal cell cancer, melanoma, and lymphoma. The cervical cord is the
most frequently involved region. Hematogenous spread or carcinomatous
meningitis can occur concurrently, possibly by direct extension through nerve
roots. Two radiographic signs of intramedullary spinal cord metastases may be
seen: rim and flame. A thin rim of peripheral enhancement and a flame-shaped
appearance in the region of enhancement at the superior and inferior margins
should suggest a non-CNS metastatic intramedullary tumor rather than one of
primary spinal cord origin.45,46 The flame-shaped ovoid lesion is hypointense on
T2-weighted sequences with a hyperintense rim with enhancement (FIGURE 5-8).
RADIATION-RELATED MYELOPATHY
Despite careful attention to dosimetry, the risk of permanent myelopathy
from radiation remains possible and frequently is devastating. Early
symptoms of radiation toxicity include paresthesia with the Lhermitte sign
occurring 2 to 4 months after treatment, which may respond to a brief
corticosteroid course. Less readily reversible signs and symptoms, such as
paresthesia, pain, sphincter dysfunction, and weakness, can develop later.
MRI shows hyperintensity on T2-weighted sequences with or without
enhancement. At later stages, spinal cord atrophy predominates. Many
treatment interventions have been attempted for these disabling symptoms,
including high-dose corticosteroids, hyperbaric oxygen, anticoagulation, and
bevacizumab (CASE 5-7).47 Another
complication of radiation therapy,
cavernous malformations (which have
been well described intracranially) can
also be found in the spinal cord and may
cause sudden paraplegia due to
hemorrhage.
CHEMOTHERAPY-RELATED
MYELOPATHY
Both intrathecally and systemically
administered cytotoxic agents can
infrequently result in a longitudinally
devastating myelopathy. The most
frequently implicated agents are
methotrexate and cytarabine. The onset is
often rapid; sometimes after a first dose,
recovery is possible, although it is often
incomplete (CASE 5-8).
EXTRADURAL PRIMARY SPINAL
CORD TUMORS
Rarely, schwannomas and meningiomas
FIGURE 5-8 may be predominantly in the extradural
Intramedullary metastasis. Sagittal compartment. Meningiomas in this
postcontrast T1-weighted MRI shows a location are often en plaque. This pattern
flame-shaped enhancing lesion due to
intramedullary metastasis from lung
can mimic extradural metastatic tumors
cancer. The associated vertebral body (such as those of breast, lung, or prostate
change is radiation related. origin) or primary dural lymphoma, a
136 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
low-grade B-cell marginal zone lymphoma. Myxopapillary ependymomas also can KEY POINTS
have an extradural component.
● Treatment of epidural
cord compression is
NON-NEOPLASTIC SPINAL CORD NEOPLASM MIMICS palliative, with the principle
Spinal cord enlargement seen on imaging with or without contrast enhancement goals of pain relief,
can have diverse causes, and it often falls to the neurologic consultant to generate preservation of neurologic
function, maintenance of
an appropriate differential diagnosis. Although cord enlargement from the
spinal stability, and
above-discussed intramedullary tumors is always on the diagnostic list, the improvement in quality of
physician must also consider the consequences of radiation and adverse life while avoiding the toxic
effects of cancer therapies. The differential of cord pathology is broad and consequences of radiation
and chemotherapy.
includes many non-neoplastic entities, many of which can be excluded based
on the timing of symptom onset and demographic features. However, it is ● A thin rim of peripheral
always prudent to at least consider various non-neoplastic disease categories enhancement and a
(FIGURE 5-1). flame-shaped appearance
This section briefly covers some of the many processes that can mimic in the region of
enhancement at the superior
spinal cord neoplasm. Since cord biopsy is often a hazardous undertaking, and inferior margins should
recognition of processes that do not warrant invasive procedures is a valuable suggest a non–central
contribution to patient care. Certain situations should raise concern for spinal nervous system metastatic
cord neoplasia. intramedullary tumor rather
than one of primary spinal
Enhancement can persist for months to years after spinal cord compression, cord origin.
such as from cervical spondylosis, often taking the shape of pancake enhancement.
Acute demyelinating disease, including aquaporin-4-IgG–seropositive ● Compared with patients
NMOSD and myelin oligodendrocyte glycoprotein (MOG) antibody–associated with nonparaneoplastic
neuromyelitis optica
disorder, can produce longitudinally extensive, sometimes enhancing spinal
spectrum disorder
cord abnormalities. In the context of neoplasm-associated myelopathic (NMOSD), patients with
processes, demographic features suggestive of paraneoplastic myelopathies, paraneoplastic NMOSD are
including those with an NMOSD phenotype, should be recognized.48,49 In one older at symptom onset and
series, five of 156 patients had paraneoplastic NMOSD and these authors more frequently male. Thus,
older patients presenting
included 12 previously reported patients with paraneoplastic NMOSD in their with NMOSD, particularly if
series. Adenocarcinoma of lung and breast accounted for five cases each. male, should be investigated
Compared with patients with non-paraneoplastic NMOSD, patients with for neoplasia.
paraneoplastic NMOSD were older at symptom onset (median age 55 compared
● In the context of immune
to 40) and more frequently male. Thus, older patients presenting with NMOSD, checkpoint inhibitor
particularly if male, should be investigated for neoplasia.49 The development of treatment, paraneoplastic
longitudinally extensive transverse myelitis in an older patient should prompt antibody–associated spinal
investigation for an occult tumor. cord syndromes have
emerged. Reported
NMOSD-related myelopathy has also emerged recently in the setting of
antibodies include
immune checkpoint inhibitor use. The anti–programmed cell death protein 1 anti-Hu/ANNA-1,
(PD1) antibody nivolumab and others are now standard treatment for non–small CRMP-5/anti-CV2, and
cell lung cancer and melanoma. Such patients may harbor paraneoplastic aquaporin-4 IgG.
antibodies, and aquaporin-4-IgG–seropositive NMOSD has emerged after just
one or two cycles of PD1 inhibitor chemotherapy.50 Other paraneoplastic
antibody–associated spinal cord syndromes have also been reported to emerge in
the setting of PD1 therapy.51 Reported antibodies include antineuronal nuclear
antibody type 1 (ANNA-1/anti-Hu), collapsin response mediator protein-5
(CRMP-5)/anti-CV2, and aquaporin-4 IgG. Immune checkpoint inhibitor
treatment may correlate with ANNA-1/anti-Hu levels.52 Kunchok and
colleagues53 reported CRMP-5 IgG–associated paraneoplastic myelopathy with
the programmed death ligand 1 (PD-L1) inhibitor atezolizumab. These immune
checkpoint inhibitor toxicities differ from their non–immune checkpoint
CONTINUUMJOURNAL.COM 137
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
CASE 5-7 A 62-year-old woman with kappa light chain multiple myeloma
developed back pain and was treated with local radiation to lytic lesions
at T5 and T7 in 10 daily fractions to 3000 cGy. She received multiple other
chemotherapy regimens but had progressive plasmacytomas in many
bony sites. Nine months after the radiation, she developed progressive
back pain and left leg weakness along with new lytic fractures at T12, L2
through L4, and S1 that were treated with vertebroplasty. Her gait was
further impaired by significant peripheral neuropathy from bortezomib
and pomalidomide as well as proximal weakness from multiple extended
corticosteroid courses. MRI showed enhancement of the spinal cord
from T7 through T10 without mass lesion (FIGURE 5-9) and was felt to be
most consistent with radiation myelitis. She also had chronic
compression fractures at multiple levels.
FIGURE 5-9
Imaging of the patient in CASE 5-7 with myeloma and multiple bone lesions presenting with
rapidly progressive leg weakness. The T2 signal abnormality extends beyond the radiation
fields on sagittal T2-weighted cervical (A) and thoracic (B) spine images, but the area
receiving the largest dose of radiation shows an expansile enhancing lesion on sagittal
postcontrast T1-weighted image (C, arrow).
COMMENT This case illustrates the spread of bone tumor to the spinal canal,
causing weakness and pain and complicated by radiation myelitis,
chemotherapy-associated peripheral neuropathy, and
corticosteroid-related myopathy. Multiple comorbidities must be
considered when a patient has been treated with radiation and neurotoxic
chemotherapy but also has evidence of advancing disease. Vertebroplasty
can be an effective palliative maneuver.
138 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
inhibitor–associated counterparts in that they appear after therapy has begun
and in close association with use of immune checkpoint inhibitors. The high
doses of steroids necessary to control these syndromes may reduce the
antineoplastic efficacy of immune checkpoint inhibitors. With the
ever-widening indications for these drugs, other antibody-mediated syndromes
are likely to emerge.
Neurosarcoidosis can produce both leptomeningeal and intramedullary spinal
cord pathology that can mimic neoplastic processes radiographically and in the
associated CSF formula of lymphocytic meningitis, CSF hypoglycorrhachia, and
A 47-year old woman had stage IV breast cancer, diagnosed when she CASE 5-8
was found to have thoracic compression fractures in the course of a
back-pain evaluation. She was treated systemically with denosumab,
letrozole, and palbociclib. Initial CSF cytology was positive, and she
received seven intrathecal methotrexate treatments. She continued to
have increasing back pain, which was treated with spinal radiation and
fusion. Nine months later, she had progressive leg spasms and
progressive right footdrop as well as urinary retention and within 48 hours
developed paraplegia. MRI showed extensive posterior fossa and spinal
cord leptomeningeal enhancement as well as developing hydrocephalus.
Repeat CSF cytology was again positive.
FIGURE 5-10
Imaging of the patient in CASE 5-8. Axial fluid-attenuated inversion recovery (FLAIR) MRI (A)
and axial FLAIR MRI 1 month later (B) reflect a rapid rise in intracranial pressure and
transependymal flow of CSF, with impaired CSF resorption and development of
hydrocephalus. The posterior fossa and cervical spine leptomeningeal enhancement are
visible on sagittal postcontrast T1-weighted MRI (C), consistent with carcinomatous
meningitis.
This case illustrates multiple complications of advanced breast cancer. COMMENT
MRI showed both the original bone metastases and holocord involvement,
which could be from either carcinomatous meningitis or intrathecal
methotrexate, the latter being less likely because of the interval from
treatment (FIGURE 5-10).
CONTINUUMJOURNAL.COM 139
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
elevated protein. Longitudinally extensive and sometimes enhancing lesions in
various compartments can be caused by infection. Some of the most frequently
implicated offending pathogens are Mycobacterium tuberculosis, Toxoplasma
gondii, Schistosoma, cytomegalovirus (cauda equina involvement), and West
Nile virus.
Numerous toxic/metabolic states can produce cord swelling seen on imaging
with or without gadolinium enhancement.
Although uncommon, posterior reversible encephalopathy syndrome (PRES)
can, at times, involve the spinal cord and may be longitudinally extensive,
sometimes in association with aquaporin-4 IgG.54,55
Tarlov cysts, large arachnoid cystic lesions usually in the lumbosacral area, are
often felt to be incidental findings; however, at times they can produce lumbar
and sacral radicular symptoms (including incontinence) and thus should be
evaluated for possible surgical intervention.56
CONCLUSION
Early recognition of signs and symptoms of spinal cord tumors leads to
expeditious neuroimaging that can define the compartment involved and focus
the differential diagnosis with excellent accuracy among different histologies.
Pain is the predominant symptom of spinal cord tumors and may not be
alleviated with surgical resection. Surgery is the first-line treatment of
symptomatic primary spinal cord tumors and is more effective for control of
ependymomas than for astrocytomas. The histologic grade of the tumor and
extent of resection are important determinants of outcome. Newer techniques,
including separation surgery and stereotactic radiosurgery, offer better chances
of quality survival in patients with spinal cord metastasis from systemic
malignancies. The H3 K27M mutant diffuse midline glioma has been recently
recognized, and some targeted therapies may have efficacy. Experience with
chemotherapy for recurrent spinal cord tumors is limited, although successes
with intracranial counterparts of similar histology may suggest potentially
helpful agents.
REFERENCES
1 Chamberlain MC, Tredway TL. Adult primary 5 Parks NE, Goyal G, Go RS, et al. Neuroradiologic
intradural spinal cord tumors: a review. Curr manifestations of Erdheim-Chester disease.
Neuro Neurosci Rep 2011;11(3):320-328. Neurol Clin Pract 2018;8(1):15-20. doi:10.1212/
doi:10.1007/s11910-011-0190-2 CPJ.0000000000000422
2 Ostrom QT, Cioffi G, Gittleman H, et al. CBTRUS 6 Chiapparini L, Cavalla G, Langella T, et al. Adult
Statistical Report: primary brain and other central leukoencephalopathies with prominent
nervous system tumors diagnosed in the United infratentorial involvement can be caused by
States in 2012-2016. Neuro Oncol 2019;21(suppl 5): Erdheim-Chester disease. J Neurol 2018;265(2):
v1-v100. doi:10.1093/neuonc/noz150 273-284. doi:10.1007/s00415-017-8692-8
3 Mechtler LL, Nandigam K. Spinal cord tumors: 7 Zhang M, Iyer RR, Azad TD, et al. Genomic
new views and future directions. Neurol Clin landscape of intramedullary spinal cord gliomas.
2013;31(1):241-268. doi:10.1016/j.ncl.2012.09.011 Sci Rep 2019;9(1):18722. doi:10.1038/s41598-019-
54286-9
4 Wu J, Ranjan S. Neoplastic myelopathies.
Continuum (Minneap Minn) 2018;24(2, Spinal 8 Muccilli A, Cavrol R, Kvam KA. A case of
Cord Disorders):474-496. doi:10.1212/ progressive myelopathy in a middle-aged
CON.0000000000000585 woman. JAMA Neurol 2019;76(10):1253-1254.
doi:10.1001/jamaneurol.2019.2806
140 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
9 Alvi MA, Ida CM, Paolini MA, et al. Spinal cord 22 Yi S, Choi S, Shin DA, et al. Impact of H3.3 K27M
high-grade infiltrating gliomas in adults: mutation on prognosis and survival of grade IV
clinico-pathological and molecular evaluation. spinal cord glioma on the basis of new 2016
Mod Pathol 2019;32(9):1236-1243. doi:10.1038/ World Health Organization classification of the
s41379-019-0271-3 central nervous system. Neurosurgery 2019;84(5):
1072-1081. doi:10.1093/neuros/nyy150
10 Shankar GM, Lelic N, Gill CM, et al. BRAF
alteration status and the histone H3F3A gene 23 Solomon DA, Wood MD, Tihan T, et al. Diffuse
K27M mutation segregate spinal cord midline gliomas with histone H3-K27M mutation:
astrocytoma histology. Acta Neuropathol 2016; a series of 47 cases assessing the spectrum of
131(1):147-150. doi:10.1007/s00401-015-1492-2 morphologic variation and associated genetic
alterations. Brain Pathol 2016;26(5):569-580.
11 Schindler G, Capper D, Meyer J, et al. Analysis of
doi:10.1111/bpa.12336
BRAF V600E mutation in 1,320 nervous system
tumors reveals high mutation frequencies in 24 Goldstein ED, Kyper CM, Siegel JL. Diffuse
pleomorphic xanthoastrocytoma, ganglioglioma midline glioma H3 K27M-mutant manifested as
and extra-cerebellar pilocytic astrocytoma. Acta progressive paraplegia. Neurohospitalist 2020;
Neuropathol 2011;121(3):396-405. doi:10.1007/ 10(1):73-74. doi:10.1177/1941874419847347
s00401-011-0802-6
25 Arrillaga-Romany I, Chi AS, Allen JE, et al. A phase
12 Takayima S, Hatanaka KC, Ishi Y, et al. Spinal cord 2 study of the first imipridone ONC201, a
anaplastic astrocytoma with BRAF V600E selective DRD2 antagonist for oncology,
mutation: a case report and review of literature. administered every three weeks in recurrent
Neuropathology 2020; doi:10/1111/neup12636 glioblastoma. Oncotarget 2017;8(45):
79238-79304. doi:10.18632/oncotarget.17837
13 Garnier L, Ducray F, Verlut C, et al. Prolonged
response induced by single agent vemurafenib in 26 Buerki R, Lapointe S, Solomon D, et al. Path-09.
a BRAF V600E spinal ganglioglioma: a case report Clinical characteristics of adults with H3
and review of the literature. Front Oncol 2019; K27M-mutant gliomas at UCSF. Neuro Oncol
9:177. doi:10.3389/fonc.2019.00177 2018:20(suppl 6):vi159-vi160. doi:10.1093/neuonc/
noy148.665
14 Louis DN, Perry A, Reifenberger G, et al. The
2016 World Health Organization classification of 27 Wang S, Dougan DA. The direct molecular target
tumors of the central nervous system: a for imipridone ONC201 is finally established.
summary. Acta Neuropathol 2016;131(6):803-820. Cancer Cell 2019;35(5):707-708. doi:10.1016/
doi:10.1007/s00401-016-1545-1 j.ccell.2019.04.010
15 Rawal S, Cruz JP. Case of the week: spinal cord 28 Oral ONC201 in recurrent GBM, H3 K27M glioma,
subependymomas. Published September 5, and midline glioma. ClinicalTrials.gov identifier
2019. Accessed December 4, 2020. ajnr.org/ NCT02525692. Updated January 6, 2020.
content/cow/09052019/tab-diagnosis Accessed December 4, 2020. clinicaltrials.gov/
ct2/show/NCT02525692
16 Green RM, Cloughesy TF, Stupp R, et al.
Bevacizumab for recurrent ependymoma. 29 Chi AS. Pediatric and adult H3 K27M-mutant
Neurology 2009;73(20):1677-1680. doi:10.1212/ diffuse midline glioma treated with the selective
WNL.0b013e3181c1df34 DRD2 antagonist ONC201. J Neurooncol 2019;
145(1):97-105. doi:10.1007/s11060-019-03271-3
17 Fouladi M, Stewart CF, Blaney SM, et al. Phase I
trial of lapatinib in children with refractory CNS 30 Gessi M, Gielen GH, Dreschmann V, et al. High
malignancies: a pediatric brain tumor consortium frequency of H3F3A (K27M) mutations
study. J Clin Oncol 2010;28(27):4221-4227. characterizes pediatric and adult high-grade
doi:10.1200/JCO.2010.28.4687 gliomas of the spinal cord. Acta Neuropathol
2015;130(3):435-437. doi:10.1007/s00401-
18 Landi A, Palmarini V, D'Elia A, et al. Magnetic
015-1463-7
resonance diffusion tensor imaging and
fiber-tracking diffusion tensor tractography in 31 Kotecha R, Mehta MP, Chang EL, et al. Updates in
the management of spinal astrocytomas. World J the management of intradural spinal cord
Clin Cases 2016;4(1):1-4. doi:10.12998/wjcc.v4.i1.1 tumors: a radiation oncology focus. Neuro Oncol
2019;21(6):707-718. doi:10.1093/neuonc/noz014
19 Savari AJ, Pardo C, Basques BA, Colman MW.
Review of robotic-assisted surgery: what the 32 Benesch M, Nemes K, Neumayer P. Spinal cord
future looks like through a spine oncology lens. atypical teratoid/rhabdoid tumors in children:
Ann Transl Med 2019;7(10):224-233. doi:10.21037/ clinical, genetic, and outcome characteristics in a
atm.2019.04.69 representative European cohort. Pediatr Blood
Cancer 2020;67(1):e28022. doi:10.1002/
20 Khalid S, Kelly R, Carlton A, et al. Adult intradural
pbc.28022
intramedullary astrocytomas: a multicenter
analysis. J Spine Surg 2019;5(1):19-30. 33 Omar AI. Bevacizumab for the treatment of
doi:10.21037/jss.2018.12.06 surgically unresectable cervical cord
hemangioblastoma: a case report. J Med Case
21 Minehan KJ, Brown PD, Scheithauer BW, et al.
Rep 2012;6:238. doi:10.1186/1752-1947-6-238
Prognosis and treatment of spinal cord
astrocytoma. Int J Radiat Oncol Biol Phys 2009;
73(3):727-733. doi:10.1016/j.ijrobp.2008.04.060
CONTINUUMJOURNAL.COM 141
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEOPLASTIC MYELOPATHIES
34 Riklin C, Seystahl K, Hofer S, et al. Antiangiogenic 46 Grillo A, Capasso R, Petrillo A, et al. An
treatment for multiple CNS hemangioblastomas. intramedullary “flame” recognized as being an
Onkologie 2012;35(7-8):443-445. doi:10.1159/ intramedullary spinal cord metastasis from
000341075 esophageal cancer. J Radiol Case Rep 2019;13(7):
14-20. doi:10.3941/jrcr.v13i7.3555
35 Flanagan EP, O'Neill BP, Porter AB, et al. Primary
intramedullary spinal cord lymphoma. Neurology 47 Psimaras D, Tafani C, Ducray F, et al.
2011;77(8):784-791. doi:10.1212/ Bevacizumab in late-onset radiation-induced
WNL.0b013e31822b00b9 myelopathy. Neurology 2016;86(5):454-457.
doi:10.1212/WNL.0000000000002345
36 Ahmad A, Schiff D. Multimodality therapy of
patients with refractory meningiomas. Curr Treat 48 Flanagan EP, McKeon A, Lennon VA, et al.
Options Oncol 2019;20(6):50. doi:10.1007/s11864- Paraneoplastic isolated myelopathy: clinical
019-0648-z course and neuroimaging clues. Neurology 2011;
76(24):2089-2095. doi:10.1212/
37 Dombi E, Baldwin A, Marcus LJ, et al. Activity of
WNL.0b013e31821f468f
selumetinib in neurofibromatosis type 1-related
plexiform neurofibromas. N Engl J Med 2016; 49 Sepulveda M, Sola-Valls N, Escudero D, et al.
375(26):2550-2560. doi:10.1056/NEJMoa1605943 Clinical profile of patients with paraneoplastic
neuromyelitis optica spectrum disorder and
38 Berkowitz AL, Miller MB, Mir SA. Glioproliferative
aquaporin-4 antibodies. Mult Scler 2018;24(13):
lesion of the spinal cord as a complication of
1753-1759. doi:10.1177/1352458517731914
“stem-cell tourism.” N Engl J Med 2016;375(2):
196-198. doi:10.1056/NEJMc1600188 50 Narumi Y, Yoshida R, Minami Y, et al.
Neuromyelitis optica spectrum disorder
39 Pellerino A, Buffoni L, Rudà R, Soffietti R.
secondary to treatment with anti-PD-1 antibody
Complete response of spinal metastases from
nivolumab: the first report. BMC Cancer 2018;
non-small cell lung cancer with ALK inhibitors.
18(1):95-98. doi:10.1186/s12885-018-3997-2
Neurology 2019;93(50):217-219. doi:10.1212/
WNL.0000000000007866 51 Gill A, Perez M, Bae C, et al. A case series of PD-1
inhibitor-associated paraneoplastic neurologic
40 Alghamdi M, Sahgal A, Soliman H, et al.
syndromes. J Neuroimmunol 2019;334:576980.
Postoperative stereotactic body radiotherapy
doi:10.1016/j.jneuroim.2019.576980
for spinal metastases and the impact of epidural
disease grade. Neurosurgery 2019;85(6): 52 Raibagkar P, Ho D, Gunturu KS, Srinivasan J.
E1111-E1118. doi:10.1093/neuros/nyz349 Worsening of anti-Hu paraneoplastic
neurological syndrome related to anti-PD-1
41 Xiaozhou L, Xing Z, Xin S, et al. Efficacy analysis of
treatment: case report and review of literature.
separation surgery combined with SBRT for
J Neuroimmunol 2020;341:577184. doi:10.1016/
spinal metastases—a long-term follow-up study
j.jneuroim.2020.577184
based on patients with spinal metastatic tumor in
a single-center. Orthop Surg 2020;12(2):404-420 53 Kunchok A, Zekeridou A, Pittock S. CRMP5-IgG-
doi:10.1111/os.12594 associated paraneoplastic myelopathy with
PD-L1 inhibitor therapy. JAMA Neurol 2020;77(2):
42 Yáñez ML, Miller JJ, Batchelor TT. Diagnosis and
255-256. doi:10.1001/jamaneurol.2019.4379
treatment of epidural metastases. Cancer 2017;
123(7):1106-1114. doi:10.1002/cncr.30521 54 Magaña SM, Matiello M, Pittock SJ, et al.
Posterior reversible encephalopathy syndrome
43 Barzilai O, Laufer I, Yamada Y, et al. Integrating
in neuromyelitis optica spectrum disorders.
evidence-based medicine for treatment of
Neurology 2009;72(8):712-717. doi:10.1212/01.
spinal metastases into a decision framework:
wnl.0000343001.36493.ae
neurologic, oncologic, mechanicals stability, and
systemic disease. J Clin Oncol 2017;35(21): 55 De Havenon A, Joos Z, Longenecker L, et al.
2419-2427. doi:10.1200/JCO.2017.72.7362 Posterior reversible encephalopathy syndrome
with spinal cord involvement. Neurology 2014;
44 Pruitt AA. Epidemiology, treatment, and
83(22):2002-2006. doi:10.1212/
complications of central nervous system
WNL.0000000000001026
metastases. Continuum (Minneap Minn) 2017;
23(6, Neuro-oncology):1580-1600. doi:10.1212/ 56 Oaklander AL, Long DM, Larvie M, Davidson CJ.
CON.0000000000000551 Case Records of the Massachusetts General
Hospital. Case 7-2013. A 77-year-old woman with
45 Rykken JB, Diehn FE, Hunt CH, et al. Rim and
long-standing unilateral thoracic pain and
flame signs: postgadolinium MRI findings
incontinence. N Engl J Med 2013;368(9):853-861.
specific for non-CNS intramedullary spinal cord
doi:10.1056/NEJMcpc1114034
metastases. AJNR Am J Neuroradiol 2013;34(4):
908-915. doi:10.3174/ajnr.A3292
142 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Neuroimaging of Spinal REVIEW ARTICLE
Cord and Cauda Equina CONTINUUM AUDIO
INTERVIEW AVAILABLE
ONLINE
Disorders
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNrC3bBuCzr1RdmqNUpjE4IY on 04/28/2022
By Felix E. Diehn, MD; Karl N. Krecke, MD, FACR
ABSTRACT
PURPOSE OF REVIEW: This article reviews the neuroimaging of disorders of the
spinal cord and cauda equina, with a focus on MRI. An anatomic approach
is used; diseases of the extradural, intradural-extramedullary, and
intramedullary (parenchymal) compartments are considered, and both
neoplastic and non-neoplastic conditions are covered. Differentiating
imaging features are highlighted.
RECENT FINDINGS:Although T2-hyperintense signal abnormality of the spinal
cord can have myriad etiologies, neuroimaging can provide specific
diagnoses or considerably narrow the differential diagnosis in many cases.
Intradural-extramedullary lesions compressing the spinal cord have a
limited differential diagnosis and are usually benign; meningiomas and
schwannomas are most common. Extradural lesions can often be CITE AS:
CONTINUUM (MINNEAP MINN)
specifically diagnosed. Disk herniations are the most commonly 2021;27(1, SPINAL CORD DISORDERS):
encountered mass of the epidural space. Cervical spondylotic myelopathy 225–263.
can cause a characteristic pattern of enhancement, which may be
mistaken for an intrinsic myelopathy. A do-not-miss diagnosis of the Address correspondence to
Dr Felix E. Diehn, Department of
extradural compartment is idiopathic spinal cord herniation, the Radiology, Division of
appearance of which can overlap with arachnoid cysts and webs. Neuroradiology, 200 First St SW,
Rochester, MN 55905,
Regarding intrinsic causes of myelopathy, the lesions of multiple sclerosis
diehn.felix@mayo.edu.
are characteristically short segment but can be confluent when multiple.
Postcontrast MRI can be particularly helpful, including when attempting to R E L A T I O N SH I P D I S C LO SU R E :
Dr Diehn has received personal
differentiate the long-segment myelopathy of neurosarcoidosis and compensation for travel
aquaporin-4 (AQP4)-IgG–seropositive neuromyelitis optica spectrum disorder expenses for speaking
(NMOSD) and when characterizing spinal cord tumors such as primary engagements from the
American Academy of
neoplasms and metastases. Spinal dural arteriovenous fistula is another Neurology, the American
do-not-miss diagnosis, with characteristic MRI features both precontrast and Academy of Pain Medicine,
postcontrast. Tract-specific white matter involvement can be a clue for Mayo Clinic Department of
Radiology, and the Spine
diseases such as subacute combined degeneration, paraneoplastic Intervention Society. Dr Krecke
myelopathy, and radiation myelitis, whereas gray matter–specific reports no disclosure.
involvement can suggest conditions such as cord infarct, viral myelitis, or UNLABELED USE OF
myelin oligodendrocyte glycoprotein (MOG)-IgG associated disorder. PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
Drs Diehn and Krecke report no
SUMMARY: Knowledge of the neuroimaging findings of the many causes of disclosures.
spinal cord and cauda equina dysfunction is critical for both neurologists
and neuroradiologists. A structured approach to lesion compartmental
© 2021 American Academy
location and imaging feature characterization is recommended. of Neurology.
CONTINUUMJOURNAL.COM 225
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
INTRODUCTION
I
n patients with myelopathy, spinal cord signal abnormality on MRI,
particularly increased T2 signal, can occur with a wide variety of diseases
intrinsic and extrinsic to the spinal cord. To arrive at a specific diagnosis for
such myelopathic signal abnormality or a limited imaging differential
diagnosis, additional clinical and imaging features must be evaluated. The
preceding articles in this issue detail many of the clinical considerations and
therefore these are not further discussed here. Such additional imaging features
include, but are not limited to, the cross-sectional pattern of involvement, the
longitudinal extent, cord expansion, associated findings in the spinal cord,
enhancement, any extrinsic compressive/adhesive cause of myelopathic signal,
and findings outside the spinal canal. A complete workup that includes MRI can
more often than not provide a specific diagnosis for a patient’s myelopathy.1 The
wastebasket term idiopathic transverse myelitis, which is a diagnosis of exclusion,
should generally not be used in MRI interpretations at primary presentation.2
This article focuses on causes of myelopathy for which advanced imaging
(particularly MRI but also CT or CT myelography) can provide specific
diagnoses or short lists of differential considerations.
Select extrinsic causes of myelopathy are discussed first, since compression of
the cord/cauda equina is more common than intrinsic myelopathy and the
imaging findings can often specifically identify the disease process. This is
followed by a discussion of intrinsic cord diseases. Because of space constraints,
acute traumatic myelopathy (eg, fractures, traumatic malalignment, traumatic
disk herniations, cord contusion/hemorrhage) is not considered specifically
herein, nor are neurodegenerative/hereditary myelopathies. The brain MRI
findings that can help diagnose diseases such as multiple sclerosis (MS) are also
not included.
SPINAL CORD IMAGING BASICS
MRI is the principal modality for anatomic evaluation of the spinal cord and canal
(TABLE 10-13). The ability of MRI to noninvasively demonstrate and differentiate
structures of the extradural, intradural-extramedullary, and intramedullary
compartments in multiple anatomic planes is unparalleled. Radiographs, CT, CT
myelography, conventional angiography, and CT angiography have more
limited applications. CT of the spine is the modality of choice for trauma settings
because of speed of acquisition and wide availability. As a first-line modality,
the fundamental magnetic and radiofrequency environment of MRI systems is
relatively inhospitable to the patient who is acutely traumatized, the necessary
support devices, and personnel. Patients presenting with myelopathy may be
intolerant of or unsafe for the MRI environment because of claustrophobia, body
habitus, or critical medical devices. CT myelography can be a robust technique
in these patients.
The standard MRI protocol of the spine relies on T1-weighted and
T2-weighted sequences (TABLE 10-2) (FIGURE 10-1). Together, they produce
outstanding evaluation of the extradural and intradural-extramedullary spaces.
Higher sensitivity evaluation of the cord parenchyma is achieved by adding a
sagittal T2-weighted short tau inversion recovery (STIR) sequence optimized to
cord signal abnormality (inversion time of approximately 110 ms to 130 ms)
rather than bone or paraspinal signal abnormality (inversion time of
226 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Utility of Various Advanced Spinal Imaging Modalities in Evaluating the TABLE 10-1
Spinal Cord
Modality Clinical scenario Comments
MRI First line for any suspected nontraumatic For initial complete evaluation of a myelopathy
myelopathy; follow-up of most or suspected/known infection/active
myelopathies; in acute traumatic inflammation/neoplasm/vascular cause,
myelopathy after initial evaluation with CT should be performed without and with IV
to assist in spinal canal evaluation and gadolinium; include segments of spine
potential operative planning clinically affected; protocol used depends on
indication (refer to TABLE 10-2)
Magnetic resonance Suspected or known vascular myelopathy; Typically performed with IV gadolinium; not a
angiography (MRA) workup of myelopathy demonstrated on substitute for conventional angiography but
MRI of unknown cause; arterial dissection can help guide spinal angiography if suggests
(including vertebral artery) level of dural arteriovenous fistula; CT
angiography is an infrequently used
alternative, especially if patient not an MRI
candidate or MRI is not available; CT
angiography is first line for acute arterial injury
CT Acute trauma; assess for degree of Soft tissue attenuation lesions in the canal may
calcification/ossification of a compressive be difficult/impossible to discriminate from
lesion, degree of osseous stenosis; CSF/cord
reasonable first-line examination (over CT
myelography) if patient not an MRI
candidate or MRI is not available; assess
margins/nature of osseous lesions causing
compressive myelopathy seen on MRI
Conventional myelography Patient not an MRI candidate or MRI is not Minimally invasive; dynamic capabilities
and postmyelography CT available (including when CT has not (temporal: initial contrast flow at level of a
diagnosed the cause of a myelopathy); space-occupying lesion; positional: lateral
surgical planning or problem solving; decubitus, prone); other uses include
differentiation of arachnoid cyst, arachnoid evaluation of spontaneous intracranial
web, and spinal cord herniation; assess hypotension/CSF leak (usually not in a setting
dynamic nature of lumbar spinal stenosis of myelopathy)
with standing cone-beam technique
Conventional angiography Dural arteriovenous fistula (localizing level Minimally invasive; MRA can inform search for
and, in appropriate cases, treatment); other fistula and decrease time/radiation dose;
spinal vascular malformation, including complete examination is from vertebral to
arteriovenous malformation; spinal internal iliac arteries; CT angiography is an
vasculitis; localize artery of Adamkiewicz alternative for artery of Adamkiewicz
localization
Fludeoxyglucose positron Not typically used primarily for myelopathy Spinal canal a relative blind spot; normal
emission tomography but most commonly for metastatic workup variant increased uptake of conus; both
(FDG-PET) CT of many suspected/known malignancies neoplastic and, less commonly, inflammatory
causes may show increased uptake3
CSF = cerebrospinal fluid; CT = computed tomography; IV = intravenous; MRI = magnetic resonance imaging.
CONTINUUMJOURNAL.COM 227
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
approximately 150 ms to 170 ms). Axial plane imaging of cord and canal is most
effective using T2-weighted techniques. Cord gray-white differentiation is best
appreciated on axial images, with the gray matter expected to be slightly more
hyperintense than the white matter. An axial gradient recalled echo (GRE)
sequence can demonstrate the gray-white differentiation to better advantage
than T2-weighted images; the inherently normal gray matter hyperintensity on
this sequence relative to white matter should not be mistaken for abnormal. GRE
sequences also have fewer CSF flow artifacts. Together and in conjunction with
sagittal sequences, the two axial sequences can be complementary in evaluating
intradural anatomy and pathology. IV administration of gadolinium with
postcontrast T1-weighted imaging performed in at least the sagittal plane, if not also
the axial plane, is recommended for complete evaluation of suspected intrinsic
myelopathy with blood–spinal cord barrier breakdown (eg, infectious, active
inflammatory, vascular, or neoplastic causes). Inclusion of diffusion-weighted
imaging (DWI) in the MRI protocol is suggested for any hyperacute or acute
myelopathy, particularly to help assess for infarct.4
CT myelography involves percutaneous intrathecal access and injection of
iodinated contrast material, typically via lumbar puncture with fluoroscopic
TABLE 10-2 MRI Protocols for Nontraumatic Myelopathy
Indication Tailored MRI protocol
Nontraumatic Basic protocol:
Sagittal: T1-weighted; T2-weighted; short tau inversion recovery (STIR) optimized for
cord signal abnormality or proton densitya (myelopathy sequence); with or without
T2-weighted fat-suppressed sequence (STIR or fat saturation), especially if axial pain
is present, as this helps evaluate for edema-type signal abnormality in bones/
paraspinal soft tissues
Axial: T2-weighted; with or without gradient recalled echo (GRE)a
Initial complete evaluation includes postgadolinium sagittal with or without axial
T1-weighted (fat suppression is based on radiologist preference, but strictly speaking
not needed for intramedullary disease)a
Vascular Basic protocol as above, including gadolinium; diffusion-weighted imaging if
hyperacute/acutea; magnetic resonance angiography (MRA)a; consider thin-section
heavily T2-weighted three-dimensional GRE steady state sequencesb for dural
arteriovenous fistula; consider GRE (sagittal with or without axial) for blood products
Neoplasm, infection, active Basic protocol as above, including gadolinium; sagittal with or without axial
inflammation T2-weighted fat-suppressed sequence (STIR or fat saturation)a; include fat saturation
on postgadolinium T1-weighted images in at least one plane (sagittal or axial);
consider diffusion-weighted imaginga if abscess suspected
Spinal cord herniation, arachnoid Basic protocol as above; consider thin-section heavily T2-weighted three-
cyst, arachnoid web dimensional GRE steady state sequencesb
Scoliosis Basic protocol as above; consider coronal plane (T2-weighted with or without
T1-weighted)
MRI = magnetic resonance imaging.
a
Sequences that ordering clinicians may want to specifically ask for in MRI request to ensure they are included.
b
Examples include fast imaging employing steady state acquisition (FIESTA) and constructive interference in steady state (CISS).
228 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 10-1
Normal spinal cord and cauda equina. Multiplanar multisequence images of the cervical
(A through F), thoracic (G through J, N, O), and lumbar (K through M, P, Q) spine. The spinal
cord contour is smooth throughout. The signal intensity of the spinal cord is relatively
homogeneous, especially on sagittal images. Sagittal short tau inversion recovery (STIR)
sequences optimized to detect spinal cord signal abnormality (cervical, B; thoracic, H)
demonstrate mild normal T2 hyperintensity of cord gray matter more so than standard
T2-weighted images. Gray-white differentiation is better appreciated on axial gradient
recalled echo (GRE) (F) than conventional T2-weighted (E) images; the former are most useful
in the cervical spine. CSF flow voids are more evident on axial T2-weighted (E, N, arrows)
than GRE (F) images. Postcontrast, the basivertebral plexus accumulates gadolinium (D, J, M,
arrows) and thus enhances compared to unenhanced T1-weighted images (C, I, L). The spinal
cord expands slightly at the conus (sagittals G through J, K through M; axials O). The tip of the
conus is normally above the L2-L3 interspace level; in this patient, it is at L1 (P). The cauda
equina nerve roots are anatomically distributed and layer dependently posteriorly within the
thecal sac in this supine patient (K, P, Q); they do not normally demonstrate appreciable
enhancement (M). Fat suppression was employed on the postcontrast lumbar spine sagittal
T1-weighted images but is not specifically necessary when evaluating the spinal cord and
cauda equina.
CONTINUUMJOURNAL.COM 229
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-2
Normal variant and artifacts of the spinal cord. The central canal of the spinal cord is an
ependyma-lined CSF space that can be mildly prominent as an anatomic variant (A through
E); this is not a pathologic syrinx. Artifactual spinal cord signal abnormality (F through K) can
occur for a variety of reasons, such as patient motion (eg, respiration, swallowing); it is
usually more apparent on short tau inversion recovery (STIR) (H, I) than on conventional
T2-weighted images (F, G). Evaluation of the spinal cord in two planes is essential; axial
images (J, K) in this patient do not confirm the apparent T2 hyperintensity seen on sagittal
images. Artifactual cord enhancement (L through N) can occur for similar reasons. Often, it is
seen only in one of the two planes (seen sagittally in L and M but not axially in N, and no
corresponding cord T2 hyperintensity is seen [O, P]). CSF flow artifact (Q, R) can simulate
intrathecal pathology to the uninitiated; it is most apparent on conventional T2-weighted
images (Q, R, arrows), and in this patient was misconstrued as nodular drop metastases. Note
that it is not evident on the T1-weighted image (S) and does not enhance (T). In patients
with chronic repetitive subarachnoid hemorrhage resulting in superficial siderosis, the
low-signal-intensity hemosiderin that coats the pial surface of the spinal cord and conus
(U through W, white arrows) can cause an artifact of pseudoparenchymal T2 hyperintensity
(blue arrows, V, W).
230 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
guidance. Although myelography has decreased in popularity over the years, it is KEY POINTS
a low-risk technique for evaluating myelopathy in patients poorly suited for MRI,
● IV administration of
for surgical planning, and for problem solving, including for clarifying the gadolinium with
differential diagnosis of arachnoid cyst, arachnoid web, and idiopathic spinal postcontrast T1-weighted
cord herniation. Myelography can also allow real-time observation of CSF imaging performed in at
dynamics and tailored patient positioning. least the sagittal plane, if
not also the axial plane, is
recommended for complete
Normal Anatomy and Anatomic Variants evaluation of suspected
A slight expansion of the cord is evident in the cervical-thoracic region, from intrinsic myelopathy with
approximately C3 through T2. The thoracolumbar region of the spinal cord also blood–spinal cord barrier
breakdown.
expands slightly from approximately T9 through T12 before it progresses
inferiorly to form the conus. These normal expansions may be missing in the ● Inclusion of diffusion-
pathologically atrophic cord, which is a nonspecific morphology that can be weighted imaging in the
short or long segment. Cord atrophy can result from essentially any chronic or MRI protocol is suggested
treated cause of myelopathy as well as from hereditary/neurodegenerative for any hyperacute or acute
myelopathy, particularly to
myelopathies. help assess for infarct.
The conus is normally located no lower than L2-L3. An ependyma-lined
central canal is located within the spinal cord. This extends from the inferior ● The central canal can be
aspect of the fourth ventricle to the tip of the conus, where it slightly dilates physiologically prominent
and thereby evident as a
transiently during childhood into the normal ventriculus terminalis
normal variant on MRI; this is
(the so-called fifth ventricle), which is rarely seen in adults. The central canal can thin, usually only a few
be physiologically prominent and thereby evident as a normal variant on MRI; millimeters in diameter, and
this is thin, usually only a few millimeters in diameter, and should not be should not be confused with
a syrinx.
confused with a syrinx (FIGURE 10-2). A syrinx (syringohydromyelia) is
pathologic fluid within the spinal cord (central canal or parenchyma) and can ● The normal gray matter is
have a wide variety of causes; when encountered for the first time, this finding slightly more hyperintense
should be evaluated with MRI without and with contrast to exclude a neoplastic than the white matter, which
cause. Findings that suggest a syrinx over a physiologically prominent central may simulate abnormal T2
hyperintensity anteriorly
canal include a beaded appearance, eccentric location, cord enlargement, and centrally on sagittal
surrounding T2 hyperintensity, and an associated solid mass or enhancement. T2-weighted images.
For a complete discussion of the anatomy of the spinal cord, refer to the article
“Spinal Cord Anatomy and Localization” by Todd A. Hardy, PhD, MBBS,
FRACP,5 in this issue of Continuum.
Pitfalls
A few pitfalls regarding the use of MRI for myelopathy deserve specific mention.
The normal gray matter is slightly more hyperintense than the white matter,
which may simulate abnormal T2 hyperintensity anteriorly and centrally on
sagittal T2-weighted images (FIGURE 10-1). Second, patient motion can cause
apparent but artifactual signal abnormality, including false-positive T2
hyperintensity in the cord (FIGURE 10-2). Third, adjacent to the cord, CSF flow
artifact can confound; it can be particularly prominent on conventional
T2-weighted images (FIGURE 10-2). Especially on axial images, this artifactual T2
hypointensity can simulate extradural or intradural lesions such as disk
herniations, osteophytes, or nerve sheath tumors. As artifact, it often cannot be
confirmed as truly lesional on sagittal images or other sequences. Axial GRE
images are less susceptible to such motion artifact and can help problem solve.
Fourth, chronic repetitive subarachnoid hemorrhage can result in superficial
siderosis. In this condition, the T2-hypointense hemosiderin that coats the spinal
cord can cause the parenchyma to appear relatively T2 hyperintense
CONTINUUMJOURNAL.COM 231
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
(pseudomyelopathic signal abnormality) (FIGURE 10-2). Finally, contrast-enhanced
features are critical for correctly diagnosing a myelopathy (TABLE 10-3).
However, apparent enhancement on postcontrast T1-weighted images is not
always true enhancement. Precontrast images should always be reviewed for
inherently T1-hyperintense substances (such as blood products) that can
simulate enhancement on postgadolinium images.
COMPARTMENT APPROACH TO MYELOPATHY
The spinal canal can be divided into the extradural, intradural-extramedullary,
and intramedullary compartments. Each compartment contains unique
anatomic and histologic structures, greatly informing and simplifying the
differential diagnosis of lesions in each compartment (FIGURE 10-3). Extrinsic
causes of myelopathy or cauda equina symptoms can occur in the
intradural-extramedullary and extradural compartments. The intramedullary
compartment includes the parenchyma (spinal cord and conus).
Extradural Compartment
A wide variety of spinal or paraspinal lesions, both benign and malignant, may
cause myelopathy or cauda equina symptoms by compression of neural tissue.
Selected causes that are important to recognize are discussed here.
DISK HERNIATIONS. The most common mass in the epidural space is a disk
herniation. Most disk herniations are located in the ventral/ventrolateral epidural
space and remain in anatomic continuity with their parent disk, a key clue to
the diagnosis. The disk herniation, especially when acute/subacute, may not
have the same signal characteristics as the parent disk, which can cause
confusion. Less commonly encountered locations for disk herniations that can
compress neural tissue include the lateral/dorsal epidural space and the
intradural compartment (FIGURE 10-4).6 A highly prevalent finding for dorsal
disk herniations is that the abnormal epidural soft tissue still typically maintains
continuity with the parent disk in the ventrolateral epidural space, wrapping
around the thecal sac dorsally.7 Because of a lack of familiarity with this less
commonly encountered location of disk herniation and given the often-acute
clinical presentation with cauda equina syndrome, such dorsal herniations are
frequently initially misdiagnosed as epidural hematomas, epidural abscesses, or
synovial cysts. Misdiagnosis occurs in part because any of these lesions, including
disk herniations, can and often do demonstrate peripheral enhancement.
Peripheral enhancement is expected for disk herniations because of the
surrounding inflammatory/fibrotic reaction. It is also the rule for synovial cysts
and epidural abscesses (FIGURE 10-4). An additional uncommon location for disk
herniations is the intradural compartment (FIGURE 10-4). In the lumbar spine,
occasionally the dorsal edge of an intradural disk herniation may demonstrate a
sharp posterior edge, the so-called hawk-beak sign.8 Although disk herniations in
the thoracic spine are commonly asymptomatic, they have a propensity to
calcify, especially when giant. Such giant calcified disk herniations have a
tendency to erode the dura and be intradural.6 The calcified nature of a disk
herniation is most easily appreciated on CT; on MRI, this often manifests as very
low signal on T1-weighted and T2-weighted images. A clue to the diagnosis of
any disk herniation is air within the lesion (ie, the vacuum phenomenon) due to
accumulation of nitrogen gas.
232 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SYNOVIAL CYSTS. The spectrum of posterior element spondylotic changes includes KEY POINTS
synovial cysts (also known as facet joint cysts), which are most common in
● The most common mass
the lumbar spine, particularly at L4-L5. Although most such synovial cysts are in the epidural space is a
small and asymptomatic and often even external to the spinal canal,9 some can disk herniation. Most disk
impair the traversing cauda equina nerve roots as the cysts project typically herniations are located in
anteromedially from the facet joint into the spinal canal (FIGURE 10-4). Anatomic the ventral/ventrolateral
epidural space and remain in
continuity with the adjacent arthropathic facet joint in at least one plane allows
anatomic continuity with
confident diagnosis on MRI but is not always identifiable. Additional clues to the their parent disk, a key clue
diagnosis are arthropathy of the adjacent facet joint, including increased fluid to the diagnosis.
within the joint; characteristic location laterally within the spinal canal, including
in the lateral recess (although other locations, including foraminal and dorsal ● A highly prevalent finding
for dorsal disk herniations is
midline, also occur); fluidlike or heterogeneous internal signal intensity of the that the abnormal epidural
cyst; and a sometimes relatively thick and T2-hypointense rim that typically soft tissue still typically
enhances after contrast (FIGURE 10-4). The heterogeneous internal signal maintains continuity with the
characteristics of synovial cysts are wide-ranging and include T1 and T2 parent disk in the
ventrolateral epidural
hypointensity or hyperintensity or a combination. CT can more readily identify space, wrapping around the
the calcification that synovial cysts may harbor in their wall or internally. thecal sac dorsally.
EXTRADURAL HEMATOMAS AND ABSCESSES. Extradural hematomas and abscesses ● The heterogeneous
internal signal
are more commonly epidural than subdural. A history of trauma, spinal
characteristics of synovial
procedure/surgery, or anticoagulated/coagulopathic state can be a helpful clue to cysts are wide-ranging and
the diagnosis of extradural hematoma. The signal characteristics of spinal include T1 and T2
hematomas can be quite variable because of the inherently complex signal of hypointensity or
blood products and the varying possible and potentially mixed age contents of hyperintensity or a
combination.
such collections.10
Confident diagnosis of an extradural abscess can be aided by symptoms, signs, ● MRI of extradural
and laboratory markers of infection. MRI of extradural abscesses may show abscesses may show
associated adjacent inflammatory changes, including in the paraspinal soft associated adjacent
inflammatory changes,
tissues and bones, or frank findings of spondylodiskitis (FIGURE 10-4).11 The including in the paraspinal
inflammatory changes, phlegmon, or abscess are often best visualized on images soft tissues and bones, or
with fat suppression, which are critical sequences in this setting. On T2-weighted frank findings of
fat-suppressed images, hyperintensity is expected, and on postgadolinium spondylodiskitis.
T1-weighted fat-suppressed images, enhancement will be present. Extradural
● On CT, ossification of the
abscesses should enhance peripherally, with central fluidlike T2-hyperintense posterior longitudinal
and T1-hypointense contents (FIGURE 10-4). ligament is readily
identifiable as flowing
ossification along the
OSSIFICATION OF THE POSTERIOR LONGITUDINAL LIGAMENT. Ossification of the
expected course of the
posterior longitudinal ligament may cause compression of the spinal cord, alone posterior longitudinal
or in combination with spondylotic changes (FIGURE 10-5). It is implicated in up ligament in and along the
to one-fourth of cases of cervical myelopathy and is most common in the cervical midline at the ventral aspect
spine.12 On CT, ossification of the posterior longitudinal ligament is readily of the spinal canal.
identifiable as flowing ossification along the expected course of the posterior
longitudinal ligament in and along the midline at the ventral aspect of the spinal
canal. Like diskal calcifications or marginal osteophytes, the ossification can be
limited to disk space/endplate levels. However, it is also typically continuous and
located posterior to vertebral bodies. On axial images, particularly on CT,
characteristic inverted T morphology may be identified. Because of its dense
osseous nature, when mature, ossification of the posterior longitudinal ligament
signals hypointense on T1-weighted and T2-weighted images and does not
enhance; the hypointensity becomes more prominent on GRE images (called
CONTINUUMJOURNAL.COM 233
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
TABLE 10-3 Specific Enhancement Findings in the Diagnosis of T2-hyperintense Spinal
Cord Lesionsa
Enhancement findings
Disease postgadolinium Other key helpful MRI findings
Extradural
Cervical spondylotic (compressive) Pancakelike on sagittal, at/just Spondylotic changes causing cord
(FIGURES 10-5G through 10-5R) below maximal stenosis, within compression, which may be
larger region of increased T2 greatest in extension
signal; often peripheral on axial,
sparing gray matter
Disk herniation (FIGURES 10-4A through 10-4Q); Peripheral enhancement Disk herniation: usually ventral
synovial cyst (FIGURES 10-4R through 10-4W); expected for these lesions (acute epidural but can be lateral/dorsal,
epidural or subdural hematoma hematoma usually does not rarely intradural
or abscess (FIGURES 10-4X through 10-4AA) enhance)
Synovial cyst: may have complex
internal signal with or without
T2-hypointense rim
Abscess: usually has associated
inflammatory changes elsewhere,
such as in bone/disks
(osteomyelitis-diskitis) and
paraspinal regions
Hirayama disease (FIGURES 10-7G through 10-7R) Robust enhancement of the Loss of cervical kyphosis, loss of
enlarged dorsal epidural space on dural attachment, asymmetric
flexion cord atrophy/flattening, focal
myelomalacia
Intrinsic: neoplastic-primary
Ependymoma (FIGURES 10-11A through 10-11I) Typically present, well-defined Central location, relatively well
defined, cystic change, cap sign
(polar hemorrhage)
Astrocytoma (FIGURES 10-11J through 10-11P) Usually present but may not be; Eccentric location, relatively
may be patchy/ill-defined/subtle poorly defined, can be holocord
Hemangioblastoma (FIGURES 10-11Q through 10-11V) Avidly enhancing nodule on cord With or without cyst, with
surface, often dorsally significant cord edema/syrinx for
lesion size; if von Hippel-Lindau
disease, often multiple, with or
without lesions in posterior
fossa, with or without cysts/
neoplasms in pancreas, kidneys,
adrenal glands
Intrinsic: neoplastic-secondary
Metastasis (FIGURES 10-11W through 10-11BB) Rim, flame, and/or central Significant cord edema for lesion
dot signs size, evidence for other metastatic
disease with or without
primary tumor
CONTINUED ON PAGE 235
234 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
CONTINUED FROM PAGE 234
Enhancement findings
Disease postgadolinium Other key helpful MRI findings
Intrinsic: demyelinating/immune-mediated/
inflammatory
Multiple sclerosis Enhancing lesion(s) when acute/ Small, peripheral, multiple; usually
active; ill-defined, solid/nodular, no cord enlargement
ring, or partial ring
Aquaporin-4-IgG neuromyelitis optica Ring/partial ring, of a Cervicomedullary junction
spectrum disorder (NMOSD) long-segment myelopathy involved; T1-hypointense
(FIGURES 10-12H through 10-12T) components,T2-hyperintense
spotty foci
Neurosarcoidosis (FIGURES 10-12U through 10-12EE) Along dorsal subpial/pial aspect With or without hilar/mediastinal
of a long-segment myelopathy; adenopathy; with or without
with or without extension into meningeal more than osseous
central canal (trident sign); may lesions
persist over months
Myelin oligodendrocyte glycoprotein Lacking or mild Multiple longitudinally extensive
(MOG)-IgG–associated myelitis lesions predominate; T2
(FIGURES 10-12FF through 10-12KK) hyperintensity confined to gray
matter; thoracolumbar
Paraneoplastic (FIGURES 10-13I through 10-13N) Tract-specific when present Long segment; evidence for
primary tumor with or without
metastatic disease
Intrinsic: vascular
Infarct (FIGURES 10-14A through 10-14L) Anterior cord/central gray if Restricted diffusion when acute
anterior spinal artery infarct;
associated bone infarcts typically
enhance, and cauda equina may
enhance (both usually in subacute
phase)
Dural arteriovenous fistula Vascular-type along conus/cord T2-hypointense flow voids along
(FIGURES 10-14M through 10-14V) surface (serpiginous, conus/cord surface; parenchymal
corresponding to T2-hypointense T2-hyperintense signal sparing
flow voids); parenchyma may periphery
enhance, including missing
piece sign
Cavernous malformation Minimal, if any (apparent Heterogeneity (blood products),
(FIGURES 10-14W through 10-14CC) enhancement may reflect including blooming on gradient
inherent T1 hyperintensity) recalled echo (GRE) imaging;
edema if hemorrhage is acute/
subacute; blood products in
adjacent spinal cord extending
craniocaudally
IgG = immunoglobulin G.
a
Many other causes of myelopathy can enhance, especially if in an acute/active phase, but variably so and without such relatively specific patterns.
CONTINUUMJOURNAL.COM 235
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-3
Causes of nontraumatic myelopathy identifiable on imaging, based on location and category.
ADEM = acute disseminated encephalomyelitis; AIDP = acute inflammatory demyelinating
polyradiculoneuropathy; ALS = amyotrophic lateral sclerosis; AQP4 = aquaporin-4; AVF = arteriovenous
fistula; AVM = arteriovenous malformation; CIDP = chronic inflammatory demyelinating
polyradiculoneuropathy; CSF = cerebrospinal fluid; MOG = myelin oligodendrocyte glycoprotein;
MRI = magnetic resonance imaging; NMOSD = neuromyelitis optica spectrum disorder; OPLL = ossification
of the posterior longitudinal ligament.
a
Discussed in detail and/or illustrated specifically in this article.
236 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 10-4
Disk herniations in unusual locations and other common peripherally enhancing extradural
lesions. Dorsal disk herniations (A through H) can cause diagnostic uncertainty on imaging,
even for neuroradiologists. A clue to a disk herniation in any location can be the presence
of air within the lesion (A, B, white arrows); this is an extension of the intradiskal vacuum
sign that occurs as a result of accumulation of nitrogen gas within a degenerated disk.
When located in the dorsal epidural space, disk herniations (A through H, white arrows)
tend to still demonstrate a connection with the parent disk in the ventral epidural space
(B, black arrow; C, D, H, blue arrows). In this patient, the dorsal disk herniation migrates
cranial and caudal to the parent L4-L5 interspace, and like disk herniations in any location,
peripherally enhances (G, H). Intradural disk herniations (I through Q, white arrows) are
uncommon. Air within the lesion (P, Q), peripheral enhancement (K, N), and continuity with
adjacent parent disk material in the ventral epidural space can be clues to the diagnosis.
CT myelography can be used to problem solve (O, Q), in this case confirming the diagnosis
by demonstrating a partially air-containing intrathecal filling defect. Synovial cysts
(R through W, white arrows) can have variable signal characteristics. The rim of the lesion
may be T2 hypointense (R, T, white arrows), and this rim typically enhances (V, W, white
arrows). Connection to or at least continuity with an arthropathic facet joint (T, blue arrow)
can be a helpful clue. Epidural abscesses (X through AA) (and subdural abscesses, not
shown) also peripherally enhance (Y, AA, white arrows). The central aspect of the lesion
should be T2 hyperintense (X) and T1 hypointense (Y through AA), owing to the purulent
contents. Adjacent findings of spondylodiskitis, such as diskal T2 hyperintensity
(X, arrowhead), vertebral body T2 hyperintensity, and contrast enhancement suggesting
osteomyelitis (X, Y, blue arrows), can be helpful clues.
CONTINUUMJOURNAL.COM 237
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-5
Extradural benign compressive cervical and thoracic myelopathy. Ossification of the
posterior longitudinal ligament (A through F) can cause significant spinal cord compression
even in the absence of appreciable spinal cord T2 hyperintensity (A, C, D). It can have
variable signal characteristics, but most commonly mature bone signals hypointense on
T2-weighted and T1-weighted images (A and C; B, respectively). Because of the osseous
nature, the ossified ligament often appears more prominent on gradient recalled echo (GRE)
imaging (D). CT can more definitely characterize this entity (E, F). The ossification involves not
only disk space but also vertebral body levels, a finding that distinguishes it from
disk-osteophyte complexes at interspace levels. Cervical spondylotic (compressive)
myelopathy (G through J, K through N, O through R, three different MRI dates in the same
patient) can present with characteristic imaging findings but may be confused with
inflammatory/neoplastic myelopathy. On the initial sagittal T2-weighted image of this
patient, the spinal cord compression is related to both anterior (G, blue arrow) and posterior
(G, white arrow) spondylotic changes (ie, a disk osteophyte complex and ligamentum flavum
redundancy, respectively). T2 hyperintensity of the spinal cord is longitudinal, spindle-shaped,
and mildly expansile (G, H). A characteristic enhancement pattern features peripheral
distribution (white matter involvement, sparing gray matter) in the axial plane (I) and
pancakelike morphology at/just caudal to the cord compression in the sagittal plane (J, white
arrow). After an anterior decompressive surgery, the findings persisted (K through N), as they
may for months to even years, with the spinal cord mildly expanding into the more
capacious canal. The patient underwent posterior decompressive surgery, and the characteristic
findings again persisted (O through R), which is common. Thoracic spondylotic (compressive)
myelopathy (S through V) occurs with lower frequency than its cervical counterpart; most
spondylotic changes encountered in the thoracic spinal canal are asymptomatic. Findings can be
similar, including cord compression from anteriorly or posteriorly (S, blue arrow; S, U, V, white
arrows, respectively) and focal enhancement (T, white arrow).
238 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
blooming) (FIGURE 10-5). It can cause significant spinal cord compression, but KEY POINT
owing to its slow chronic development, spinal cord T2 hyperintensity may be
● After gadolinium
minimal or absent (FIGURE 10-5). Ossification of the posterior longitudinal administration, T1-weighted
ligament can be seen in association with diffuse idiopathic skeletal hyperostosis images in cervical
(DISH).12 DISH is characterized primarily by ossification of the anterior spondylotic myelopathy
longitudinal ligament along the ventral aspect of the spinal column, with relative often demonstrate a
characteristic narrow
disk space and facet joint preservation. transverse (pancakelike)
band of cord enhancement
CERVICAL AND THORACIC SPONDYLOTIC MYELOPATHY. Cervical spondylotic at or slightly caudal to the
myelopathy deserves special mention, especially given its characteristic but focus of spinal stenosis.
underrecognized pattern of spinal cord enhancement after gadolinium
(FIGURE 10-5), which can be confused with inflammatory or neoplastic intrinsic
myelopathy. The spondylotic compressive findings are those that typically
narrow the spinal canal, any of which may be present: a developmentally narrow
canal (short pedicles), spondylolisthesis, disk herniations, osteophytes,
ossification of the posterior longitudinal ligament, and ligamentum flavum
redundancy/ossification. The cord may be compressed ventrally or dorsally, or
both (FIGURE 10-5). The nature of intramedullary signal abnormality, if present,
has pathologic correlation. T2 hyperintensity is often longitudinal, spindle-
shaped, and mildly expansile. This signal abnormality represents a range of
reversible (eg, edema) and irreversible (eg, demyelination, gliosis, cystic
necrosis) causes. When faint and indistinct, it more likely represents reversible
edema. When very intense and well defined, it is more likely caused by fixed
gliosis or cystic necrotic change. Similarly, intramedullary T1 hypointensity
correlates with irreversible necrosis and myelomalacia.12 Similar to a cord that
has been previously acutely traumatized, T2 hyperintensity may be present
cephalad to the cord compression in the posterior columns because of wallerian
degeneration or caudal to the compression in the lateral columns because of
corticospinal tract degeneration.
After gadolinium administration, T1-weighted images in cervical spondylotic
myelopathy often demonstrate a characteristic narrow transverse (pancakelike)
band of cord enhancement at or slightly caudal to the focus of spinal stenosis
(FIGURE 10-5).13,14 On axial images, the cross-sectional involvement of cord
enhancement is variable, but it is often peripheral and limited to the white
matter, either hemicord or bilateral. This enhancement, first reported in 2004,15
occurs within the region of abnormal cord T2 hyperintensity; the latter is much
greater in longitudinal extent. It often persists for a variable duration even after
decompressive surgery (FIGURE 10-5).14 Awareness of the enhancement pattern
is critical for expedient diagnosis, treatment, and avoidance of unnecessary
biopsy.14 Of note, even in cases demonstrating intramedullary enhancement, the
canal narrowing may not appear compressive in the recumbent neutral position.
Additional sagittal sequences in passive extension and flexion may reveal
compressive stenosis with extension and may more clearly show intrinsic cord T2
hyperintensity in flexion.16 Findings on diffusion tensor imaging, a sophisticated
MRI technique that is not yet routinely used clinically in most centers, may better
correlate with clinical severity than standard techniques.17
Compressive myelopathy also occurs in the thoracic spine but with less
frequency (FIGURE 10-5). A developmentally small spinal canal, degenerative
hypertrophy of facet joints, ligamentum flavum redundancy/ossification, and
large disk herniations can cause cord compression. Hypertrophy of facet joints
CONTINUUMJOURNAL.COM 239
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-6
Lumbar spinal stenosis. Multilevel multifactorial lumbar spinal stenosis (A through N, Q
through V, W through DD, three different patients) is common in patients who present with
neurogenic intermittent claudication. In the first patient (A through N), unenhanced CT (A
through D) demonstrates spinal stenosis, although MRI (E through N) displays the contributing
findings and degree of narrowing to better advantage. In this patient, multifactorial spinal
canal narrowing is mild at L2-L3 (B, H), moderate at L3-L4 (C, J), and advanced at L4-L5
(D through G, K through M). The stenosis has both ventral (A through F, K, white arrows) and
dorsal components (A, C through E, black arrows; J through K, blue arrows). Ventrally, disk
bulges contribute at L2-L3 through L4-L5, and at the latter, low-grade anterolisthesis also
contributes. At the advanced L4-L5 stenosis, the CSF is nearly completely effaced (D, K,
arrowheads) and the cauda equina focally enhances (G, M, white arrows). Because of the
high-grade stenosis, the cauda equina nerve roots are redundant/tortuous in the sagittal
plane (E, blue arrows) and abnormally ventrally located at several levels in the axial plane
(sedimentation sign; I at L3, N at L5, blue arrows); a normal comparison at these levels is
provided (O, P), demonstrating normally posteriorly dependently layering nerve roots. A
companion case of multilevel, multifactorial lumbar stenosis (Q through V) demonstrates
moderate spinal stenosis at L2-L3 and advanced stenosis at L3-L4 (Q, white arrows). At L2-L3,
L3, and L4-L5, the nerve roots are located more ventrally than normal (S, T, V, blue arrows,
respectively). At the high-grade L3-L4 stenosis (U), one cannot evaluate for the
sedimentation sign. A second companion case of multilevel, multifactorial lumbar spinal
stenosis (W through DD) also demonstrates cauda equina redundancy/tortuosity (W, blue
arrows) and cauda equina enhancement greatest at the highest degree of narrowing (CC, DD,
blue arrows). A developmentally narrow spinal canal contributes to the spinal stenosis.
Superimposed spondylotic changes result in spinal stenosis that is moderate at L2-L3 (Y, blue
arrow) and advanced at L3-L4 and L4 vertebral body levels (Z, AA, blue arrows, respectively).
A large disk extrusion posterior to the L4 vertebral body primarily contributes to the spinal
stenosis (W, AA through DD, white arrows); this peripherally enhances as can be expected
(refer to FIGURE 10-4). Neoplastic spinal stenosis (EE through II) can also occur, especially with
neoplastic involvement of the ventral epidural space (FF through II, white arrows), which in
this patient contributes to relatively advanced spinal canal narrowing (EE, blue arrow). On
axial images, the bilateral ventral epidural involvement with preservation of the midline septum
(draped curtain sign, GG through II, white arrows) suggests an indolent process such as
malignancy over a more rapidly aggressive process such as infection. In this patient, enhancing
tumor involves the basivertebral vein (FF, II, blue arrows) and paraspinal metastatic disease is
evident in the right retroperitoneal musculature (GG through II, black arrows).
240 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
can be especially subtle as the encroachment intrudes from the posterolateral KEY POINTS
aspects of the canal; thus, it is difficult to recognize in the sagittal plane due to
● Findings that suggest a
volume averaging. These stenoses tend to occur in the upper thoracic levels or the relatively high grade and
region of the lumbar cord and conus medullaris. symptomatic lumbar
stenosis include
LUMBAR SPINAL STENOSIS. Lumbar spinal stenosis is often a multifactorial and redundancy/tortuosity of
the cauda equina nerve
multilevel process (FIGURE 10-6). The compartments that may be involved
roots and the sedimentation
include the thecal sac, the lateral recesses of the traversing nerve rootlets within sign.
the spinal canal, and the neural foramina. Similar to cervical spondylotic
myelopathy, any or all of the following may be present: a developmentally ● If Hirayama disease is
narrow canal (short pedicles), spondylolisthesis, disk herniations, osteophytes, suspected clinically or
based on neutral position
epidural lipomatosis, and ligamentum flavum redundancy/ossification or facet MRI, flexion MRI should be
arthropathy. Synovial cysts associated with facet arthropathy are discussed performed as it can
separately above. Epidural lipomatosis can partially contribute to or primarily demonstrate findings to
result in spinal stenosis; the diagnostic clues are relatively diffuse increase in the better advantage and
increase diagnostic
amount of epidural fat and a lack of normal segmentation of the dorsal epidural confidence.
fat at the base of spinous processes. Lumbar spinal canal stenosis is often an
incidental asymptomatic finding; this is a specificity flaw of imaging.12 However,
especially when at least moderate in degree, multicompartmental, or multilevel,
lumbar spinal canal stenosis may impair the cauda equina nerve roots and result
in neurogenic intermittent claudication.
Findings that suggest a relatively high grade and symptomatic lumbar stenosis
include redundancy/tortuosity of the cauda equina nerve roots and the
sedimentation sign (FIGURE 10-6). In the supine patient with no lumbar stenosis,
cauda equina nerve roots layer dependently at the posterior aspect of the thecal
sac. In patients in whom the course of the nerve roots is altered by spinal stenosis,
the nerve roots fail to layer in such dependent fashion and are located ventrally in
the thecal sac (the sedimentation sign).18 Although large studies have not been
performed, a 2019 meta-analysis of available literature suggests high sensitivity,
specificity, and clinical diagnostic performance for this sign.19 An additional
associated finding that can cause confusion, analogous to cervical spondylotic
myelopathy, is focal enhancement of the cauda equina nerve roots centered at
the level of spinal canal stenosis (FIGURE 10-6). A shortcoming of standard
imaging is the sensitivity flaw of trying to detect spinal stenosis in the relaxed
supine patient. Imaging in an axial load-bearing position can accentuate or even
reveal stenosis compared to supine examinations. Such imaging can be
performed in the upright position, for example, with cone-beam CT
myelography (FIGURE 10-7) or select MRI scanners (eg, 0.6T open upright
systems), neither of which are in widespread use.
HIRAYAMA DISEASE. The purported pathophysiology of Hirayama disease
(also known as monomelic amyotrophy) (FIGURE 10-7) is a short dura mater
(relative to vertebral column length) that moves anteriorly during neck
flexion and results in compression of the posterior aspect of the spinal cord.
If Hirayama disease is suspected clinically or based on neutral position
MRI, flexion MRI should be performed as it can demonstrate findings to better
advantage and increase diagnostic confidence.20,21 MRI may demonstrate
loss of normal cervical lordosis in the neutral position, a finding that is not
diagnostically specific. Asymmetric cord atrophy or flattening of the lower
cervical/upper thoracic cord may also be present, often greatest at C6,22 with
CONTINUUMJOURNAL.COM 241
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-7
Dynamic lumbar and cervical spinal stenosis. Dynamic lumbar spinal stenosis (A through F) is
not optimally imaged in routine supine MRI or CT/CT myelography. In this patient, such
standard recumbent imaging demonstrates, at most, moderate spinal stenosis at L4-L5
(A, B, white arrows, MRI; C, D, CT myelography). A small right synovial cyst (B) contributes to
the spinal canal narrowing. When the patient is imaged in the standing position of axial
loading using cone-beam CT myelography, the degree of stenosis changes to advanced (E, F,
white arrows) and the cauda equina becomes redundant/tortuous (F, blue arrow). Hirayama
disease (G through K; L, M; N through R, three different patients) is a dynamic flexion
myelopathy. On neutral images, loss of normal cervical lordosis (G) and loss of attachment of
the dura to the lamina can be present; the latter best seen on axial images (H through I, white
arrows). This loss of dural attachment on axial images may become more prominent in flexion
(J, white arrow), and the dorsal epidural space can be seen to expand, especially on sagittal
images in flexion (K, R) compared to neutral positioning (G, white arrow). This results in
dynamic spinal canal narrowing and mass effect on the cord. In the first companion case
(Patient 2) (L, M), the dorsal epidural space becomes prominent in flexion (L, white arrow;
neutral not shown) and accompanying bilateral myelomalacia of the cord is seen (M, white
arrows). A second companion case (Patient 3) (N through R) again demonstrates loss of
cervical lordosis (N, O) and loss of dural attachment to the lamina axially (P, white arrow).
Postcontrast and in flexion, compared to images in neutral positioning (N through P), the
dorsal epidural space significantly enlarges, acts with mass effect on the spinal cord, and
enhances robustly (Q, R, white arrows).
242 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
or without focal myelomalacia-type T2 hyperintensity. When present, the KEY POINTS
short-segment abnormal T2 hyperintensity in the focally atrophied cord primarily
● For enhancing
involves the bilateral anterior or anterior and lateral horns of the gray matter (the intradural-extramedullary
owl-eyes or snake-eyes sign, discussed further in the later section on spinal cord masses, the two most
infarcts).23 The posterior dura can be seen to be anteriorly displaced (loss of likely possibilities are
attachment to the adjacent lamina), a finding that can be present on neutral meningiomas and nerve
root sheath tumors
imaging24 but for which flexion images increase confidence. This finding is
(schwannomas and
associated with engorgement of the dorsal epidural venous plexus, which acts as neurofibromas).
an epidural mass, can cause cord flattening, and typically robustly enhances.21,24
● Characteristic, although
not entirely specific,
OTHER EXTRADURAL CAUSES OF MYELOPATHY. The diagnoses discussed above are imaging findings suggestive
not all of the extradural causes of myelopathy or cauda equina impairment. of spinal meningioma
include dural tail(s) of
Primary malignant and benign osseous lesions may grow into the spinal canal but
contrast enhancement and
are beyond the scope of this discussion. Metastatic disease and multiple myeloma, avid and homogeneous
plasmacytoma, and lymphoma are commonly encountered and usually arise from enhancement of the lesion,
the osseous components of the spine, including the vertebral body and posterior which may be relatively T2
elements. Metastatic disease can also affect the epidural or, very rarely, subdural hypointense because of
cellularity or calcification.
compartments; the former is commonly because of extension from adjacent
osseous disease (FIGURE 10-6). The rule for such malignant causes of cord and
cauda equina compression is gadolinium enhancement of the soft tissue lesions.
When in the ventral epidural space, a relatively slow-growing malignancy may
demonstrate the suggestive but not specific draped curtain sign, caused by
preservation of the midline central septum (anterior meningovertebral ligament)
(FIGURE 10-6). This sign may also be observed in indolent infectious processes
such as tuberculosis,25 whereas more rapidly aggressive epidural disease processes,
such as epidural infection (phlegmon, abscess) or hematoma, may lack this sign
because of violation of the midline ligament.26 Uncommonly encountered
extradural disease processes include conditions such as extramedullary
hematopoiesis, Erdheim-Chester disease, idiopathic hypertrophic
pachymeningitis, and calcifying pseudoneoplasm of the neuraxis (FIGURE 10-3).
Intradural-Extramedullary Compartment
A multitude of disease processes can occur in the intradural-extramedullary
compartment of the spinal canal.
INTRADURAL-EXTRAMEDULLARY NEOPLASMS. Lesions occurring in the intradural-
extramedullary compartment can be diagnosed by their widening of the
subarachnoid space ipsilaterally and, when large enough, compression/
displacement of the spinal cord and effacement of the subarachnoid space
contralaterally (FIGURE 10-8). Fortunately, such intradural-extramedullary lesions
are most commonly benign. For enhancing intradural-extramedullary masses, the
two most likely possibilities are meningiomas and nerve root sheath tumors
(schwannomas and neurofibromas).27 Distinguishing between these entities can
be challenging, but certain clues can suggest the correct diagnosis. As for virtually
any enhancing lesion in the spine, metastatic disease is in the differential diagnosis.
MENINGIOMAS. Spinal meningiomas are most common in the thoracic spine and
most often lateral to the cord.27 Characteristic, although not entirely specific,
CONTINUUMJOURNAL.COM 243
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-8
Intradural-extramedullary disease. Meningiomas (A through F) may be relatively T2
hypointense (B, E) because of their high cellularity or calcification. They tend to enhance
avidly postcontrast (C, F) and may have adjacent enhancing dural tails (C, white arrows). Axial
images demonstrate the characteristic features of intradural-extramedullary masses; the
ipsilateral subarachnoid space is expanded immediately above and below the lesion (D, F,
white arrows, respectively), with displacement of the spinal cord contralaterally (D through
F, blue arrows). At the level of the lesion, the spinal cord is significantly compressed (E, blue
arrow), whereas the T2-hypointense lesion fills the adjacent subarachnoid space. Benign
nerve sheath tumors (schwannomas [G through I] and neurofibromas [J through M]) can be
difficult to differentiate. This cervical schwannoma enhances avidly (G, H), extends through
and expands the neural foramen, fills the subarachnoid space, and displaces the spinal cord
contralaterally (I). Neurofibromas may similarly extend through and expand neural foramina,
as is true for many lesions in this patient with neurofibromatosis type 1 (eg, J, white arrow).
These tumors may characteristically be centrally relatively T2 hypointense and peripherally
relatively T2 hyperintense (target sign; L, white arrow). Myxopapillary ependymomas (N, O)
classically present as well-defined, avidly enhancing oval masses of the tip of the conus,
proximal cauda equina, or filum terminale. Although focal intradural-extramedullary lesions
are typically benign, low grade, or slow growing (such as meningiomas, nerve sheath tumors,
and myxopapillary ependymomas), intradural-extramedullary metastases (P through R) can
occur in this compartment. The metastasis in this patient causes extensive T2 hyperintensity
in the spinal cord (P, Q; Q, blue arrow), with associated focal cord enhancement (R, blue arrow).
The lesion is heterogeneously signaling and enhancing and occupies the subarachnoid space
and neural foramen (Q, R, white arrows). Multifocal leptomeningeal disease (S through U)
presenting as multifocal smooth or nodular enhancement is not diagnostically specific and
can be benign or malignant. Among benign causes, neurosarcoidosis is in the differential
diagnosis. This patient with neurosarcoidosis has both smooth pial enhancement along the
conus and multifocal nodular enhancement along the cauda equina (S through U, white arrows).
244 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
imaging findings suggestive of spinal meningioma include dural tail(s) of KEY POINTS
contrast enhancement and avid and homogeneous enhancement of the lesion,
● When an isolated,
which may be relatively T2 hypointense because of cellularity or calcification incidental, small enhancing
(FIGURE 10-8). In the authors’ clinical experience, spinal meningiomas have a nodule of the cauda equina
propensity to calcify, although the literature suggests this is uncommon. nerve roots is encountered,
Multiple lesions are less common than solitary lesions and usually suggest the most likely
consideration is a nerve
neurofibromatosis type 2 or, much less commonly, meningiomatosis. sheath tumor.
NERVE SHEATH TUMORS. Benign nerve sheath tumors (schwannomas and ● Myxopapillary
ependymomas are usually
neurofibromas) are well-circumscribed neoplasms that can be difficult to relatively large, oval or
differentiate by imaging. Schwannomas are more prevalent than neurofibromas. sausage shaped, well
When located at least partially in the neural foramen, dumbbell morphology is a circumscribed, T2
characteristic feature (FIGURE 10-8). Schwannomas have a higher propensity to hyperintense, and avidly
enhancing.
demonstrate cystic change or intratumoral hemorrhage than either
neurofibromas or meningiomas. A classic appearance of a neurofibroma is a
peripherally T2-hyperintense lesion that is relatively T2 hypointense centrally,
the so-called target sign (FIGURE 10-8). Multiple schwannomas can be seen in
neurofibromatosis type 2 or, less commonly, schwannomatosis, whereas
multiple neurofibromas can occur in neurofibromatosis type 1. When an
isolated, incidental, small enhancing nodule of the cauda equina nerve roots is
encountered, the most likely consideration is a nerve sheath tumor. Malignant
peripheral nerve sheath tumors are rare. Although these tumors often have a
heterogeneous appearance, they may mimic the appearance of their benign
counterparts, particularly since they too are usually well-circumscribed.27
MYXOPAPILLARY EPENDYMOMAS. The most common neoplasm of the region of
the tip of the conus, proximal cauda equina, and filum terminale is the
myxopapillary ependymoma, a slow-growing variant of ependymoma.27 This
usually intradural-extramedullary neoplasm typically occurs along the filum
terminale, can be solitary or multiple, and usually has a characteristic appearance.
Myxopapillary ependymomas are usually relatively large, oval or sausage shaped,
well circumscribed, T2 hyperintense, and avidly enhancing (FIGURE 10-8). The
tumors may contain blood products, causing heterogeneous signal characteristics.
Owing to the neoplasm’s vascular nature, subarachnoid hemorrhage may be
present as a fluid-debris level in the cul-de-sac or superficial siderosis. The less
common paraganglioma can mimic the appearance of ependymoma.
MENINGEAL METASTATIC AND INFECTIOUS/INFLAMMATORY DISEASE. The presence
of one or more enhancing nodules along the surface of the cord/conus, cauda
equina nerve roots, or dura may reflect a metastatic or infectious/inflammatory/
toxic process (FIGURE 10-8). Enhancement is the rule for metastatic disease,
which is more commonly because of hematogenous dissemination than from
drop metastases from a more cephalad, usually intracranial, central nervous
system (CNS) primary malignancy. Extensive nodular coating of the pial surface
of the cord can occur, the so-called Zuckerguss appearance (German for
sugarcoating). Enhancing metastatic lesions in other anatomic locations on the
MRI and identification of the primary malignancy itself can help make the
diagnosis of metastatic disease. Although nodular or nonuniform thickening is
typical, diffuse smooth enhancement of the cord surface, cauda equina, or dura
CONTINUUMJOURNAL.COM 245
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-9
Arachnoiditis and inflammatory demyelinating polyneuropathies. Arachnoiditis (A through P,
three different patients) can have varying imaging findings and causes. It is often idiopathic
(A through D) or can result from specific irritants within the thecal sac, such as stem cells
(E through J) or infections (K through P). Thickening or nodularity of cauda equina nerve roots
may be evident, best seen on T2-weighted images (A, B, E, H, white arrows). The nerve roots
are commonly nonanatomically distributed (B through D, H) and may be centrally clumped
(C, H) or dispersed peripherally (empty thecal sac sign, D, white arrows). Abnormal
enhancement is often only mild if present (F, J, white arrows). Adhesive arachnoiditis
(K through P) such as that caused by infections (including tuberculosis) may cause bizarre
appearances related to adhesions and loculations in the thecal sac, altered CSF dynamics,
and effects on the spinal cord. The spinal cord may be displaced (M, N, blue arrows) and may
contain T2 hyperintensity or a syrinx (K, O, white arrows). Thickening and enhancement of the
meninges, including the dura, may be observed (L, P, white arrows). Acute inflammatory
demyelinating polyradiculoneuropathy (AIDP) (Q through S) and chronic inflammatory
demyelinating polyradiculoneuropathy (CIDP) (T through V) are considerations when
thickened (Q, U, white arrows) or enhancing (R through T, V, white arrows) nerve roots are
encountered but the distribution is anatomic. AIDP has a predilection to involve the ventral
nerve roots (Q through S, white arrows).
246 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
can also occur. The latter smooth appearance is not as strongly suggestive for KEY POINTS
metastatic disease, since infectious/inflammatory/toxic causes are generally
● Varied appearances of
more likely to cause such a uniform abnormality than to be nodular.27 For this arachnoiditis include nerve
diverse group of non-neoplastic disorders, unless ancillary imaging findings roots that are irregularly
such as those discussed in the intramedullary sections below are present, a clumped, clumped into a
specific diagnosis often requires alternative tests, particularly CSF analysis. mass of neural tissue
centrally, or dispersed to
the margins of the dura (the
NON-NEOPLASTIC INTRADURAL-EXTRAMEDULLARY DISEASES OF THE ARACHNOID AND empty thecal sac sign).
DURA. Among intradural-extramedullary disease processes, several non-neoplastic
● The most common
diseases that can affect the arachnoid and dura are important to recognize. location for an arachnoid
cyst is dorsal to the thoracic
ARACHNOIDITIS. Irritation of the arachnoid resulting in postinflammatory cord; although these
lesions tend to be well
adhesions can be idiopathic or occur for variety of known reasons, including most circumscribed, their wall is
commonly as an iatrogenic complication or because of trauma/subarachnoid often imperceptible,
hemorrhage or inflammation/infection, such as intrathecal stem cell therapy especially on MRI.
(FIGURE 10-9).28 Arachnoiditis can have varying imaging presentations and most
commonly involves the cauda equina nerve roots. The affected nerve roots may
lack the normal anatomic distribution (ie, they do not layer dependently in the
supine patient and lack their normal organization). Varied appearances of
arachnoiditis include nerve roots that are irregularly clumped, clumped into a mass
of neural tissue centrally, or dispersed to the margins of the dura (the empty thecal
sac sign) (FIGURE 10-9). The nerve roots may or may not be abnormally thickened
or enhancing. If diffusely thickened, particularly if the thickening is marked and
symmetric but the distribution is anatomic, chronic inflammatory demyelinating
polyradiculoneuropathy (CIDP) is a differential consideration (FIGURE 10-9).
Acute inflammatory demyelinating polyradiculoneuropathy (AIDP, Guillain-Barré
syndrome) can also present with thickened nerve roots; the ventral cauda equina
nerve roots are typically asymmetrically affected and often enhance, and the pial
surface of the conus may also enhance (FIGURE 10-9).29 Adhesive arachnoiditis is a
severe end-stage manifestation of inflammatory processes such as infections,
leading to adhesions and loculations in the thecal sac (FIGURE 10-9). When
involving the cervicothoracic spine, the spinal cord can be affected by
displacement, myelomalacia, T2 hyperintensity, or syrinx. Arachnoiditis ossificans
is a rare, chronic, and severe manifestation of arachnoiditis; the intradural
calcifications are often best appreciated on CT.30
ARACHNOID/DURAL LESIONS CAUSING EXPANSION OF THE DORSAL ASPECT OF THE
THECAL SAC, DORSAL CORD FLATTENING, OR VENTRAL CORD DISPLACEMENT.
Abnormalities of arachnoid and dura can result in abrupt distortions of the cord that
are difficult to resolve on MRI. The CSF space is typically widened, and the cord
displaced without evident mass lesion. Myelography can be useful in more precisely
depicting the fine detail and flow dynamics of the extramedullary abnormality.
Arachnoid cysts. Arachnoid cysts can occur in other compartments of the spinal
canal but are usually intradural-extramedullary. The most common location for
an arachnoid cyst is dorsal to the thoracic cord; although these lesions tend to be
well circumscribed, their wall is often imperceptible, especially on MRI
(FIGURE 10-10). As a result, and since their signal characteristics are generally
isointense to CSF (fluid-type high T2 signal, low T1 signal), they may be difficult
CONTINUUMJOURNAL.COM 247
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-10
Dorsal cord flattening: spectrum of disease. Arachnoid cysts (A through H), arachnoid webs
(I through N), and idiopathic spinal cord herniation (O through Q, R through W, two different
patients) can all cause flattening of the dorsal aspect of the spinal cord and apparent
expansion of the dorsal subarachnoid space. Spinal cord T2 hyperintensity or syrinx
formation can be present with any of these entities, such as the syrinx seen in the case of
arachnoid cyst (A, B, blue arrows). On MRI, expansion of the dorsal subarachnoid space
(A through C, white arrows) is associated with ventral displacement and dorsal flattening of
the cord, well seen axially (C). On fluoroscopic myelographic visualization before CT
myelography, a filling defect is observed (D, white arrows) consistent with an arachnoid cyst;
by the time the patient has been transferred to CT, the arachnoid cyst has filled with contrast
(E through G, white arrows). The walls of the cyst are not visualized on either MRI or CT
myelography. Spinal cord compression can be observed, just as on MRI (G, blue arrow).
Above this level of maximal mass effect, the spinal cord is ventrally displaced and atrophic
(F, blue arrow), whereas below it the caliber is normal (H). Arachnoid webs classically present
with a sharply marginated dorsal cord contour irregularity; this is sometimes better seen on CT
myelography than MRI (scalpel sign; M, N, compared to J, white arrows). As with other causes
of myelopathic signal abnormality, spinal cord T2 hyperintensity (J through L, blue arrows) is
seen to slightly better advantage on short tau inversion recovery (STIR) than conventional
T2-weighted images (K compared to J, blue arrows). The arachnoid web itself is not visualized.
Idiopathic spinal cord herniation has similar imaging findings to arachnoid cysts and webs,
including dorsal cord contour irregularity and expansion of the dorsal subarachnoid space
(O through Q, R through W, white arrows, two different patients) as well as spinal cord T2
hyperintensity (O, blue arrow). Extreme ventral cord positioning on sagittal images with loss of
subarachnoid space between the cord and posterior aspect of the vertebral bodies/disk can
be a clue (O, R) and is best evaluated on axial images, which can better show the herniation of
the spinal cord through the dura (P through Q; S). Prominent ventral extradural fluid is an
additional clue (P, blue arrows; Q, black arrow; S, U, W, blue arrows). Thin-section heavily
T2-weighted three-dimensional steady state sequences can be useful to depict the focal
ventral transdural cord herniation in high resolution (S).
248 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
to visualize on MRI. Indeed, in some cases, the mass effect that they may cause KEY POINTS
on the spinal cord may be the primary clue to their presence. Because of their
● Typically, arachnoid webs
chronic nature, arachnoid cysts may remodel or expand the spinal canal in cause mass effect on and
benign fashion. Because they also can be dynamic lesions that may fill rapidly or flattening of the dorsal cord,
slowly, sophisticated imaging techniques may be required to diagnose arachnoid with a characteristic but not
cysts confidently, including conventional myelography under fluoroscopy with pathognomonic morphology
termed the scalpel sign that
real-time visualization in the early phase of opacification of the spinal canal with
is best seen sagittally on
contrast (FIGURE 10-10), multipositional CT myelography, and delayed images either T2-weighted images
on either modality. On MRI, thin-section heavily T2-weighted images can also be or CT myelography.
helpful (TABLE 10-2).
● On MRI or CT
myelography, the
Arachnoid webs. Arachnoid webs are lesions of unknown etiology that may be characteristic findings of
closely related to arachnoid cysts. Some postulate that these may represent the idiopathic spinal cord
incomplete/disrupted formation of an arachnoid cyst.31 Such webs are bands of herniation include ventral
arachnoid tissue along the dorsal aspect of the spinal cord, most commonly displacement of a short
segment of cord that is
occurring in the upper to midthoracic spine. The band itself is only rarely focally distorted/kinked,
demonstrated on imaging. Typically, arachnoid webs cause mass effect on and with the subarachnoid space
flattening of the dorsal cord, with a characteristic but not pathognomonic being lost ventrally and
morphology termed the scalpel sign that is best seen sagittally on either T2-weighted expanded dorsally.
images or CT myelography (FIGURE 10-10). The initial and largest series to date
describing this sign included 14 patients, but nine were not surgically proven.31
Indeed, it can be difficult or, in some cases, impossible to confidently differentiate
arachnoid cysts and webs, despite high-resolution MRI and CT myelography.
Idiopathic spinal cord herniation. The spinal cord may herniate through a defect in
the dura into the extradural compartment (FIGURE 10-10).32 Such herniation
typically occurs ventrally in the thoracic spine (usually T4 through T7) and in
many, but not all, cases at a disk space level.33 In some cases, diskal calcification
or osteophytes at the disk space level probably erode the dura and result in the
cord herniation. Making the diagnosis is important because surgical treatment
may allow reversal or at least stabilization of neurologic deficits. On MRI or CT
myelography, the characteristic findings of idiopathic spinal cord herniation
include ventral displacement of a short segment of cord that is focally
distorted/kinked, with the subarachnoid space being lost ventrally and expanded
dorsally (FIGURE 10-10). A ventral extradural CSF collection (leak) may be
present. An arachnoid cyst may also be coexistent. Differentiating between a
dorsal arachnoid cyst that displaces the cord ventrally and ventral cord
herniation with or without an arachnoid cyst can be challenging. Just as is the
case for diagnosis of arachnoid cysts and webs, thin-section heavily T2-weighted
images on MRI can be helpful (FIGURE 10-10). CT myelography is often
required, but in subtle/challenging cases, especially when an arachnoid cyst is
coexistent, confident and correct diagnosis may be elusive until surgery.
Intramedullary (Intrinsic) Compartment
When spinal cord signal abnormality is intrinsic in nature without a causative
lesion external to the spinal cord, arriving at the correct diagnosis is often more
challenging. Such disease processes can be broadly divided into neoplastic and
non-neoplastic categories. For these diseases, a detailed analysis of the imaging
features of the spinal cord lesion itself as well as the noncord structures may help
in arriving at the correct diagnosis or limiting the list of differential conditions.
CONTINUUMJOURNAL.COM 249
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-11
Intramedullary neoplastic myelopathy. Ependymomas (A through I) are expansile neoplasms
that may demonstrate blood products, including as T1- and T2-hypointense regions at the
margin of the tumor (cap sign; A, C, F, white arrows); this is related to hemosiderin content,
which blooms or becomes more pronounced on gradient recalled echo (GRE) images
(B, white arrow). Blood products may also layer dependently as blood-fluid levels (A, E, blue
arrows). One clue for ependymoma over astrocytoma is the centrally located nature of the
tumor (D). Ependymomas tend to enhance (H, I, white arrows). Astrocytomas (J through P)
tend to be eccentrically located, which may be most evident at the margins of the expansile
neoplasm (L, N, white arrows, at slices along the superior and inferior aspects of the
tumor, compared to M at a slice in the midportion). Enhancement may be absent or minimal
(O, P). Hemangioblastomas (Q through T, U and V, two different patients) typically have a
markedly different appearance compared to ependymomas and astrocytomas. The lesions
are often located on the dorsal cord surface, avidly enhancing, and small (R through T, white
arrows), especially with regard to the extensive spinal cord T2 hyperintensity, syrinx, or cysts
they produce (Q, R). Lesions can be multiple (V, white arrows) and may have significant
associated vascularity, well seen as hypointense flow voids in the CSF on T2-weighted
images (U, white arrows). Like hemangioblastomas, intramedullary spinal cord metastases
(W through BB) can produce significant cord T2 hyperintensity for neoplasm size
(W compared to Y). The lesions may demonstrate one or more of three characteristic
enhancement features: a rim of more intense enhancement around the enhancing mass (rim
sign; Y, BB, blue arrows); ill-defined flame-shaped enhancement at the superior or inferior, or
both, margins of the lesion (flame sign; Y, white arrows); and a punctate focus of
enhancement in/near the center of the lesion (central dot sign; BB, arrowhead). On
fludeoxyglucose positron emission tomography (FDG-PET), spinal cord metastases are
typically FDG avid (Z, AA); just as on MRI, other evidence for metastatic disease may be
present (Z, white arrow, a metastatic paratracheal lymph node from a lung carcinoma).
250 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Relevant features include the cross-sectional pattern of involvement (white matter KEY POINTS
versus gray matter versus both), the longitudinal extent of the lesion (short versus
● Neoplasms tend to
long), expansion (presence or absence), associated findings in the spinal cord (such expand the spinal cord, to
as hemorrhage, cysts, and other lesions), enhancement (presence and pattern, if have a mass or masslike
present), and findings outside the spinal canal (such as in the osseous vertebral appearance, and to
column, paraspinal regions, and extraspinal regions). enhance. The presence of
associated adjacent cord
Broadly speaking, differentiating neoplastic from non-neoplastic intrinsic
cysts or hemorrhage
cord lesions may not always be possible, but several features can be helpful. typically suggests a
Neoplasms tend to expand the spinal cord, to have a mass or masslike neoplastic process.
appearance, and to enhance.34 The presence of associated adjacent cord cysts or
hemorrhage typically suggests a neoplastic process. Such features are not perfect, ● Internal or adjacent
heterogeneity, including
however. For example, occasionally neoplasms are ill-defined/infiltrative related to the presence
appearing, and occasionally non-neoplastic diseases are tumorlike. Similarly, a of cystic change (polar
long-segment abnormality with patchy enhancement favors a non-neoplastic cyst) or hemorrhage
process, but neoplasms can also be quite extensive with patchy/ill-defined (T2-hypointense
hemosiderin cap sign) at the
enhancement, especially astrocytomas. margins of the lesion, is
more commonly
INTRAMEDULLARY NEOPLASMS. Primary cord neoplasms are more common than encountered with
metastases. The three most common primary cord neoplasms are ependymoma, ependymoma than with
astrocytoma.
astrocytoma, and hemangioblastoma. Ependymoma is the most common
primary cord neoplasm in adults, whereas astrocytoma predominates in children. ● Although astrocytomas
Other primary tumors, such as gangliogliomas and spinal cord lymphomas, are usually enhance, they may
not discussed here. not; when they do enhance,
it may be fairly mild in
amount/intensity or
EPENDYMOMAS. Ependymomas arise from the ependymal lining of the central ill-defined.
canal of the spinal cord. Thus, these neoplasms typically have a central location
within the spinal cord. They tend to be well-circumscribed expansile lesions
(FIGURE 10-11). Enhancement is typically present and often well defined.
Internal or adjacent heterogeneity, including related to the presence of cystic
change (polar cyst) or hemorrhage (T2-hypointense hemosiderin cap sign) at
the margins of the lesion, is more commonly encountered with ependymoma
than with astrocytoma (FIGURE 10-11). Spinal cord ependymomas can be seen in
patients with neurofibromatosis type 2.
ASTROCYTOMAS. Astrocytomas are the second most common primary cord
neoplasm in adults. In contrast to ependymomas, these expansile tumors tend to
be eccentrically rather than centrally located (FIGURE 10-11) and are more likely
to be poorly defined. If a tumor is holocord, it is more likely to be an astrocytoma
than an ependymoma. Although astrocytomas usually enhance, they may not;
when they do enhance, it may be fairly mild in amount/intensity or ill-defined
(FIGURE 10-11). Hemorrhage is not a common feature. Spinal cord astrocytomas
can be seen in patients with neurofibromatosis type 1.
HEMANGIOBLASTOMAS. The third most common primary spinal cord tumor in
adults is the hemangioblastoma. These neoplasms are highly vascular and can
occur sporadically or in the setting of von Hippel-Lindau disease. They can
be solitary or multiple (FIGURE 10-11) and intramedullary or intradural-
extramedullary. Because of their vascular nature, avid enhancement is the rule,
and prominent vascularity may be evident as flow voids, especially on
T2-weighted images within or adjacent to the lesion (FIGURE 10-11).
CONTINUUMJOURNAL.COM 251
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-12
Longitudinally extensive intramedullary inflammatory/demyelinating myelitis. Long-segment
multiple sclerosis is not common, but confluent multiple sclerosis may result from
innumerable adjacent T2-hyperintense lesions (A, B, D through G), best seen sagittally on
short tau inversion recovery (STIR) (B) and axially on gradient recalled echo images (GRE) (F)
compared to traditional T2-weighted images (A, E). In the chronic phase, the lesions do not
enhance (C) and atrophy may be evident (A, G, white arrows). Aquaporin-4-IgG neuromyelitis
optica spectrum disorder (NMOSD) (H through M; N through R; S and T, three different
patients) characteristically presents as a longitudinally extensive myelitis (H, N, S). Imaging
features with relative specificity include small foci on axial images that are at least as T2
hyperintense as CSF (bright spotty lesions; J through M, white arrows) and ring/partial ring
enhancement on sagittal or axial images (I, Q, R, white arrows). Any myelopathy can cause
atrophy in the chronic phase, which can be short or long segment (S, T). Neurosarcoidosis
(U through AA, BB through EE, two different patients) is also usually long segment (U, BB). A
characteristic enhancement pattern is broad-based involvement of the dorsal subpial/pial
aspect of the cord (W, X, Z, AA, CC through EE, white arrows), which may also involve the
central canal of the cord (DD, EE, blue arrows) as best seen on axial images; this concomitant
dorsal subpial/pial and central canal enhancement of the cord on axial images is termed the
trident sign. When the thoracic spine is imaged, cord T2 hyperintensity/enhancement (V,
white arrow) may not be the only critical observation; mediastinal/hilar adenopathy can be
a clue to the diagnosis (V, blue arrow). The spinal cord findings typically are responsive to
steroids, but even when improving they can persist for months after treatment has been
initiated (Z, AA compared to W, X, white arrows). Myelin oligodendrocyte glycoprotein
(MOG)-IgG myelitis (FF through KK) similarly tends to be long segment and commonly involves
the thoracolumbar region (FF), often with central/gray matter selective involvement (HH, II,
white arrows). Enhancement may be absent (JJ) or minimal (KK, white arrow), a clue to the
diagnosis.
Hemangioblastomas have a propensity to be eccentrically located and abut the
surface of the spinal cord, with an enhancing pial/subpial nodule especially
dorsally. The neoplasms may present as cystic or partially cystic lesions with
nodular enhancement (FIGURE 10-11). Even when small, the lesions can produce
a significant amount of abnormal intramedullary T2 hyperintensity, indicating
edema, syringohydromyelia, or cyst formation (FIGURE 10-11). Evidence of
prior hemorrhage in or along the spinal cord may be present.
252 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
METASTASIS. Intramedullary spinal cord metastases are most commonly singular KEY POINTS
(FIGURE 10-11), with multiple lesions occurring in 20% of patients on initial
● Hemangioblastomas have
(index) scans at clinical presentation. Several recently described features of a propensity to be
intramedullary spinal cord metastases can help make a specific diagnosis. Two eccentrically located and
highly specific enhancement characteristics of intramedullary spinal cord abut the surface of the
metastases are reasonably prevalent in these lesions and not commonly seen in spinal cord, with an
enhancing pial/subpial
primary cord tumors: the rim and flame signs (FIGURE 10-11).35 The rim sign
nodule especially dorsally.
refers to a more intense partial or complete rim of enhancement surrounding a The neoplasms may present
less intensely enhancing noncystic/necrotic lesion. The flame sign refers to an as cystic or partially cystic
ill-defined flame-shaped region of enhancement in the spinal cord along the lesions with nodular
enhancement.
superior or inferior, or both, aspects of the lesion. A third less prevalent sign is
the central dot sign, a punctate focus of intense enhancement at/near the center ● Two highly specific
of an enhancing lesion, seen in a small minority of intramedullary spinal cord enhancement
metastases but not in primary cord tumors, based on a 2020 study (FIGURE 10-11).36 characteristics of
The presence of extensive spinal cord T2 hyperintensity with respect to a intramedullary spinal cord
metastases are reasonably
relatively small lesion size can also be a clue to the diagnosis (FIGURE 10-11) and prevalent in these lesions
is a poor prognostic factor,37 although the aforementioned hemangioblastoma and not commonly seen in
may similarly cause this finding. Hemorrhage and cystic change/necrosis are primary cord tumors: the rim
uncommon in intramedullary spinal cord metastases.38 Evidence of other and flame signs.
metastatic disease (eg, in the bones of the spine or paraspinal regions) or of the
● Characteristically,
primary malignancy (eg, a lung carcinoma) is often present on the index MRI.38 multiple sclerosis lesions
Intramedullary spinal cord metastases are typically avid on fludeoxyglucose are short segment (fewer
positron emission tomography (FDG-PET) examinations (FIGURE 10-11) but than two segments
craniocaudally),
may be underreported on this modality.39
asymmetrically and
eccentrically located (not
NON-NEOPLASTIC INTRAMEDULLARY DISEASES. A plethora of non-neoplastic involving the entire
intramedullary diseases can cause myelopathy. Selected causes that are commonly cross-sectional area), and
encountered in clinical practice are discussed first below. affect white or white plus
gray matter. Common
cross-sectional locations
MULTIPLE SCLEROSIS. MS is the prototypical CNS demyelinating disease. MRI of include the lateral and
the brain and spinal cord are the paraclinical tests of highest utility for the dorsal aspects of the cord.
diagnosis of MS, and they can substitute for clinical data in the determination of
dissemination in space or dissemination in time in the setting of a typical
clinically isolated syndrome.40 The 2017 revised McDonald diagnostic criteria
for MS allow for both symptomatic and asymptomatic MRI cord lesions to be
used for determining dissemination in space or dissemination in time. When MS
affects the spinal cord, the lesions tend to be small and multiple (FIGURE 10-12).
The cervical cord is more commonly involved than the thoracic cord, and silent
MS lesions frequently occur.41 Characteristically, MS lesions are short segment
(less than two segments craniocaudally), asymmetrically and eccentrically
located (not involving the entire cross-sectional area), and affect white or white
plus gray matter. Common cross-sectional locations include the lateral and
dorsal aspects of the cord. Although not pathognomonic, these morphologic and
locational features can strongly suggest the diagnosis. As is true for lesions in the
brain, enhancement is compatible with active demyelination and can be seen in
the acute to subacute phases. This can be of varying morphologies, including
ill-defined, solid/nodular, ring, or partial ring. Acute lesions can be expansile but
usually not markedly so given their often-small size. Long-segment involvement
of the cord is not common in adult patients and is sometimes the result of the
confluence of multiple small lesions (FIGURE 10-12).42
CONTINUUMJOURNAL.COM 253
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-13
Intramedullary nontumoral inflammatory myelopathies. Viral myelitis (A through G) may
result in long-segment T2 hyperintensity of the central gray matter (A through E), which can
enhance in the acute phase (G, H, arrows). Paraneoplastic myelopathy (I through N) may
cause long-segment T2 hyperintensity (I, J) and enhancement (L through N, arrows). A clue
can be the tract-specific nature of the signal abnormality or of the enhancement, as is
evident in this case of lateral column enhancement bilaterally (L, M, arrows). Subacute
combined degeneration (O through T) characteristically causes T2 hyperintensity of the
dorsal columns (O through Q, arrows). The morphology on axial images may be that of an
inverted V or inverted rabbit ears (P, arrows). If acute-subacute, the process may be mildly
expansile (O), and enhancement can occur (S, T, arrows). Radiation-induced myelopathy
(U through X) can present with nonspecific spinal cord T2 hyperintensity (U, V), which can be
confluent or patchy (U), may involve the central cord (V), and may enhance (X, Y, arrows).
A key clue is the radiation-induced inherent (precontrast) marrow T1 hyperintensity of the
regional spinal column (eg, W, arrow). This manifests as very hypointense signal on
fat-suppressed T2-weighted (U) or T1-weighted postcontrast (X) images. The patient shown
also has multifocal T1-hypointense enhancing osseous metastases.
LONGITUDINALLY EXTENSIVE MYELITIS (MOST COMMONLY AQP4-IgG–SEROPOSITIVE
NMOSD, NEUROSARCOIDOSIS, AND MOG-IgG–ASSOCIATED DISORDER). A commonly
encountered scenario is a long-segment myelopathy (three or more segments
craniocaudally), with variably expansile T2 hyperintensity and a relative lack of
a neoplasmlike appearance. The three primary neuroimaging considerations
based on prevalence are AQP4-IgG–seropositive NMOSD, neurosarcoidosis, and
MOG-IgG–associated disorder,43 although other causes exist. For more
information, refer to the articles “Myelitis and Other Autoimmune Myelopathies”
254 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
by Sebastian Lopez Chiriboga, MD, and Eoin P. Flanagan, MBBCh,44 and KEY POINTS
“Infectious Myelopathies” by Michel Toledano, MD,45 in this issue of Continuum.
● Three characteristic
AQP4-IgG–seropositive NMOSD characteristically causes a long-segment features of aquaporin-4-
autoimmune myelopathy, with lesions tending to be three or more segments in IgG–seropositive
length and often expansile (FIGURE 10-12). Three characteristic features of neuromyelitis optica
AQP4-IgG–seropositive NMOSD that may be present are involvement of the spectrum disorder that
may be present are
cervicomedullary junction, T1-hypointense components of the lesion, and foci on
involvement of the
axial images that are at least as T2 hyperintense as CSF (bright spotty lesions) cervicomedullary junction,
(FIGURE 10-12).46-48 The enhancement pattern is often patchy and T1-hypointense components
heterogeneous, and ring or partial ring enhancement (with a prevalence of of the lesion, and foci on
axial images that are at least
approximately 30% to 35% among NMOSD cases) can strongly suggest the
as T2 hyperintense as CSF
diagnosis over neurosarcoidosis (FIGURE 10-12).49,50 (bright spotty lesions).
Sarcoidosis is a noncaseating granulomatous disease that can affect any aspect
of the neuraxis, including any compartment of the spine. The classic finding of ● The enhancement pattern
neurosarcoidosis of the cord is a long-segment myelopathy, with characteristic in aquaporin-4-IgG–
seropositive neuromyelitis
enhancement at the dorsal subpial/pial aspect of the cord (FIGURE 10-12).51 When optica spectrum disorder is
such broad contact with the dorsal cord surface is present, the appearance may be often patchy and
plaquelike or sheetlike. When the enhancement also involves the central canal of heterogeneous, and ring or
the spinal cord, a trident sign can be evident axially (FIGURE 10-12).52 Even partial ring enhancement
can strongly suggest the
during successful treatment, the enhancement may persist (FIGURE 10-12); in a diagnosis over
2016 study, 97% of patients with neurosarcoidosis demonstrated persistent spinal neurosarcoidosis.
cord enhancement at 2 months after presentation compared to 12% of patients
with AQP4-IgG–seropositive NMOSD.53 The spinal canal may also be positive for ● The classic finding of
neurosarcoidosis of the cord
enhancing leptomeningeal disease elsewhere, such as thickening (smooth or
is a long-segment
nodular) of the pial surface or cauda equina nerve roots. Ancillary findings myelopathy, with
outside of the spinal canal should be sought on the index spinal MRI; these characteristic enhancement
include mediastinal and hilar adenopathy (FIGURE 10-12) and osseous lesions. at the dorsal subpial/pial
The latter tend to be lytic or mixed lytic-sclerotic but are not common.54 aspect of the cord.
Among other causes of a longitudinally extensive myelopathy, MOG- ● Selective viral
IgG–associated myelitis can be suggested on MRI. Findings for this involvement of the anterior
inflammatory myelitis are not entirely specific but include more than one horn cells can result in acute
lesion, T2 hyperintensity confined to gray matter, preferential involvement of flaccid paralysis. An
example is the 2014
the thoracolumbar region, and lack of or only minimal enhancement outbreak related to
(FIGURE 10-12).43 enterovirus D68, which
typically resulted in
OTHER NONTUMORAL INFLAMMATORY MYELOPATHIES. Although not as common as the long-segment T2
hyperintensity of the central
aforementioned non-neoplastic intramedullary causes of myelopathy, several
gray matter, particularly in
other intrinsic inflammatory spinal cord diseases are important to recognize. the cervical cord.
Viral myelitis/myelopathy. The spinal cord can be affected by a host of infectious
diseases, including (but not limited to) viruses. For more information, refer to
the article “Infectious Myelopathies” by Michel Toledano, MD,45 in this issue of
Continuum. Other infections, including bacterial, fungal, and rare or endemic
organisms, such as parasites, are not considered here. Both acute viral infection
(myelitis) (FIGURE 10-13) and postviral immunologic reaction (myelopathy) can
occur. MRI can be normal.55 Selective viral involvement of the anterior horn cells
can result in acute flaccid paralysis. An example is the 2014 outbreak related to
enterovirus D68, with its resultant viral myelitis typically characterized by
long-segment T2 hyperintensity of the central gray matter, particularly in the
cervical cord.56 Other viruses with such predilection include polioviruses,
CONTINUUMJOURNAL.COM 255
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
coxsackieviruses, enterovirus 71, West Nile virus, Japanese B encephalitis
virus, and tick-borne encephalitis virus.56 A second primary form of clinical
presentation is mixed motor and sensory dysfunction due to involvement of
white matter or gray matter, or both. This pattern can be seen with infections
such as herpes simplex virus type 2, varicella-zoster virus, cytomegalovirus,
Epstein-Barr virus, rabies, and coxsackieviruses. Human immunodeficiency
virus (HIV) can present with a vacuolar myelopathy that has a predilection for
the lateral and posterior columns, but it can also involve the central aspects of the
cord, including gray matter; neither of these presentations typically enhance.57
Viral myelitis/myelopathy tends to be long segment and can be asymmetric or
symmetric on axial images (FIGURE 10-13). The T2 hyperintensity may be
expansile in nature, and enhancement of the cord or the adjacent meninges or
nerve roots may be present in the acute-early subacute phase (FIGURE 10-13). If
present, hemorrhagic necrosis manifests as heterogeneous signal abnormality,
potentially including hyperintensity on T1-weighted images.58 Viral (and other types
of CNS infections) can also involve the cauda equina nerve roots, which may be
diffusely thickened or enhancing.
Paraneoplastic myelopathy. A rare but likely underreported and underrecognized
immune-mediated cause of myelopathy is a paraneoplastic syndrome most
commonly associated with lung and breast carcinomas. When present, the
spinal cord T2 hyperintensity of paraneoplastic myelopathy is often long
segment, symmetric, and tract specific, such as confined to the lateral or
dorsal columns (FIGURE 10-13).59 The gray matter can also be involved. Because
of tract specificity, the appearance may be relatively linear on sagittal images.
Enhancement after gadolinium administration may be present and may
also be tract specific (FIGURE 10-13).60 An extraspinal primary neoplasm or
evidence of metastatic disease can be a clue to the diagnosis. Other autoimmune
causes of myelopathy can have an identical appearance to paraneoplastic
myelopathy.
TOXIC-METABOLIC-IATROGENIC MYELOPATHY. An important category of intrinsic
myelopathy is that which includes toxic, metabolic, and iatrogenic causes.
SUBACUTE COMBINED DEGENERATION. Subacute combined degeneration of the
spinal cord due to vitamin B12 deficiency has multiple potential causes, including
primary vitamin B12 deficiency (pernicious anemia), inadequate vitamin B12
intake, and nitrous oxide toxicity. The characteristic feature on MRI is selective
involvement of the dorsal columns (FIGURE 10-13); the lateral columns may also
be involved. MRI is relatively insensitive for subacute combined degeneration
but, when positive, demonstrates T2 hyperintensity of the dorsal columns
with an inverted V or inverted rabbit ears morphology on axial images,
especially in the cervical and upper thoracic cord (FIGURE 10-13).61 If the lateral
columns are also involved, a three-point sign may be present. In the
acute-subacute phase, the cord may be mildly enlarged, without or with
enhancement (FIGURE 10-13). With prompt treatment, the cord findings
typically resolve, although not always. The differential of a posterior/
posterolateral column syndrome includes (but is not limited to) copper
deficiency,62 vitamin E deficiency, heroin-induced myelopathy, methotrexate
toxicity, and HIV myelopathy.
256 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RADIATION-INDUCED MYELOPATHY. Radiation-induced myelopathy is rare. It is a KEY POINTS
dose-dependent complication of radiation therapy and can manifest in an acute,
● When present, the spinal
early delayed, or late time frame. When present, MRI features include cord T2 hyperintensity of
nonspecific confluent spindle-shaped or fusiform spinal cord T2 hyperintensity, paraneoplastic myelopathy
with or without expansion. Characteristically, the lateral spinothalamic tracts is often long segment,
and dorsal columns are affected, but the involvement can also be patchy and symmetric, and tract
specific, such as confined to
can include the central cord (FIGURE 10-13). Parenchymal enhancement may be
the lateral or dorsal
present (FIGURE 10-13). In the chronic phase, nonspecific atrophy or columns.
cystic myelomalacia may be present. A key ancillary imaging clue for
radiation-induced myelopathy is associated vertebral body marrow T1 ● MRI is relatively
hyperintensity (fatty marrow replacement) encompassing the radiation port insensitive for subacute
combined degeneration but,
(FIGURE 10-13).63 Cauda equina involvement with abnormal enhancement of when positive,
the nerve roots may also occur as a sequela of radiation. demonstrates T2
hyperintensity of the dorsal
VASCULAR MYELOPATHY. Although a myriad of vascular diseases may affect the columns with an inverted V
or inverted rabbit ears
spinal cord, the two most commonly encountered clinically and on neuroimaging
morphology on axial images,
are spinal cord infarcts and spinal dural arteriovenous fistulas. The clinical especially in the cervical
presentation and imaging findings are distinct. For more information on vascular and upper thoracic cord.
disease affecting the spinal cord, refer to the article “Vascular Myelopathies” by
Nicholas L. Zalewski, MD,64 in this issue of Continuum. ● A key ancillary imaging
clue for radiation-induced
myelopathy is associated
SPINAL CORD INFARCT. Spinal cord infarcts most commonly affect the thoracic cord vertebral body marrow T1
and conus, typically in an anterior spinal artery distribution (FIGURE 10-14). hyperintensity (fatty marrow
replacement) encompassing
MRI may be normal acutely. DWI of the spine is technically challenging
the radiation port.
compared to of the brain; however, it can be sensitive even very early in the
course of the disease. Similar to arterial infarcts in the brain, restricted diffusion ● Similar to arterial infarcts
(with high signal on DWI and low signal on apparent diffusion coefficient in the brain, restricted
images) can be seen in acute spinal cord infarcts (FIGURE 10-14). On diffusion (with high signal on
diffusion-weighted imaging
T2-weighted images of an anterior spinal artery infarct, preferential and low signal on apparent
involvement of the gray matter manifests as an H-shaped or butterfly-shaped diffusion coefficient images)
appearance (FIGURE 10-14), or as an owl-eyes or snake-eyes sign.65 Central gray can be seen in acute spinal
matter involvement is highly characteristic but not pathognomonic, as diseases cord infarcts.
such as acute viral myelitis or Hirayama disease can have a similar appearance.
● On T2-weighted images
The less common posterior spinal artery cord infarct involves the posterolateral of an anterior spinal artery
one-third of the cord, dorsal columns, and posterior horns. In the early infarct, preferential
hyperacute-acute phases of spinal cord infarcts, parenchymal T2 signal involvement of the gray
matter manifests as an
hyperintensity is usually nonexpansile, thin, and pencil-like on sagittal images.65
H-shaped or butterfly-
In the later acute–early subacute phases, cord enlargement may be present. shaped appearance, or as
Spinal cord infarcts can demonstrate parenchymal enhancement in the an owl-eyes or snake-eyes
acute-subacute phase, often linearly involving the anterior gray matter sign.
(FIGURE 10-14).66 Hemorrhagic conversion can occur3 but is not common.67
● Because of the shared
Because of the shared blood supply of the spinal cord and vertebral bodies, blood supply of the spinal
vertebral body infarcts may be observed, usually 1 to 2 weeks after the initial cord and vertebral bodies,
presentation of spinal cord infarct. These osseous infarcts are characterized by vertebral body infarcts may
geographic, irregular, often serpiginously marginated regions of vertebral be observed, usually 1 to
2 weeks after the initial
marrow abnormality and enhancement (FIGURE 10-14). Enhancement of the presentation of spinal cord
ventral cauda equina roots may be evident in the subacute phase of spinal cord infarct.
infarct (FIGURE 10-14).68,69 This finding is of unknown etiology, although
potentially caused by wallerian degeneration or direct ischemia. The underlying
vascular origin for the infarct can be sought on imaging but is infrequently
CONTINUUMJOURNAL.COM 257
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
FIGURE 10-14
Vascular myelopathies. Spinal cord infarct (A through G, I through L, two different patients)
may be MRI negative, especially on conventional T2-weighted images shortly after symptom
onset (A). In the later acute and early subacute phase, involvement of the thoracic cord/
conus by T2 hyperintensity is most common (B through D, I, white arrows). An anterior spinal
artery infarct commonly affects the gray matter preferentially, with an H-shaped or
butterfly-shaped pattern on axial images (C, white arrows). Markedly hyperintense signal on
diffusion-weighted imaging matched by hypointense signal on apparent diffusion
coefficient (restricted diffusion, E, F, white arrows) is a key clue for an acute infarct. The
infarct may also demonstrate gray matter enhancement in the acute-subacute phase (G, H, J,
white arrows). Two helpful ancillary findings that may be present, especially in the subacute
phase, are vertebral body infarcts (I, J, blue arrows) and cauda equina enhancement (J, K,
arrowheads). Spinal dural arteriovenous fistula (M through V) is an often-missed diagnosis.
Key clues are parenchymal T2 hyperintensity, especially of the distal cord/conus sagittally
on lumbar spine MRI (M, P, blue arrows) and T2-hypointense flow voids (M, white arrows) or
vascular enhancement (R, white arrows) along the cord/conus, related to increased pial
vascularity. These subtle findings were not detected on this MRI, with the spinal stenosis at
L4-L5 (M through O) being a major distracting feature. Six months after presentation, with the
patient now having undergone an L4-L5 laminectomy (Q), a lumbar spine and myelopathy
protocol thoracic spine MRI were performed. The spinal cord T2 hyperintensity (P, blue
arrow), surface flow voids (P, white arrows), and vascular enhancement (R, white arrows)
were identified. The parenchymal T2 hyperintensity is well seen on sagittal short tau
inversion recovery (STIR) images (T, blue arrow) and involves the central aspects of the cord
on axial images (S, blue arrow). Magnetic resonance angiography (MRA) shows the abnormal
vascularity (U, white arrows) and suggests an origin for the arteriovenous malformation at L4
(U, blue arrow), confirmed on conventional angiography upon injection of a common L4
segmental arterial trunk (V, blue arrow). Cavernous malformations (cavernomas)
(W through CC) usually have heterogeneous signal intensity on both T2-weighted (W, X) and
T1-weighted images (BB). This heterogeneity can include inherent T1 hyperintensity due to
subacute blood products (BB). The lesions may present with partial or complete
T2-hypointense rims (W, X, blue arrows). Even more prevalent is relatively linear extension of
typically T2-hypointense and often also T1-hypointense blood products in the spinal cord
cranially or caudally away from the lesion (W, Y through AA, white arrows). Enhancement of
cavernous malformations is usually either lacking (CC) or minimal, when allowing for inherent
T1 hyperintensity.
258 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
evident on MRI, MRA, CT angiography, or conventional angiography; after KEY POINTS
full imaging and clinical workup, the cause of a spinal cord infarct frequently
● Enhancement of the
remains occult. ventral cauda equina roots
may be evident in the
SPINAL DURAL ARTERIOVENOUS FISTULA. Spinal dural arteriovenous fistulas are the subacute phase of spinal
most common type of spinal cord vascular malformation. They typically cord infarct.
represent a single arterial-to-venous shunt at a thoracic or lumbar radicular artery
● The classic finding of a
in the dural nerve root sleeve and can occur anywhere from the vertebral to the spinal dural arteriovenous
internal iliac arteries. This abnormal shunt causes venous hypertension of the fistula is increased posterior
spinal cord. Early detection is critical to maximize the chance of a good outcome; pial serpentine vascularity,
however, despite characteristic imaging features, spinal dural arteriovenous typically best seen on
T2-weighted sagittal images
fistulas are frequently missed or misdiagnosed.70 The classic finding of a spinal as prominent flow voids
dural arteriovenous fistula is increased posterior pial serpentine vascularity, within the dilated veins
typically best seen on T2-weighted sagittal images as prominent flow voids within along the dorsal cord
the dilated veins along the dorsal cord surface (FIGURE 10-14). These flow voids surface.
represent a dilated coronal venous plexus and demonstrate enhancement with
gadolinium because of slowed flow. They are present in approximately 85% of
cases. In strongly suspected but subtle cases, heavily T2-weighted thin-section
volumetric sequences may help visualize the flow voids and fistula.71 Differential
considerations for such flow voids include other rare vascular malformations
such as arteriovenous malformations and vascular neoplasms such as
hemangioblastomas, myxopapillary ependymomas, and paragangliomas. The
venous hypertension of the spinal cord parenchyma typically results in edema and
expansile cord and conus T2 hyperintensity often sparing the peripheralmost
aspect of the cord (FIGURE 10-14), with or without amorphous cord enhancement.
The conus is involved in the majority of cases (95%). If the conus is spared, the
location of the fistula is likely thoracic.72 The upper cervical cord may be involved
from a posterior fossa arteriovenous fistula. In a 2018 series, enhancement was
observed in 86% of cases of spinal dural arteriovenous fistulas, with 43% of these
demonstrating a so-called missing piece morphology, which is defined as at least
one focal geographic nonenhancing area within a long (more than two vertebral
segments) segment of intense holocord (whole cross-sectional area of spinal cord)
gadolinium enhancement.73 MRA with gadolinium-bolus technique can localize
or suggest the likely level of the shunting lesion and guide conventional catheter
angiography (FIGURE 10-14), thus decreasing the time, radiation dose, and volume
of contrast material required to identify the nidus.74 Catheter angiography is the
gold standard imaging technique for diagnosis, allowing localization of the shunt
and of the anterior spinal artery. After treatment with embolization or surgery,
imaging findings can persist, even if therapy has been successful. Progression of
findings, particularly worsening of parenchymal T2 hyperintensity, suggests
incomplete treatment or recurrence.75
CAVERNOUS MALFORMATION. Cavernous malformations of the cord are tumors
related to repetitive hemorrhage and present as mass lesions (FIGURE 10-14).
These low-flow vascular lesions are often relatively small at presentation; larger
size (>1 cm) is a predictor of subsequent hemorrhage.76 They can be multiple
or synchronously present in the brain, especially in familial cases. The presence
of hemorrhage within or adjacent to the lesion is a clue to the diagnosis. Blood
products have complex signal characteristics on MRI, which are age dependent.
As in the brain, spinal cord cavernous malformations classically may have a
CONTINUUMJOURNAL.COM 259
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
KEY POINT popcorn-type morphology, with well-circumscribed but lobulated margins and
a reticulated core of heterogeneous T1 and T2 signal abnormality. If subacute
● Adjacent hemorrhage in
the spinal cord extending
hemorrhage is present, T1 hyperintensity is expected (FIGURE 10-14). Classically,
craniocaudally away from a a T2-hypointense rim representing hemosiderin may surround the lesion
cavernous malformation is (FIGURE 10-14). Sequences sensitive to hemosiderin, such as GRE, will
relatively prevalent; a 2020 demonstrate pronounced hypointensity (blooming) of the lesion. Spinal cord
retrospective series
edema may accompany a cavernous malformation if it has recently bled.
demonstrated that this
finding is more common than Adjacent hemorrhage in the spinal cord extending craniocaudally away from a
some classic features of cavernous malformation is relatively prevalent; a 2020 retrospective series
these lesions, such as demonstrated that this finding is more common than some of the
popcorn morphology and
aforementioned classic features of these lesions, such as popcorn morphology
T2-hypointense rim.
and T2-hypointense rim (FIGURE 10-14).77 Lesional enhancement is typically
either not present or only minimal in degree. The differential diagnosis for a
hemorrhagic cord lesion also includes a neoplasm (especially hemangioblastoma
or ependymoma) and posttraumatic contusion/hematoma.
CONCLUSION
A rational imaging approach to myelopathy should be employed. MRI is typically
first line, and a protocol tailored to the indication is advised. Abnormal T2
hyperintensity of the spinal cord has a broad differential diagnosis. Imaging
features should be sought that can help arrive at specific diagnoses or a narrowed
list of differential considerations. The process of narrowing the differential
diagnosis starts with placing the lesion into one of three compartments:
extradural, intradural-extramedullary, and intramedullary. Imaging features of
the lesion itself and of the adjacent spinal column, paraspinal soft tissues, and
visualized nonspinal regions must be evaluated. Both precontrast and
postcontrast MRI can hold clues to the diagnosis. Specific contrast enhancement
patterns can be helpful in correctly identifying individual disease processes. CT
myelography can help evaluate lesions of the arachnoid and dura, particularly the
spectrum of disease that includes arachnoid cyst, arachnoid web, and idiopathic
cord herniation. For some conditions that have a dynamic positional component,
flexion MRI or upright MRI/CT myelography can be helpful.
REFERENCES
1 Zalewski NL, Flanagan EP, Keegan BM. Evaluation 4 Vargas MI, Gariani J, Sztajzel R, et al. Spinal cord
of idiopathic transverse myelitis revealing ischemia: practical imaging tips, pearls, and
specific myelopathy diagnoses. Neurology 2018; pitfalls. AJNR Am J Neuroradiol 2015;36(5):
90(2):e96-e102. doi:10.1212/ 825-830. doi:10.3174/ajnr.A4118
WNL.0000000000004796
5 Hardy TA. Spinal cord anatomy and localization.
2 Lee MJ, Aronberg R, Manganaro MS, et al. Continuum (Minneap Minn) 2021;27(1, Spinal Cord
Diagnostic approach to intrinsic abnormality of Disorders):12-29.
spinal cord signal intensity. Radiographics 2019;
6 Diehn FE, Maus TP, Morris JM, et al. Uncommon
39(6):1824-1839. doi:10.1148/rg.2019190021
manifestations of intervertebral disk pathologic
3 Flanagan EP, Hunt CH, Lowe V, et al. conditions. Radiographics 2016;36(3):801-823.
[(18)F]-fluorodeoxyglucose-positron emission doi:10.1148/rg.2016150223
tomography in patients with active myelopathy.
Mayo Clin Proc 2013;88(11):1204-1212. doi:10.1016/j.
mayocp.2013.07.019
260 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
7 Zarrabian MM, Diehn FE, Kotsenas AL, et al. Dorsal 21 Boruah DK, Prakash A, Gogoi BB, et al. The
lumbar disc migrations with lateral and ventral importance of flexion MRI in Hirayama disease
epidural extension on axial MRI: a case series and with special reference to laminodural space
review of the literature. AJNR Am J Neuroradiol measurements. AJNR Am J Neuroradiol 2018;
2016;37(11):2171-2177. doi:10.3174/ajnr.A4875 39(5):974-980. doi:10.3174/ajnr.A5577
8 Choi JY, Lee WS, Sung KH. Intradural lumbar disc 22 Hirayama K, Tokumaru Y. Cervical dural sac and
herniation–is it predictable preoperatively? spinal cord in juvenile muscular atrophy of distal
A report of two cases. Spine J 2007;7(1):111-117. upper extremity. Neurology 2000;54(10):
doi:10.1016/j.spinee.2006.02.025 1922-1926. doi:10.1212/wnl.54.10.1922
9 Maus T. Imaging the back pain patient. Phys Med 23 Huang YL, Chen CJ. Hirayama disease.
Rehabil Clin N Am 2010;21(4):725-766. doi:10.1016/ Neuroimaging Clin N Am 2011;21(4):939-50, ix-x.
j.pmr.2010.07.004 doi:10.1016/j.nic.2011.07.009
10 Pierce JL, Donahue JH, Nacey NC, et al. Spinal 24 Chen CJ, Hsu HL, Tseng YC, et al. Hirayama
hematomas: what a radiologist needs to know. flexion myelopathy: neutral-position MR imaging
Radiographics 2018;38(5):1516-1535. doi:10.1148/ findings–importance of loss of attachment.
rg.2018180099 Radiology 2004;231(1):39-44. doi:10.1148/
radiol.2311030004
11 Diehn FE. Imaging of spine infection. Radiol Clin North
Am 2012;50(4):777-798. doi:10.1016/j.rcl.2012.04.001 25 Strauss SB, Gordon SR, Burns J, et al.
Differentiation between tuberculous and
12 Maus TP. Imaging of spinal stenosis: neurogenic
pyogenic spondylodiscitis: the role of the
intermittent claudication and cervical
anterior meningovertebral ligament in patients
spondylotic myelopathy. Radiol Clin North Am
with anterior epidural abscess. AJNR Am J
2012;50(4):651-679. doi:10.1016/j.rcl.2012.04.007
Neuroradiol 2020;41(2):364-368. doi:10.3174/ajnr.
13 Flanagan EP, Marsh RW, Weinshenker BG. A6370
Teaching neuroimages: "pancake-like"
26 Kim DH, Rosenblum JK, Panghaal VS, et al.
gadolinium enhancement suggests compressive
Differentiating neoplastic from nonneoplastic
myelopathy due to spondylosis. Neurology 2013;
processes in the anterior extradural space.
80(21):e229. doi:10.1212/WNL.0b013e318293e346
Radiology 2011;260(3):825-830. doi:10.1148/
14 Flanagan EP, Krecke KN, Marsh RW, et al. Specific radiol.11102287
pattern of gadolinium enhancement in
27 Koeller KK, Shih RY. Intradural extramedullary
spondylotic myelopathy. Ann Neurol
spinal neoplasms: radiologic-pathologic
2014;76(1):54-565. doi:10.1002/ana.24184
correlation. Radiographics 2019;39(2):468-490.
15 Boet R, Chan YL, King A, et al. Contrast enhancement doi:10.1148/rg.2019180200
of the spinal cord in a patient with cervical
28 Madhavan AA, Summerfield D, Hunt CH, et al.
spondylotic myelopathy. J Clin Neurosci
Polyclonal lymphocytic infiltrate with
2004;11(5):512-514. doi:10.1016/j.jocn.2004.02.005
arachnoiditis resulting from intrathecal stem cell
16 Conway BL, Clarke MJ, Kaufmann TJ, Flanagan EP. transplantation. Neuroradiol J 2020;33(2):174-178.
Utility of extension views in spondylotic doi:10.1177/1971400920902451
myelopathy mimicking transverse myelitis.
29 Mohajeri Moghaddam S, Bhatt AA. Location,
Mult Scler Relat Disord 2017;11:62-64. doi:10.1016/
length, and enhancement: systematic approach
j.msard.2016.12.004
to differentiating intramedullary spinal cord
17 Stino AM, LoRusso SJ. Myelopathies due to lesions. Insights Imaging 2018;9(4):511-526.
structural cervical and thoracic disease. doi:10.1007/s13244-018-0608-3
Continuum (Minneap Minn) 2018;24(2, Spinal
30 Anderson TL, Morris JM, Wald JT, Kotsenas AL.
Cord Disorders):567-583. doi:10.1212/
Imaging appearance of advanced chronic
CON.0000000000000594
adhesive arachnoiditis: a retrospective review.
18 Barz T, Melloh M, Staub LP, et al. Nerve root AJR Am J Roentgenol 2017;209(3):648-655.
sedimentation sign: evaluation of a new doi:10.2214/AJR.16.16704
radiological sign in lumbar spinal stenosis. Spine
31 Reardon MA, Raghavan P, Carpenter-Bailey K,
(Phila Pa 1976) 2010;35(8):892-897. doi:10.1097/
et al. Dorsal thoracic arachnoid web and the
BRS.0b013e3181c7cf4b
"scalpel sign": a distinct clinical-radiologic entity.
19 Wang G, Peng Z, Li J, et al. Diagnostic AJNR Am J Neuroradiol 2013;34(5):1104-1110.
performance of the nerve root sedimentation doi:10.3174/ajnr.A3432
sign in lumbar spinal stenosis: a systematic
32 Haber MD, Nguyen DD, Li S. Differentiation of
review and meta-analysis. Neuroradiology 2019;
idiopathic spinal cord herniation from
61(10):1111-1121. doi:10.1007/s00234-019-02248-3
CSF-isointense intraspinal extramedullary lesions
20 Lehman VT, Luetmer PH, Sorenson EJ, et al. displacing the cord. Radiographics 2014;34(2):
Cervical spine MR imaging findings of patients 313-329. doi:10.1148/rg.342125136
with Hirayama disease in North America: a
multisite study. AJNR Am J Neuroradiol 2013;
34(2):451-456. doi:10.3174/ajnr.A3277
CONTINUUMJOURNAL.COM 261
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMAGING OF SPINAL CORD AND CAUDA EQUINA
33 Brus-Ramer M, Dillon WP. Idiopathic thoracic 45 Toledano M. Infectious myelopathies.
spinal cord herniation: retrospective analysis Continuum (Minneap Minn) 2021;27(1, Spinal Cord
supporting a mechanism of diskogenic dural Disorders):93-120.
injury and subsequent tamponade. AJNR Am J
46 Yonezu T, Ito S, Mori M, et al. "Bright spotty
Neuroradiol 2012;33(1):52-56. doi:10.3174/ajnr.
lesions" on spinal magnetic resonance imaging
A2730
differentiate neuromyelitis optica from multiple
34 Koeller KK, Rosenblum RS, Morrison AL. sclerosis. Mult Scler 2014;20(3):331-337.
Neoplasms of the spinal cord and filum doi:10.1177/1352458513495581
terminale: radiologic-pathologic correlation.
47 Chee CG, Park KS, Lee JW, et al. MRI features of
Radiographics 2000;20(6):1721-1749. doi:10.1148/
aquaporin-4 antibody-positive longitudinally
radiographics.20.6.g00nv151721
extensive transverse myelitis: insights into the
35 Rykken JB, Diehn FE, Hunt CH, et al. Rim and diagnosis of neuromyelitis optica spectrum
flame signs: postgadolinium MRI findings disorders. AJNR Am J Neuroradiol 2018;39(4):
specific for non-CNS intramedullary spinal cord 782-787. doi:10.3174/ajnr.A5551
metastases. AJNR Am J Neuroradiol 2013;34(4):
48 Pekcevik Y, Mitchell CH, Mealy MA, et al.
908-915. doi:10.3174/ajnr.A3292
Differentiating neuromyelitis optica from other
36 Madhavan AA, Diehn FE, Rykken JB, et al. The causes of longitudinally extensive transverse
central dot sign: a specific post-gadolinium myelitis on spinal magnetic resonance imaging.
enhancement feature of intramedullary spinal Mult Scler 2016;22(3):302-311. doi:
cord metastases. Clin Neuroradiol. Published 10.1177/1352458515591069
online May 7, 2020. doi:10.1007/s00062-020-
49 Zalewski NL, Morris PP, Weinshenker BG, et al.
00909-y
Ring-enhancing spinal cord lesions in
37 Diehn FE, Rykken JB, Wald JT, et al. Intramedullary neuromyelitis optica spectrum disorders.
spinal cord metastases: prognostic value of MRI J Neurol Neurosurg Psychiatry 2017;88(3):218-225.
and clinical features from a 13-year institutional doi:10.1136/jnnp-2016-314738
case series. AJNR Am J Neuroradiol 2015;36(3):
50 Yokote H, Nose Y, Ishibashi S, et al. Spinal cord
587-593. doi:10.3174/ajnr.A4160
ring enhancement in patients with neuromyelitis
38 Rykken JB, Diehn FE, Hunt CH, et al. optica. Acta Neurol Scand 2015;132(1):37-41. doi:
Intramedullary spinal cord metastases: MRI and 10.1111/ane.12354
relevant clinical features from a 13-year
51 Nesbit GM, Miller GM, Baker HL Jr, et al. Spinal
institutional case series. AJNR Am J Neuroradiol
cord sarcoidosis: a new finding at MR imaging
2013;34(10):2043-2049. doi:10.3174/ajnr.A3526
with Gd-DTPA enhancement. Radiology 1989;
39 Mostardi PM, Diehn FE, Rykken JB, et al. 173(3):839-843. doi:10.1148/radiology.173.3.2813795
Intramedullary spinal cord metastases: visibility
52 Zalewski NL, Krecke KN, Weinshenker BG, et al.
on PET and correlation with MRI features. AJNR
Central canal enhancement and the trident sign
Am J Neuroradiol 2014;35(1):196-201. doi:10.3174/
in spinal cord sarcoidosis. Neurology 2016;87(7):
ajnr.A3618
743-744. doi:10.1212/WNL.0000000000002992
40 Thompson AJ, Banwell BL, Barkhof F, et al.
53 Flanagan EP, Kaufmann TJ, Krecke KN, et al.
Diagnosis of multiple sclerosis: 2017 revisions of
Discriminating long myelitis of neuromyelitis
the McDonald criteria. Lancet Neurol 2018;17(2):
optica from sarcoidosis. Ann Neurol 2016;79(3):
162-173. doi:10.1016/S1474-4422(17)30470-2
437-447. doi:10.1002/ana.24582
41 Traboulsee A, Simon JH, Stone L, et al. Revised
54 Soni N, Bathla G, Pillenahalli Maheshwarappa R.
Recommendations of the Consortium of MS
Imaging findings in spinal sarcoidosis: a report of
Centers Task Force for a Standardized MRI
18 cases and review of the current literature.
Protocol and Clinical Guidelines for the Diagnosis
Neuroradiol J 2019;32(1):17-28.
and Follow-Up of Multiple Sclerosis.
doi:10.1177/1971400918806634
AJNR Am J Neuroradiol 2016;37(3):394-401.
doi:10.3174/ajnr.A4539 55 Grill MF. Infectious myelopathies. Continuum
(Minneap Minn) 2018;24(2, Spinal Cord
42 Asnafi S, Morris PP, Sechi E, et al. The frequency
Disorders):441-473. doi:10.1212/
of longitudinally extensive transverse myelitis
CON.0000000000000597
in MS: a population-based study. Mult Scler
Relat Disord 2020;37:101487. doi:10.1016/j. 56 Maloney JA, Mirsky DM, Messacar K, et al. MRI
msard.2019.101487 findings in children with acute flaccid
paralysis and cranial nerve dysfunction occurring
43 Dubey D, Pittock SJ, Krecke KN, et al. Clinical,
during the 2014 enterovirus D68 outbreak.
radiologic, and prognostic features of myelitis
AJNR Am J Neuroradiol 2015;36(2):245-250.
associated with myelin oligodendrocyte
doi:10.3174/ajnr.A4188
glycoprotein autoantibody. JAMA Neurol 2019;
76(3):301-309. doi:10.1001/jamaneurol.2018.4053 57 Rovira A, Auger C. Spinal cord in multiple
sclerosis: magnetic resonance imaging features
44 Lopez Chiriboga S, Flanagan EP. Myelitis and
and differential diagnosis. Semin Ultrasound CT
other autoimmune myelopathies. Continuum
MR 2016;37(5):396-410. doi:10.1053/j.
(Minneap Minn) 2021;27(1, Spinal Cord Disorders):
sult.2016.05.005
62-92.
262 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
58 Yokota H, Yamada K. Viral infection of the 69 Zalewski NL, Rabinstein AA, Krecke KN, et al.
spinal cord and roots. Neuroimaging Clin N Am Spinal cord infarction: clinical and imaging
2015;25(2):247-258. doi:10.1016/j.nic.2015.01.005 insights from the periprocedural setting. J Neurol
Sci 2018;388:162-167. doi:10.1016/j.jns.2018.03.029
59 Zalewski NL, Flanagan EP. Autoimmune and
paraneoplastic myelopathies. Semin Neurol 2018; 70 Brinjikji W, Nasr DM, Morris JM, et al. Clinical
38(3):278-289. doi:10.1055/s-0038-1660856 outcomes of patients with delayed diagnosis
of spinal dural arteriovenous fistulas.
60 Madhavan AA, Carr CM, Morris PP, et al. Imaging
AJNR Am J Neuroradiol 2016;37(2):380-386.
review of paraneoplastic neurologic syndromes.
doi:10.3174/ajnr.A4504
AJNR Am J Neuroradiol 2020;41(12):2176-2187. doi:
10.3174/ajnr.A6815 71 Morris JM, Kaufmann TJ, Campeau NG, et al.
Volumetric myelographic magnetic resonance
61 Schwendimann RN. Metabolic and toxic
imaging to localize difficult-to-find spinal dural
myelopathies. Continuum (Minneap Minn) 2018;
arteriovenous fistulas. J Neurosurg Spine 2011;
24(2, Spinal Cord Disorders):427-440. doi:10.1212/
14(3):398-404. doi:10.3171/2010.11.SPINE10328
CON.0000000000000596
72 Muralidharan R, Saladino A, Lanzino G, et al. The
62 Kumar N, Ahlskog JE, Klein CJ, Port JD. Imaging
clinical and radiological presentation of spinal
features of copper deficiency myelopathy: a
dural arteriovenous fistula. Spine (Phila Pa 1976)
study of 25 cases. Neuroradiology 2006;48(2):
2011;36(25):E1641-E1647. doi:10.1097/
78-83. doi:10.1007/s00234-005-0016-5
BRS.0b013e31821352dd
63 Khan M, Ambady P, Kimbrough D, et al.
73 Zalewski NL, Rabinstein AA, Brinjikji W, et al.
Radiation-induced myelitis: initial and follow-up
Unique gadolinium enhancement pattern in
MRI and clinical features in patients at a single
spinal dural arteriovenous fistulas. JAMA Neurol
tertiary care institution during 20 years. AJNR Am J
2018;75(12):1542-1545. doi:10.1001/
Neuroradiol 2018;39(8):1576-1581. doi:10.3174/ajnr.
jamaneurol.2018.2605
A5671
74 Luetmer PH, Lane JI, Gilbertson JR, et al.
64 Zalewski NL. Vascular myelopathies. Continuum
Preangiographic evaluation of spinal dural
(Minneap Minn) 2021;27(1, Spinal Cord Disorders):
arteriovenous fistulas with elliptic centric
30-61.
contrast-enhanced MR angiography and effect
65 Kranz PG, Amrhein TJ. Imaging approach to on radiation dose and volume of iodinated
myelopathy: acute, subacute, and chronic. Radiol contrast material. AJNR Am J Neuroradiol
Clin North Am 2019;57(2):257-279. 2005;26(4):711-718.
doi:10.1016/j.rcl.2018.09.006
75 Muralidharan R, Mandrekar J, Lanzino G, et al.
66 Zalewski NL, Rabinstein AA, Krecke KN, et al. Prognostic value of clinical and radiological signs
Characteristics of spontaneous spinal in the postoperative outcome of spinal dural
cord infarction and proposed diagnostic criteria. arteriovenous fistula. Spine (Phila Pa 1976) 2013;
JAMA Neurol 2019;76(1):56-63. 38(14):1188-1193. doi:10.1097/
doi:10.1001/jamaneurol.2018.2734 BRS.0b013e31828b2e10
67 Laur O, Nandu H, Titelbaum DS, et al. 76 Goyal A, Rinaldo L, Alkhataybeh R, et al. Clinical
Nontraumatic spinal cord compression: MRI presentation, natural history and outcomes of
primer for emergency department radiologists. intramedullary spinal cord cavernous
Radiographics 2019;39(6):1862-1880. malformations. J Neurol Neurosurg Psychiatry
doi:10.1148/rg.2019190024 2019;90(6):695-703. doi:10.1136/jnnp-2018-319553
68 Diehn FE, Hunt CH, Lehman VT, et al. Vertebral 77 Panda A, Diehn FE, Kim DK, et al. Spinal cord
body infarct and ventral cauda equina cavernous malformations: MRI commonly shows
enhancement: two confirmatory findings of adjacent intramedullary hemorrhage.
acute spinal cord infarct. J Neuroimaging 2015; J Neuroimaging 2020;30(5):690-696.
25(1):133-135. doi:10.1111/jon.12058 doi:10.1111/jon.12738
CONTINUUMJOURNAL.COM 263
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
REVIEW ARTICLE
Spinal Cord Anatomy
C O N T I N UU M AUDIO
I NT E R V I E W A V AI L A B L E
ONLINE
and Localization
By Todd A. Hardy, PhD, MBBS, FRACP
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNrC3bBuCzr1RdmqNUpjE4IY on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This
article focuses on clinically relevant teaching points
in spinal anatomy and localizing the lesion in myelopathy.
RECENT FINDINGS: The principles underlying spinal
cord lesion localization are
well established, but improvements in MRI and the discovery of pathologic
antibodies associated with causes of transverse myelitis distinct from
multiple sclerosis, such as aquaporin-4 IgG and myelin oligodendrocyte
glycoprotein IgG, have assisted in diagnosis.
SUMMARY: The spinal cord has a highly organized neuroanatomy of
ascending and descending tracts that convey sensory, motor, and
autonomic information. Using integration of clues from the patient’s history
and neurologic examination, the effective clinician can distinguish spinal
cord from peripheral nerve or brain pathology, often determine the level
CITE AS: and parts of the spinal cord affected by a lesion, and focus on a likely
CONTINUUM (MINNEAP MINN) diagnosis. The advent of MRI of the spine has revolutionized investigation
2021;27(1, SPINAL CORD DISORDERS):
12–29.
of spinal cord disorders, but an important place for strong clinical acumen
still exists in assessing the patient with a myelopathy.
Address correspondence to
Dr Todd A. Hardy, Department of
Neurology, Concord Repatriation
General Hospital, Hospital Road, INTRODUCTION
Concord, NSW 2139, Australia,
A
todd.hardy@sydney.edu.au. thorough understanding of the anatomy of the spinal cord is of
value to the neurologist because patients can present with an array
RELATIONSHIP DISCLOSURE:
Dr Hardy serves as coeditor of
of symptoms and signs referable to the spinal cord, and the capacity
Advances in Clinical to distinguish cord pathology from brain or peripheral nerve
Neuroscience and Rehabilitation pathology facilitates early diagnosis and avoids unnecessary
and on an advisory board for
Merck & Co, Inc. Dr Hardy has
investigations. Early diagnosis is particularly important because the consequences
received personal compensation of delayed diagnosis of spinal cord pathology can be devastating, with the
for speaking engagements from potential for permanent disability.
Biogen; Merck & Co, Inc; Novartis
AG; Sanofi Genzyme; and Teva The neuroanatomy of the spinal cord is somatotopically and segmentally
Pharmaceutical Industries Ltd organized, with tracts and pathways that transmit sensory information from
and research/grant support from
organs and peripheral receptors to the brain and motor information from the
Novartis AG.
brain to internal and peripheral effector organs. This means that sensory or
UNLABELED USE OF motor deficits in one area of the body can often be deduced to be due to damage
PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
in a specific area of the spinal cord.
Dr Hardy reports no disclosure. The localization of lesional pathology is an essential skill for the neurologist
and helps with differential diagnosis and targeted investigation. For the most
© 2021 American Academy part, spinal cord lesions are associated with upper motor neuron signs. The
of Neurology. approach to a patient with a suspected myelopathy involves ascertaining the
12 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
motor and sensory level of the lesion. Certain patterns of signs may lead a KEY POINT
neurologist to diagnose a spinal cord syndrome, such as a Brown-Séquard
● Lumbar puncture is
syndrome accompanying a partial transverse myelitis, which may provide a clue typically performed at the
to the etiology of the underlying disease process. L3-L4 or L4-L5 level.
The advent of MRI has revolutionized the diagnosis of myelopathies to the
extent that specific diagnoses can often be made with MRI alone. Nevertheless,
not all myelopathies are associated with MRI lesions, and, occasionally, subtle
spinal cord lesions may be missed or difficult to appreciate on MRI. MRI can also
identify unrelated pathologies or red herrings that may divert attention away
from the actual diagnosis, which means that the clinical history and examination
must be used in conjunction with MRI or other adjunctive investigations to
establish a diagnosis.
This article focuses on clinically relevant neuroanatomy of the spinal cord and
explains how neurologic symptoms and signs relate to the anatomy to give clues
that enable the correct localization of spinal cord pathology.
ANATOMY OF THE SPINAL CORD
The spinal cord is a central nervous system (CNS) structure that arises from the
inferior medulla of the brainstem above the C1 vertebra and runs in the spinal
canal to terminate at the L1-L2 level of the lumbar spine (FIGURE 1-11). It is
covered in the meninges, which are contiguous with the meninges of the brain;
from the innermost layer to the outermost layer, the meninges are the pia,
arachnoid, and dura mater. The spinal cord is broadly divided longitudinally into
the cervical, thoracic, and lumbar regions, with the sacral spinal cord region that
represents the very lower aspect of the spinal cord referred to as the conus
medullaris. A modified fibrous termination of the pia mater called the filum
terminale extends from the conus medullaris caudally to the coccyx, fusing at its
lower end with the dura mater, where it anchors the entire spinal cord to the
vertebral column.2,3
Enlargements in the cervical region and lumbar regions reflect increased
numbers of neurons in these regions to supply the upper and lower limbs,
respectively (FIGURE 1-1). Pairs of sensory and motor nerve roots emerge at
distinct spinal levels throughout the length of the cord.3 Sensory nerve roots
emerge dorsally from the cord and motor nerve roots emerge ventrally before
they meet to form mixed motor and sensory spinal nerves. The nerve roots are
numbered C1 through C8 when they arise from the cervical cord and T1 through
T12 when they arise from the thoracic cord. The lumbar L1 nerve roots emerge
just below the T12 nerve roots. The lowermost nerve roots (lumbar, L2 through
L5; sacral, S1 through S5; and the coccygeal nerve) fan out distally from the lower
cord and are referred to as the cauda equina (Latin for horse’s tail). Critically,
only the sacral nerve roots emerge from the conus medullaris. The lowermost
nerve roots inhabit the CSF-filled subarachnoid space that is formed because the
pia-covered spinal cord terminates at L1-L2, but the arachnoid and dura continue
to the S2 vertebral level. The subarachnoid space is clinically relevant as the site
from which CSF can be collected in a lumbar puncture without risk to the spinal
cord, as it is typically performed at the L3-L4 or L4-L5 level.4
Cross-sectional Anatomy of the Spinal Cord
The spinal cord is highly somatotopically organized, and its function is to
transmit motor, sensory, and autonomic information.2,3 The neurons of the
CONTINUUMJOURNAL.COM 13
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
FIGURE 1-1
The gross anatomy of the spinal cord and adjacent spinal nerve roots.
Reprinted with permission from Moore KL, et al, Wolters Kluwer/Lippincott Williams & Wilkins.1
© 2014 Lippincott Williams & Wilkins.
spinal cord are located centrally in an H-shaped or butterfly-shaped area known
as the central gray matter (FIGURE 1-2). The central gray matter is connected
across the midline by the gray commissure, within which lies the central canal of
the cord. The anterior and posterior columns of the gray matter are usually
referred to as the ventral and dorsal horns. The ventral horns contain alpha and
gamma motor neurons and interneurons. Somatic motor neurons travel in the
medial motor columns, where they innervate the axial muscles of the body, or in
the lateral motor columns, where they innervate the upper and lower limbs. The
dorsal horns are where somatic and visceral afferent (sensory) fibers enter the
cord. Their cell bodies are in adjacent dorsal root ganglia. The intermediate gray
14 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
● The butterfly-shaped
area of the spinal cord in
cross section is known as
the central gray matter.
● The descending motor
pathways in the cord before
the anterior horns are called
upper motor neurons, and
those of the anterior horns
and somatic motor nerves
are called lower motor
neurons.
FIGURE 1-2
Cross-sectional anatomy of the gray and white matter tracts of the spinal cord.
Reprinted with permission from Cho TA, Continuum (Minneap Minn).3 © 2015 American
Academy of Neurology.
layer between the ventral and dorsal horns is where autonomic preganglionic
cells lie, divided into intermediolateral and intermediomedial groups; the
preganglionic sympathetic neurons are located from C8 through L1. The
preganglionic parasympathetic neurons are located from S2 through S4.
The white matter of the spinal cord surrounds the gray matter and is
composed of myelinated axons. Principal white matter tracts of clinical
significance include the descending motor pathways of the corticospinal
(pyramidal) tract, which run laterally and anteriorly (ventrally) in the cord
throughout its length (FIGURE 1-3).5 These convey somatic motor information
arising from the contralateral cerebral cortex, which decussates in the anterior
medulla just before entering the cervical spinal cord. The descending motor
pathways of the corticospinal tract synapse with the anterior horns cells that
convey motor information via the motor nerve roots and then via somatic
(peripheral) motor neurons to a target muscle. The descending motor pathways
in the cord before the anterior horns are called upper motor neurons, and those of
the anterior horns and somatic motor nerves are called lower motor neurons.
Additional descending motor pathways referred to as extrapyramidal tracts
arise from the brainstem and convey involuntary information important in
different aspects of motor control (FIGURE 1-3).5 Important extrapyramidal tracts
include the rubrospinal tract, which transmits information to the spinal
interneurons to maintain balance; the reticulospinal tract, which transmits
motor information from the reticular formation in the brainstem; the tectospinal
tract, which assists in coordinating head and eye movements; and the
vestibulospinal tract, which transmits balance information to the extremities
from the vestibular system.
Somatosensory information in the form of temperature, pinprick sensation,
and touch is carried anterolaterally in the cord via the spinothalamic (also known
CONTINUUMJOURNAL.COM 15
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
FIGURE 1-3
Cross-sectional anatomy of the principal white matter tracts of the spinal cord.
Reprinted with permission from Cho TA, Continuum (Minneap Minn).3 © 2015 American
Academy of Neurology.
as the anterolateral) tracts (FIGURE 1-3).3 This information is referred to the
contralateral thalamus of the brain as the sensory nerve roots entering via the two
dorsal horns synapse with second-order neurons. The axons of the second-order
neurons ascend for two to three vertebral segments above where they enter the
cord and then decussate across the midline. Proprioception, vibration, and touch
are carried in the dorsal columns of the cord to the ipsilateral dorsal column
nuclei of the medulla. The parts of the dorsal columns transmitting information
from the lower limbs are referred to as gracile and those from the upper limbs are
referred to as cuneate.
The spinocerebellar tracts (dorsal and ventral) are ipsilateral to the cerebellum
and run laterally in the cord, transmitting proprioceptive information from
muscles, tendons, and joints of the lower limbs. Cerebellar information from the
upper limbs is conveyed by tracts arising from the external cuneate nucleus of
the caudal medulla. White matter tracts are also involved in the transmission of
information related to autonomic nervous system control of bowel and bladder
function and reflexes.
The spinal cord also has the capacity to produce a motor response that is
independent of the brain when triggered by external stimuli by way of spinal
reflexes.6 The components of the monosynaptic spinal reflex arc include primary
sensory afferents arising from peripheral stretch receptors synapsing directly in
the spinal cord on alpha motor neurons that make up the efferent pathway to a
muscle and therefore mediate a final motor response. The classic example in clinical
practice is the patellar reflex, which occurs when stretch receptors in the patellar
tendon are activated by the tendon hammer of a clinician causing reflex contraction
of the quadriceps femoris muscle by way of a monosynaptic spinal reflex. More
complex polysynaptic reflexes involving an integrated response to sensory input
across multiple spinal segments to produce a motor response also occur as a result of
spinal interneurons between afferent and efferent pathways. A polysynaptic reflex
underlies the startle response to an unexpected touch to the trunk or limbs.
16 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Vascular Supply of the Spinal Cord KEY POINTS
The vascular supply of the spinal cord has clinical importance. The anterior spinal
● The monosynaptic spinal
artery runs ventrally along the length of the cord and supplies blood to the reflex is caused by
anterior two-thirds of the spinal cord (including the corticospinal tracts), with activation of peripheral
the remaining dorsal one-third of the spinal cord (including the dorsal columns) stretch receptors
supplied by the paired posterior spinal arteries. All three of these arteries emerge transmitting an impulse
along primary sensory
as branches of the vertebral arteries at the cervical-cranial junction, but some of
afferents that synapse
their blood supply also comes from the thyrocervical trunk via the cervical directly on alpha motor
arteries. Separate radiculomedullary arteries also arise from the thyrocervical neurons, causing a final
trunk to supply the cervical spinal cord sequentially at the different levels at efferent motor response.
which they enter the vertebral canal. More caudal radiculomedullary arteries
● The artery of
emerge directly from the aorta to supply the thoracolumbar cord. The Adamkiewicz is the large
radiculomedullary artery that anastomotically supplies the anterior spinal artery radiculomedullary artery
between T9 and T12 in most individuals is the great anterior radiculomedullary that supplies the anterior
artery, or artery of Adamkiewicz (FIGURE 1-47).8 The artery of Adamkiewicz is spinal artery between T9
and T12 in most individuals.
responsible for supplying blood to the anterior cord from its point of entry in the
lower thoracic cord down to the conus medullaris. ● The somatotopic
The venous drainage of the spinal cord is from the dorsal spinal and ventral organization of the spinal
spinal veins into the internal and external venous plexus adjacent to the dural sac cord allows determination
of the approximate or, in
and vertebral bodies. From there, venous blood is transported to the dural venous
some cases, precise level of
sinuses.9 a spinal cord lesion.
IMPORTANCE OF THE CLINICAL HISTORY
Whether neurologic symptoms are the result of a myelopathy or brain or
peripheral nervous system pathology and the precise location of the lesion in the
cord can often be determined by an accurate history and examination combined
with knowledge of the somatotopic and segmental anatomy of the spinal cord
(TABLE 1-1).10 Clues to a spinal cord lesion in the history include bilateral sensory
FIGURE 1-4
The arterial supply of the spinal cord.
Reprinted with permission from Martirosyan NL, et al, J Neurosurg Spine.7 © 2011 Nicholas Theodore, MD.
CONTINUUMJOURNAL.COM 17
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
and/or motor symptoms in the limbs, particularly if concomitant sphincter
disturbance is present. Patients may report stiffness in the legs or sustained
(tonic) or rhythmic (clonic) spasm. Other clues include a history of neck or back
pain associated with neurologic symptoms when there is extrinsic compression
on the cord, such as due to a cervical or thoracic vertebral metastasis, but
intrinsic spinal cord pathology typically does not have associated neck or spine
pain. Bladder symptoms, sensory symptoms, and pain that precede the
development of weakness favor an extrinsic (compressive) myelopathy over an
intrinsic cord lesion. Particular care should be taken in patients with a history of
known metastatic cancer or risk factors for cancer (eg, cigarette smoking) that
may suggest myelopathy due to evolving metastatic spinal cord compression,
which is a neurologic emergency.
The Uhthoff phenomenon occurs when patients with a demyelinating disease
(such as multiple sclerosis [MS]) develop a recrudescence of symptoms
attributable to a CNS demyelinating lesion with an increase in body temperature,
such as when febrile, during exercise, or when ambient temperatures are hot (eg,
in the shower). Other features that may be present include a feeling as if a tight
TABLE 1-1 Clues to a Spinal Cord Lesion From the History
General symptoms
◆ Bilateral greater than unilateral sensory and/or motor symptoms
◆ Bladder, bowel, and/or sexual dysfunction
◆ Stiffness in the legs
◆ Neck and/or back pain in association with neurologic symptoms, particularly if the patient
had preceding trauma or if pain is exacerbated by neck flexion or extension
◆ Lhermitte or Uhthoff phenomenon
◆ Sensory level across the trunk (often more reliable as a symptom than a sign)
◆ Tight band around the trunk or torso
◆ Neurogenic claudication (suggests cauda equina pathology rather than a lower cord lesion)
◆ Sensory ataxia (can also occur with peripheral nervous system disorders)
◆ Dyspnea when lying flat (C3-C5 lesion)
Time course of symptoms
◆ Acute
◇ Trauma
◇ Vascular (infarction, hemorrhage)
◆ Subacute
◇ Demyelination
◇ Space-occupying lesion (eg, epidural abscess)
◆ Chronic or progressive
◇ Primary or secondary progressive multiple sclerosis
◇ Hereditary spastic paraparesis
◇ Motor neuron disease (amyotrophic lateral sclerosis, primary lateral sclerosis)
18 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
band is around the chest or torso. When this is present in patients with MS, it is KEY POINTS
commonly referred to as the MS hug.
● The Uhthoff phenomenon
A careful history is also vital in trying to establish the level of the lesion in the commonly occurs when
spinal cord. Cervical cord lesions tend to affect the upper limbs but can affect all patients with multiple
four limbs or, more rarely, just the lower limbs. When present, the Lhermitte sclerosis experience an
phenomenon (defined as an electrical pain or tingling brought on by neck flexion exacerbation of symptoms
with an increase in body
that runs from the neck down the back and sometimes into the arms or legs) is
temperature.
a clue to cervical myelopathy most commonly due to a demyelinating lesion, but
it may be encountered with other etiologies, including cervical spondylotic ● Spinal injury can lead to
myelopathy. Cervical cord lesions can disrupt the origin of the phrenic nerves either a flaccid or spastic
and cause diaphragmatic paralysis, hence the medical school mnemonic “C3, 4, 5 bladder, with a range of
symptoms, including urinary
keeps the diaphragm alive.” Patients with diaphragmatic paralysis typically frequency, urgency,
report dyspnea when lying flat, but severe cervical cord injury can result in incontinence, and urinary
respiratory failure11 and severe autonomic dysfunction (refer to the section retention due to a lack of
Spinal Shock Versus Neurogenic Shock). Thoracic lesions typically cause sensory coordination between the
detrusor muscle of the
and/or motor symptoms in the lower limbs. bladder and the urinary
Painful cramping or weakness in the legs that presents after walking a set sphincter.
distance and improves with rest (neurogenic claudication) is a feature of
clinically significant lumbar spinal canal stenosis causing intermittent ● The patient’s previous
medical history and the
compression of cauda equina nerve roots; patients may report doing better when
temporal onset of
the spine is in flexion, which widens the lumbar canal (eg, when bent forward neurologic symptoms can be
leaning over a shopping cart).10 Sensory ataxia is less specific to spinal cord used to narrow the
pathology but is nevertheless a common manifestation of cord disease caused by differential diagnosis of a
spinal cord lesion.
dorsal column dysfunction and can arise from cervical, thoracic, or even lumbar
cord or cauda equina lesions.
Ascending numbness with preserved (or increased) reflexes is usually
secondary to myelopathy (most often sensory myelitis of MS) but is frequently
mistaken for peripheral nervous system involvement. Indeed, if a patient
mentions altered sensation or numbness from a particular level on the trunk that
extends downward (often noticed in the shower or when swimming), it is a clue
to a spinal sensory level.
Bladder and bowel dysfunction can also relate to lesions in the cervical,
thoracic, or lumbar cord; conus medullaris; or cauda equina. Sphincter
disturbance arises because normal voluntary voiding of the bowel and bladder
relies on afferent feedback of a sense of fullness in these organs via the spinal
cord to the brain. When this feedback is interrupted, a neurogenic bowel and
bladder can develop. Spinal injury can lead to either a flaccid or spastic bladder,
with a range of symptoms, including urinary frequency, urgency, incontinence,
and urinary retention due to lack of coordination between the detrusor muscle of
the bladder (which contracts during normal micturition) and the urinary
sphincter (which relaxes during normal micturition).12 Similarly, bowel
dysfunction from spinal cord injury can lead to constipation or fecal urgency and
incontinence with a dilated anal sphincter. Male and female sexual dysfunction
often accompanies neurogenic bowel and bladder symptoms and commonly
manifests as erectile dysfunction, retrograde ejaculation, and anorgasmia in
males and vaginal dryness and anorgasmia in females.12
The demographic profile of the patient and a detailed history can also help to
generate a relevant differential diagnosis list. Older patients are more likely to
experience a spinal cord infarct than younger patients, and MS is 3 times more
common in females than males.13 A history of trauma raises the possibility of a
CONTINUUMJOURNAL.COM 19
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
compressive myelopathy; therefore, a history of trauma to the neck or back
preceding neurologic symptoms should always prompt consideration of spinal
cord injury either directly (traumatic myelopathy) or indirectly (eg, spinal cord
watershed infarction secondary to vertebral artery dissection).
The time course of myelopathic symptoms is also informative. Acute
symptoms suggest trauma or a vascular cause, such as infarction or hemorrhage;
subacute symptoms may suggest demyelination or an extrinsic compressive
cause (eg, epidural abscess); and an insidious onset with chronic progression
could indicate a progressive form of MS, hereditary spastic paraparesis, or
primary lateral sclerosis.14 Relapsing symptoms could indicate MS or other
TABLE 1-2 Clues to a Spinal Cord Lesion From the Examination
Upper motor neuron signs
◆ Spasticity
◆ Hyperreflexia (including Hoffman sign and crossed adductor response)
◆ Clonus
◆ Pyramidal weakness
◆ Upgoing (extensor) plantar response
Paraparesis or quadriparesis
Inverted biceps or brachioradialis/supinator reflex
◆ Testing of the biceps or brachioradialis/supinator reflex (C5-C6) may lead to finger flexion
instead of flexion of the elbow from loss of the biceps jerk (C5-C6) or brachioradialis (C5-C6)
and spread to the finger flexors (C8); suggests a lesion at C5-C6 (lower motor neuron damage
at the lesion and upper motor neuron damage below)
Involvement of multiple contiguous dermatomes
Absent abdominal reflexes (not always reliable)
Gait disturbance
◆ Stiff legs
◆ Circumduction
◆ Scissoring
◆ Sensory ataxia with positive Romberg sign (can also occur with peripheral nervous system
disease)
Spinal shock or neurogenic shock
Spinal cord syndrome
◆ Posterior cord syndrome
◆ Central cord syndrome
◆ Anterior cord syndrome
◆ Brown-Séquard syndrome
◆ Transverse (complete or partial) myelitis
◆ Cauda equina syndrome
◆ Conus medullaris syndrome
20 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
inflammatory demyelinating disorders, such as aquaporin-4 IgG–seropositive KEY POINT
neuromyelitis optica spectrum disorder (NMOSD) or myelin oligodendrocyte
● The likelihood of upper
glycoprotein (MOG) IgG–associated demyelination.15 motor neuron pathology is
Purely motor symptoms might indicate spinal cord infarction, particularly increased if hyperreflexia
if acute in onset, with a common etiology being embolization from the occurs accompanied by
artery of Adamkiewicz to the anterior spinal artery affecting the ventral other upper motor neuron
signs, such as an extensor
corticospinal tracts in the thoracic spine at a point usually between T9 and T12.
plantar response or
Unsteadiness when the eyes are closed (eg, in the shower) is highly suggestive pyramidal weakness, or
of dorsal column pathology such as from subacute combined degeneration both.
of the spinal cord due to vitamin B12 deficiency or copper deficiency. Fever in
the context of neurologic symptoms referable to the spinal cord should
initiate investigations for diskitis, spinal epidural abscess, or vertebral
osteomyelitis, particularly if the patient has a history of systemic infection
(eg, endocarditis) or is an IV drug user.
CLINICAL EXAMINATION FINDINGS
The neurologic examination is essential for lesion localization in a patient with
a suspected myelopathy (TABLE 1-2).10 Typically, patients will have upper motor
neuron signs, such as spasticity, hyperreflexia, and clonus, or pyramidal
weakness characterized by weakness of shoulder abduction, elbow extension,
wrist extension, and finger extension and the interossei in the upper limbs.
Patients may also have weakness of hip flexion, knee flexion, and ankle
dorsiflexion in the lower limbs. Upper motor neuron signs develop consequent to
loss of descending inhibitory pathways in the spinal cord, leading to
hyperexcitability.16 It is not uncommon to see young patients with
hyperreflexia and nonsustained clonus without significant neurologic
pathology, so these signs cannot always be relied upon as indicators of CNS
disease; however, the likelihood of upper motor neuron pathology is increased
if hyperreflexia occurs in the company of other upper motor neuron signs,
such as an extensor plantar response or pyramidal weakness, or both.
Occasionally, patients with spinal cord pathology will have a normal clinical
examination (eg, asymptomatic spinal cord lesions in MS).
The reflexes most often assessed in the neurologic examination are the biceps
jerks, triceps jerks, and supinator (brachioradialis) reflexes in the upper limbs
and knee jerks, ankle jerks, and plantar responses in the lower limbs.17 Reflexes
are graded as 0 or absent, 1+ when present but reduced, 2+ when normal,
3+ when brisker or more exaggerated than normal (hyperreflexia), and 4+ when
hyperreflexia is accompanied by clonus. Clonus is a rhythmic involuntary
movement most often elicited at the ankle, where a sudden sharp dorsiflexion of
the ankle by the examiner results in rhythmic plantar flexion of the foot.16 Clonus
may fatigue after a few beats (nonsustained) or occur indefinitely (sustained),
with the latter usually indicating a more significant CNS insult.
Other reflexes can also be checked and are often helpful in providing further
information if doubt exists regarding hyperreflexia, including deltoid and pectoral
reflexes and finger jerks in the upper limbs and adductor reflexes in the lower
limbs. A positive Hoffman sign (or reflex) occurs when the tip of the middle finger
is flicked downward, causing the thumb of the hand to flex and adduct; this can
indicate a cervical myelopathy.18 Spread of reflexes into the fingers may cause the
fingers to flex when the biceps jerk or supinator reflex is being elicited in the
setting of hyperactive finger flexors. An inverted brachioradialis/supinator reflex
CONTINUUMJOURNAL.COM 21
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
(C5, C6) occurs when an attempt to elicit the biceps jerk leads to flexion of the
fingers rather than elbow flexion because of a lesion at the C5 and/or C6 level.
Injury to the C5 and/or C6 nerve root leads to an absent brachioradialis jerk
(ie, no elbow flexion or supination), and spinal cord damage below that level leads
to hyperactivity of the finger flexor (C8) jerks and finger flexion from spread
when the adjacent brachioradialis tendon is struck.19 An inverted biceps reflex can
similarly occur from a lesion at this location when loss of the biceps jerk is
associated with spread to the hyperactive triceps, causing elbow extension rather
than the expected flexion. Cervical spondylosis is the most common etiology of
these inverted reflexes in the upper limb. The presence of a crossed adductor reflex
(contraction of both hip adductors when testing a reflex at the ipsilateral knee)
from either or both lower limbs is considered an upper motor neuron sign.
Superficial abdominal reflexes are cutaneous reflexes that can be tested in
the four quadrants of the abdomen by stroking the skin (eg, with an orange stick)
in the direction of the umbilicus, which causes reflex contractions of the
abdominal wall. The upper abdominal reflexes are supplied by T9 through T11
and the lower reflexes by T11 and T12. The superficial abdominal reflexes are
absent when a spinal cord lesion above the segmental level is present, but their
clinical relevance is limited as it can be difficult to elicit abdominal reflexes in
patients who are obese, have undergone abdominal surgery, are pregnant, or are
elderly, and they may be absent in 15% of healthy individuals.20 The Beevor sign,
which is also nonspecific, refers to upward displacement of the umbilicus when
the neck is flexed on getting up from a reclining position; it occurs because of
relative weakness of the lower abdominal muscles compared to the upper
abdominal muscles.21 The Beevor sign can indicate a thoracic cord lesion between
T10 and T12 but is also seen in fascioscapulohumeral muscular dystrophy.
An extensor plantar response (positive Babinski reflex) is a major clue,
particularly if bilateral, as it suggests involvement of the corticospinal tracts in
the spinal cord, whereas an isolated unilateral extensor plantar response could be
caused by either ipsilateral cord or contralateral brain pathology. The plantar
response is elicited by gently scraping along the lateral border of the foot and
then across the ball of the foot to the middle metatarsophalangeal joint; it is
considered abnormal in adult patients when extension (rather than flexion) of
the great toe is seen, with or without fanning of the other toes.22 It is worth
mentioning that spinal cord pathology can still be present even with a flexor
plantar response, so the sign is more helpful in localizing cord pathology when
extensor rather than when flexor.
A dermatome is the area of skin supplied by the sensory nerve root of a single
spinal segment (FIGURE 1-5).23 Knowledge of the dermatomes can help the
clinician establish the level of a lesion involving sensation in the nervous system.
If a spinal cord lesion is suspected, a dedicated search to try to determine the
spinal sensory level of the lesion should be conducted, including over the anterior
and posterior trunk.10 Anatomic landmarks, such as the position of the nipples
(which correspond to approximately the T4 dermatomal level) and the umbilicus
(which corresponds to the T10 level), can greatly assist the clinician. Light touch,
pinprick, and temperature sensation can all be tested over the trunk anteriorly or
posteriorly. It is worth remembering that the C4 dermatome abuts the T2
dermatome on the chest. A spinal cord lesion affecting the spinothalamic tract(s)
may cause anesthesia below the lesion. The most caudal dermatome of normal
pain and temperature sensation on the trunk (truncal sensory level) occurs two
22 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
to three vertebral segments below KEY POINTS
the level of the actual lesion in
● The C4 dermatome abuts
the spinal cord because the the T2 dermatome on the
spinothalamic tracts ascend as chest.
they decussate. This anatomic
arrangement means that a lesion ● A truncal sensory level is
defined as the highest
affecting the spinothalamic tract
dermatomal area of normal
of the right hemicord only will sensation to pinprick and
cause impaired temperature and temperature on the trunk.
pinprick sensation on the left
trunk and lower limb below the ● A lesion affecting the
spinothalamic tract of the
level of the cord lesion. A sensory right hemicord only will
level is most reliable if the patient cause impaired temperature
has described altered sensation at and pinprick sensation on
that level during the history. the left trunk and lower limb
two to three vertebral levels
Involvement of multiple below the level of the cord
contiguous dermatomes tends to lesion because the
favor spinal cord pathology over spinothalamic tracts ascend
radiculopathy, particularly if it as they decussate.
occurs in the context of other
● The term paresis is used
upper motor neuron signs. A to denote weakness,
spinal motor level can be whereas plegia is used to
determined by ascertaining which denote absence of any
muscles are affected by weakness voluntary movement.
FIGURE 1-5 and relating that to knowledge of
The human dermatomes. Evidence-based the myotomes, which are defined
dermatome map representing the most
consistent tactile dermatomal areas for each
as the group of muscles innervated
spinal dorsal nerve root found in most individuals, by a single spinal nerve.
based on the best available evidence. The Patients with significant spinal
dermatomal areas shown are not autonomous cord pathology will often have an
zones of cutaneous sensory innervation since,
abnormal gait. As in other parts
except in the midline where overlap is minimal,
adjacent dermatomes overlap to a large and of the examination, the location
variable extent. Blank regions indicate areas of of the lesion determines the way
major variability and overlap. in which the gait will be
Modified with permission from Lee MWL, et al, Clin
23
Anat. © 2008 Wiley-Liss, Inc.
abnormal. Spasticity is usually
present and is defined clinically
as a velocity-dependent increase
in normal resting muscle tone arising from upper motor neuron pathology.16 The
term paresis is used to denote weakness, whereas plegia is used to denote absence
of any voluntary movement. Patients with a lesion involving the bilateral
corticospinal tracts may be paraplegic (no voluntary movement in either leg) or
quadriplegic/tetraplegic (have no movement in any of their four extremities)
with severe cervical cord lesions. Patients with spinal cord disease may have a
spastic paraparesis (with weakness but some preserved voluntary movement)
and an accompanying spastic gait with a tendency for the legs to veer laterally
from the midline during each stride (circumduction); they may also exhibit
scissoring, in which the feet cross in front of each other during walking.19 A
spastic monoparesis (weakness but some preserved voluntary movement) can
occur when patients have unilateral corticospinal tract pathology, but
contralateral pathology in the brain also should be considered.
CONTINUUMJOURNAL.COM 23
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
Lesions involving afferent pathways in the cord, particularly the dorsal
columns, give rise to a sensory ataxia; a positive Romberg sign (marked
unsteadiness when standing with the feet together and the eyes closed) and
pseudoathetosis (involuntary writhing movements more pronounced with eyes
closed from loss of joint position sensation in the hands) may be seen.19
A coexistent stocking-glove peripheral neuropathy causing lower motor
neuron signs (hyporeflexia or areflexia, wasting, fasciculations, hypotonia) can
mask the upper motor neuron signs of a spinal cord lesion, so it may be
appropriate to image the spinal cord in selected patients if a clinical possibility of
a myelopathy exists, despite an absence of upper motor neuron signs.
SPINAL SHOCK VERSUS NEUROGENIC SHOCK
Spinal shock occurs when hyperacute or acute injury (particularly trauma) to the
spinal cord results in flaccid areflexia below the level of the lesion, and the
absence of upper motor neuron signs can lead to diagnostic confusion. The signs
of spinal shock may last from days to weeks. Neurogenic shock occurs in acute
trauma or occasionally in acute nontraumatic myelopathies above the level of T6,
which leads to loss of sympathetic tone below the lesion causing hypotension and
unopposed vagal activity leading to bradycardia.24 The hypotension may require
IV fluids, inotropes, and vasopressors or combinations thereof, whereas the
bradycardia may require atropine or temporary pacing.
AUTONOMIC DYSREFLEXIA
Autonomic dysreflexia occurs when patients have injury above T6, leading to an
exaggerated sympathetic nervous system response to sensory stimuli (eg, urinary
retention, urinary tract infection, or constipation) below the level of injury. A
reflex response causes a strong sympathetic response, leading to constriction of
splanchnic blood vessels and arterial hypertension. Carotid baroreceptors
trigger descending inhibitory signals to reduce sympathetic tone via the spinal
cord, but a signal cannot reach most sympathetic outflow levels because of the
cord lesion at or above T6. A further compensatory parasympathetic vagal
response tries to reduce blood pressure by lowering the heart rate. In addition to
hypertension and bradycardia, the excessive sympathetic tone below the lesion
results in pale cool extremities with piloerection. Above the lesion, the
parasympathetic activity results in pupil constriction, flushing, and sweating.
Autonomic dysreflexia is managed by treating the offending stimulus.
SPINAL CORD SYNDROMES
Spinal cord syndromes are classic examination findings that can suggest the site
or nature of a spinal cord lesion. (TABLE 1-2) (FIGURE 1-625).26
Central Cord Syndrome
A central cord syndrome usually occurs as a result of a neck hyperextension
cervical spinal cord injury, leading to damage to medial structures in the cord.
A characteristic pattern of distal greater than proximal weakness in the upper
limbs (predominantly the hands from damage to the anterior horn cells at that
level) ensues, and the upper limbs are more affected than the lower limbs. The
upper motor neuron pathology can lead to bladder dysfunction and priapism (in
males). Classically, a capelike area of sensory loss to pain and temperature occurs
over the upper trunk and arms at the level of the lesion as the decussating
24 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
spinothalamic tract fibers are KEY POINTS
affected; this is called a
● Spinal shock occurs when
suspended sensory level because hyperacute or acute injury
the sensory loss is “suspended” (particularly trauma) to the
or “hangs” on the trunk without spinal cord results in flaccid
involving the sacrum or lower areflexia below the level of
the lesion.
limbs.27 This is often seen with a
central cord lesion due to ● Neurogenic shock occurs
syringomyelia (CASE 1-1). A due to acute pathology
patchy loss of pain, temperature, above the level of T6, which
and light touch can be seen leads to loss of sympathetic
tone below the lesion
below the level of the lesion. causing hypotension and
Relative preservation of sacral unopposed vagal activity
and lower limb sensation occurs leading to bradycardia.
because the lower extremity
● Autonomic dysreflexia
spinothalamic tracts run more occurs when patients have
laterally than those of the upper injury above the T6 level,
extremities and so are not leading to an exaggerated
affected early. This finding can sympathetic nervous system
response to sensory stimuli
also be helpful in distinguishing
below the level of the lesion
FIGURE 1-6
an intraaxial lesion (within the (eg, bladder filling).
Spinal cord syndromes occurring from lesions cord) from an extraaxial lesion
above the conus medullaris. Paraplegia arises (intradural or extradural). ● A central intraaxial spinal
from lesions of the thoracic cord affecting motor Impairment of spinothalamic cord lesion often causes
pathways, and tetraplegia arises from similar sensory symptoms and signs
lesions of the cervical cord. When transverse
sensation without involvement of in the upper limbs and trunk
myelopathy or transection of the cord occurs, dorsal column sensation, as seen before the lower limbs and
sensation below the level of the lesion is also in this syndrome, is an example of sacral regions (called a
affected. For simplicity, the other spinal cord dissociated sensory loss. suspended sensory level).
syndromes are depicted as resulting from a This is because the lower
cervical cord lesion. extremity spinothalamic
Anterior Cord Syndrome
Reprinted with permission from O’Phelan K, De Jesus I.25 tracts run more laterally
© 2019 Cambridge University Press. In an anterior cord syndrome, than those of the upper
damage to the ventral cord extremities and so take
longer to be affected by an
results in motor weakness and, expanding central cord
often, loss of pain and temperature sensation below the level of the lesion. lesion.
Proprioception and vibration are preserved as the dorsal columns run posteriorly
in the cord. Anterior cord syndromes classically occur with anterior spinal artery
infarction, which is recognized as an iatrogenic complication resulting from cross
clamping of the aorta intraoperatively.
Posterior Cord Syndrome
A posterior cord syndrome occurs when pathology of one or both dorsal columns
of the spinal cord is present. The prototypic cause is vitamin B12 deficiency,
leading to subacute combined degeneration of the cord in which the lateral
columns are also involved concurrently. Patients may present with sensory ataxia
and have proprioceptive deficits on examination as well as impaired appreciation
of vibration. In the case of vitamin B12 deficiency, peripheral neuropathy,
cognitive deficits, and megaloblastic anemia may also be seen. Other causes of
posterior cord syndromes in the absence of a mass lesion or extrinsic compression
on MRI include nitrous oxide abuse (causing vitamin B12 deficiency), neurosyphilis,
MS, and copper deficiency. For more information on the effects of vitamin
CONTINUUMJOURNAL.COM 25
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
deficiencies and nitrous oxide use, refer to the article “Metabolic and Toxic
Myelopathies” by Natalie Elizabeth Parks, MD,28 in this issue of Continuum.
Brown-Séquard Syndrome
Brown-Séquard syndrome refers to ipsilateral upper motor neuron motor
weakness in one lower limb (and rarely proprioceptive loss) with spinothalamic
pain and temperature loss in the contralateral lower limb. It is caused by a lesion
that involves the lateral half of the cord, affecting the corticospinal,
spinothalamic, and, sometimes, proprioceptive tracts on that side. Patients will
have a truncal sensory level to pain and temperature on the contralateral side of
the lesion two or three segments below the level of the lesion. Causes include MS,
unilateral cord compression due to spinal degenerative disease, or
hemitransection of the cord due to a knife injury or other trauma.
CASE 1-1 A 50-year-old woman presented with a 13-day history of sensory
disturbance in the upper limbs, pain in the shoulders, and weakness in the
hands following a flulike illness. She had no relevant past medical history.
Examination revealed mild weakness and wasting of the intrinsic
muscle of the hands, with impaired temperature and pain sensation
throughout the upper limbs and upper trunk in a capelike distribution.
Upper limb reflexes were reduced. Lower limb motor and sensory
examination was normal, and sacral function was intact. Lower limb
reflexes were normal. Plantar responses were downgoing.
Routine blood tests and nerve conduction studies were normal. MRI of
the cervical spine (FIGURE 1-7) showed slight descent of the cerebellar
tonsils into the foramen magnum, with a cervical cord syrinx extending
from C4 to T2. She underwent foramen magnum decompression surgery
that resulted in improvement in her symptoms.
COMMENT The differential diagnosis in this patient included an acquired
demyelinating peripheral neuropathy such as Guillain-Barré syndrome
because of the red herring of the flulike illness, distal sensory and motor
symptoms, and reduced reflexes, at least in the upper limbs, but the
wasting of the intrinsic muscles of the hands suggested a more chronic
process. The downgoing plantar responses did not immediately implicate
spinal cord pathology but the key was the capelike distribution of pain and
temperature loss in the upper trunk, which would not be present in chronic
inflammatory demyelinating polyradiculoneuropathy (CIDP) and was more
in keeping with a central cord syndrome. Bilateral involvement of the upper
limbs and sparing of the lower limbs with sphincter preservation favored
an intrinsic rather than an extrinsic cord lesion (keeping in mind that
compressive myelopathies affecting the central cord can sometimes
present with this pattern) and helped to localize the lesion to the cervical
cord. The wasting in the hands and reduced reflexes in the upper limbs are
not upper motor neuron signs but likely occurred in this case as a result of
the large syrinx chronically impinging on the anterior horn cells.
26 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Transverse Myelitis
The term transverse myelitis can result in confusion as by definition it should
involve the entire transverse diameter of the spinal cord, yet it is often stratified
clinically into complete and partial forms. A partial transverse myelitis (typically
encountered in MS) refers to spinal cord inflammation in which symptoms
and signs occur that are attributable to only a portion of the cord axially rather
than involving the entire transverse diameter. A complete transverse myelitis
(typically encountered with aquaporin-4 IgG–seropositive NMOSD) is
attributable to spinal cord inflammation involving its entire cross section, usually
resulting in severe bilateral sensory and motor dysfunction. Transverse myelitis
also can be defined radiologically by the length of the T2-hyperintense lesion on
sagittal sequences, which is probably more useful diagnostically than the clinical
definition. Involvement may either affect a short segment of the cord (fewer
FIGURE 1-7
Imaging of the patient in CASE 1-1, who presented with a central cord syndrome due to
cervical syringomyelia. A, Sagittal T2-weighted MRI of the cervical spine shows cerebellar
ectopia at the level of the foramen magnum (arrowhead ) with a T2-hyperintense lesion of
similar signal intensity to CSF in the central cord from C4 to T2 (arrows), consistent with a
syrinx. B, Axial T2-weighted MRI confirms that the syrinx involves the central cord. C,
Sagittal T2-weighted MRI of the cervical spine after foramen magnum decompression
shows significant improvement in the caliber of the syrinx.
CONTINUUMJOURNAL.COM 27
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPINAL CORD ANATOMY AND LOCALIZATION
KEY POINTS than three vertebral segments in length) on sagittal images, which is typical of
MS, or may be longitudinally extensive (extending three or more vertebral
● A partial transverse
myelitis refers to spinal cord
segments in length), which is characteristic of aquaporin-4 IgG–seropositive
inflammation in which NMOSD.13,15 A variety of causes of transverse myelitis exist. Some have argued
symptoms and signs occur for a new classification of spinal cord inflammatory disorders that removes the
that are attributable to only term transverse from its definition as a large proportion of inflammatory
a portion of the spinal cord
myelopathies do not involve the entire transverse dimension of the spinal cord.
in cross section rather than
involving the entire For more information on transverse myelitis, refer to the article “Myelitis and
transverse diameter. A Other Autoimmune Myelopathies” by Sebastian Lopez Chiriboga, MD, and
complete transverse Eoin P. Flanagan, MBBCh,29 in this issue of Continuum.
myelitis is attributable to
spinal cord inflammation Cauda Equina Syndrome
involving its entire cross
section. Cauda equina syndrome refers to distal greater than proximal weakness and
sensory disturbance in the lower limbs accompanied by impairment of sphincter
● Patients with a control, including weakness of the anal sphincter, with areflexia of the ankle
longitudinally extensive jerks but preserved knee jerks. Patients may report saddle anesthesia. The most
transverse myelitis should
be tested for aquaporin-4
common cause is compression of the cauda equina by a structural lesion, such as
IgG and myelin a prolapsed lumbosacral disk or tumor, but the syndrome can occur due to
oligodendrocyte infiltration of the cauda equina by neoplasm or involvement by infection or
glycoprotein IgG. granulomatous disease. For more information on cauda equina syndrome, refer
to the article “Disorders of the Cauda Equina” by Samantha LoRusso, MD,30 in
this issue of Continuum.
Conus Medullaris Syndrome
The upper level of the conus medullaris is not well defined. Although the
corresponding spinal cord segments of the conus medullaris are typically from S1
through S5, the classic conus medullaris syndrome usually encompasses lesions of
the cord as rostral as L2; therefore, the clinical picture is of varying degrees of
mixed upper and lower motor neuron signs in both lower limbs. The patient may
report back pain, and the examination may reveal distal greater than proximal
weakness, brisk knee jerks, and absent ankle jerks, with saddle and lower limb
numbness; bladder, bowel, and sexual dysfunction is particularly common in
these patients.
CONCLUSION
When a patient reports neurologic symptoms that are potentially attributable
to the spinal cord or cauda equina, a careful history and examination may
provide numerous clinical clues that, together with a thorough knowledge
of spinal neuroanatomy, can assist with lesion localization and suggest a
differential diagnosis.
REFERENCES
1 Moore KL, Dalley AF, Agur AMR. Clinically 3 Cho TA. Spinal cord functional anatomy.
oriented anatomy. 7th ed. Wolters Kluwer/ Continuum (Minneap Minn) 2015;21(1 Spinal Cord
Lippincott Williams & Wilkins Health, 2014: xxviii:1134. Disorders):13-35. doi:10.1212/01.
CON.0000461082.25876.4a
2 Bican O, Minagar A, Pruitt AA. The spinal cord: a
review of functional neuroanatomy. Neurol Clin
2013;31(1):1-18. doi:10.1016/j.ncl.2012.09.009
28 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
4 Bezov D, Lipton RB, Ashina S. Post-dural puncture 16 Kheder A, Nair KP. Spasticity: pathophysiology,
headache: part I diagnosis, epidemiology, evaluation and management. Pract Neurol 2012;
etiology, and pathophysiology. Headache 2010; 12(5):289-298. doi:10.1136/practneurol-2011-000155
50(7):1144-1152. doi:10.1111/j.1526-4610.2010.01699.x
17 Talley NJ, O'Connor S. Clinical examination: a
5 Lemon RN. Descending pathways in motor systematic guide to physical diagnosis. 3rd ed.
control. Annu Rev Neurosci 2008;31:195-218. MacLennan & Petty, 1996.
doi:10.1146/annurev.neuro.31.060407.125547
18 Fogarty A, Lenza E, Gupta G, et al. A systematic
6 Côté MP, Murray LM, Knikou M. Spinal control of review of the utility of the Hoffmann sign for the
locomotion: individual neurons, their circuits and diagnosis of degenerative cervical myelopathy.
functions. Front Physiol 2018;9:784. doi:10.3389/ Spine (Phila Pa 1976) 2018;43(23):1664-1669.
fphys.2018.00784 doi:10.1097/BRS.0000000000002697
7 Martirosyan NL, Feuerstein JS, Theodore N, et al. 19 Morris JGL. The neurology short case. 2nd ed.
Blood supply and vascular reactivity of the spinal Edward Arnold Publishers Ltd, 2005.
cord under normal and pathological conditions.
20 Dick JP. The deep tendon and the abdominal
J Neurosurg Spine 2011;15(3):238-251.
reflexes. J Neurol Neurosurg Psychiatry 2003;
doi:10.3171/2011.4.SPINE10543
74(2):150-153. doi:10.1136/jnnp.74.2.150
8 Carmichael SW, Gloviczki P. Anatomy of the
21 Pearce JMS. Beevor's sign. Eur Neurol 2005;53(4):
blood supply to the spinal cord: the artery of
208-209. doi:10.1159/000086731
Adamkiewicz revisited. Perspect Vasc Surg
Endovasc Ther 1999;12(1):113-122. 22 Ambesh P, Paliwal VK, Shetty V, Kamholz S. The
doi:10.1177/153100359901200118 Babinski sign: a comprehensive review. J Neurol
Sci 2017;372:477-481. doi:10.1016/j.jns.2016.10.041
9 Rabinstein AA. Vascular myelopathies.
Continuum (Minneap Minn) 2015;21(1 Spinal Cord 23 Lee MWL, McPhee RW, Stringer MD. An
Disorders):67-83. doi:10.1212/01. evidence-based approach to human
CON.0000461085.79241.e0 dermatomes. Clin Anat 2008;21(5):363-373.
doi:10.1002/ca.20636
10 Cho TA, Bhattacharyya S. Approach to
myelopathy. Continuum (Minneap Minn) 2018; 24 Ahuja CS, Wilson JR, Nori S, et al. Traumatic spinal
24(2, Spinal Cord Disorders):386-406. doi:10.1212/ cord injury. Nat Rev Dis Primers 2017;3:17018.
CON.0000000000000583 doi:10.1038/nrdp.2017.18
11 Onders RP, Elmo M, Kaplan C, et al. Long-term 25 O'Phelan K, De Jesus I. Management of the spinal
experience with diaphragm pacing for traumatic cord injury in the neurocritical care unit. In:
spinal cord injury: early implantation should be Torbey MT, ed. Neurocritical care. Cambridge
considered. Surgery 2018;164(4):705-711. University Press, 2019:290-298.
doi:10.1016/j.surg.2018.06.050
26 Kunam VK, Velayudhan V, Chaudhry ZA, et al.
12 Benevento BT, Sipski ML. Neurogenic bladder, Incomplete cord syndromes: clinical and imaging
neurogenic bowel, and sexual dysfunction in review. Radiographics 2018;38(4):1201-1222.
people with spinal cord injury. Phys Ther 2002; doi:10.1148/rg.2018170178
82(6):601-612. doi:10.1093/ptj/82.6.601
27 Clarke C, Frackowiak R, Howard R, et al. The
13 Brownlee WJ, Hardy TA, Fazekas F, Miller DH. language of neurology: symptoms, signs and
Diagnosis of multiple sclerosis: progress and basic investigations. In: Clarke C, Howard R,
challenges. Lancet 2017;389(10076):1336-1346. Rossor M, Shorvon S, editors. Neurology: a queen
doi:10.1016/S0140-6736(16)30959-X square textbook. Wiley-Blackwell, 2009:75-108.
14 Mariano R, Flanagan EP, Weinshenker BG, Palace 28 Parks NE. Metabolic and toxic myelopathies.
J. A practical approach to the diagnosis of spinal Continuum (Minneap Minn) 2021:27(1, Spinal Cord
cord lesions. Pract Neurol 2018;18(3):187-200. Disorders):143-162.
doi:10.1136/practneurol-2017-001845
29 Lopez Chiriboga S, Flanagan EP. Myelitis and
15 Hardy TA, Reddel SW, Barnett MH, et al. Atypical other autoimmune myelopathies. Continuum
inflammatory demyelinating syndromes of the (Minneap Minn) 2021:27(1, Spinal Cord Disorders):
CNS. Lancet Neurol 2016;15(9):967-981. 62-92.
doi:10.1016/S1474-4422(16)30043-6
30 LoRusso S. Disorders of the cauda equina.
Continuum (Minneap Minn) 2021:27(1, Spinal Cord
Disorders):205-224.
CONTINUUMJOURNAL.COM 29
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Spondylotic and Other REVIEW ARTICLE
Structural Myelopathies C O N T I N U UM AUDIO
INTERVIEW AVAILABLE
ONLINE
By Shamik Bhattacharyya, MD, MS
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNo65TEub0G9tZtPaMachiqn on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: This article highlights both common structural causes of
myelopathy, such as spondylotic disease, and infrequent but treatable
causes, such as syringomyelia, spinal cord herniation, arachnoid cyst,
arachnoid band and web, epidural lipomatosis, Hirayama disease, and
arachnoiditis.
RECENT FINDINGS:Neuroimaging improvements and availability have
uncovered many structural abnormalities in the spines and spinal cords of
patients who were asymptomatic or minimally symptomatic. Recent
published clinical series have improved our knowledge of the natural
history of structural abnormalities and the risks of intervention versus
conservative management.
SUMMARY: Myelopathy from a suspected structural cause is a common
reason for neurologic consultation. Correlation between the history, CITE AS:
examination, and imaging are especially important to determine whether CONTINUUM (MINNEAP MINN)
2020;27(1, SPINAL CORD DISORDERS):
intervention is necessary or conservative management is the best option. 163–184.
Address correspondence to
Dr Shamik Bhattacharyya,
INTRODUCTION Brigham and Women’s Hospital,
S
tructural causes of myelopathy are important to diagnose early and Department of Neurology,
75 Francis Rd, Boston, MA 02115,
accurately because symptoms can often be improved or at least sbhattacharyya3@bwh.harvard.
arrested with timely intervention. Despite the widespread availability edu.
of imaging, structural etiologies are the leading source of nontraumatic RELATIONSHIP DISCLOSURE:
spinal cord injury.1 On the other hand, most practicing neurologists Dr Bhattacharyya has served as
know of patients who have undergone spinal surgeries with little benefit or were a consultant for Alexion
Pharmaceuticals, Inc and has
worse off after the surgery. Accurate estimates of “unnecessary surgeries” are received personal
hard to come by, but a single-center study showed about 17% of patients compensation for providing
recommended to undergo spinal surgeries were unlikely to benefit from them.2 second opinion service for
Teladoc Health, Inc. Dr
The neurologist has a critical role in assessing the cause of neurologic symptoms, Bhattacharyya receives
prognosis, and risks and benefits of intervention in structural causes of myelopathy. publishing royalties from
Springer and UpToDate, Inc.
CERVICAL SPONDYLOTIC MYELOPATHY UNLABELED USE OF
Cervical spondylotic myelopathy is defined broadly as spinal cord dysfunction PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
caused by degenerative disease of the cervical spine with narrowing of the Dr Bhattacharyya reports no
vertebral canal through which the spinal cord traverses. Because the mechanisms disclosure.
of narrowing of the vertebral canal and injury to the spinal cord are usually
multifactorial, involving bony, soft tissue, and vascular structures, some prefer © 2021 American Academy
to refer to cervical spondylotic myelopathy more generally as degenerative of Neurology.
CONTINUUMJOURNAL.COM 163
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
cervical myelopathy. Accurate estimates of the incidence and prevalence of
cervical spondylotic myelopathy are unavailable. This paucity of data for a
common disease results from lack of accurate coding, lack of definite correlation
between imaging findings and symptoms, lack of accuracy in presurgical
diagnoses (not all who received surgery for cervical spondylotic myelopathy
likely had the disease), and lack of recognition of cervical spondylotic
myelopathy in patients with mild symptoms. With these limitations, an
estimate of the prevalence of cervical spondylotic myelopathy in North America
is 605 per 1 million.3
Pathogenesis
As with many other slowly progressive diseases, the final clinical development of
cervical spondylotic myelopathy is frequently preceded by years of subclinical
changes. Susceptibility factors for clinical disease are congenital spinal stenosis,
osteoarthritis, ossification of the ligamentum flavum and posterior longitudinal
ligament, inflammatory arthritides such as rheumatoid arthritis or ankylosing
spondylitis, Down syndrome, and Klippel-Feil syndrome. In congenital stenosis
of the cervical spine, patients developmentally have a narrow cervical spinal
canal and are predisposed to get cervical spondylotic myelopathy from relatively
minor spinal degenerative disease. Based on large series of cadaveric
measurements, an anterior-posterior cervical spinal canal measurement of 13 mm
or less may define congenital narrowing of the cervical canal (FIGURE 7-1).4
Others have countered that absolute measurement of the spinal canal width is
less important than the relative fraction of space occupied by the spinal cord
compared to the width of the canal itself. This parameter is known as the spinal
cord occupancy ratio, and values greater than 70% may more accurately capture
the concept of a congenitally narrow canal.5 Among different inflammatory
arthritis syndromes, rheumatoid arthritis frequently affects the cervical spine;
MRI of the cervical spine shows
evidence of degenerative disease
in more than 70% of patients
with chronic rheumatoid
arthritis.6 The cause of this
tropism is unclear but may have
to do with the exclusively
synovial joints in the upper
cervical spine.
Klippel-Feil syndrome is
characterized by congenital
fusion of multiple cervical
vertebral bodies, resulting in
spinal instability and propensity
FIGURE 7-1 for injury. Clinically, patients
Congenital spinal stenosis. A, Sagittal
T2-weighted MRI of the cervical spine showing
with Klippel-Feil syndrome have
congenital stenosis. The anterior-posterior decreased neck mobility, a low
distance of the thecal sac averages about 10 mm, posterior hairline, and a short
putting the patient at risk for spondylotic neck. Most patients with
myelopathy from mild degenerative disease. B,
For comparison, sagittal T2-weighted MRI of the
Klippel-Feil syndrome do not
cervical spine of a patient without congenital have all these features, and no
spinal stenosis. single unifying genetic basis for
164 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
this syndrome has been identified (the syndrome is seen as part of other discrete KEY POINTS
genetic disorders).
● Cervical spondylotic
Among nonbony susceptibility factors, ossification of the posterior myelopathy is caused by
longitudinal ligament demonstrates the importance of ligamentous structures in degenerative disease of the
cervical spondylotic myelopathy (FIGURE 7-2). This disorder was traditionally cervical spine resulting in
thought to be more common in Japan, presumably from genetic influence, but narrowing of the spinal
canal.
2016 data show that more than 20% of patients with cervical spondylotic
myelopathy in the United States have posterior longitudinal ligament ossification ● Cervical spondylotic
as well.7 Many patients have questions about the risk of cervical spondylotic myelopathy is
myelopathy from various occupations. Anecdotal reports indicate that workers overdiagnosed in some
experiencing high levels of cervical spine stress, such as those in construction patients (symptoms
misattributed to imaging
who use jackhammers, may be at higher risk. However, definitive data are findings) and missed in
lacking. A small study of grape-growing farmworkers with extension strain others (mild symptoms that
concluded that they have a higher risk of degenerative spine disorder.8 are not investigated).
In spondylotic cervical myelopathy, although narrowing of the spinal canal is
● Congenital narrowing of
always present, the narrowing itself is not enough to cause disease. Clinical the spinal canal is a frequent
symptoms result from a combination of static stenosis, dynamic stress of risk factor for the
movement, and microvascular ischemia. In most cases, the first stage of development of cervical
spondylotic disease is thought to be degenerative disk disease driven by spondylotic myelopathy.
desiccation of the inner layer of the intervertebral disk (nucleus pulposus). Disk
● Patients with Klippel-Feil
degeneration results in increased stress on the bony and ligamentous elements of syndrome clinically have
the cervical spine, which is hypothesized to lead to disk fragment herniation, decreased neck mobility, a
ligament hypertrophy and ossification, misalignment of vertebral bodies, low posterior hairline, and a
osteophyte growth, and uncovertebral joint hypertrophy.3 In most patients, canal short neck; imaging shows
fusion of multiple cervical
stenosis is caused by a combination of these disease processes. vertebral bodies.
Static stenosis alone, however, may not cause myelopathy. This was seen in a
large-scale cervical spine MRI study of more than 1200 asymptomatic subjects.
About 5% had significant spinal cord compression, and 2.3% even had cord signal
changes.9 The importance of other factors was also demonstrated in an animal
study of 14 dogs, in which the spinal canal was experimentally narrowed by
about 29%. In 12 of the 14 dogs,
the onset of clinical myelopathy
was delayed an average of
7 months, after which the animals
developed progressive signs.10 A
proposed mechanism of delayed
injury is microcirculatory
ischemia caused by extension of
the spinal cord over a stenotic
region. This may explain the
predilection for injury of the
anterior horns of the spinal cord,
which are supplied by the
anterior spinal artery and are
near the end arterial zone. Other
mechanisms include
FIGURE 7-2 neuroinflammatory injury
Sagittal CT of the cervical spine showing
ossification of the posterior longitudinal ligament,
induced by chronic
causing spinal stenosis at the C2-C3 and C3-C4 microglia/macrophage
levels (arrows). activation, endothelial cell
CONTINUUMJOURNAL.COM 165
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
dysfunction, and blood–spinal cord barrier disruption.3 The neurobiology of
injury is likely multifactorial, which may explain why significant variability
exists in clinical course, response to therapy, and correlation between imaging
and symptoms.
Clinical Symptoms and Signs
Cervical spondylotic myelopathy can become symptomatic acutely or in a more
chronic fashion. Acute symptoms often follow trauma to the cervical spine in the
background of prior cervical spinal stenosis. Hyperextension injuries, such as
from a car accident, and falls with head injury are frequent triggers for acute
presentations in older patients. In younger patients, high-impact accidents with
fracture of the cervical spine and compression of the spinal cord are a more
common cause. Acute injury of the spinal cord generally causes a central cord
syndrome. In central cord syndrome, patients have more motor weakness in
their arms than in their legs and urinary retention.11 Anatomically, the
corticospinal tract projections that control the arms are located more internally
compared to the projections to the legs; hence, in central cord syndrome, the
arms are affected more significantly. A variable degree of sensory loss is seen
below the level of the lesion. Other myelopathic examination findings, such as
spasticity, hyperreflexia, or upgoing toes, may not be present acutely; these
findings may develop over the space of days to weeks.
A chronic presentation of cervical spondylotic myelopathy is more common.
In contrast to acute central cord syndrome, gait disorder is one of the earliest
symptoms in chronic disease, usually described as a stiff gait with a feeling of
clumsiness and uncertainty. In brief office examinations of very early cases, gait
abnormalities may not be clearly visible. Having the patient walk for an extended
length, such as down the hallway, may elicit subtle stiffness in walking. As the
disease progresses, more symptoms are seen, such as decreased dexterity in the
hands, especially with fine movements such as writing, typing, or opening jars.
Paresthesia in the fingertips is common as well. It is important to note that neck
pain does not correlate with the severity of spinal cord compression. In a clinical
series of cervical spondylotic myelopathy, axial neck pain was only present in
about one-third of patients.12 Axial neck pain is generated by disease of the
musculoskeletal structures, such as the paraspinal muscles, ligaments, and bones,
rather than nerve root or spinal cord compression. Another important clinical
note is that bowel/bladder dysfunction, although typical in central cord
syndrome, is infrequent in slowly progressive cervical spondylotic myelopathy.
Bladder dysfunction is likely present in less than 5% of patients.12 From an
anatomic viewpoint, the autonomic fibers are present in the central areas of the
spinal cord and are likely spared from slow extrinsic compression. Overactive
bladder is a frequent symptom in patients with cervical spondylotic myelopathy,
but its relationship with cord compression is unclear because of lack of consistent
improvement after treatment.13
On neurologic examination, the usual findings are signs of myelopathy,
including weakness in the intrinsic muscles of the hands, spasticity in the legs,
and increased muscle stretch reflexes. If concurrent nerve root compression is
present, findings of cervical radiculopathy might be present as well, causing
mixed lower and upper motor neuron findings. An example is the inverted
brachioradialis also known as the inverted supinator reflex first described by
Joseph Babinski.14 This finding refers to percussion of the brachioradialis muscle
166 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
causing flexion of the fingers (exaggerated reflex at the C8 level) without flexion KEY POINTS
of the elbow (absent reflex at the C5-C6 level).
● Cervical spondylotic
A clear sensory level is usually not seen as is found in other causes of acute myelopathy is likely caused
myelopathy, but decreased sense of vibration and joint position sense in the legs by a combination of canal
are common. In more severe cases, weakness in an upper motor neuron pattern narrowing, stretch of the
can be found, especially in the flexor muscles in the legs. Among the different spinal cord over the stenotic
region, and microvascular
signs of corticospinal injury in patients with mild myelopathy, the Hoffman sign
ischemia.
(involuntary flexion of the thumb after flicking the fingernail of the middle
finger downward) may be more sensitive than the Babinski sign. In a clinical ● Cervical spondylotic
series of 225 surgically treated patients with cervical spondylotic myelopathy, the myelopathy can have acute,
Hoffman sign was present before surgery in 46% of those with mild myelopathy, subacute, and chronic
presentations.
whereas the Babinski sign was present in only 10%.15 In those with more severe
myelopathy, the Hoffman and Babinski signs were both present in more than 80%. ● Acute cord injury from
extension in patients with
Imaging cervical spondylotic
myelopathy causes central
Generally, clinical suspicion for cervical spondylotic myelopathy is followed by cord syndrome in which
imaging. In neurologic clinical practice, the opposite also occurs when patients patients have urinary
are referred for concerning imaging and the goal is to evaluate the clinical retention and greater
significance. MRI is the preferred imaging modality for evaluation of the spinal weakness in their arms than
in their legs.
cord because it can show the parenchyma of the spinal cord, boundaries of the
cord and CSF, and soft tissue structures. In patients for whom MRI is ● Chronic cervical
contraindicated, a CT myelogram can also accurately show the contours of the spondylotic myelopathy
spinal cord and degree of cord compression. However, cord signal abnormalities causes initial symptoms of
cannot be seen by myelography. X-ray of the cervical spine is useful, especially progressive gait disorder.
after prior instrumentation, to assess for displacement of the hardware ● Lack of neck pain does
(FIGURE 7-3). Another use of x-ray imaging is in flexion/extension images. In this not exclude cervical
procedure, an x-ray image is first spondylotic myelopathy.
taken with the neck flexed, and
● Bladder and bowel
then the image is repeated with
sphincter dysfunction are
the neck extended. If significant atypical in chronic
change in the alignment of the progressive cervical
bones is seen, dynamic spondylotic myelopathy.
instability is present; static
● The Babinski sign is not
images obtained in a flat position very sensitive for cervical
may underestimate the degree of spondylotic myelopathy and
dynamic stenosis. In some may be absent in early
centers, flexion and extension disease. The Hoffman sign
may be positive more often.
views of the cervical spine can
also be obtained by MRI and ● MRI of the cervical spine
show ligamentous and bony without contrast is the
instability better than x-ray.16 preferred study to evaluate
for cervical degenerative
When examining an MRI of a
disease.
patient with suspected cervical
spondylotic myelopathy, the ● X-ray of the cervical spine
most important parameters are is useful to evaluate
the degree of stenosis, the nature instrumentation and for
FIGURE 7-3 dynamic instability of bony
of bony or soft tissue changes, structures with flexion and
Sagittal x-ray of the cervical spine showing C4-C5
anterior cervical diskectomy with intervertebral
and cord signal intensity. Having extension of the neck.
disk graft placement and fusion. X-ray imaging can no cervical spinal stenosis
show hardware without significant artifact. essentially excludes the
CONTINUUMJOURNAL.COM 167
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
KEY POINTS possibility of cervical spondylotic myelopathy. However, as discussed before,
even severe cervical spinal stenosis can exist on imaging without corresponding
● The majority of older
adults will have
clinical symptoms. Degenerative changes in the cervical spine of any kind are
degenerative changes of extremely common on imaging. More than 80% of adults over the age of 60 who
the cervical spine on MRI. are asymptomatic have degenerative disk changes.17
How to accurately assess the clinical significance of stenosis on imaging is a
● Categorization as
work in progress. At first pass, a broad categorization is to classify areas of spinal
moderate or severe stenosis
of the cervical spine based canal narrowing as having no stenosis or some narrowing. The degree of
on the degree of CSF narrowing is usually classified further as moderate or severe based on
obliteration has modest T2-weighted images (FIGURE 7-4). In moderate stenosis, some CSF is still present
correlation with clinical around the contours of the spinal cord, whereas in severe stenosis, the CSF rim is
symptoms.
completely effaced. This categorization into moderate or severe stenosis
● Clinical myelopathy from unfortunately does not translate well into clinical symptoms. Some patients with
cervical spinal stenosis can moderate stenosis are symptomatic, whereas others with severe stenosis do not
occur without any T2 cord have any symptoms of myelopathy. Research to improve interpretation of MRI
signal changes.
of the cervical spine to correlate better with clinical symptoms is ongoing. For
● The presence or absence example, the cross-sectional area of the spinal cord at the area of stenosis may
of cord signal hyperintensity correlate better with symptoms than qualitative interpretation of the degree of
does not correlate with obliteration of the subarachnoid space.18 Some of these techniques will likely
outcome after surgery.
enter clinical practice in the coming years.
● T2 hyperintensity in the After examination of the musculoskeletal structures and vertebral canal, the
spinal cord from cervical spinal cord is generally examined by T2-weighted sequences to look for cord
spondylotic myelopathy signal changes. Absence of cord signal changes does not exclude the presence of
may have a snake-eye myelopathy. Summarizing multiple series, the sensitivity of cord signal change
appearance, with areas of
hyperintensity in the
for the presence of cervical spondylotic myelopathy is in the range of 58% to
anterior horns bilaterally. 85%.18 Hence, patients may have symptoms and benefit from intervention
without necessarily having cord signal
changes, especially patients with mild
myelopathy (CASE 7-1). In fact, in clinical
series of imaging before and after surgery,
the presence of any cord signal
hyperintensity does not correlate strongly
with outcome either positively or
negatively.19
Even in patients with cord signal
hyperintensity, varying underlying
pathology is present, ranging from edema
and demyelination to necrosis and gliosis.
If very bright cord signal T2 changes
(same intensity as the CSF) are seen in
combination with T1 hypointensity, then
underlying gliosis that may not be
reversible is likely present.20 Fluffy, mildly
hyperintense T2 changes may reflect
edema that may improve with treatment;
however, this remains to be prospectively
FIGURE 7-4 validated in large clinical series. When
Sagittal T2-weighted MRI showing
moderate cervical spine stenosis at
cord signal changes occur from cervical
C5-C6 (arrow). A thin rim of CSF is still spondylotic myelopathy, they can have
visible posteriorly at this level. variable morphology. However, especially
168 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
with chronic compression, a snake-eye pattern (in which there are circumscribed
areas of high T2 signal intensity in the anterior cord) can evolve (FIGURE 7-6).
The location of the T2 signal hyperintensity may not occur at the region of
greatest stenosis but rather just adjacent to it. Finally, although IV gadolinium
contrast is generally not used to evaluate for cervical spondylotic myelopathy,
enhancement may be seen on postcontrast T1-weighted images. A specific
pattern of enhancement called the pancakelike pattern has been described in
patients with spondylotic myelopathy. It refers to a flattened appearance of
enhancement different from the typical rostrocaudal enhancement throughout a
lesion that accompanies transverse myelitis and has the following characteristics:
A 54-year-old man presented CASE 7-1
for evaluation of long-standing
neck pain and new paresthesia
in his fingertips. His primary
care doctor obtained an MRI
of his cervical spine, which led
to referral for neurosurgical
consultation and initial
recommendation for spinal
surgery. He sought a second
opinion from a neurologist.
On examination, he had
minimal weakness in left knee
flexion, hyperreflexia in his
left leg, and downgoing plantar FIGURE 7-5
responses. He had restricted Imaging of the patient in CASE 7-1. Axial T2-weighted
range of motion of his neck to MRI shows a right-sided disk protrusion with
flattening of the right side of the cervical cord
lateral movement bilaterally.
(arrow) and rotation of the spinal cord.
MRI of his cervical spine
(FIGURE 7-5) showed severe
stenosis of the cervical spinal
cord at C3-C4 by a right-sided
disk protrusion.
The optimal management strategy in this case is unclear. The patient had COMMENT
signs of mild myelopathy from cervical spondylotic disease that could
stabilize or progress with time. After discussing different options, he
elected to continue conservative management with physical therapy and
sequential neurologic examinations. Five years later, he continued to be
stable with minimal myelopathic signs. Another observation is that
although the patient had more significant right-sided spinal cord
compression, he was symptomatic on the left side of the body. This
mismatch between the side of the compression and side with more
symptoms is a known phenomenon and does not exculpate the
compressive lesion.
CONTINUUMJOURNAL.COM 169
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
FIGURE 7-6
Severe multilevel degenerative disease. A, Sagittal T2-weighted MRI shows severe multilevel
degenerative disease of the cervical spine with abnormal focal T2 hyperintensity of the cord
at C5-C6 just caudal to the level of the greatest stenosis at C5-C6 (arrow). B, Axial
T2-weighted MRI at C5-C6 (level of arrow in panel A) shows bilateral anterior cord T2
hyperintensity that is more hyperintense on the right compared to the left.
(1) a transverse band of enhancement with width of enhancement that is greater
than or equal to the height, (2) location at or just below the site of maximal
stenosis and at the center of the T2 hyperintensity, and (3) circumferential
enhancement of white matter on axial sequences sparing the gray matter
(FIGURE 7-721).22 The enhancement resolves slowly and can persist for many
months even after surgical decompression. Clinically, apart from the diagnostic
utility of the imaging sign, it is important for neurologists to be aware of the
possibility of enhancement with cervical spondylotic myelopathy. The author is
personally aware of patients who have undergone multiple investigations for
myelitis and neoplasms because of “atypical” finding on contrast-enhanced MRI.
Since conventional MRI does not accurately capture the underlying
neuropathology and corresponding prognosis with intervention, multiple new
imaging techniques are being developed to look for injury to the spinal cord in
cervical spondylotic myelopathy. Some of the more promising techniques
include diffusion tensor imaging, magnetization transfer, and magnetic
resonance spectroscopy. Most of these techniques, which were initially
developed for brain imaging, show artifacts introduced by spinal imaging. It is
likely that in the coming 5 to 10 years, these techniques will become better
refined and enter routine clinical practice for better evaluation of the spinal cord
in cervical spondylotic myelopathy.
Treatment
How best to treat cervical spondylotic myelopathy is controversial, and
significant regional and practitioner variation exists. This variability originates
from a lack of understanding of the natural history of untreated disease and lack
of robust trials comparing conservative and interventional methods. To begin
with, patients with severe cervical spinal stenosis on imaging without
myelopathic symptoms likely do not all need surgery. The natural history of
cervical spondylotic myelopathy was evaluated in a cohort of 199 patients with
asymptomatic severe cervical spinal stenosis followed for a median of 44 months.
Although about 22% developed symptoms of myelopathy during follow-up, no
170 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
association was seen between minor KEY POINTS
traumatic events and the onset of
● The natural history of
myelopathy.23 This is in contrast to the untreated cervical
often-heard advice that the goal of early spondylotic myelopathy is
surgery is to prevent the development of unclear and has
severe myelopathy from relatively minor considerable variability.
trauma (such as hitting one’s head on a
● Minor trauma is an
doorframe). For those who progressed to unusual precipitant of acute
clinical myelopathy within a year, myelopathy in patients with
predictive factors were the presence of asymptomatic severe
clinical cervical radiculopathy and cervical spine stenosis.
abnormal evoked potentials ● Patients with untreated
(somatosensory or motor); MRI factors, cervical spondylotic
such as cord hyperintensity or cord myelopathy often have a
cross-sectional area, were not predictive stepwise course, with
periods of stability and then
of early conversion to myelopathy. episodes of acute
Most experts would agree that surgery deterioration. Some
aimed at decompressing the cervical patients relentlessly
spinal canal is indicated for patients with progress, whereas others
can remain stable for years.
myelopathy with significant disability
(CASE 7-2). What to do with symptoms of
mild myelopathy (such as findings of
hyperreflexia in the legs and a mild sense
of instability) is far less clear. Even in the
earliest clinical series, it was observed that
not all patients relentlessly progress to
disability and that the untreated clinical
course often had a stepwise progression
with phases of deterioration followed by
long periods of stability.24 Clinical trial
FIGURE 7-7 evidence for the benefit of conservative
Pancakelike enhancement in cervical management versus surgical intervention
spondylotic myelopathy. Sagittal
T2-weighted cervical spine MRI shows a
is principally limited by small numbers.
longitudinally extensive One trial randomly assigned 68 patients
T2-hyperintense lesion in the cervical with mild or moderate cervical
cord (A, arrows) with moderate to spondylotic myelopathy to either
severe stenosis at the C4-C5 level. The
conservative or surgical treatment and
presence of a flat pancakelike
enhancement in which the width is followed them for 3 years.25 At last
equal to the height on sagittal follow-up, patients treated conservatively
postcontrast T1-weighted MRI (B, did no worse on scores of myelopathy
arrows) involving the white matter and
than those treated surgically. In fact, on
sparing the gray matter on axial
sequences (C, arrows) is highly the timed walking test, patients treated
characteristic of the enhancement conservatively walked 10 meters faster
associated with cervical spondylotic than those treated surgically after 3 years.
myelopathy.
In both groups, about one-third of
Reprinted with permission from Flanagan EP,
Handb Clin Neurol.21 © 2016 Elsevier BV. patients had T2 hyperintensity on initial
cervical spinal cord MRI. Another smaller
trial randomly assigned 49 patients with
mild or moderate cervical spondylotic
myelopathy to surgical or conservative
CONTINUUMJOURNAL.COM 171
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
treatment and followed them for 2 years.26 In this trial also, no clear differences
were seen in myelopathy rating scores or in electrophysiologic measures between
the two groups after 2 years.
These small randomized trials contrast with usual clinical practice at many
centers. Prospective clinical series demonstrate neurologic and pain
improvement with surgery, although any surgical intervention necessarily has a
large placebo effect.27,28 More patients likely have surgery for mild myelopathy
than benefit in the long term. On the other hand, cervical spondylotic
myelopathy continues to be a major cause of morbidity and neurologic injury.
The clinical trials are small and underpowered, and the clinical scales used in the
trials may not be sensitive to small improvements in spinal cord function. In
clinical practice, the author of this article generally recommends conservative
therapy for signs or symptoms of mild myelopathy present for many months or
years (CASE 7-2) and recommends intervention for significant disability or
progressive neurologic injury in sequential clinical examinations.
CASE 7-2 A 50-year-old man with prior spinal cord trauma and residual mild
left-sided weakness experienced increasing difficulty walking and loss of
dexterity with fine finger movements. On examination, he had moderate
weakness in the flexor muscles
of his legs, spasticity in his
left arm and both legs, and
diminished sensation to
vibration in both legs.
MRI of his cervical spine
showed disk protrusion at the
C6-C7 level causing severe
stenosis of the cervical spine
in addition to prior cord
trauma at C4-C5 (FIGURE 7-8A).
Surgery was recommended,
but the patient did not
follow up. He returned FIGURE 7-8
3 years later and was walker Imaging of the patient in CASE 7-2. A, Sagittal
dependent with persistent T2-weighted MRI shows an area of T2 cord
spasticity in the legs. Repeat hyperintensity at C4-C5 and disk protrusion
causing severe canal stenosis at C6-C7 (arrow). B,
MRI showed resolution of
Repeat sagittal T2-weighted MRI obtained 3 years
the disk protrusion at later shows resolution of the prior disk protrusion
C6-C7 (FIGURE 7-8B). at C6-C7 (arrow) without surgery.
COMMENT This case illustrates that if the spinal cord is compressed for long enough,
irreversible injury to the spinal cord can occur. In this case, the disk
reabsorbed back without any intervention, but the patient’s neurologic
signs did not improve. His disability may have been preventable if he had
gotten surgical decompression.
172 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Even in cases in which conservative management is chosen, no clear KEY POINTS
consensus exists on what is meant by this aside from no surgery. In some centers,
● Conservative therapy for
patients undergo physical therapy to improve strength and balance in cervical spondylotic
combination with gentle neck stretching exercises to improve any coexistent myelopathy generally
neck pain. All patients should avoid activities that cause severe flexion/extension involves physical therapy
neck movements that may cause further injury to the spinal cord and can provoke and gentle cervical spine
range-of-motion exercises.
an acute central cord syndrome. None of these interventions have individually
been tested in clinical trials, and which are most beneficial is unclear.29 ● Cervical spinal stenosis
can be decompressed via
SURGICAL APPROACHES. The concept that surgery could potentially improve either an anterior or a
spondylotic myelopathy originated in the 1920s when Byron Stookey of Bellevue posterior approach. No
clear consensus exists on
Hospital described decompression of the cervical canal and improvement in which approach is superior.
neurologic function in patients with ventral herniations of what he called
“cervical chondromas.”30 Since then, many different surgical techniques have ● C5 radiculopathy can be a
been developed to address cervical spinal cord compression from spondylotic postoperative complication
of cervical spine surgery.
disease. However, in the surgical community, no clear consensus exists on the
best operative technique. Hence, an identical structural pathology could be ● Upper extremity strength
addressed differently based on the surgeon and the center. Generally, surgery for recovers best following
cervical spondylotic myelopathy can be divided into anterior and posterior surgery for cervical
spondylotic myelopathy,
approaches. In the anterior approach, the compressing disk is generally removed,
whereas recovery of leg
often in combination with placement of a graft in the intervertebral space for strength and sensory
fusion. Instrumentation with plating of the vertebra anteriorly is frequently used dysfunction are less
to improve rates of fusion. Innovations in hardware, including plates with complete.
dynamic load sharing, plates with smaller screws, and low-profile plates, have
decreased rates of fusion failure. Biodegradable plates are in the process of
development and may enter clinical use in coming years. The alternative
decompression approach is a posterior one, in which the goal is to provide more
space in the spinal canal via laminectomy or laminectomy with fusion in cases of
dynamic instability. Similar to innovations in anterior instrumentation, the
hardware used for posterior instrumentation has also changed, with improved
axial load sharing and better sagittal balance with goals of decreasing stress on the
adjacent spine and decreasing rates of hardware failure.
Whether one approach is better than the other is a matter of controversy and
surgeon preference. Overall, for multiple levels, the posterior approach is likely
easier, whereas for a single level of compression from a large ventral disk, the
anterior approach may be preferred. Primary surgical complications include
wound infection, bleeding, displacement of hardware, and failure of fusion.
Some more specific neurologic complications include C5 radiculopathy, even in
surgeries that do not directly involve the C5 nerve root. The cause of this
complication is unclear. Injury to the recurrent laryngeal nerve can occur,
especially in anterior approaches, causing hoarseness of voice.
Following surgery, some improvement in upper extremity function occurs in
about 60% to 80% of patients based on unblinded clinical series.28,31 Recovery of
lower extremity dysfunction and sensory dysfunction are usually less robust
compared to arm strength recovery. Neurologic recovery continues to occur over
the first few months but typically plateaus at around 6 months. A risk of
spondylosis occurring at adjacent levels exists (called adjacent segment disease),
especially after fusion surgeries of the spine. This risk is calculated to be around
2% per year, and patients often need careful monitoring for recurrent symptoms
following surgery.28
CONTINUUMJOURNAL.COM 173
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
SYRINGOMYELIA
Syringomyelia refers to the presence of a syrinx, a fluid-filled, glial-lined cavity,
within the parenchyma of the spinal cord. This entity must be distinguished from
an enlarged central canal (hydromyelia), which is an ependymal-lined enlargement
of the normally obliterated central canal. This is an important distinction that is
sometimes not recognized and can lead to inappropriate diagnosis and therapies.
The central canal is a circular midline structure located at the junction of the ventral
one-third and dorsal two-thirds of the spinal cord. The central canal is an
embryologic remnant that progressively becomes obliterated during adulthood.
However, not uncommonly, some portions of the central canal can remain visible
on imaging and are often found incidentally (FIGURE 7-9). In an MRI spine series of
794 patients, the central canal was enlarged in 12, corresponding to a rate of 1.5%.32
In none of the patients was the central canal enlargement pathogenic or related to
the clinical syndrome leading to the imaging study. When enlargement of the
central canal is visible, the contours are generally smooth and without nodularity.
Most instances of incidental enlarged central canal are in the thoracic spinal cord,
although cervical spinal cord enlarged central canals are also seen.32
By contrast, syringomyelia can occur in the cervical or thoracic segments and
has variable appearance. The prevalence of syringomyelia is estimated to be 3.3
per 100,000 to 8.5 per 100,000, with variation in different ethnic groups.33
Epidemiologically, syringomyelia can be primary or associated with other
predisposing conditions. The most common predisposing condition is Chiari type
I malformation, which can be clinically silent but seen on imaging as herniation
of the cerebellar tonsils into the foramen magnum. About a 65% to 80% incidence
of syringomyelia is seen with Chiari type I malformation (FIGURE 7-10).34 More
uncommonly, patients with syringomyelia may have Chiari type II malformations,
in which both the cerebellum and brainstem herniate into the foramen magnum,
often accompanied by myelomeningocele in the lumbar spine. Acquired spinal
FIGURE 7-9
Enlarged central canal. A, Sagittal fat-suppressed short tau inversion recovery (STIR)
MRI shows a dilated cystic region at the C6 level. B, Axial T2-weighted image shows a
rounded central structure without myelomalacia that is most consistent with an enlarged
central canal.
174 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
● An enlarged central canal
is often incidentally found
on imaging and is generally
not pathogenic.
● Chiari type I malformation
can be clinically silent and
associated with
syringomyelia.
● Syrinx formation from
spinal cord injury can be
delayed by many years.
FIGURE 7-10
Syringomyelia with Chiari type I malformation. A, Sagittal T2-weighted MRI shows
syringomyelia at the C6-C7 level. B, Concurrent T1-weighted sagittal brain MRI shows a mild
Chiari type I malformation with herniation of the cerebellar tonsils (arrow) into the foramen
magnum. These findings were incidental for the patient.
cord injury can also lead to syrinx formation. Traumatic spinal cord injury can
predispose to late development of a syrinx. In one study, the mean interval
between spinal cord injury and syrinx development was 8.6 years.35
Other causes of spinal cord injury, such as spinal cord infarction or myelitis from
multiple sclerosis or neuromyelitis optica (NMO), may also infrequently lead to
syringomyelia in a delayed fashion. Neoplasms are an important secondary cause of
acquired syringomyelia. Midline neoplasms in the spinal cord, such as ependymoma
or hemangioblastoma, are primarily associated with syringomyelia. Interestingly,
the syrinx is most frequently located above the tumor, followed by both above and
below the level of the tumor. It is infrequent to have a syrinx located solely below the
level of the tumor. The chances of developing a syrinx are generally higher with a
more rostral tumor in the spinal cord.36 Familial syringomyelia has also been
described in small clusters, pointing to as-yet undiscovered genetic causes.
Pathogenesis
Many different theories exist to explain the development and progression of
syringomyelia. An early theory hypothesized that syringomyelia represents the
cavitation of a glial tumor that became necrotic from insufficient blood supply.37
However, histopathology did not show tumor cells in most syringes, and
tumor-directed treatment with radiation therapy did not resolve the syringes.
Others observed that in the nervous system, vascular injury evolved to
cavitation. They hypothesized that either ischemic or hemorrhagic injury to the
spinal cord evolved with time to have the final appearance of a syrinx. However,
these theories do not explain the progressive nature of a syrinx, which often
expands with time and causes increasing spinal cord dysfunction. Many patients
did not have signs or symptoms of vascular injury to the spinal cord before the
development of myelopathy from the syrinx.
Over time, hydrodynamic theories have gained favor as the cause of
syringomyelia. Simple occlusion of the central canal and impairment of bulk flow of
CONTINUUMJOURNAL.COM 175
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
CSF are not fully explanatory since most healthy adults have an occluded central
canal and do not develop a syrinx. The English neurosurgeon Bernard Williams
developed one of the first widely accepted hydrodynamic theories seeking to
explain why syringomyelia is more common in Chiari malformations. He
hypothesized that activities such as coughing or sneezing transiently displace CSF
from the head into the spinal canal. In patients with Chiari malformation and a
crowded foramen magnum with impaired circulation of CSF, a longer time passes
before pressure in the head and spinal canal equilibrate. During this vulnerable time,
CSF is postulated to be sucked into the spinal cord either through the central canal or
potentially through the spinal cord itself, causing a cystic cavitation.37 Although the
theory has empirical support in cases of Chiari malformation, the theory does not
explain other causes of syringomyelia in which no crowding of the foramen
magnum is present. An alternative theory postulates that with interference of CSF
circulation in the spinal subarachnoid space, the velocity of CSF in the subarachnoid
space increases. Following the Bernoulli law, the increased velocity of the fluid
results in lower net subarachnoid pressure, which causes a distending force on the
spinal cord. Over time, this gradually results in a cavitary expansion of the spinal
cord, causing a syrinx.38 Many other theories have been postulated to explain the
buildup of fluid in the spinal cord. Although we do not yet have a definitive answer,
a unifying theme appears to be impairment of free CSF flow in the spinal
subarachnoid space. Understanding the mechanism will be important in the future
because treatment directed at improving the flow of CSF, such as by lysis of
adhesions in arachnoiditis or decompression of the foramen magnum, may be
sufficient to prevent the progression of syringomyelia.
Clinical Features
Classically, slow expansion of a syrinx in the central cord causes interruption of the
crossing spinothalamic tracts via the anterior commissure. Hence, early on,
patients develop a band of numbness limited to pain and temperature sensation in
the affected dermatomes with preserved vibration and joint position sense
(dissociated sensory loss). This pattern of sensory loss has been called a capelike
distribution of sensory loss as the cervical and upper thoracic dermatomes are
often affected by syringomyelia. Over time, as the syrinx expands and causes
further spinal cord destruction, descending tracts (such as the corticospinal tract)
are affected, causing weakness and spasticity in the legs. In clinical practice,
many types of syrinx are not located exactly in the midline but are eccentric
to one side. Hence, many patients do not have the classic progression from
the capelike bilateral sensory loss pattern to weakness. Wide variability can
exist in the clinical syndrome, such as starting with a slowly progressive
hemicord syndrome.
Because of the interruption of the spinothalamic tracts, neuropathic pain that is
often poorly localized is an important early feature. For example, in a case series of
midline cord ependymomas, neuropathic pain with sensory loss was the earliest
feature, present for a median of 13 months before diagnosis of the tumor.39 Other
important clinical clues are lower motor neuron features that gradually become
apparent as the anterior horn cells become injured. This can cause muscle atrophy
in the arms with a cervical spinal cord syrinx. When the paraspinal muscles
become weak, progressive scoliosis is common as well. Since autonomic fibers
descend in the midline, slow expansion of midline lesions as in syringomyelia can
cause early autonomic dysfunction. This can take the form of bowel and urinary
176 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
sphincter dysfunction, sexual dysfunction, and sympathetic dysfunction such as KEY POINTS
Horner syndrome with high cervical cord lesions.
● Free CSF flow impairment
in the spinal subarachnoid
Treatment space is a common theme
How to best manage syringomyelia is uncertain, and recommendations derive among the different
from small case series rather than randomized trials. The first question is whether predisposing causes of
syringomyelia.
anything needs to be done. The natural history of the disease may depend on the
age of the patient and the underlying predisposing condition. In a group of 17 ● A small midline syrinx
pediatric patients with mild neurologic symptoms followed for an average of 3 causes interruption of
years, 15 of the 17 patients did not need an intervention.40 The two children who crossing spinothalamic
needed surgery had underlying Chiari malformations. In another natural history tracts and a capelike
distribution of numbness to
study of 19 patients followed for a median of 9 years, eight had no progression of pain and temperature.
symptoms, another eight had a slowly progressive course, and three had
intermittent periods of progression.41 Finally, in a larger series, 38 patients who did ● The natural history of
not undergo surgery were followed for an average of about 5 years; about half syringomyelia is
unpredictable. Many
eventually had progression of symptoms, whereas the other half remained patients remain
unchanged or even improved.42 In this series, patients with segmental sensory asymptomatic, whereas
signs had a more benign prognosis, whereas those with paraparesis from others can progress with
myelopathy or bowel/bladder dysfunction were more likely to progress. time.
Hence, many patients with mild symptoms will not benefit from interventions,
and, despite prominent imaging findings, a conservative approach with
symptomatic management and sequential neurologic examinations may be the best
course. In patients with progressive myelopathy, surgical intervention is usually the
next step. Because of the uncertainty in the pathogenesis, development, and
progression of syringomyelia, how best to treat remains unclear as well. One
approach is to improve CSF circulation by decreasing resistance in the spinal
subarachnoid space. For many patients with Chiari malformation, this takes the
form of suboccipital craniectomy and decompression of the posterior fossa. In a
surgical series of 75 patients, most of whom had Chiari malformations,
craniocervical decompression alone appeared to relieve or stabilize symptoms in
about 75%.43 Additional intervention to improve the syrinx did not confer more
benefit. In those with syringomyelia from other causes, spinal subarachnoid
circulation can be improved by laminectomy at the affected levels along with
lysis of adhesions for those with arachnoiditis.
Despite these steps, many patients continue to progress with enlargement of
their syrinx. In these patients, additional interventions should be performed.
Most commonly, a syringosubarachnoid shunt is placed, connecting the syrinx
with the subarachnoid space (FIGURE 7-11). This is a high-risk procedure in
which a small incision is made in the spinal cord itself to reach the shunt. In a
small series, the shunting procedure appeared to successfully decompress the
syrinx and improve symptoms.44 This procedure may be especially useful in
patients with a large syrinx. A caveat with shunting is that although the syrinx
may improve rapidly immediately, a high rate of syrinx reaccumulation exists,
either from shunt failure or the development of a new syrinx in the cord that does
not communicate with the syrinx that was drained.
OTHER STRUCTURAL MYELOPATHIES
Other, less common, structural abnormalities of the spine may present with
progressive myelopathy. The following sections give brief overviews of a
selection of these abnormalities.
CONTINUUMJOURNAL.COM 177
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
Idiopathic Spinal Cord Herniation
Spinal cord herniation is characterized by
a defect through which the spinal cord is
displaced, typically in the ventral dura.
This syndrome primarily affects the
thoracic spinal cord. Clinically, patients
develop thoracic myelopathy that slowly
progresses over the course of months to
years. In large case series and meta-
analyses, a mild female predominance
was seen, with the average age of
diagnosis about 51 years.45 Progressive
Brown-Séquard syndrome is the most
common clinical syndrome. Diagnosis is
typically made by MRI of the spine. The
usual finding is adhesion of the spinal cord
to the anterior portion of the spinal canal,
FIGURE 7-11 with deformity in the contour of the spinal
Sagittal T2-weighted MRI shows a cord in sagittal sections (seen as kinking of
large multiloculated syrinx in the
upper thoracic spinal cord. A
the cord). Cord T2 signal changes may or
syringosubarachnoid shunt (arrow) did may not be seen. With CT myelography,
not stop the progression of the syrinx. intrathecal contrast is seen in the dorsal
aspect of the spinal cord but not in the
ventral region. This finding can
distinguish spinal cord herniation from a dorsal arachnoid cyst, in which
impairment of CSF flow is seen on myelography.
In patients with symptomatic and progressive disease, treatment is with
surgical correction. Generally, two different surgical approaches are used to treat
spinal cord herniation.46 The first is a dural patch of the defect with release of the
spinal cord to a more natural physiologic state. The second approach is
paradoxical widening of the dural defect with the goal of creating enough space
to prevent spinal cord strangulation. At present, no clear consensus exists on
what the optimal technique is. Most patients improve after surgical correction,
and those with Brown-Séquard syndrome have a better prognosis compared to
those with a more significant myelopathy.
Arachnoid Cyst
Spinal arachnoid cysts are intradural-extramedullary cystic structures in the
subarachnoid space. In many cases, arachnoid cysts are found incidentally on
routine imaging of the spine and are clinically asymptomatic. The etiology of the
cysts is unclear; many are idiopathic, whereas others are associated with
congenital spinal deformities in children or with spinal trauma in adults, such as
after epidural hematoma or lumbar myelography. The latter etiologies suggest
impairment of subarachnoid fluid flow or arachnoiditis as possible contributors
to cyst formation. Overall, spinal arachnoid cysts are located primarily in the
thoracic spine dorsal to the spinal cord, although anterior thoracic arachnoid
cysts and cervical arachnoid cysts have also been rarely described. MRI is the
preferred imaging modality to diagnose arachnoid cysts. Arachnoid cysts have
the same signal intensity as CSF, with generally visible boundaries and
displacement of the spinal cord (FIGURE 7-12). The boundaries of the cysts do not
178 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
enhance after IV gadolinium injection, KEY POINTS
and restricted diffusion is not seen within
● Idiopathic spinal cord
the cyst (more typical in epidermal cysts). herniation is characterized
In CT myelography, a variable degree of by a defect through which
contrast opacification of the cyst is seen. the spinal cord is displaced,
Clinically asymptomatic cases are typically in the ventral dura
and generally presenting
followed by serial clinical examinations
with progressive
and imaging. When clinically myelopathy.
symptomatic, patients often report
symptoms of myelopathy, such as leg ● Spinal arachnoid cysts are
weakness, gait instability, or urinary intradural-extramedullary
cysts in the subarachnoid
dysfunction, in combination with space that can cause
radicular neuropathic pain.47 Treatment myelopathy by compression
of symptomatic arachnoid cysts is of the spinal cord.
generally surgical, and multiple
● Spinal arachnoid webs
approaches have been described in the are intradural bands of
literature. The simplest procedures are arachnoid tissue that usually
cyst fenestrations. For more refractory attach to the dorsal surface
cases, the cysts can be excised in of the spinal cord.
combination with laminectomy to
● Spinal arachnoid webs
increase subarachnoid space. may not be seen directly on
MRI but rather inferred from
Arachnoid Web change in caliber of the
Like spinal cord herniation and arachnoid spinal cord with dorsal cord
indentation.
cyst formation, arachnoid web primarily
FIGURE 7-12
affects the thoracic spine, causing ● Spinal epidural
Sagittal T2-weighted MRI shows progressive myelopathy. Spinal arachnoid lipomatosis refers to
multiloculated arachnoid cysts with webs are intradural bands of arachnoid accumulation of fat in the
cord atrophy (arrow) in a patient with epidural space that can be
tissue that usually attach to the dorsal asymptomatic or cause
congenital spinal deformities.
surface of the spinal cord. The cause of symptoms from
web formation is unclear, but based on compression of nerve roots
similar location, some authors speculate that an arachnoid web represents an or the spinal cord.
incomplete or collapsed arachnoid cyst. Presenting symptoms are typically back
or neck pain in combination with progressive myelopathy, such as difficulty
walking or numbness in the legs. On MRI, the arachnoid web is often not seen
directly. Instead, the effects are seen indirectly on the spinal cord, in which a
dorsal indentation is seen. T2 cord hyperintensity and, frequently, syringomyelia
may be seen. The abrupt change in caliber of the spinal cord with a dorsal cord
indentation where the arachnoid web attaches has been called the scalpel sign.48
Treatment is usually by surgical sectioning of the arachnoid web combined with
laminectomy. In a small case series, surgical correction helped improve or stop
further progression of symptoms.49
Epidural Lipomatosis
Spinal epidural lipomatosis refers to the accumulation of fat in the epidural space.
When enough fat is present to encroach on the spinal canal or foramina,
patients can have symptoms of myelopathy, neurogenic claudication, or
radiculopathy. Spinal epidural lipomatosis can be idiopathic or secondary to
other conditions, such as exogenous steroids, hypercortisolism, or obesity.
Epidural corticosteroid injections are strongly associated with epidural fat
CONTINUUMJOURNAL.COM 179
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
proliferation. In a retrospective series of 28,902 consecutive patients undergoing
spinal MRI, the prevalence of spinal epidural lipomatosis was estimated
at 2.5%.50 Of these patients, only 5% had symptoms that were attributable
to the epidural fat. For the rest, the finding was either incidental or did not
explain the clinical syndrome. Hence, for most patients with this finding,
intervention for the epidural lipomatosis will not be needed. On imaging,
epidural lipomas are hyperintense on both T1 and T2 sequences but suppressed
on short tau inversion recovery (STIR) or other fat-suppressive sequences.
Epidural fat can span multiple vertebral segments, and whereas the lumbar
spine is the most commonly affected single region, the thoracic spine is next
most common.
The first step of treatment is to address secondary factors contributing to the
accumulation of epidural fat. For example, epidural corticosteroid injections
should generally be stopped. Investigations for undiagnosed causes of
hypercortisolism should be conducted as well. For symptomatic cases that do not
respond to conservative therapy, surgical therapy is generally laminectomy and
resection of epidural fat.51
Hirayama Disease
Initially described in Japan and other Asian countries, the characteristic feature
of this eponymous disease is insidious onset of weakness and atrophy of the
hand and forearm, predominantly in young males in their teens or twenties
without other cranial or pyramidal signs. The weakness is typically asymmetric
or unilateral. After progression for several years, the disease stops with static
weakness. When initially described, the proposed mechanism was thought to be
motor neuron disease of a restricted spinal segment, which the authors called
monomelic amyotrophy.52 Subsequently, Hirayama and colleagues53 established
that in patients who are symptomatic and in whom the disease is progressive,
movement of the dural sac occurs in flexion and extension postures. When
imaged with the neck extended and flexed, the diameter of the dural sac
decreases during flexion, with corresponding stenosis and pressure on the
spinal cord. Typically, no movement is seen in the bony elements. The
hypothesis is that with repeated neck flexion and extension movements,
the anterior horn of the lower cervical spinal cord is injured, accounting
for the forearm and hand weakness. Recognition of the clinical syndrome
is important because the dynamic movement of the dural sac can be missed
entirely on static MRI with the neck extended. How best to manage the
disease is unclear. In most patients, conservative therapy with avoidance
of neck flexion can stabilize the disease. The natural history of the disease
is generally of progression initially with long periods of stability. If patients
have progressive disability, cervical decompression and fusion can be performed.
Chronic Adhesive Arachnoiditis
Adhesive arachnoiditis is progressive fibrosis of the arachnoid membrane,
usually triggered by physical or chemical injury to the subarachnoid space. Cases
have been known to occur after spinal surgery, subarachnoid hemorrhage,
meningitis, trauma, or myelography using older oil-based contrast agents.
Symptoms are caused by a combination of mechanisms. The arachnoiditis in the
subarachnoid space causes radicular injury to traversing nerve roots. This is
seen on imaging as clumping and tethering of the nerve roots. Arachnoiditis can
180 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
also tether the spinal cord and cause consequent myelopathy. The impairment KEY POINTS
in free flow of CSF in the subarachnoid space also predisposes to syrinx
● Hirayama disease is
formation, which can then cause progressive myelopathy. Clinically, characterized by the
arachnoiditis presents after a time delay from the inciting event that can range insidious onset of weakness
from weeks to years.54 In patients with arachnoiditis of the lumbar spine, the and atrophy of the hand and
presentation is primarily of progressive lumbosacral radiculopathy. In others forearm, predominantly in
young males in their teens or
who have more widespread arachnoid injury, symptoms of slowly progressive
twenties without other
myelopathy with radicular findings predominate. Diagnosis is usually by MRI, cranial or pyramidal signs.
which shows the clumping of the nerve roots, often with enhancement.55 Thin
septations are often visible, tethering or displacing the spinal cord (FIGURE 7-13). ● In Hirayama disease,
Cord T2 hyperintensity or a cystic cavity may be present. In severe cases, the when imaged with the neck
extended and flexed, the
arachnoid can have calcium deposition (a process called ossification). No clear diameter of the dural sac
treatment has been identified for this debilitating and progressive disease. decreases during flexion
Further intervention to the spine should generally be minimized to decrease with corresponding stenosis
further arachnoid fibrosis. Patients are usually treated with a combination of and pressure on the spinal
cord without movement in
physical therapy and pain management. Anti-inflammatory therapies, including the bony elements.
corticosteroids and IV immunoglobulin (IVIg) have been tried without
controlled trials to support use. In infrequent cases in which a focal area of ● Spinal adhesive
adhesion causing progressive symptoms is present, surgery to lyse cord adhesion arachnoiditis refers to
progressive fibrosis of the
can be performed. The results, however, are mixed, with benefits offset by
arachnoid membrane with
further arachnoiditis. injury to the nerve roots,
tethering of the spinal cord,
CONCLUSION and disruption of free flow
of CSF.
In addition to cervical spondylotic myelopathy and syringomyelia, many other
structural abnormalities in the spine (which are individually infrequent but as a ● Arachnoiditis often
group common) can compromise the spinal canal and cause myelopathy. These presents after a time delay
include thoracic spine degenerative disease, arachnoid cysts, spinal arachnoid from the initial spinal injury
webs, spinal bony defects causing cord herniation, and Hirayama disease. In ranging from weeks to years.
patients with acute, subacute, or progressive myelopathy, structural causes
should remain high on the list of differential diagnoses and be investigated for
urgently. Neurologists have an important role in determining whether the
imaged abnormality is relevant to the clinical syndrome and being aware of the
appropriate management options and the prognosis with conservative
management.
FIGURE 7-13
Arachnoiditis with spinal cord tethering. A, Axial T2-weighted MRI of the cervical spine
shows tethering of the cervical spinal cord (arrow) from arachnoiditis. B, Sagittal
T2-weighted MRI also shows tethering of the cord (arrow) through the arachnoid space.
CONTINUUMJOURNAL.COM 181
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
REFERENCES
1 New PW, Reeves RK, Smith É, et al. International 12 Sadasivan KK, Reddy RP, Albright JA. The natural
retrospective comparison of inpatient history of cervical spondylotic myelopathy.
rehabilitation for patients with spinal cord Yale J Biol Med 1993;66(3):235-242.
dysfunction epidemiology and clinical outcomes.
13 Wang Z, Sakakibara T, Kasai Y. Overactive bladder
Arch Phys Med Rehabil 2015;96(6):1080-1087.
in cervical spondylotic myelopathy. J Orthop Sci
doi:10.1016/j.apmr.2015.02.016
2014;19(1):22-25. doi:10.1007/s00776-013-0491-1
2 Epstein NE, Hood DC. “Unnecessary” spinal
14 Estanol BV, Marin OS. Mechanism of the
surgery: a prospective 1-year study of one
inverted supinator reflex. A clinical and
surgeon’s experience. Surg Neurol Int 2011;2:83.
neurophysiological study. J Neurol Neurosurg
doi:10.4103/2152-7806.82249
Psychiatry 1976;39(9):905-908. doi:10.1136/
3 Nouri A, Tetreault L, Singh A, et al. Degenerative jnnp.39.9.905
cervical myelopathy: epidemiology, genetics,
15 Houten JK, Noce LA. Clinical correlations of
and pathogenesis. Spine (Phila Pa 1976)
cervical myelopathy and the Hoffmann sign.
2015;40(12):E675-E693. doi:10.1097/
J Neurosurg Spine 2008;9(3):237-242. doi:10.3171/
BRS.0000000000000913
SPI/2008/9/9/237
4 Bajwa NS, Toy JO, Young EY, Ahn NU.
16 Conway BL, Clarke MJ, Kaufmann TJ, Flanagan EP.
Establishment of parameters for congenital
Utility of extension views in spondylotic
stenosis of the cervical spine: an anatomic
myelopathy mimicking transverse myelitis. Mult
descriptive analysis of 1,066 cadaveric
Scler Relat Disord 2017;11:62-64. doi:10.1016/j.
specimens. Eur Spine J 2012;21(12):2467-2474.
msard.2016.12.004
doi:10.1007/s00586-012-2437-2
17 Matsumoto M, Fujimura Y, Suzuki N, et al. MRI of
5 Nouri A, Tetreault L, Nori S, et al. Congenital
cervical intervertebral discs in asymptomatic
cervical spine stenosis in a multicenter global
subjects. J Bone Joint Surg Br 1998;80(1):19-24.
cohort of patients with degenerative cervical
doi:10.1302/0301-620x.80b1.7929
myelopathy: an ambispective report based on a
magnetic resonance imaging diagnostic criterion. 18 Nouri A, Martin AR, Mikulis D, Fehlings MG.
Neurosurgery 2018;83(3):521-528. doi:10.1093/ Magnetic resonance imaging assessment of
neuros/nyx521 degenerative cervical myelopathy: a review of
structural changes and measurement
6 Younes M, Belghali S, Kriâa S, et al. Compared
techniques. Neurosurg Focus 2016;40(6):E5.
imaging of the rheumatoid cervical spine:
doi:10.3171/2016.3.FOCUS1667
prevalence study and associated factors. Joint
Bone Spine 2009;76(4):361-368. doi:10.1016/j. 19 Matsumoto M, Toyama Y, Ishikawa M, et al.
jbspin.2008.10.010 Increased signal intensity of the spinal cord on
magnetic resonance images in cervical
7 Abiola R, Rubery P, Mesfin A. Ossification of the
compressive myelopathy. Does it predict the
posterior longitudinal ligament: etiology,
outcome of conservative treatment?
diagnosis, and outcomes of nonoperative and
Spine (Phila Pa 1976) 2000;25(6):677-682.
operative management. Global Spine J 2016;6(2):
doi:10.1097/00007632-200003150-00005
195-204. doi:10.1055/s-0035-1556580
20 Vedantam A, Rajshekhar V. Does the type of
8 Takamiya Y, Nagata K, Fukuda K, et al.
T2-weighted hyperintensity influence surgical
Cervical spine disorders in farm workers
outcome in patients with cervical spondylotic
requiring neck extension actions. J Orthop Sci
myelopathy? A review. Eur Spine J 2013;22(1):
2006;11(3):235-240. doi:10.1007/
96-106. doi:10.1007/s00586-012-2483-9
s00776-006-1005-1
21 Flanagan EP. Autoimmune myelopathies. Handb
9 Kato F, Yukawa Y, Suda K, et al. Normal
Clin Neurol 2016;133:327-351. doi:10.1016/
morphology, age-related changes and
B978-0-444-63432-0.00019-0
abnormal findings of the cervical spine.
Part II: magnetic resonance imaging of 22 Flanagan EP, Krecke KN, Marsh RW, et al. Specific
over 1,200 asymptomatic subjects. pattern of gadolinium enhancement in
Eur Spine J 2012;21(8):1499-1507. spondylotic myelopathy. Ann Neurol 2014;76(1):
doi:10.1007/s00586-012-2176-4 54-65. doi:10.1002/ana.24184
10 al-Mefty O, Harkey HL, Marawi I, et al. 23 Bednařík J, Sládková D, Kadaňka Z, et al. Are
Experimental chronic compressive cervical subjects with spondylotic cervical cord
myelopathy. J Neurosurg 1993;79(4):550-561. encroachment at increased risk of cervical spinal
doi:10.3171/jns.1993.79.4.0550 cord injury after minor trauma? J Neurol
Neurosurg Psychiatry 2011;82(7):779-781.
11 Hashmi SZ, Marra A, Jenis LG, Patel AA. Current
doi:10.1136/jnnp.2009.198945
concepts: central cord syndrome. Clin Spine
Surg 2018;31(10):407-412. doi:10.1097/
BSD.0000000000000731
182 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
24 Nurick S. The natural history and the results of 36 Samii M, Klekamp J. Surgical results of 100
surgical treatment of the spinal cord disorder intramedullary tumors in relation to
associated with cervical spondylosis. Brain 1972; accompanying syringomyelia. Neurosurgery
95(1):101-108. doi:10.1093/brain/95.1.101 1994;35(5):865-873; discussion 873.
doi:10.1227/00006123-199411000-00010
25 Kadanka Z, Mares M, Bednaník J, et al.
Approaches to spondylotic cervical myelopathy: 37 Elliott NSJ, Bertram CD, Martin BA, Brodbelt AR.
conservative versus surgical results in a 3-year Syringomyelia: a review of the biomechanics.
follow-up study. Spine (Phila Pa 1976) 2002; J Fluids Structures 2013;40:1-24. doi:10.1016/j.
27(20):2205-2210; discussion 2210-2211. jfluidstructs.2013.01.010
doi:10.1097/01.BRS.0000029255.77224.BB
38 Greitz D. Unraveling the riddle of syringomyelia.
26 Bednarík J, Kadanka Z, Vohánka S, et al. The value Neurosurg Rev 2006;29(4):251-263; discussion
of somatosensory- and motor-evoked potentials 264. doi:10.1007/s10143-006-0029-5
in predicting and monitoring the effect of
39 Waldron JN, Laperriere NJ, Jaakkimainen L, et al.
therapy in spondylotic cervical myelopathy.
Spinal cord ependymomas: a retrospective
Prospective randomized study.
analysis of 59 cases. Int J Radiat Oncol Biol Phys
Spine (Phila Pa 1976) 1999;24(15):1593-1598.
1993;27(2):223-229. doi:10.1016/0360-3016(93)
doi:10.1097/00007632-199908010-00014
90231-j
27 Sampath P, Bendebba M, Davis JD, Ducker TB.
40 Singhal A, Bowen-Roberts T, Steinbok P, et al.
Outcome of patients treated for cervical
Natural history of untreated syringomyelia in
myelopathy. A prospective, multicenter study
pediatric patients. Neurosurg Focus 2011;31(6):
with independent clinical review.
E13. doi:10.3171/2011.9.FOCUS11208
Spine (Phila Pa 1976) 2000;25(6):670-676.
doi:10.1097/00007632-200003150-00004 41 Anderson NE, Willoughby EW, Wrightson P. The
natural history of syringomyelia. Clin Exp Neurol
28 Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper
1986;22:71-80.
PR. Cervical spondylotic myelopathy: patterns of
neurological deficit and recovery after anterior 42 Boiardi A, Munari L, Silvani A, et al. Natural history
cervical decompression. Neurosurgery and postsurgical outcome of syringomyelia. Ital J
1999;44(4):762-769; discussion 769-770. Neurol Sci 1991;12(6):575-579. doi:10.1007/
doi:10.1097/00006123-199904000-00041 BF02336954
29 Rhee JM, Shamji MF, Erwin WM, et al. 43 Logue V, Edwards MR. Syringomyelia and its
Nonoperative management of cervical surgical treatment–an analysis of 75 patients.
myelopathy: a systematic review. Spine (Phila Pa J Neurol Neurosurg Psychiatry 1981;44(4):273-284.
1976) 2013;38(22 suppl 1):S55-S67. doi:10.1097/ doi:10.1136/jnnp.44.4.273
BRS.0b013e3182a7f41d
44 Hida K, Iwasaki Y, Koyanagi I, et al. Surgical
30 Stookey B. Compression of the spinal cord due indication and results of foramen magnum
to ventral extradural cervical chondromas: decompression versus syringosubarachnoid
diagnosis and surgical treatment. Arch Neur shunting for syringomyelia associated with Chiari
Psych 1928;20(2):275-291. doi:10.1001/ I malformation. Neurosurgery 1995;37(4):673-678;
archneurpsyc.1928.02210140043003 discussion 678-679. doi:10.1227/
00006123-199510000-00010
31 Machino M, Yukawa Y, Hida T, et al. Persistent
physical symptoms after laminoplasty: analysis 45 Groen RJM, Lukassen JNM, Boer GJ, et al.
of postoperative residual symptoms in 520 Anterior thoracic spinal cord herniation: surgical
patients with cervical spondylotic myelopathy. treatment and postoperative course. an
Spine (Phila Pa 1976) 2012;37(11):932-936. individual participant data meta-analysis of 246
doi:10.1097/BRS.0b013e318238f15c cases. World Neurosurg 2019;123:453.e15-463.e15.
doi:10.1016/j.wneu.2018.11.229
32 Petit-Lacour MC, Lasjaunias P, Iffenecker C, et al.
Visibility of the central canal on MRI. 46 Summers JC, Balasubramani YV, Chan PCH,
Neuroradiology 2000;42(10):756-761. doi:10.1007/ Rosenfeld JV. Idiopathic spinal cord herniation:
s002340000373 clinical review and report of three cases. Asian J
Neurosurg 2013;8(2):97-105. doi:10.4103/
33 Brickell KL, Anderson NE, Charleston AJ, et al.
1793-5482.116386
Ethnic differences in syringomyelia in New
Zealand. J Neurol Neurosurg Psychiatry 2006; 47 Petridis AK, Doukas A, Barth H, Mehdorn HM.
77(8):989-991. doi:10.1136/jnnp.2005.081240 Spinal cord compression caused by idiopathic
intradural arachnoid cysts of the spine: review of
34 Paul AB. Syringohydromyelia. In: Small JE,
the literature and illustrated case. Eur Spine J
Noujaim DL, Ginat DT, et al, eds. Neuroradiology:
2010;19 Suppl 2:S124-S129. doi:10.1007/
spectrum and evolution of disease. Elsevier,
s00586-009-1156-9
2019:236-241.
48 Reardon MA, Raghavan P, Carpenter-Bailey K,
35 el Masry WS, Biyani A. Incidence, management,
et al. Dorsal thoracic arachnoid web and the
and outcome of post-traumatic syringomyelia. In
“scalpel sign”: a distinct clinical-radiologic entity.
memory of Mr Bernard Williams. J Neurol
AJNR Am J Neuroradiol 2013;34(5):1104-1110.
Neurosurg Psychiatry 1996;60(2):141-146.
doi:10.3174/ajnr.A3432
doi:10.1136/jnnp.60.2.141
CONTINUUMJOURNAL.COM 183
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
SPONDYLOTIC AND OTHER STRUCTURAL MYELOPATHIES
49 Sridharan A, Heilman CB. Transverse dorsal 53 Hirayama K, Tokumaru Y. Cervical dural sac and
arachnoid web and syringomyelia: case report. spinal cord in juvenile muscular atrophy of distal
Neurosurgery 2009;65(1):E216-E217; discussion upper extremity. Neurology 2000;54(10):
E217. doi:10.1227/01.NEU.0000348007.84175.FA 1922-1926. doi:10.1212/wnl.54.10.1922
50 Theyskens NC, Paulino Pereira NR, Janssen SJ, 54 Killeen T, Kamat A, Walsh D, et al. Severe
et al. The prevalence of spinal epidural adhesive arachnoiditis resulting in progressive
lipomatosis on magnetic resonance imaging. paraplegia following obstetric spinal
Spine J 2017;17(7):969-976. doi:10.1016/j. anaesthesia: a case report and review.
spinee.2017.02.010 Anaesthesia 2012;67(12):1386-1394.
doi:10.1111/anae.12017
51 Kellett CG, Siva V, Norman ICF, et al.
Symptomatic idiopathic spinal epidural 55 Anderson TL, Morris JM, Wald JT, Kotsenas AL.
lipomatosis in 9 patients: clinical, radiologic, and Imaging appearance of advanced chronic
pathogenetic features. World Neurosurg 2019; adhesive arachnoiditis: a retrospective review.
126:e33-e40. doi:10.1016/j.wneu.2019.01.098 AJR Am J Roentgenol 2017;209(3):648-655.
doi:10.2214/AJR.16.16704
52 Gourie-Devi M, Suresh TG, Shankar SK.
Monomelic amyotrophy. Arch Neurol
1984;41(4):388-394. doi:10.1001/
archneur.1984.04050160050015
184 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
REVIEW ARTICLE
Vascular Myelopathies
C O N T I N UU M A UD I O By Nicholas L. Zalewski, MD
I NT E R V I E W A V AI L A B L E
ONLINE
Downloaded from http://journals.lww.com/continuum by wqLe/H3/oM2vx1Qs5A5qMemKKHLPqE4qkmGNpdheG3ikf1o85ttJSkFL2oTkgOkhMEmawHvsuTTE5xJG2ZjqccytIAhVn2qegy060KLcKJuPZsx5htaYiopRjp2zor2egUzWJAEWYNrC3bBuCzr1RdmqNUpjE4IY on 04/28/2022
ABSTRACT
PURPOSE OF REVIEW: Neurologists should be able to identify clinical and
neuroimaging features that distinguish vascular disorders from other
causes of myelopathy.
RECENT FINDINGS:Although certain clinical features suggest a vascular
etiology in acute and chronic myelopathy settings, accurate MRI
interpretation within the clinical context is key. Recent studies have shown
vascular myelopathies are frequently misdiagnosed as transverse myelitis,
and recognition of this diagnostic pitfall is important. Many different
vascular mechanisms can cause myelopathy; this article provides a
comprehensive review that simplifies disease categories into arterial
ischemia, venous congestion/ischemia, hematomyelia, and
extraparenchymal hemorrhage.
SUMMARY: It is important to recognize and manage vascular disorders of the
spinal cord as significant causes of acute, subacute, and progressive
myelopathy.
INTRODUCTION
T
wo large retrospective studies recently showed that patients initially
CITE AS: diagnosed with idiopathic transverse myelitis frequently had
CONTINUUM (MINNEAP MINN) alternative myelopathy diagnoses, with vascular etiologies among the
2020;27(1, SPINAL CORD DISORDERS):
30–61.
most common.1,2 Vascular disorders of the spinal cord have important
time-to-treatment considerations as delays in diagnosis can be
Address correspondence to associated with worse outcomes,3 highlighting the importance of considering
Dr Nicholas L. Zalewski,
vascular causes early. Physicians should also be aware that treatments used for
Department of Neurology, Mayo
Clinic, Mayo Clinic Building, inflammatory disorders can potentially worsen symptoms and outcomes in
13400 E Shea Blvd, Scottsdale, vascular myelopathies.4-7 Although certain features strongly suggest a vascular
AZ 85259, zalewski.nicholas@
mayo.edu.
myelopathy in acute (severe deficits developing within ≤12 hours with pain) and
chronic (exertional/Valsalva worsening) settings, accurate MRI interpretation
RELATIONSHIP DISCLOSURE: within the clinical context is most critical. Many different vascular mechanisms
Dr Zalewski reports no
disclosure. exist; to simplify organization, this article divides vascular myelopathies into the
categories of arterial ischemia, venous congestion/ischemia, hematomyelia, and
UNLABELED USE OF
extraparenchymal hemorrhage.
PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE: Myelopathy should be presumed as acute and a potential neurologic
Dr Zalewski discusses the emergency at initial presentation until proven otherwise. Practically speaking, if
unlabeled/investigational use of
IV alteplase for the treatment of
a patient presents with rapid accumulation of deficits within approximately
spinal cord infarction. 24 hours or the acuity is indeterminate, a time-sensitive five-step, five-category
approach is recommended (TABLE 2-1). This approach provides an important
© 2021 American Academy
framework for compressive and noncompressive diagnoses and management
of Neurology. considerations in the acute setting.
30 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR ANATOMY OF THE SPINAL CORD
An understanding of the basic framework of spinal cord vascular anatomy helps
provide important insights into clinical features and mechanisms. The vascular
anatomy of the spinal cord consists of a single anterior spinal artery and paired
posterior spinal arteries that run along the length of the spinal cord. The anterior
spinal artery typically forms from two branches of intracranial V4 segments of
the vertebral arteries (or posterior inferior cerebellar arteries [PICAs] or cervical
segmental branches), whereas the paired posterior spinal arteries (often forming
a plexus) originate from PICAs or the proximal vertebral arteries. The anterior
spinal artery is often noncontinuous in the midthoracic region, referred to as the
watershed area.8
Conceptualizing the pathway of extrinsic vasculature to reinforce the anterior
spinal artery and posterior spinal arteries provides insight into localization of
pathology that could contribute to ischemia (FIGURE 2-19). This can be visualized
as starting at the central venous return of the caval system, to the right heart, to
the pulmonary vasculature, to the left heart, to the aortic arch, to the multiple
reinforcing artery branches. These reinforcing artery branches are (rostral to
caudal): the vertebral arteries (and PICA branches), subclavian arteries (with
ascending cervical and deep cervical artery branches), posterior intercostal
arteries, lumbar arteries, and iliac arteries (with lateral sacral and hypogastric
artery branches). These arteries feed into spinal branches (entering the neural
Approach to Acute Myelopathy (Rapid Deficits, Approximately 24 Hours) TABLE 2-1
Airway, breathing, and circulation (and optimize)
Trauma?
◆ Trauma protocol (eg, cervical collar), emergent spine surgery consult
Aortic dissection?
◆ CT angiography (eg, risk factors, chest/back pain, vital sign/pulse changes)
Emergent MRI spine, with diffusion-weighted imaging of cervical, thoracic, and lumbar
levels, unless clear localization (eg, quadriplegia). Assess for:
◆ Cord compression
◇ Structural/spondylosis (rarely acute, unless severe compression with or without new
trauma or fall)
◇ Tumor/mass
◇ Hematoma
◇ Infection (epidural abscess/space-occupying infection)
◆ Blood
◆ Flow voids
◆ Cord lesion (noncompressive and no blood or flow voids)
◆ Normal/equivocal
Stroke laboratory studies, with or without head CT (especially consider if MRI spine within
normal limits and no sensory level or pain)
CT = computed tomography; MRI = magnetic resonance imaging.
CONTINUUMJOURNAL.COM 31
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
foramina) that divide into paired
anterior and posterior radicular
arteries at each spinal segmental
level (FIGURE 2-2). However,
only a portion of radicular
arteries provide significant
contributions to the spinal cord,
termed anterior and posterior
radiculomedullary arteries,
whereas the rest terminate
within the nerve root, dura,
or pial plexus. Anterior
radiculomedullary arteries
provide significant
reinforcement to the anterior
spinal artery, whereas posterior
radiculomedullary arteries
FIGURE 2-1
supply the posterior spinal Extensive and flexible collateral vascular supply
arteries. Wide variability to the spinal cord. A, Longitudinal view of
exists in the number of segmental arteries branching off the aorta with
radiculomedullary arteries, with supplemental perfusion to the spinal cord. B,
Anastomotic network depicted showing vascular
anywhere from two to 17 supply of the spinal cord, paraspinal muscles, and
8,10,11
unpaired arteries. A main paravertebral tissue creating a longitudinally
cervical radiculomedullary connected flexible system.
artery is usually present at C3 Reprinted with permission from English SW, Zalewski NL,
8 Semin Neurol.9 © 2021 Thieme Medical Publishers, Inc.
and another at C6-C7. The
thoracic cord is supplied by deep
cervical and intercostal arteries.
The great anterior radiculomedullary artery (artery of Adamkiewicz) is most
often located between T9 and T12 (range T5 through L3); some patients may even
lack this artery. Great posterior radiculomedullary arteries have been
demonstrated as well.12 Notably, the anterior spinal artery can facilitate
anterograde or retrograde flow, depending on demand and variable anatomy.
The spinal cord also receives extrinsic vascular reinforcement from adjacent
paraspinal muscles and paravertebral tissue, creating a longitudinally connected
flexible system relatively resistant to ischemia.10,13 This is supported in everyday
practice when vascular surgeons occlude the aorta’s segmental branches with
large grafts, yet patients most often do not experience spinal cord ischemia.
Intrinsically, the anterior spinal artery supplies the anterior two-thirds of the
spinal cord through deep penetrating branches of central sulcal arteries, running
deep to superficial.14 Smaller posterior spinal arteries supply intrinsic vasculature
to the posterior one-third of the spinal cord and are a predominant contribution
to the vasocorona surrounding the cord, with superficial radial penetrating
arteries supplying superficial to deep.14 At the tip of the conus, an anastomotic
loop exists between the anterior spinal artery and posterior spinal arteries.15,16
Proximal nerve roots also receive vascular supply from branches of the anterior
spinal artery and radiculomedullary arteries,17 highlighting root involvement in
many patients with spinal cord infarction.7
The venous system drains the spinal cord through radially oriented
intramedullary veins that connect to a pial venous network on the surface
32 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
of the cord into both anterior and posterior KEY POINTS
spinal veins and subsequently to the
● Two large retrospective
internal venous plexus of the cord. This studies recently showed
venous system located within the that patients initially
subarachnoid space joins epidural veins diagnosed with idiopathic
(internal vertebral plexus) via a transverse myelitis
frequently had alternative
radiculomedullary vein in neural
myelopathy diagnoses, with
foramina, which then subsequently exits vascular etiologies among
to the external vertebral plexus. The the most common.
venous system then converges through
ascending lumbar (lumbar region), azygos ● Vascular disorders of the
spinal cord have important
(thoracic region), and innominate time-to-treatment
(cervical region) veins before returning to considerations as delays in
the caval system.18 diagnosis can be associated
with worse outcomes,
highlighting the importance
ARTERIAL ISCHEMIA of considering vascular
Arterial ischemia affecting the spinal cord causes early.
is classified as periprocedural spinal cord
infarction, spontaneous spinal cord ● The vascular anatomy of
the spinal cord consists of a
infarction, or spinal cord transient
single anterior spinal artery
ischemic attack (TIA). and paired posterior spinal
FIGURE 2-2 arteries that run along the
Representative view of the extrinsic Periprocedural Spinal Cord Infarction length of the spinal cord.
vascular supply to a vertebral level of Periprocedural spinal cord infarction was
the spinal cord. The aorta is shown ● Open or endovascular
first described by Sir Astley Cooper in 1825 thoracic aortic aneurysm
supplying posterior intercostal arteries,
traversing closely to vertebral bodies,
in a patient with a large traumatic repair is the most common
with supply of a spinal branch in the aneurysm of the iliac artery extending into procedure associated with
neural foramen dividing into anterior the lower aorta. Since then, many spinal cord infarction,
and posterior radiculomedullary artery representing approximately
different operations and medical 50% of periprocedural spinal
branches supplying reinforcement to the
procedures have been associated with cord infarction cases. Spinal
anterior and posterior spinal arteries.
© 2020 Mayo Clinic. spinal cord infarction.19 Open or cord infarction has also
endovascular thoracic aortic aneurysm been associated with other
aortic surgeries and an array
repair is the most common procedure of other procedures (eg,
associated with spinal cord infarction, representing approximately 50% of cases cardiac surgery, spinal
of periprocedural spinal cord infarction.19 Spinal cord infarction has also been decompression, epidural
associated with other aortic operations (15%) and an array of other procedures injection, angiography,
nerve block, embolization,
(eg, cardiac surgery, spinal decompression, epidural injection, angiography,
other vascular surgery, and
nerve block, embolization, other vascular surgery, and thoracic surgery).19 thoracic surgery).
The majority of patients (80%) with periprocedural spinal cord infarction
wake up from their procedure with maximum deficits, whereas others develop
symptoms several hours or days after the procedure and may accumulate deficits
over many hours. Although flaccid paraplegia is common, a number of patients
(>30%) have less severe deficits. Pain is much less frequent (15% of cases) than in
spontaneous spinal cord infarction (approximately 60% to 70% of cases); this
may signify an association with mechanisms of spinal cord infarction (eg, arterial
dissection, fibrocartilaginous embolism), although analgesics and other factors
could confound this. Emergent spinal cord imaging is important to rule out an
alternative treatable myelopathy mechanism (eg, epidural hematoma). Also,
typical imaging patterns can confirm the diagnosis of spinal cord infarction.
Periprocedural spinal cord infarction has provided insights into the diversity of
CONTINUUMJOURNAL.COM 33
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
CASE 2-1 A 66-year-old man was lifting heavy equipment when he acutely
developed severe neck pain and a sense of general weakness. The
following day, he suddenly developed worsening leg weakness and
urinary retention. He took a brief nap and awoke developing rapid
paraplegia within minutes. He was taken to the emergency department,
nearly quadriplegic and in respiratory distress. He was intubated and
transferred for further care.
Examination demonstrated skew deviation, severe asymmetric
quadriparesis in proximal and distal muscles, and a truncal sensory level
to temperature and pain on the left at C4 and the right at T4. Dorsal
column function was preserved. Resting tone was flaccid with areflexia.
Emergent MRI revealed
T2-hyperintense signal in the
upper cervical spinal cord,
predominantly in the ventral
gray matter (FIGURE 2-3A).
Characteristic owl eyes were
observed on axial cuts,
typical of spinal cord
infarction (FIGURE 2-3B).
CT angiography of the
head and neck identified
a left vertebral artery
dissection as the etiology.
Brain MRI confirmed
multifocal strokes
in the cerebellum contributing
to skew deviation (FIGURE 2-3C).
The patient was treated with
mean arterial blood pressure FIGURE 2-3
Imaging of the patient in CASE 2-1. A, Sagittal
augmentation and a lumbar T2-weighted MRI shows T2-hyperintense signal in
drain for 48 hours, then the upper cervical spinal cord, predominantly in
placed on aspirin for the ventral gray matter (arrow). B, Axial
long-term treatment. T2-weighted MRI shows characteristic owl eyes
(arrow), typical of spinal cord infarction. C, Axial
Follow-up several months
brain diffusion-weighted MRI confirms multifocal
later revealed subtle residual strokes in the cerebellum contributing to
motor and sensory deficits. skew deviation.
COMMENT This case highlights several points. Despite the patient’s reported earlier
symptoms of pain and generalized weakness, the sudden change with
rapid severe myelopathy was an essential clue to suspect spinal cord
infarction; examination suggesting deficits in the anterior spinal artery
territory raised additional suspicion for spinal cord infarction. Typical
imaging findings were seen on T2-weighted imaging, with owl eyes and
severe deficits out of proportion to a smaller lesion, and specific findings
confirmed spinal cord infarction (dissection, concurrent cerebral stroke).
Treatment was pursued, and the patient had an excellent outcome.
34 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
clinical and imaging findings that can be seen in spontaneous spinal cord KEY POINTS
infarction, in which diagnosis can be more challenging.
● During spinal cord
During spinal cord ischemia, the goal of treatment is to increase spinal cord ischemia, the goal of
perfusion pressure through collaterals. This is accomplished by lowering pressure treatment is to increase
within the spinal canal via CSF drainage (eg, drain 10 mL every 2 to 4 hours; goal spinal cord perfusion
CSF pressure 8 mm Hg to 12 mm Hg, depending on response) or mean arterial blood pressure through collaterals
by lowering pressure within
pressure (MAP) augmentation (eg, goal MAP >90 mm Hg or increase by 10 mm Hg
the spinal canal via CSF
to 20 mm Hg increments, observing for benefit), or both. Potential benefit needs to drainage or mean arterial
be weighed against risks (eg, overdrainage). Although two randomized clinical trials blood pressure
and multiple meta-analyses have shown benefit using prophylactic lumbar drains,20 augmentation.
data are limited regarding treatment benefit once ischemia has occurred. When
● Two large studies
ischemia occurs, early poor prognostication is generally not recommended, as many highlighted the frequent
patients have substantial improvements despite significant deficits.19,21 Factors misdiagnosis of spinal cord
associated with poor outcomes include a larger lesion on MRI, clinical severity,22 infarction as “transverse
flaccid areflexia, absence of a Babinski reflex,21 age, and comorbid medical factors. myelitis” in approximately
15% of referred cases.
Spontaneous Spinal Cord Infarction ● Although an older patient
The incidence of spinal cord infarction has recently been estimated at population with vascular risk
3.1 per 100,000 people; in this small study, six were spontaneous and two factors is common in spinal
cord infarction, mechanisms
periprocedural.23 Other studies have published similarly low estimates,
affecting younger patients
representing approximately 1% of strokes and 5% to 8% of cases of acute also occur (eg,
myelopathy.16,22 However, two large studies highlighted the frequent fibrocartilaginous embolism,
misdiagnosis of spinal cord infarction as “transverse myelitis” in approximately vertebral dissection),
highlighting that spinal cord
15% of referred cases.2,7 The recent introduction of diagnostic criteria may
infarction can occur at any
further increase our understanding of the true incidence. Although an older age.
patient population with vascular risk factors is common, mechanisms affecting
younger patients also occur (eg, fibrocartilaginous embolism, vertebral ● From the earliest days, it
dissection), highlighting that spinal cord infarction can occur at any age. has been recognized that
spinal cord infarction
frequently results in acute
CLINICAL FEATURES. From the earliest days, it has been recognized that spinal cord deficits localized to an
infarction frequently results in acute deficits localized to the anterior spinal anterior spinal artery
artery territory (bilateral corticospinal tract, lower motor neuron at lesion level, territory (bilateral
corticospinal tract, lower
and pain/temperature loss) or, less frequently, the posterior spinal artery motor neuron at lesion level,
territory (dorsal column dysfunction); these deficits may distinguish spinal cord and pain/temperature loss)
infarction from other myelopathies. Over time, other clinical syndromes, such as or, less frequently, a
Brown-Séquard syndrome, central cord syndrome, and complete cord posterior spinal artery
territory (dorsal column
syndrome, were also described.24 Although identifying a classic vascular territory
dysfunction); these deficits
is helpful, absence of a classic pattern is frequent and other premorbid conditions may distinguish spinal cord
(eg, peripheral neuropathy) can confound. infarction from other
Diagnosis has shifted to a focus on establishing severe nontraumatic myelopathies.
myelopathy deficits within 12 hours. Although labeling deficits as severe can be
● Severe acute pain (back,
challenging retrospectively, the timeline of severe paresis/plegia (usually chest, neck, limb) at or
bilateral) within hours is usually well delineated. In posterior spinal artery before onset is another
infarctions, this may manifest as a severe objective sensory deficit (eg, sensory helpful feature that is
ataxia). Approximately 25% of patients reach nadir after 12 hours but still display reported in approximately
70% of patients with spinal
a component of severe deficits within a 12-hour time frame of their acute cord infarction but is
stepwise/stuttering decline. The faster and more severe the deficits, the easier to atypical acutely in myelitis.
diagnose spinal cord infarction. Severe acute pain (back, chest, neck, limb) at
or before onset is another helpful feature that is reported in approximately 70%
of patients7 but is atypical acutely in myelitis (CASE 2-1). Pain may be an insight
CONTINUUMJOURNAL.COM 35
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
into the mechanism (eg, dissection, fibrocartilaginous embolism), given its higher
frequency in spontaneous spinal cord infarction than periprocedural cases.19 A
truncal sensory level or localized pain, or both, is helpful in localization of spinal cord
infarction; clinicians should consider alternative localizations if these features are
absent (bilateral anterior cerebral artery territory, rapid peripheral disorder). Strictly
unilateral presentations can occur but are rare and raise suspicion for cerebral
localization (eg, contralateral anterior cerebral artery territory with leg weakness). A
physical maneuver (eg, lifting, back hyperextension, neck movement, Valsalva) is
frequently reported at or before onset. This serves as a clue to the diagnosis and
potential mechanism (eg, arterial dissection, fibrocartilaginous embolism, radicular
artery compression from disk, or other mechanical mechanism).
NEUROIMAGING. Once spontaneous spinal cord infarction is suspected, it is
important to understand the typical MRI appearance in acute, subacute, and
chronic settings.
ACUTE. Refer to TABLE 2-1 for the emergent protocol for acute myelopathy. A low
threshold for MRI of the entire spine should exist, unless the localization is clear
(eg, cervical spinal cord in quadriplegia). Diffusion-weighted imaging (DWI)/
apparent diffusion coefficient (ADC) should be performed, but the sensitivity
is incomplete (50% to 70%),7,19 and sometimes takes days to evolve.25 In the
initial hours of symptoms, imaging is likely normal or equivocal.7 Early
FIGURE 2-4
MRI findings in spinal cord infarctions. Typical patterns of T2-hyperintense signal seen
in spinal cord infarction include owl eyes (A), associated with noncontiguous anterior
pencillike hyperintensity (B); anteromedial spot (C), confirmed with short anterior pencillike
hyperintensity on sagittal view (D); residual cystic myelomalacia with very bright T2
hyperintensity (E, F) and associated T1 hypointensity (G, H), seen more than 1 month after
spinal cord infarction; anteromedial T2 hyperintensity (I) with associated anterior pencillike
hyperintensity (J); anterior U or V shape (K) with associated anterior pencillike hyperintensity
on sagittal view (L); hologray (entire gray matter) pattern (M) with associated edematous T2
hyperintensity on sagittal view (N); and holocord (entire spinal cord) pattern (O) with
associated edematous T2 hyperintensity extending through the conus on sagittal view (P).
Modified with permission from Zalewski NL, et al, JAMA Neurol.7 © 2019 American Medical Association.
36 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
T2-hyperintense signal typical of spinal cord infarction (FIGURE 2-4) may be KEY POINTS
seen. Significant edema/swelling or enhancement is unusual acutely. Adjacent
● Once spontaneous spinal
dissection/occlusion or concurrent cerebral infarction may also be identified. cord infarction is suspected,
it is important to understand
SUBACUTE. A variety of axial T2-hyperintensity patterns can be seen in the day(s) the typical MRI appearance
after spinal cord infarction (FIGURE 2-5). The lower thoracic cord into the conus in acute, subacute, and
chronic settings.
frequently demonstrates larger cross-sectional lesion areas that do not respect
classic vascular territories. Although identifying typical T2-hyperintense ● A low threshold for MRI of
imaging patterns is helpful, the spectrum can be diverse and atypical. However, the entire spine should exist,
some T2-hyperintensity findings raise a red flag for an etiology other than spinal unless the localization is
cord infarction, including a large lesion out of proportion to mild deficits, signal clear (eg, cervical spinal
cord in quadriplegia).
extending the entire length of the cord, separate well-defined lesions (although Diffusion-weighted
noncontiguous lesions are common), and a small lesion with severe edema. imaging/apparent diffusion
When present (in approximately 40% of cases), gadolinium enhancement in coefficient should be
spinal cord infarction is usually a linear craniocaudal strip (FIGURE 2-6); performed, but the
sensitivity is incomplete and
resolution of enhancement is typically seen within months.7 Adjacent nerve root sometimes takes days to
enhancement (non-nodular) can be seen subacutely (FIGURE 2-6). Specific findings evolve. In the initial hours of
confirming spinal cord infarction include diffusion restriction, vertebral body symptoms, imaging is likely
infarction, and adjacent arterial dissection/occlusion. Well-defined DWI normal or equivocal.
hyperintensity should be confirmed on ADC, especially given the technical
difficulties inherent in DWI of the cord. At times, T2-hyperintense signal in the
anterior spinal artery is seen, suggesting slow flow or thrombus,19 but the specificity
is unclear. It is important to correctly identify vertebral body infarctions; new
well-defined posterior or anterior T2-hyperintense signal, often in a wedge or
triangular shape on axial views, may enhance subacutely. However,
misinterpreting vertebral body hemangiomas and degenerative changes could lead
to misdiagnosis. Rib and muscle infarctions can also rarely be seen.26,27 Dissections
can be difficult to find; therefore, a dissection protocol (eg, cervical MRI with
T1-weighted fat saturation) should be used. Dissections and other mechanical
pathology affecting smaller feeding arteries may be responsible for some idiopathic
cases. Magnetic resonance angiography (MRA) of the spinal canal is currently of
limited value in spinal cord infarction, unless a rare acute presentation of spinal
dural arteriovenous fistula/arteriovenous malformation (AVM) is suspected.
Rarely, large artery27 or long anterior spinal artery occlusions can be found. The
cost and risk of digital subtraction angiography (DSA) likely outweigh its utility in
assessing spinal cord infarction, unless strong concern for an alternative diagnosis
(eg, spinal dural arteriovenous fistula) or a rare etiology (vasculitis) remains.
CHRONIC. Several weeks to months after a spinal cord infarction, differentiating
imaging findings from other causes of myelopathy becomes more difficult.
Although, at times, classic findings of myelomalacia (very bright focal T2
hyperintensity with T1 hypointensity and volume loss) (FIGURE 2-4),7 cord
atrophy, or residual T2 hyperintensity respecting a vascular territory can be
seen, many cases are more difficult to distinguish.
ADDITIONAL TESTS. Many patients with spinal cord infarction are initially
suspected to have Guillain-Barré syndrome. When nerve conduction studies/EMG
and CSF evaluation are obtained, it is important to recognize frequent abnormalities
attributable to spinal cord infarction. In one series, 13 of 19 patients with spinal
cord infarction had EMG abnormalities corresponding to the area of infarction.7,28
CONTINUUMJOURNAL.COM 37
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
FIGURE 2-5
Axial MRI findings of spinal cord infarctions. A variety of axial T2-hyperintense MRI patterns can
be seen in spinal cord infarctions, which are often incomplete, asymmetric, or noncontiguous,
including owl eyes (large [A] or small [B]), hologray (entire gray matter) (C), anteromedial spot
(D), and anterior U or V (E). Infarcts often involve territories other than the typical anterior
two-thirds of the spinal cord, including holocord (entire spinal cord), dorsomedial (F), and
lateral (G). A small focus of bright T2-hyperintense signal (F) accompanied by focal T1
hypointensity (not shown) represents residual cystic myelomalacia as a chronic finding after
infarction. Anterior spinal artery T2 hyperintensity (H) (demonstrated ventral to an anteromedial
spot) is observed in some cases, supporting the presence of a thrombus or slow flow
contributing to ischemia. T1-weighted contrast enhancement highlights the predominant area of
ischemia, which is often an owl-eye pattern (I), and in this example demonstrates associated
ventral root enhancement.
Reprinted with permission from Zalewski NL, et al, J Neurol Sci.19 © 2018 Elsevier BV.
CSF often shows mild to moderate protein elevation, frequently confused for the
albuminocytologic dissociation seen in Guillain-Barré syndrome. In some cases
(<10%),7 mild elevation in inflammatory markers is seen, raising caution for
alternatives, but it is important to note that mild abnormalities can still be
consistent with spinal cord infarction; significant elevations of greater than
25 cells/mm3 would be unlikely.
DIAGNOSIS. Spinal cord infarction diagnostic criteria are outlined in TABLE 2-2.7
Clinicians should err on the side of using a working diagnosis of “possible spinal
cord infarction” acutely, as criterion 4 highlights a workup ensuring alternative
diagnoses are not likely.
38 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINT
● It is reasonable to discuss
risks and benefits of IV
recombinant tissue
plasminogen activator
within the first 4.5 hours
after onset if suspicion of
spinal cord infarction is high
and the patient understands
the limited evidence.
FIGURE 2-6
Confirmatory MRI findings and typical gadolinium enhancement pattern in spinal cord
infarctions. Vertebral body infarction is seen on short tau inversion recovery (STIR) images (A)
with associated gadolinium enhancement (B) of the vertebral body infarct, spinal cord
infarction (C), and anterior cauda equina (D); T1-weighted fat-suppressed images show
cervical artery dissection with significantly decreased left vertebral flow (E, F), with
confirmed intramural hematoma (G) adjacent to spinal cord infarction. Diffusion-weighted
image shows diffusion restriction (H) with correlation on apparent diffusion coefficient (I)
image. Gadolinium enhancement of spinal cord infarction demonstrated with a typical
craniocaudal linear strip on sagittal views (J, K) and corresponding anterior predominant gray
matter (L) and anteromedial spot (M) patterns on axial views, highlighting the predominant
areas of ischemia.
Reprinted with permission from Zalewski NL, et al, JAMA Neurol.7 © 2019 American Medical Association.
TREATMENT. Data on treatment for spinal cord infarction are limited. It is
reasonable to discuss risks and benefits of IV recombinant tissue plasminogen
activator (rtPA) within the first 4.5 hours after onset once the acute myelopathy
algorithm (TABLE 2-1) has been followed and if suspicion of spinal cord infarction
is high and the patient understands the limited evidence. At least 13 cases of the use
of rtPA in spinal cord infarction had been published at the time this article was
written,7,29 many of which described benefit and no significant complications. If
rtPA is not administered, MAP augmentation with or without lumbar drainage can
be considered, as discussed in the periprocedural spinal cord infarction section.
Secondary stroke prevention should focus on the suspected mechanism
(TABLE 2-3). In many cases, the mechanism is not clear, and the focus is on
rehabilitation, reducing vascular risk factors, and maintaining a healthy lifestyle.
Most patients receive antiplatelet therapy, but no evidence has established its use
unless supported by a specific mechanism. In some cases with atherosclerotic risk
factors and stuttering decline, dual-antiplatelet therapy and a high-intensity
statin could be considered.30
CONTINUUMJOURNAL.COM 39
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
MECHANISM. Atherosclerosis, arterial dissection, and fibrocartilaginous embolism
are the most common presumed mechanisms of spontaneous spinal cord
infarction. Patients frequently have thorough evaluations with no clear
mechanism identified. Given the frequent history of various activities occurring
in the context in many cases, mechanical mechanisms should be closely
considered (eg, fibrocartilaginous embolism, dissection, compression of
radicular artery by a disk). Other more diverse mechanisms that are not currently
understood may also exist (eg, arterial vasospasm). Some studies have
demonstrated compressive intersegmental artery mechanisms suspected in
spinal cord infarction and spinal TIAs (eg, diaphragmatic crus syndrome,
endothoracic fascia compression, and disko-osteo-arterial conflict)31; symptoms
related to such lesions could also be related to vasospasm or dissection.31 Many
additional mechanisms of spinal cord infarction have been seen (TABLE 2-3), and
investigations can be individually tailored (TABLE 2-4).
VASCULITIS. Primary angiitis of the central nervous system (CNS), systemic
autoimmune vasculitis (eg, antineutrophil cytoplasmic antibody [ANCA],
giant cell arteritis), infectious vasculitis with or without meningitis
TABLE 2-2 Spinal Cord Infarction Diagnostic Criteriaa
Criteria
1 Acute nontraumatic myelopathy (no preceding progressive myelopathy)
Onset to nadir of severe deficitsb 12 hours or less
If stuttering course is more than 12 hours, severe deficits rapidly develop over 12 hours or less
2 MRI
A No spinal cord compression
B Supportive: intramedullary T2-hyperintense spinal cord lesion
C Specific (one of ): diffusion-weighted imaging/apparent diffusion coefficient restriction,
associated vertebral body infarction, arterial dissection/occlusion adjacent to lesion
3 CSF
Noninflammatory (normal cell count and IgG index and no oligoclonal bands)
4 Alternative diagnoses
Alternative diagnosis is not more likely
Type and diagnostic certainty of spinal cord infarction
◆ Definite spontaneous spinal cord infarction (requires all of the following: 1, 2A, 2B, 2C, 4)
◆ Probable spontaneous spinal cord infarction (requires all of the following: 1, 2A, 2B, 3, 4)
◆ Possible spontaneous spinal cord infarction (requires all of the following: 1, 4)
◆ Definite periprocedural spinal cord infarction (requires all of the following: 1, 2A, 2B, 4)
◆ Probable periprocedural spinal cord infarction (requires all of the following: 1, 4)
CSF = cerebrospinal fluid; IgG = immunoglobulin G; MRI = magnetic resonance imaging.
a
Modified with permission from Zalewski NL, et al, JAMA Neurol.7 © 2019 American Medical Association.
b
A severe acute deficit (motor and/or sensory) typically consists of loss of antigravity strength or worsened
severe objective sensory loss impairing function (eg, severe sensory ataxia).
40 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
(eg, varicella-zoster virus, syphilis, hepatitis), and paraneoplastic vasculitis
(eg, Hodgkin lymphoma) can rarely affect spinal cord vasculature, with
spinal cord infarction, subarachnoid hemorrhage, or hematomyelia. The
spinal cord is usually affected as part of a more widespread presentation (with
or without systemic features), leading to suspicion. A large series of primary
angiitis of the CNS showed spinal cord involvement in 5% of cases; all had
cerebral involvement, one initially presented with myelopathy, and all had
significant CSF pleocytosis.32 In a large series of spontaneous spinal cord
infarction, 1.5% of cases were secondary to vasculitis.7
Etiologies of Spinal Cord Infarctiona TABLE 2-3
Atherosclerosis
Dissection
◆ Aortic dissection
◆ Vertebral artery dissection
◆ Subclavian artery dissection
Mechanical
◆ Fibrocartilaginous embolism
◆ Surfer’s myelopathy
◆ Arterial compression (disk, other)
Embolic
◆ Fibrocartilaginous embolism
◆ Aortic embolism (eg, atheroma, calcium)
◆ Cardioembolic (eg, atrial fibrillation, endocarditis, myxoma, fat, paradoxical)
◆ Fungal embolus
Vasculitis
◆ Primary angiitis of the central nervous system
◆ Systemic vasculitis (eg, giant cell arteritis)
◆ Infectious (eg, varicella-zoster virus, syphilis, fungal, schistosomiasis, Lyme disease,
tuberculous meningitis, hepatitis)
Hypotension
Hypercoagulability
◆ Lupus anticoagulant/antiphospholipid antibody syndrome
◆ Malignancy
◆ Sickle cell disease, hereditary spherocytosis, polycythemia vera
◆ Disseminated intravascular coagulation
Pharmacologic
◆ Medications (sildenafil, oral contraceptives, phentermine, others)
◆ Drugs of abuse (eg, cocaine, cannabis)
a
Modified with permission from English SW, Zalewski NL, Semin Neurol.9 © 2021 Thieme Medical Publishers, Inc.
CONTINUUMJOURNAL.COM 41
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
TABLE 2-4 Evaluation of a Spinal Cord Infarctiona
Standard evaluation
◆ Imaging
◇ MRI cervical/thoracic spine (with diffusion-weighted imaging/apparent diffusion
coefficient and gadolinium, with or without brain MRI)
◇ Magnetic resonance angiography (MRA) cervical (if cervical level affected, with T1 fat
saturation for dissection)
◆ Blood tests
◇ Hemoglobin A1c, fasting lipids, glucose
◇ Complete blood cell count, prothrombin time/activated partial thromboplastin time
◆ CSF (can consider deferring if clear diagnosis)
◇ Cell count, glucose, protein, IgG index, oligoclonal bands
Additional testing to consider
◆ Imaging
◇ MRI brain (evaluate for concurrent stroke, alternative lesions)
◇ MRA spinal canal or angiogram (clinical/radiographic concern for spinal dural
arteriovenous fistula/arteriovenous malformation, or vasculitis)
◇ CT chest/abdomen/pelvis (malignancy concern)
◆ Blood
◇ Aquaporin-4-IgG, myelin oligodendrocyte glycoprotein (MOG)-IgG
◇ Syphilis and Lyme serology
◇ Hypercoagulable profile
◇ Erythrocyte sedimentation rate, C-reactive protein
◇ Antinuclear antibody, extractable nuclear antigen, antineutrophil cytoplasmic antibody
panel, dsDNA
◇ Paraneoplastic autoantibody evaluation
◇ Toxicology screen (with urine)
◆ CSF
◇ Varicella-zoster virus polymerase chain reaction (PCR)
◇ Venereal Disease Research Laboratory test
◇ Lyme serology/PCR
◇ Cryptococcus antigen
◆ Cardiac evaluation
◇ Transesophageal echocardiogram
◇ Holter monitoring
◆ Other
◇ EMG (suspicion of Guillain-Barré syndrome)
◇ Temporal artery biopsy (concern of giant cell arteritis)
CSF = cerebrospinal fluid; CT = computed tomography; dsDNA = double-stranded deoxyribonucleic acid;
EMG = electromyography; IgG = immunoglobulin G; MRI = magnetic resonance imaging.
a
Modified with permission from English SW, Zalewski NL, Semin Neurol.9 © 2021 Thieme Medical Publishers, Inc.
42 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
LONG-TERM FOLLOW-UP AND PROGNOSIS. Outcomes after spontaneous spinal cord KEY POINTS
infarction are variable. Despite severe deficits, approximately 50% of patients
● Atherosclerosis, arterial
ultimately ambulate without a gait aid.7 Residual neurogenic bowel/bladder and dissection, and
neuropathic pain are common. Examination may demonstrate lower motor fibrocartilaginous embolism
neuron dysfunction (eg, atrophy), depending on lesion location.27 Long-term are the most common
recurrence of spontaneous spinal cord infarction (outside of an initial stuttering presumed mechanisms of
spontaneous spinal cord
presentation) is exceedingly rare.7
infarction.
Spinal Cord Transient Ischemic Attack ● Outcomes after
Spinal cord TIAs are questioned at times in patients with spells affecting bilateral spontaneous spinal cord
infarction are variable.
limbs. TIAs can be difficult to prove, even in cerebrovascular disease, with a
Despite severe deficits,
number of mimickers. Working around limitations, a recent study found 4 of 133 approximately 50% of
patients (3%) who ultimately had a spontaneous spinal cord infarction and patients ultimately ambulate
initially experienced spinal cord TIAs.33 Traditional vascular risk factors were without a gait aid.
seen in 75% of patients; the patients developed spinal cord infarction in the same
● The incidence of spinal
distribution as their spinal cord TIAs, and all had experienced multiple spinal dural arteriovenous fistula is
cord TIAs. Symptoms lasted from seconds to minutes before return to baseline. 5 to 10 cases per million per
No patients had pain as a feature. Spinal cord TIA is different than the stuttering year. An older population is
decline frequently seen in spinal cord infarction (23% of cases), in which deficits typical (40 to 80 years), with
male predominance (80%),
fluctuate but accumulate. Given the rarity of spinal cord TIAs, physicians should and patients frequently
carefully consider alternatives. report previous back
surgeries or trauma that may
VENOUS ISCHEMIA contribute to the
development of a fistula.
Venous ischemia of the spinal cord is predominantly caused by spinal dural
arteriovenous fistula, but other mechanisms should also be considered. ● The clinical presentation
of spinal dural arteriovenous
Spinal Dural Arteriovenous Fistula fistula typically includes a
gradually progressive
Spinal dural arteriovenous fistulas (Anson-Spetzler type I AVMs) comprise 70%
thoracic myelopathy with
of spinal AVMs. This arteriovenous shunt is composed of a connection between leg weakness/numbness,
a radiculomeningeal artery and single radicular vein, typically in the neural bowel/bladder dysfunction,
foramen, leading to arterialization of the vein, venous hypertension, spinal cord symptoms frequently
congestion, and venous ischemia.34,35 The incidence of spinal dural arteriovenous referable to the conus/roots,
and episodic worsening
fistula is 5 to 10 cases per million per year.36-40 An older population is typical with exertion/Valsalva. The
(40 to 80 years), with male predominance (80%), and patients frequently strongest clinical clue is
report previous back surgeries or trauma that may contribute to the dramatic worsening of
development of a fistula.36,37 A number of cases of spinal dural arteriovenous deficits with activities
elevating venous pressure,
fistula have been demonstrated less than 2 years after spine surgery such as exertion, Valsalva,
(cervical, thoracic), in which clear evidence of a structural spine disease or lumbar puncture.
initially contributing and no preoperative evidence of spinal dural arteriovenous
fistula were seen.41
CLINICAL FEATURES. Clinical presentation typically includes a gradually
progressive thoracic myelopathy with leg weakness/numbness, bowel/bladder
dysfunction, symptoms frequently referable to the conus/roots, and episodic
worsening with exertion/Valsalva (CASE 2-2). Pain is frequent (back or
radicular).37 Acute paraplegia (in approximately 2% to 5% of cases) and stepwise
deterioration (in 11% to 32% of cases) can occur.22,24,36,37,42-44 A sensory level
is reported in 18% to 37% of cases, most frequently at L1.43,45 The strongest
clinical clue is dramatic worsening of deficits with activities elevating venous
pressure, such as exertion, Valsalva, or lumbar puncture.46 Patients are
CONTINUUMJOURNAL.COM 43
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
frequently given corticosteroids for suspected alternatives, and 50% of
patients can have significant worsening4 (venous hypertension)4,47; this is
a strong diagnostic clue. Inadvertent improvement with plasma exchange has
also been described.48 Features are often mistaken for peripheral localization
(eg, cauda equina), relating to a frequent lack of upper motor neuron signs36,44
with progressive lower motor neuron injury at the level of the conus/roots.
At diagnosis, 70% of patients have both upper motor neuron and lower motor
findings.49 Cervical myelopathy presentations with similar radiographic and
clinical features can be seen (2% of cases).36,41,50 Rarely, spinal dural
arteriovenous fistula can be an incidental finding.51
CASE 2-2 A 62-year-old man was referred for evaluation of “transverse myelitis.”
He reported 9 months of progressive weakness and sensory loss of the
right more than left leg. Walking resulted in dramatic worsening of
weakness. His past medical history included hypertension,
hyperlipidemia, and lumbar spine surgery 5 years earlier.
Examination demonstrated moderate asymmetric right more than left
leg weakness, with severe sensory loss to all modalities in the lower
extremities and no truncal sensory level. Reflexes were reduced, and
plantar responses were mute. Nerve conduction studies and EMG were
performed, revealing a lumbosacral polyradiculopathy; however, MRI of
the lumbar spine revealed T2-hyperintense signal extending into the
conus, with further imaging demonstrating T2-hyperintense signal
throughout the lower thoracic cord (FIGURE 2-7A). Multiple small
T2-hypointense flow voids were seen surrounding the cord (FIGURES 2-7A
and 2-7B), and T1-weighted imaging with gadolinium demonstrated abrupt
missing pieces within a confluent area of enhancement (FIGURES 2-7C
and 2-7D); these findings were suspicious for spinal dural arteriovenous
fistula. Digital subtraction angiography demonstrated a fistula at the right
T10 intercostal artery. Surgical obliteration was successful, and the
patient had clinical stabilization.
COMMENT This case highlights the importance of recognizing exertional or
Valsalva-induced worsening of deficits and concurrent findings of lower
motor neuron involvement in spinal dural arteriovenous fistula. Expansile
T2-hyperintense signal into the conus with accompanying flow voids and
the missing piece sign are characteristic features of spinal dural
arteriovenous fistula. A diagnosis is confirmed with digital subtraction
angiography, and treatment includes endovascular or surgical obliteration.
44 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
NEUROIMAGING. Spinal cord T2-hyperintense signal is present in approximately
95% of cases,45 is often longitudinally extensive (three or more vertebral body
segments), and frequently extends to the conus (90% of cases) (FIGURE 2-8).
T2 hyperintensity can be faint, but a large lesion with edema is typical; atrophy
can be seen in delayed diagnoses. Flow voids (engorged perimedullary veins)
are seen on the dorsal more than the ventral surface of the cord in approximately
80% of cases. They are typically demonstrated on T2-weighted imaging but
can also be seen better, at times, on T1-weighted imaging with gadolinium45,52,53;
heavily T2-weighted myelographic sequences (eg, phase-cycled fast imaging
employing steady state acquisition [PC-FIESTA], three-dimensional constructive
FIGURE 2-7
Imaging of the patient in CASE 2-2. Sagittal (A)
and axial (B) T2-weighted MRIs show
T2-hyperintense signal and edema throughout the
lower thoracic cord. Multiple small T2-hypointense
flow voids are seen surrounding the cord (A, blue arrow;
B, arrows). Sagittal (C) and axial (D) T1-weighted
images with gadolinium show abrupt missing
pieces (C, arrows) within a confluent area of
enhancement. These findings are suspicious for
spinal dural arteriovenous fistula.
CONTINUUMJOURNAL.COM 45
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
FIGURE 2-8
MRI findings in spinal dural arteriovenous fistula. Sagittal (A) and axial (B) T2-weighted thoracic
spine images reveal longitudinally extensive holocord (entire spinal cord) T2 hyperintensity (A,
B, arrows) extending to the conus with associated flow voids along the ventral and dorsal cord
surface (A, B, arrowheads). Sagittal (C) and axial (D) postcontrast T1-weighted images show
the missing piece sign (C, D, arrowheads), with a well-defined abrupt segment of gadolinium
enhancement missing amid an otherwise homogenous, avid enhancing area (C, D, arrows)
Sagittal postcontrast T1-weighted image (E) reveals another frequent enhancement pattern
with hazy enhancement (arrow) and central canal predominance (arrowhead).
Reprinted with permission from English SW, Zalewski NL, Semin Neurol.9 © 2021 Thieme Medical Publishers, Inc.
interference in steady state [CISS], or T2 sampling perfection with
application-optimized contrasts using different flip-angle evolution [SPACE])
should be requested as they may improve the yield of demonstrating flow voids.
As a general rule, high-quality MRI of the entire spine without T2-hyperintense
signal or flow voids reliably excludes spinal dural arteriovenous fistula.52,54 Flow
voids can also be seen with tumors (eg, hemangioblastoma, paraganglioma) and
other AVMs. Mild prominence of nontortuous vasculature in the lower
thoracolumbar cord is common and not pathologic. Gadolinium enhancement of
the spinal cord is common (65% to 85% of cases), and clinicians should not be
misled to suspect an inflammatory or neoplastic etiology when features are
suspicious for spinal dural arteriovenous fistula. A variety of gadolinium
enhancement patterns can be seen, commonly referred to as hazy heterogeneous
patterns throughout, although the missing piece sign or hazy with central canal
prominence pattern is helpful, when present.44,55
46 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Although DSA is the gold standard to identify a fistula, a noninvasive spinal KEY POINTS
MRA can initially be considered. The typical detection on MRA of the spinal
canal may be as high as 80% to 95% and can help localize the fistula level ● Inappropriate
corticosteroid use for
within one to two segments in approximately 95% of cases, but updated
suspected alternative
technology and an experienced neuroradiologist can increase the sensitivity diagnoses can lead to
and specificity.56-58 DSA has a very high sensitivity in detecting spinal dural clinical worsening in spinal
arteriovenous fistula with an experienced angiographer; however, evaluation is dural arteriovenous fistulas
not perfect, as seen in a review of 53 cases with delayed diagnosis that showed 19% from exacerbation of venous
had previously “normal” angiograms (incomplete angiogram or retrospectively hypertension and thus
should be avoided.
demonstrated). Some cases had multiple negative angiograms and discovery of a
fistula after durotomy.55 Fistula visualization may be compromised by ● Spinal cord
atherosclerosis of segmental arteries or thrombosis of veins.59 Intracranial T2-hyperintense signal is
localization with four-vessel angiography should be considered,60,61 particularly present in approximately
for cervical cases. Feeder vessels from the pelvis may also be identified. 95% of cases of spinal dural
arteriovenous fistula, is
often longitudinally
ADDITIONAL TESTS. Lumbar puncture should be avoided when spinal dural
extensive (three or more
arteriovenous fistula is strongly suspected.46 When obtained, findings generally vertebral body segments),
reveal noninflammatory CSF; however, dramatic inflammation with pleocytosis has and frequently extends to
been seen.62 Polyradiculopathy may be seen on nerve conduction studies and EMG.63 the conus (90% of cases).
● Flow voids (engorged
TREATMENT. Treatment options for spinal dural arteriovenous fistula include
perimedullary veins) are
embolization of the fistula via DSA (approximately 70% to 80% efficacy) or seen on the dorsal more
surgical disconnection of the draining vein (98% efficacy).4,64-66 Embolization via than the ventral surface of
DSA offers the advantage of avoiding surgery and treating at diagnosis; however, the cord in approximately
80% of cases of spinal dural
failure rates are higher, and complexity may be too high of a risk in some.
arteriovenous fistula.
LONG-TERM FOLLOW-UP AND PROGNOSIS. Improvement (>40% of cases) or ● Gadolinium enhancement
stabilization (>30% of cases) is expected after treatment. The strongest predictor of the spinal cord is common
of outcome is clinical severity before treatment.67 Follow-up MRI is commonly in spinal dural arteriovenous
fistula, and clinicians should
obtained approximately 3 months after treatment and may show persistent T2 not be misled to suspect an
hyperintensity or enhancement, but enlarged perimedullary vessels should not inflammatory or neoplastic
be seen and raise concern for treatment failure. Ultimately MRI shows significant etiology when features are
improvement or resolution of T2-hyperintense signal in 80% of patients.67 suspicious for spinal dural
arteriovenous fistula.
Spinal Epidural and Pial Arteriovenous Fistulas ● Although digital
Spinal epidural arteriovenous fistula results from an anomalous connection between subtraction angiography is
paraspinal or paravertebral arteries and the epidural venous plexus and typically the gold standard to identify
a fistula, a noninvasive spinal
presents as a slowly progressive venous congestive myelopathy.68 Additional features
magnetic resonance
may include compression of the cord or nerve roots from venous distention. Patients angiogram can initially be
may have an osseous or nonosseous spinal epidural arteriovenous fistula.69 Lesions considered to potentially
are commonly located in the cervical or upper thoracic level, and MRI findings mirror help localize the fistula
spinal dural arteriovenous fistula with the addition of possible vascular engorgement before the formal
angiography.
of the epidural space. Angiogram demonstrates involvement of the epidural venous
plexus, often with a venous pouch.68 Pial arteriovenous fistulas (superficial intradural
with direct shunt between spinal cord arteries and veins) are rare AVMs typically
found anteriorly near the conus that also present with venous congestive
myelopathy (60% of cases), whereas others present with hemorrhage (35%).70
Other Arteriovenous Malformations
Other spinal and paraspinal AVMs can also present with venous congestive
myelopathy mirroring spinal dural arteriovenous fistula, although other clinical
CONTINUUMJOURNAL.COM 47
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
presentations (eg, hematomyelia) generally predominate given the location of
the arteriovenous shunt and friable vessels.
Miscellaneous Causes of Venous Ischemic Myelopathy
Behçet disease is a systemic vasculitis with significant venous involvement.
Pathology/thrombus in spinal cord venous structures is postulated in some
patients.
Other unusual causes of venous congestive myelopathy have been reported.
Any process inhibiting venous outflow from the intrinsic veins of the spinal cord
through the caval system and to the heart could result in venous congestive
myelopathy. Inferior vena cava thrombosis,71 spinal cord compression from an
enlarged vena cava,72 and caustic ingestion with mediastinitis and venous
congestion have been seen as unusual mechanisms of myelopathy,73 whereas
obstruction of the inferior vena cava from congenital variants or thrombosis has
also been seen with polyradiculopathy.74-76 Cases of extraspinal arteriovenous
fistulas occur as well.77,78 Rare reports of a prothrombotic state with venous
thrombosis (eg, pelvic vein thrombosis, cancer, sepsis),79 epidural infection
leading to venous thrombosis, spinal cavernous malformations with recurrent
hemorrhage increasing venous congestion,80 and nitrogen emboli of the
venous system81 are additional causes of venous ischemia. Spinal cord
compression from anomalous arteries (eg, vertebral arteries) with associated
syrinx has been reported.82 A study with biopsies revealing venous congestive
myelopathy ultimately demonstrated spinal dural arteriovenous fistula in only
three of seven cases, suggesting difficulty in diagnosis or incompletely
understood mechanisms.
HEMATOMYELIA
Intraparenchymal spinal cord hemorrhage (hematomyelia) is very rare. Trauma
is the most common cause,83 followed by intramedullary spinal cord cavernous
malformation and AVMs; many additional causes are also been reported.
Hematomyelia presents similarly to spinal cord infarction, frequently with
severe back pain at onset (localizing the hemorrhage) followed by rapid severe
myelopathy deficits; however, deficits can often progress over days instead of
hours. Recognition of blood products within the spinal cord on MRI (T1
hyperintensity, dark T2 hypointensity, gradient recalled echo [GRE]
hypointensity) is critical as it significantly shifts the differential diagnosis and
acute management toward a focus on hematomyelia.
Cavernous Malformation
Intramedullary spinal cord cavernous malformations are likely the most common
etiology of nontraumatic hematomyelia. Cerebral cavernous malformations are
nonshunting vascular malformations found in about 0.5% of the general
population,84-86 whereas intramedullary spinal cord cavernous malformations
represent approximately 5% of all cavernous malformations in the CNS.87 Only
5% of patients with an intracranial cavernous malformation have an
intramedullary spinal cord cavernous malformation, whereas approximately 25%
of patients with intramedullary spinal cord cavernous malformations have an
intracranial cavernous malformation.86 A cavernous malformation is a cluster of
tightly packed dilated sinusoidal veins with no intervening parenchyma and no
feeding artery or draining vein. Lesions occur not only in the spinal cord but also
48 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
within nerve roots. Intramedullary spinal cord cavernous malformations have a KEY POINTS
slight male predominance, with median age of presentation in the fourth
● Treatment options for
decade.86,88 Cavernous malformations are now generally understood to develop spinal dural arteriovenous
over a lifetime. Most cases of intramedullary spinal cord cavernous fistula include embolization
malformations are spontaneous, but a familial history is present in approximately of the fistula via digital
10% of cases or as high as 50% in patients with multiple cavernous subtraction angiography or
surgical disconnection of
malformations89; radiation and trauma are other common predisposing factors.
the draining vein.
Intramedullary spinal cord cavernous malformation most commonly presents Improvement or stabilization
clinically with acute hematomyelia86 and carries an average hemorrhage risk of is expected after treatment.
approximately 1% to 5% per year per cavernous malformation. Annual
hemorrhage rates as high as 10% can be seen with localizing symptoms or prior ● Intraparenchymal spinal
cord hemorrhage
episodes of hemorrhage,86 and lesions larger than 1 cm in size are also at higher (hematomyelia) is very rare.
risk of bleeding. Hemorrhage rates may be as low as 0.8% with incidental Trauma is the most common
intramedullary spinal cord cavernous malformation.86 Significant back or cause, followed by
radicular pain at the site of hemorrhage is reported in 20% to 30% of patients86,88; intramedullary spinal cord
cavernous malformations
isolated episodes of pain without neurologic deficits may be seen (CASE 2-3). and arteriovenous
Strenuous activity before onset is reported in approximately 30% of patients.86 malformations; many
Myelopathy deficits can have a range of severity, depending on the extent of additional causes have also
hemorrhage. Some patients have progressive deficits due to venous been reported.
microhemorrhage with compression of the surrounding spinal cord, a stepwise
● A well-defined lobulated
presentation with recurrent hemorrhage, or a mixture of acute and progressive masslike lesion within the
decline. Symptoms may worsen during pregnancy or the puerperium or parenchyma of the spinal
with trauma.8 cord with heterogeneous
T1- and T2-weighted signal
It is important to understand the radiographic characteristics of
intensity surrounded by a
intramedullary spinal cord cavernous malformation and findings of recent well-defined dark
hemorrhage to further define the likelihood of intramedullary spinal cord T2-hypointense rim
cavernous malformation contributing to a patient’s symptoms. A well-defined (hemosiderin deposition)
lobulated masslike lesion within the parenchyma of the spinal cord with with classic popcorn
appearance is typical of an
heterogeneous T1- and T2-weighted signal intensity surrounded by a intramedullary spinal cord
well-defined dark T2-hypointense rim (hemosiderin deposition) (FIGURE 2-10) cavernous malformation,
with a classic popcorn appearance is typical, which can be best appreciated with which can be best
GRE and susceptibility-weighted imaging (SWI). Usually little perilesional appreciated with gradient
recalled echo and
edema and minimal/absent gadolinium enhancement are seen in stable lesions. susceptibility-weighted
Calcifications are less common in intramedullary spinal cord cavernous imaging.
malformations than in cerebral cavernous malformations. Size varies from 2 mm
to 3 mm to several in centimeters in diameter.90 The presence of bright ● Management of
intramedullary spinal cord
T1-hyperintense signal and perilesional edema are helpful radiographic features
cavernous malformation is
suggesting recent hemorrhage in cavernous malformations,91 with less focused on avoiding further
distinctive features specifically for cavernous malformations in the acute setting, deterioration with recurrent
which can make initial diagnosis difficult. No strong predisposition for the hemorrhage; observation is
typically recommended for
cervical or thoracic spinal cord is seen. Lesions are angiographically occult, but
asymptomatic cavernous
DSA is still often performed for assessment of alternatives. malformations or those with
Management of intramedullary spinal cord cavernous malformation is minimal symptoms.
focused on avoiding further deterioration with recurrent hemorrhage;
observation is typically recommended for asymptomatic cavernous
malformations or those with minimal symptoms.92 In patients with progressive
neurologic deterioration, surgical resection is recommended. Symptomatic
improvement (in approximately 30% of patients) is possible with careful patient
selection for surgical resection,86 but the majority of patients benefit from
stabilization, even with an incomplete resection.86,88 Favorable factors for
CONTINUUMJOURNAL.COM 49
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
surgical benefit include surgery less than 3 months after symptom onset,88
cavernous malformation size greater than 1 cm, and predominantly motor
symptoms, which along with gross total resection via hemilaminectomy can be
predictive of improved neurologic outcome. Preoperative sensory symptoms and
pain may be predictive of poor postoperative improvement. Various data have
been reported on radiosurgery in cerebral cavernous malformations, yet it
remains unclear whether it has any demonstrable benefit in the management of
intramedullary spinal cord cavernous malformations.90
Arteriovenous Malformation
An arteriovenous shunt comprises a direct connection between feeding arteries
and vein(s) without an intervening capillary network. When an arteriolovenular
network (nidus) transitions between feeding artery(s) and vein(s), it is referred
to as an AVM. When a direct connection exists between the main arterial feeder(s)
and a single vein, it is termed an arteriovenous fistula. Although spinal dural
arteriovenous fistula (type I) comprises 70% of spinal arteriovenous shunts, 30%
of cases are secondary to types II through V: intramedullary glomus AVM (type
CASE 2-3 A 50-year-old woman presented with abrupt-onset neck pain and upper
extremity weakness. Her pain became progressively more severe over
days, extending into her shoulders. Within a few more days, the pain
extended into her left arm and was accompanied by a loss of strength.
She also developed left-sided ptosis. An MRI of the cervical spine was
obtained and revealed blood in the left anterior spinal cord between C6
and C8. Symptoms were observed over several weeks, and her ptosis
resolved and left arm strength returned to normal.
Over the next few years of observation, she developed many episodes
of recurrent neck and upper extremity pain lasting hours to weeks, with
altered dysesthetic sensation and contact allodynia. Neuroimaging
findings were consistent with a cavernous malformation (FIGURE 2-9).
Surgical resection was performed, and the patient had a good outcome,
with improvement in symptoms.
COMMENT Hematomyelia is an important cause of acute myelopathy that frequently
presents with significant pain and a range in severity of accompanying
neurologic deficits. Of note, this patient had an accompanying Horner
syndrome, important to recognize as an occasional feature in acute
cervical myelopathy damaging descending first-order neurons in the
sympathetic tracts. Intraparenchymal blood products were identified by
the presence of mixed dark T2 hypointensity and T1 hyperintensity. A
well-demarcated dark T2-hypointense rim around the small masslike lesion
was typical of intramedullary spinal cord cavernous malformation, the most
common cause of hematomyelia. Recurrent symptoms attributable to the
intramedullary spinal cord cavernous malformation were an appropriate
indication to pursue surgical resection with the goal of preventing further
hemorrhage.
50 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
II), intramedullary juvenile AVM (type III), perimedullary AVF (type IV), and
extradural AVF (type V).93 To simplify for the purpose of this article, types II
through V are referred to as spinal AVM, although clinical and radiographic
differences exist between types, as mentioned earlier with discussion of
perimedullary arteriovenous fistula. Notably, a spinal cord aneurysm is associated
with 30% to 40% of spinal AVMs.94 Brain AVMs have an incidence of 1.3 per
100,000 patient-years, 10 times more common than spinal AVMs.95 Spinal
AVMs most commonly present in the third or fourth decades, with no clear
gender predilection. These malformations are associated with genetic
syndromes including germinal (hereditary hemorrhagic telangiectasia,
capillary malformation-AVM syndrome) and somatic (Cobb syndrome;
Klippel-Trenaunay-Weber syndrome; and congenital lipomatous overgrowth,
vascular malformations, and epidermal nevi syndrome) mutations.70 Spinal
arteriovenous metameric syndrome involves vascular malformations of multiple
tissue layers from skin to spinal cord, likely caused by a somatic mutation. Cobb
syndrome demonstrates arteriovenous abnormalities involving all tissue layers of a
metameric segment.70
FIGURE 2-9
Imaging of the patient in CASE 2-3. Sagittal T2-weighted (A) and T1-weighted (B) MRI of the
cervical spine shows hematomyelia with mixed T2 hypointensity (A, arrow) and T1
hyperintensity (B, arrow). Corresponding axial T2-weighted images (C, D) show a
well-demarcated T2-hypointense rim (C, arrow; D, arrow) around the masslike lesion,
typical of intramedullary spinal cord cavernous malformation.
CONTINUUMJOURNAL.COM 51
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
FIGURE 2-10
MRI findings in hematomyelia and extraparenchymal hemorrhage. Sagittal (A) and axial (B)
T2-weighted cervical spine MRIs show intramedullary and extramedullary flow voids consistent
with spinal arteriovenous malformation. Sagittal (C) and axial (D) T2-weighted thoracic spine
images reveal a mixed-signal central lesion with surrounding dark T2-hypointense rim
(C, D, arrows) typical of a cavernous malformation. Sagittal (E, G) and axial (F, H) T2-weighted
MRIs of the cervical spine reveal an extramedullary mixed T2-hyperintense and T2-hypointense
signal dorsal to the cord (E, F, arrows) representative of anticoagulation-associated
subdural hematoma, with concurrent subarachnoid hemorrhage best appreciated on axial
view (H, arrow) and associated cord edema with T2-hyperintense signal on sagittal views (G).
Reprinted with permission from English SW, Zalewski NL, Semin Neurol.9 © 2021 Thieme Medical Publishers, Inc.
The predominant clinical presentation of spinal AVM is acute myelopathy
secondary to hematomyelia (50%).96 Pain is frequent at onset; the deficits are
typically acute and can evolve over days. Other mechanisms contributing to
clinical decline include subarachnoid hemorrhage (SAH), compression from
mass effect (venous dilations, pouches, or, less likely, aneurysms), arachnoiditis
with scarring and occlusion of small vessels causing arterial ischemia,8 and
venous thrombosis with ischemia.22,42,94 Most patients (>75%) will show
favorable spontaneous recovery in the early period after acute symptoms of
hematomyelia.97 The annual hemorrhage risk in spinal AVM is 4%, with the rate
of recurrent hemorrhage higher at 10%.22,96 Patients can also present with
radiculopathy, typically because of compression by a dilated epidural vein.70
Vascular steal and high-output heart failure have rarely been suggested.70
The predominant diagnostic feature on MRI is the presence of intramedullary
flow voids (FIGURE 2-10A). As discussed earlier, it is important to look for an
accumulation of blood products with mixed T1 and T2 signal changes, dark T2
52 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
hypointensity, and active/recent blood products with T1-hyperintense signal. KEY POINTS
Prior hemorrhage can reveal cavitation, localized swelling, or atrophy in chronic
● Although spinal dural
cases. DSA confirms the presence of an AVM, defines its angioarchitecture, and arteriovenous fistula (type I)
helps plan treatment. comprises 70% of spinal
The complexity of approaching a spinal AVM should be handled by an arteriovenous shunts, 30% of
experienced angiographer and neurosurgeon. Treatment strategies are cases are secondary to
types II through V:
controversial given the rarity of spinal AVMs, and disabling deficits can occur as
intramedullary glomus
a complication of treatment in 5% to 25% of patients.97 Emergent surgery is often arteriovenous malformation
avoided because of complicating factors in acute hematomyelia and because of (type II), intramedullary
the natural history of early improvement in most patients.98 The largest natural juvenile arteriovenous
malformation (type III),
history study suggests more than 70% of patients deteriorate within 4 years
perimedullary arteriovenous
(more common early), and thus earlier treatment is generally recommended.97 fistula (type IV), and
Endovascular embolization, surgical resection, and radiosurgery are options. extradural arteriovenous
Even partial treatment can reduce hemorrhage risk; therefore, combination or fistula (type V).
staged treatment approaches are often planned.96,99,100 After treatment, the
● The predominant clinical
annual hemorrhagic risk is generally absent with complete obliteration and drops presentation of spinal
to 3% for partial treatment.96,101 Endovascular treatment is typically preferred arteriovenous malformation
because of the high risk for intraoperative complications.96 Surgical resection is acute myelopathy
may be preferred in posterolaterally located AVMs fed by radial arteries from secondary to hematomyelia.
the posterior spinal artery.70 Stereotactic radiosurgery may be considered in
some cases with favorable anatomy and may be used in addition to endovascular
treatment.102
Other Causes of Hematomyelia
Beyond the two most common identifiable causes of hematomyelia
(intramedullary spinal cord cavernous malformation and AVM), many other
mechanisms have been reported. TABLE 2-5 provides a representative overview
of categorization.
Spinal cord aneurysms present more commonly with spinal SAH than
hematomyelia. Anticoagulants have been associated with hematomyelia.
Bleeding diatheses (eg, von Willebrand disease, factor VIII/VII/XI deficiencies)
have been noted in some cases.103,104 Gowers intrasyringal hemorrhage is a rare
syrinx-related hemorrhage.105 Spinal dural arteriovenous fistula, vasculitis, and
radiation with or without thrombocytopenia are other mechanisms.83 A
component of hemorrhagic transformation after spinal cord infarction can
sometimes be seen. The question of a possible inflammatory or infectious
etiology is sometimes raised in cases without an identifiable cause, but clear
associations are very unusual and rarely reported. Longitudinally extensive
transverse myelitis with associated hemorrhage has been reported
postinfluenza,106 in addition to cases associated with varicella-zoster virus and
herpes simplex type 2 infections, more typically in immunocompromised
adults.107-109 Acute hemorrhagic leukoencephalitis has also been reported with
spinal cord involvement.110 Small asymptomatic capillary telangiectasias have
reported in the spinal cord111 but would not be expected with clinical
hematomyelia. Despite extensive evaluations, a number of hematomyelia cases
have an indeterminate mechanism.
EXTRAPARENCHYMAL SPINAL HEMORRHAGE
Extraparenchymal hemorrhage of the spinal canal is categorized into SAH,
subdural hemorrhage, and epidural hematoma (most common).
CONTINUUMJOURNAL.COM 53
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
Epidural Hematoma
Spinal epidural hematoma is most commonly encountered in trauma or after
surgery, epidural catheterization, or lumbar puncture. Epidural hematoma is
estimated to be approximately 4 times more common than subdural hematoma.8
In the postsurgical setting, deficits may be present immediately after surgery or
develop in the subsequent hours to days. Symptomatic postsurgical epidural
hematoma involves significant motor deficits in 80% of patients or isolated
intractable pain in 20% of patients.112 Other diagnostic possibilities should also be
considered, with new severe myelopathy immediately post–spinal surgery
occurring in approximately 0.2% of patients,113 including inadequate
decompression, spinal cord ischemia, graft/cage dislodgement, or presumed
direct surgical trauma. A prospective study routinely evaluating for the
radiographic presence of spinal epidural hematoma within 2 to 5 days of lumbar
decompression demonstrated spinal epidural hematoma with thecal sac
compression in 58% of patients; none had new deficits, highlighting that spinal
epidural hematoma can be an asymptomatic finding.114
The incidence of spontaneous spinal epidural hematoma is much rarer than
postsurgical spinal epidural hematoma, estimated at 0.1 per 100,000
person-years.115 Notably, radicular pain is common at onset.8 Attributable causes
are usually secondary to coagulopathy (eg, anticoagulation, liver disease, or
portal hypertension). Epidural hematomas have been described after
exertion/straining and venous thoracic outlet syndrome116 and as a rare
phenomenon of dural and epidural arteriovenous malformations.117,118
TABLE 2-5 Hematomyelia
Hematomyelia etiologies Helpful features
Trauma Most common cause of hematomyelia
Cavernous malformation Common cause of hematomyelia; young male patient;
heterogeneous lobular mass, popcorn appearance with dark
rim of T2 hypointensity; pain frequently precedes
myelopathy deficits
Arteriovenous malformation Common cause of hematomyelia; young patient;
intramedullary flow voids
Bleeding diatheses and medications Prior history of bleeds; family history; contributing
medications or supplements
Neoplasm Focal masslike component not typical of intramedullary
spinal cord cavernous malformation; history of primary
neoplasm; contrast enhancement
Miscellaneous Rare; typical radiographic and clinical features for
respective disorders
(spinal cord aneurysm, intrasyringal hemorrhage, vasculitis,
radiation, infection [eg, postinfluenza, varicella-zoster
virus, herpes simplex virus type 2, acute hemorrhagic
leukoencephalitis], checkpoint inhibitor)
Idiopathic Common diagnosis of exclusion in hematomyelia;
hypertension as typical risk factor
54 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Degenerative disk disease has been questioned as a contributing factor, and KEY POINTS
sometimes no mechanism is found.
● Spinal epidural hematoma
High-resolution CT of the spine is often the initial imaging modality; however, is most commonly
MRI has better sensitivity and provides detailed information regarding the extent encountered in trauma or
of compression for surgical planning. Acute spinal epidural hematoma is after surgery, epidural
hyperdense on CT, whereas MRI patterns vary depending on timing. T1 signal catheterization, or lumbar
puncture.
will be isointense acutely and become more hyperintense in the subacute phase.
Conversely, hemorrhage will appear hyperintense on T2-weighted sequences in ● Treatment of
the first 12 hours but become hypointense in the subsequent acute and subacute symptomatic spinal epidural
phase (FIGURE 2-10). Chronic spinal epidural hematoma will be both T1 and T2 hematoma is emergent
hypointense. Heterogeneous patterns are often seen with anticoagulation-related surgery, with improved
outcomes when performed
hemorrhage. In contrast to epidural abscesses, gadolinium enhancement is not within 12 hours of symptom
expected in spinal epidural hematoma. onset.
Similar to management of other hemorrhages, reversal of any contributing
coagulopathy should be performed immediately, and any contributing
medications should be discontinued. Treatment of symptomatic spinal epidural
hematoma is emergent surgery, with improved outcomes when performed
within 12 hours of symptom onset.119 If patients are asymptomatic or have
minimal deficits, conservative management with close observation is an option,
but it should be understood that patients may later rapidly deteriorate. Poor
outcomes have been associated with worse clinical severity at presentation,
motor and sensory impairment, and longitudinally extensive hematomas.120
Subdural Hematoma
Spinal subdural hematoma is much less common than spinal epidural hematoma
but can present similarly with acute back pain, myelopathy, or radicular
symptoms. Nontraumatic causes are generally iatrogenic from procedures and
use of anticoagulation/antiplatelet agents.83 Chronic spinal subdural hematomas
are rare, reported with antiplatelet treatment and anticoagulation,121,122 but also
may be related to prior trauma or small bleeds. In the setting of recent spine
surgery, radiographic evidence of spinal subdural hematoma is not
uncommon.123 Management considerations for symptomatic spinal subdural
hematoma are similar to spinal epidural hematoma.
Subarachnoid Hemorrhage
Spontaneous spinal SAH is rare, accounting for 1% of all SAHs, and is the initial
presenting symptom in 10% of spinal AVMs.124 Symptoms typically include the
sudden onset of severe neck or back pain, and patients also frequently have
headache, meningismus, and hyponatremia. Depending on the extent of
hemorrhage and etiology, a variable severity in myelopathy deficits can be seen.
Redistribution of blood products throughout the CNS and typical complications
of SAH may occur (eg, vasospasm). Management is generally conservative,
addressing the underlying mechanism, and treating complications similar to
cerebral aneurysmal SAH. Etiologies and risk factors include hypertension
(common), spinal AVM, aneurysm, vascular neoplasm, intramedullary spinal
cord cavernous malformation, spinal dural arteriovenous fistula, vasculitis,125
blood dyscrasia, collagen vascular disease, anticoagulation, coarctation of the
aorta, and acute aortic dissection.126,127 Of note, spinal aneurysms rarely
rupture.8 Also, the accumulation of subarachnoid blood products in the thecal sac
can occur over time from prior lumbar punctures or spinal anesthesia with
CONTINUUMJOURNAL.COM 55
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
anticoagulation and compress the spinal cord and roots, termed subarachnoid
space hematoma.
CONCLUSION
Vascular myelopathies represent uncommon but frequently underrecognized
neurologic disorders. Clinicians need to carry a high index of clinical suspicion
for a possible vascular etiology in patients presenting with myelopathy or the
correct diagnosis will often be missed or delayed because of the overlapping
clinical and imaging features that may mimic other causes of myelopathy.
Providing patients with the proper medical management while avoiding
potentially harmful and unnecessary treatments may help improve outcomes.
REFERENCES
1 Zalewski NL, Flanagan EP, Keegan BM. Evaluation 9 English SW, Zalewski NL. Vascular disorders of
of idiopathic transverse myelitis revealing the spinal cord. Semin Neurol 2021;41(1).
specific myelopathy diagnoses. Neurology
10 Colman MW, Hornicek FJ, Schwab JH. Spinal cord
2018;90(2):e96-e102. doi:10.1212/WNL.
blood supply and its surgical implications. J Am
0000000000004796
Acad Orthop Surg 2015;23(10):581-591.
2 Barreras P, Fitzgerald KC, Mealy MA, et al. Clinical doi:10.5435/JAAOS-D-14-00219
biomarkers differentiate myelitis from vascular
11 Martirosyan NL, Feuerstein JS, Theodore N, et al.
and other causes of myelopathy. Neurology
Blood supply and vascular reactivity of the spinal
2018;90(1):e12-e21. doi:10.1212/WNL.
cord under normal and pathological conditions.
0000000000004765
J Neurosurg Spine 2011;15(3):238-251.
3 Brinjikji W, Nasr DM, Morris JM, et al. Clinical doi:10.3171/2011.4.SPINE10543
outcomes of patients with delayed diagnosis of
12 Perez VH, Hernesniemi J, Small JE. Anatomy of
spinal dural arteriovenous fistulas. AJNR Am J
the great posterior radiculomedullary artery.
Neuroradiol 2016;37(2):380-386. doi:10.3174/
AJNR Am J Neuroradiol 2019;40(12):2010-2015.
ajnr.A4504
doi:10.3174/ajnr.A6304
4 Nasr DM, Brinjikji W, Rabinstein AA, Lanzino G.
13 Etz CD, Kari FA, Mueller CS, et al. The collateral
Clinical outcomes following corticosteroid
network concept: a reassessment of the
administration in patients with delayed diagnosis
anatomy of spinal cord perfusion. J Thorac
of spinal arteriovenous fistulas. J Neurointerv
Cardiovasc Surg 2011;141(4):1020-1028. doi:10.1016/
Surg 2017;9(6):607-610. doi:10.1136/neurintsurg-
j.jtcvs.2010.06.023
2016-012430
14 Vuong SM, Jeong WJ, Morales H, Abruzzo TA.
5 Cordoba JP, Larrarte C, Medina MC. Experience
Vascular diseases of the spinal cord: infarction,
in therapeutic plasma exchange by membrane
hemorrhage, and venous congestive
filtration at an academic center in Colombia:
myelopathy. Semin Ultrasound CT MR 2016;37(5):
registry of the first 500 sessions. J Clin Apher
466-481. doi:10.1053/j.sult.2016.05.008
2015;30(6):347-352. doi:10.1002/jca.21391
15 Hughes JT. Pathology of the spinal cord. Major
6 Benadiba J, Robitaille N, Lambert G, et al.
Probl Pathol 1978;6:1-257.
Intravenous immunoglobulin-associated
thrombosis: is it such a rare event? Report of a 16 Sandson TA, Friedman JH. Spinal cord infarction.
pediatric case and of the Quebec Hemovigilance Report of 8 cases and review of the literature.
System. Transfusion 2015;55(3):571-575. Medicine (Baltimore) 1989;68(5):282292.
doi:10.1111/trf.12897
17 Petterson CA, Olsson Y. Blood supply of spinal
7 Zalewski NL, Rabinstein AA, Krecke KN, et al. nerve roots. An experimental study in the rat.
Characteristics of spontaneous spinal cord Acta Neuropathol 1989;78(5):455-461.
infarction and proposed diagnostic criteria. doi:10.1007/BF00687706
JAMA Neurol 2019;76(1):56-63. doi:10.1001/
18 Miyasaka K, Asano T, Ushikoshi S, et al. Vascular
jamaneurol.2018.2734
anatomy of the spinal cord and classification of
8 Caplan L, Massaro A. Spinal cord vascular spinal arteriovenous malformations. Interv
disease. In: Caplan LR, editor. Caplan's stroke: a Neuroradiol 2000;6 suppl 1(suppl 1):195-198.
clinical approach. Cambridge University Press, doi:10.1177/15910199000060S131
2016:534-543.
56 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
19 Zalewski NL, Rabinstein AA, Krecke KN, et al. 33 English SW, Rabinstein AA, Flanagan EP, Zalewski
Spinal cord infarction: clinical and imaging NL. Spinal cord transient Ischemic attacks.
insights from the periprocedural setting. J Neurol Neurol Clin Prac 2020;10(6). doi:10.1212/
Sci 2018;388:162-167. doi:10.1016/j.jns.2018.03.029 CPJ.0000000000000778
20 Wortmann M, Böckler D, Geisbüsch P. 34 Hurst RW, Kenyon LC, Lavi E, et al. Spinal dural
Perioperative cerebrospinal fluid drainage for arteriovenous fistula: the pathology of venous
the prevention of spinal ischemia after hypertensive myelopathy. Neurology 1995;45(7):
endovascular aortic repair. Gefasschirurgie 2017; 1309-1313. doi:10.1212/wnl.45.7.1309
22(suppl 2):35-40. doi:10.1007/s00772-017-0261-z
35 Aminoff MJ, Barnard RO, Logue V. The
21 Robertson CE, Brown RD Jr, Wijdicks EF, et al. pathophysiology of spinal vascular
Recovery after spinal cord infarcts: long-term malformations. J Neurol Sci 1974;23(2):255-263.
outcome in 115 patients. Neurology 2012;78(2): doi:10.1016/0022-510x(74)90229-9
114-121. doi:10.1212/WNL.0b013e31823efc93
36 Jellema K, Tijssen CC, van Gijn J. Spinal dural
22 Rabinstein AA. Vascular myelopathies. arteriovenous fistulas: a congestive myelopathy
Continuum (Minneap Minn) 2015;21(1, Spinal Cord that initially mimics a peripheral nerve disorder.
Disorders):67-83. doi:10.1212/01.CON. Brain 2006;129(pt 12):3150-3164. doi:10.1093/
0000461085.79241.e0 brain/awl220
23 Qureshi AI, Afzal MR, Suri MFK. A 37 Fugate JE, Lanzino G, Rabinstein AA. Clinical
population-based study of the incidence of presentation and prognostic factors of spinal
acute spinal cord infarction. J Vasc Interv Neurol dural arteriovenous fistulas: an overview.
2017;9(4):44-48. Neurosurg Focus 2012;32(5):E17. doi:10.3171/
2012.1.FOCUS11376
24 Kramer CL. Vascular disorders of the spinal cord.
Continuum (Minneap Minn) 2018;24(2, Spinal 38 Thron A. Spinal dural arteriovenous fistulas [in
Cord Disorders):407-426. doi:10.1212/ German]. Radiologe 2001;41(11):955-960.
CON.0000000000000595 doi:10.1007/s001170170031
25 Kobayashi Y, Sato S, Takamatsu R, et al. Late 39 Grandin C, Duprez T, Stroobandt G, et al. Spinal
changes on magnetic resonance imaging in dural arterio-venous fistula: an underdiagnosed
posterior spinal artery syndrome: a report and disease? Acta Neurol Belg 1997;97(1):17-21.
literature review. Neurol India 2019;67(2):571-573.
40 Bradac GB, Daniele D, Riva A, et al. Spinal dural
doi:10.4103/0028-3886.258006
arteriovenous fistulas: an underestimated cause
26 Kobayashi M. Spinal cord, vertebral body, of myelopathy. Eur Neurol 1994;34(2):87-94.
paraspinal muscle, and rib infarction: tiny doi:10.1159/000117015
thrombus detected by CT. Neurology 2016;87(6):
41 Kanematsu R, Hanakita J, Takahashi T, et al. An
642-643. doi:10.1212/WNL.0000000000002953
acquired cervical dural arteriovenous fistula after
27 Weng YC, Chin SC, Wu YY, Kuo HC. Clinical, cervical anterior fusion: case report and
neuroimaging, and nerve conduction literature review. World Neurosurg 2019;128:
characteristics of spontaneous conus medullaris 50-54. doi:10.1016/j.wneu.2019.04.202
infarction. BMC Neurol 2019;19(1):328. doi:10.1186/
42 Aminoff MJ, Logue V. Clinical features of spinal
s12883-019-1566-1
vascular malformations. Brain 1974;97(1):197-210.
28 Levin KH, Daube JR. Spinal cord infarction: doi:10.1093/brain/97.1.197
another cause of “lumbosacral
43 Jellema K, Canta LR, Tijssen CC, et al. Spinal dural
polyradiculopathy”. Neurology 1984;34(3):
arteriovenous fistulas: clinical features in 80
389-390. doi:10.1212/wnl.34.3.389
patients. J Neurol Neurosurg Psychiatry 2003;
29 Jankovic J, Rey Bataillard V, Mercier N, et al. 74(10):1438-1440. doi:10.1136/jnnp.74.10.1438
Acute ischemic myelopathy treated with
44 Atkinson JL, Miller GM, Krauss WE, et al. Clinical
intravenous thrombolysis: four new cases and
and radiographic features of dural arteriovenous
literature review. Int J Stroke 2019;14(9):893-897.
fistula, a treatable cause of myelopathy. Mayo
doi:10.1177/1747493019851289
Clin Proc 2001;76(11):1120-1130. doi:10.4065/
30 Hawkes MA, Braksick SA, Zhang W, et al. Can we 76.11.1120
stop the stuttering in stroke? Interventions in
45 Muralidharan R, Saladino A, Lanzino G, et al. The
40 patients with acute lacunes. J Neurol Sci 2019;
clinical and radiological presentation of spinal
401:1-4. doi:10.1016/j.jns.2019.04.009
dural arteriovenous fistula. Spine (Phila Pa 1976)
31 Ullman N, Gregg L, Becker D, et al. Anterior 2011;36(25):E1641-E1647. doi:10.1097/BRS.
disco-osteo-arterial conflict as a cause of 0b013e31821352dd
intersegmental arterial flow impairment and
46 Koerts G, Vanthuyne V, Delavallee M, et al. Spinal
spinal cord ischemia. Neuroradiology 2016;58(11):
dural arteriovenous fistula presenting with
1109-1115. doi:10.1007/s00234-016-1739-1
paraplegia following lumbar puncture.
32 Salvarani C, Brown RD Jr, Calamia KT, et al. J Neurosurg Spine 2013;19(1):57-60. doi:10.3171/
Primary CNS vasculitis with spinal cord 2013.3.SPINE12888
involvement. Neurology 2008;70(24 pt 2):
2394-2400. doi:10.1212/01.wnl.0000314687.69681.24
CONTINUUMJOURNAL.COM 57
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
47 Lee CS, Pyun HW, Chae EY, et al. Reversible 60 Wrobel CJ, Oldfield EH, Di Chiro G, et al.
aggravation of neurological deficits after steroid Myelopathy due to intracranial dural
medication in patients with venous congestive arteriovenous fistulas draining intrathecally into
myelopathy caused by spinal arteriovenous spinal medullary veins. Report of three cases.
malformation. Interv Neuroradiol 2009;15(3): J Neurosurg 1988;69(6):934-939. doi:10.3171/
325-329. doi:10.1177/159101990901500310 jns.1988.69.6.0934
48 McKeon A, Lindell EP, Atkinson JL, et al. Pearls & 61 Kalamangalam GP, Bhattacharya J, Teasdale E,
oy-sters: clues for spinal dural arteriovenous Thomas M. Myelopathy from intracranial dural
fistulae. Neurology 2011;76(3):e10-e12. arteriovenous fistula. J Neurol Neurosurg
Psychiatry 2002;72(6):816-818. doi:10.1136/
49 Lee J, Lim YM, Suh DC, et al. Clinical presentation,
jnnp.72.6.816
imaging findings, and prognosis of spinal dural
arteriovenous fistula. J Clin Neurosci 2016;26: 62 Manners J, Jadhav AP, Xia Z. Mystery case: a
105-109. doi:10.1016/j.jocn.2015.06.030 61-year-old woman with lower extremity
paralysis and sensory loss. Neurology 2017;
50 Sato K, Terbrugge KG, Krings T. Asymptomatic
89(22):e257-e263. doi:10.1212/
spinal dural arteriovenous fistulas:
WNL.0000000000004684
pathomechanical considerations. J Neurosurg
Spine 2012;16(5):441-446. doi:10.3171/2012.2. 63 Shin MJ, Kim W, Baik SK, et al. Cauda equina
SPINE11500 syndrome caused by spinal dural arteriovenous
fistula. Ann Rehabil Med 2011;35(6):928-933. doi:
51 Shimizu K, Takeda M, Mitsuhara T, et al.
10.5535/arm.2011.35.6.928
Asymptomatic spinal dural arteriovenous fistula:
case series and systematic review. J Neurosurg 64 Steinmetz MP, Chow MM, Krishnaney AA, et al.
Spine 2019:1-9. doi:10.3171/2019.5.SPINE181513 Outcome after the treatment of spinal dural
arteriovenous fistulae: a contemporary
52 Toossi S, Josephson SA, Hetts SW, et al. Utility of
single-institution series and meta-analysis.
MRI in spinal arteriovenous fistula. Neurology
Neurosurgery 2004;55(1):77-87; discussion 87-78.
2012;79(1):25-30. doi:10.1212/WNL.
doi:10.1227/01.neu.0000126878.95006.0f
0b013e3182582f07
65 Narvid J, Hetts SW, Larsen D, et al. Spinal dural
53 Krings T, Geibprasert S. Spinal dural
arteriovenous fistulae: clinical features and
arteriovenous fistulas. AJNR Am J Neuroradiol
long-term results. Neurosurgery 2008;62(1):
2009;30(4):639-648. doi:10.3174/ajnr.A1485
159-166; discussion 166-157. doi:10.1227/01.NEU.
54 Gilbertson JR, Miller GM, Goldman MS, Marsh 0000311073.71733.C4
WR. Spinal dural arteriovenous fistulas: MR and
66 Open and endovascular treatment of spinal dural
myelographic findings. AJNR Am J Neuroradiol
arteriovenous fistulas: a 10-year experience.
1995;16(10):2049-2057.
J Neurosurg Spine 2017;26(4):519-523. doi:10.3171/
55 Zalewski NL, Rabinstein AA, Brinjikji W, et al. 2016.9.SPINE16394
Unique gadolinium enhancement pattern in
67 Muralidharan R, Mandrekar J, Lanzino G, et al.
spinal dural arteriovenous fistulas. JAMA Neurol
Prognostic value of clinical and radiological signs
2018;75(12):1542-1545. doi:10.1001/
in the postoperative outcome of spinal dural
jamaneurol.2018.2605
arteriovenous fistula. Spine (Phila Pa 1976) 2013;
56 Saraf-Lavi E, Bowen BC, Quencer RM, et al. 38(14):1188-1193. doi:10.1097/BRS.0b013e31828b2e10
Detection of spinal dural arteriovenous fistulae
68 Brinjikji W, Yin R, Nasr DM, Lanzino G. Spinal
with MR imaging and contrast-enhanced MR
epidural arteriovenous fistulas. J Neurointerv
angiography: sensitivity, specificity, and
Surg 2016;8(12):1305-1310. doi:10.1136/neurintsurg-
prediction of vertebral level. AJNR Am J
2015-012181
Neuroradiol 2002;23(5):858-867.
69 Song Y, Cho SH, Lee DW, et al. Osseous versus
57 Luetmer PH, Lane JI, Gilbertson JR, et al.
nonosseous spinal epidural arteriovenous
Preangiographic evaluation of spinal dural
fistulas: experiences of 13 patients. AJNR Am J
arteriovenous fistulas with elliptic centric
Neuroradiol 2019;40(1):129-134. doi:10.3174/
contrast-enhanced MR Angiography and effect
ajnr.A5904
on radiation dose and volume of iodinated
contrast material. AJNR Am J Neuroradiol 2005; 70 Lenck S, Nicholson P, Tymianski R, et al. Spinal
26(4):711-718. and paraspinal arteriovenous lesions. Stroke
2019;50(8):2259-2269. doi:10.1161/STROKEAHA.
58 Bowen BC, Fraser K, Kochan JP, et al. Spinal dural
118.012783
arteriovenous fistulas: evaluation with MR
angiography. AJNR Am J Neuroradiol 1995;16(10): 71 Carvalho DZ, Hughes JD, Liebo GB, et al. Venous
2029-2043. congestive myelopathy due to chronic inferior
vena cava thrombosis treated with endovascular
59 Rodriguez FJ, Crum BA, Krauss WE, et al. Venous
stenting: case report and review of the literature.
congestive myelopathy: a mimic of neoplasia.
J Vasc Interv Neurol 2015;8(1):49-53.
Mod Pathol 2005;18(5):710-718.
58 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
72 Franco MJ, Vendrame M, Haneef Z, Azizi SA. 85 Del Curling O Jr, Kelly DL Jr, Elster AD, Craven TE.
Teaching neuroimage: acute spastic monoplegia An analysis of the natural history of cavernous
secondary to spinal epidural venous angiomas. J Neurosurg 1991;75(5):702-708.
engorgement in pregnancy. Neurology 2008;71(1): doi:10.3171/jns.1991.75.5.0702
e1. doi:10.1212/01.wnl.0000316310.85132.b3
86 Goyal A, Rinaldo L, Alkhataybeh R, et al. Clinical
73 Woodcock IR, Coscini N, Mandelstam S, et al. presentation, natural history and outcomes of
Acute spinal cord syndrome secondary to intramedullary spinal cord cavernous
venous congestion. Neurology 2016;87(12): malformations. J Neurol Neurosurg Psychiatry
1302-1303. doi:10.1212/WNL.0000000000003132 2019;90(6):695-703. doi:10.1136/jnnp-2018-319553
74 Ghiassi M, Ghiassi M, Kahn E, et al. Cauda equina 87 Deutsch H, Jallo GI, Faktorovich A, Epstein F.
syndrome secondary to an absent inferior vena Spinal intramedullary cavernoma: clinical
cava managed with surgical decompression. presentation and surgical outcome. J Neurosurg
J Neurosurg Spine 2012;16(2):201-205. 2000;93(1 suppl):65-70. doi:10.3171/
doi:10.3171/2011.10.SPINE1121 spi.2000.93.1.0065
75 Mohit AA, Fisher DJ, Matthews DC, et al. Inferior 88 Badhiwala JH, Farrokhyar F, Alhazzani W, et al.
vena cava thrombosis causing acute cauda Surgical outcomes and natural history of
equina syndrome. Case report. J Neurosurg intramedullary spinal cord cavernous
2006;104:46-49. doi:10.3171/ped.2006.104.1.46 malformations: a single-center series and
meta-analysis of individual patient data: clinic
76 Oterdoom DL, de Jong BM, Hoogland PV, Groen
article. J Neurosurg Spine 2014;21:662-676.
RJ. Transient cauda equina compression
doi:10.3171/2014.6.SPINE13949
syndrome and headache caused by internal
vertebral venous plexus engorgement in a 89 Rubin MN, Rabinstein AA. Vascular diseases of
teenage female with vena cava inferior agenesis the spinal cord. Neurol Clin 2013;31(1):153-181.
and iliac vein thrombosis. J Neurol Neurosurg doi:10.1016/j.ncl.2012.09.004
Psychiatry 2007;78(11):1283-1284. doi:10.1136/
90 Brown RD Jr, Flemming KD, Meyer FB, et al.
jnnp.2007.114629
Natural history, evaluation, and management of
77 Mohimen A, Kumar KS, Jayadevan ER, et al. Spinal intracranial vascular malformations. Mayo Clin
venous hypertension secondary to pelvic Proc 2005;80(2):269-281. doi:10.4065/80.2.269
extra-spinal arteriovenous fistula-a previously
91 Flemming KD, Kumar S, Lanzino G, Brinjikji W.
unreported cause of congestive myelopathy.
Baseline and evolutionary radiologic features in
Spine J 2016;16(2):e41-e42. doi:10.1016/j.
sporadic, hemorrhagic brain cavernous
spinee.2015.09.045
malformations. AJNR Am J Neuroradiol 2019;
78 Saito A, Takahashi T, Ezura M, Tominaga T. 40(6):967-972. doi:10.3174/ajnr.A6076
Intercostal arteriovenous fistula associated with
92 Kharkar S, Shuck J, Conway J, Rigamonti D. The
neurofibromatosis manifesting as congestive
natural history of conservatively managed
myelopathy: case report. Neurosurgery 2007;
symptomatic intramedullary spinal cord
61(3):E656-E657; discussion E657. doi:10.1227/
cavernomas. Neurosurgery 2007;60(5):865-872;
01.NEU.0000290918.47847.9E
discussion 865-872. doi:10.1227/01.NEU.
79 Clarke CE, Cumming WJ. Subacute myelopathy 0000255437.36742.15
caused by spinal venous infarction. Postgrad
93 Takai K. Spinal arteriovenous shunts:
Med J 1987;63(742):669-671. doi:10.1136/
angioarchitecture and historical changes in
pgmj.63.742.669
classification. Neurol Med Chir (Tokyo) 2017;
80 Nasr DM, Rabinstein A. Spinal cord infarcts: risk 57(7):356-365. doi:10.2176/nmc.ra.2016-0316
factors, management, and prognosis. Curr Treat
94 Rosenblum B, Oldfield EH, Doppman JL, Di Chiro
Options Neurol 2017;19(8):28. doi:10.1007/
G. Spinal arteriovenous malformations: a
s11940-017-0464-3
comparison of dural arteriovenous fistulas and
81 Pollock NW, Buteau D. Updates in decompression intradural AVM's in 81 patients. J Neurosurg 1987;
illness. Emerg Med Clin North Am 2017;35(2): 67(6):795-802. doi:10.3171/jns.1987.67.6.0795
301-319. doi:10.1016/j.emc.2016.12.002
95 Hong T, Yan Y, Li J, et al. High prevalence of
82 Baba T, Chang HS, Matsumae M. Severe spinal KRAS/BRAF somatic mutations in brain and spinal
cord compression by anomalous vertebral cord arteriovenous malformations. Brain 2019;
arteries treated with Gore-Tex tape transposition 142(1):23-34. doi:10.1093/brain/awy307
technique. World Neurosurg 2020;133:253-255.
96 Gross BA, Du R. Spinal glomus (type II)
doi:10.1016/j.wneu.2019.10.050
arteriovenous malformations: a pooled analysis
83 Shaban A, Moritani T, Al Kasab S, et al. Spinal cord of hemorrhage risk and results of intervention.
hemorrhage. J Stroke Cerebrovasc Dis 2018;27(6): Neurosurgery 2013;72(1):25-32; discussion 32.
1435-1446. doi:10.1016/j.jstrokecerebrovasdis. doi:10.1227/NEU.0b013e318276b5d3
2018.02.014
97 Yu JX, Hong T, Krings T, et al. Natural history of
84 Gross BA, Lin N, Du R, Day AL. The natural history spinal cord arteriovenous shunts: an observational
of intracranial cavernous malformations. study. Brain 2019;142(8):2265-2275. doi:10.1093/
Neurosurg Focus 2011;30(6):E24. doi:10.3171/ brain/awz153
2011.3.FOCUS1165
CONTINUUMJOURNAL.COM 59
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VASCULAR MYELOPATHIES
98 Rodesch G, Hurth M, Alvarez H, et al. 110 Lann MA, Lovell MA, Kleinschmidt-DeMasters
Angio-architecture of spinal cord arteriovenous BK. Acute hemorrhagic leukoencephalitis: a
shunts at presentation. Clinical correlations in critical entity for forensic pathologists to
adults and children. The Bicetre experience recognize. Am J Forensic Med Pathol 2010;31(1):
on 155 consecutive patients seen between 7-11. doi:10.1097/PAF.0b013e3181c6be92
1981-1999. Acta Neurochir (Wien) 2004;146(3):
111 Faragò G, Rossi S, Erbetta A. Visualization of a
217-226; discussion 226-217. doi:10.1007/
spinal capillary telangiectasia with 2D DSA and
s00701-003-0192-1
cone-beam CT. Neurology 2017;89(23):
99 Kim LJ, Spetzler RF. Classification and surgical 2395-2396. doi:10.1212/WNL.0000000000004719
management of spinal arteriovenous lesions:
112 Kao FC, Tsai TT, Chen LH, et al. Symptomatic
arteriovenous fistulae and arteriovenous
epidural hematoma after lumbar
malformations. Neurosurgery 2006;59:S195-S201;
decompression surgery. Eur Spine J 2015;24(2):
discussion S193-S113. doi:10.1227/01.
348-357. doi:10.1007/s00586-014-3297-8
NEU.0000237335.82234.CE
113 Cramer DE, Maher PC, Pettigrew DB, Kuntz Ct.
100 Ducruet AF, Crowley RW, McDougall CG,
Major neurologic deficit immediately after adult
Albuquerque FC. Endovascular management of
spinal surgery: incidence and etiology over 10
spinal arteriovenous malformations.
years at a single training institution. J Spinal
J Neurointerv Surg 2013;5(6):605-611. doi:10.1136/
Disord Tech 2009;22(8):565-570. doi:10.1097/
neurintsurg-2012-010487
BSD.0b013e318193452a
101 Endo T, Endo H, Sato K, et al. Surgical and
114 Sokolowski MJ, Garvey TA, Perl J 2nd, et al.
endovascular treatment for spinal arteriovenous
Prospective study of postoperative lumbar
malformations. Review Neurol Med Chir (Tokyo)
epidural hematoma: incidence and risk factors.
2016;56(8):457-464. doi:10.2176/nmc.ra.2015-
Spine 2008;33(1):108-113. doi:10.1097/
0327
BRS.0b013e31815e39af
102 Kalani MA, Choudhri O, Gibbs IC, et al.
115 Holtås S, Heiling M, Lönntoft M. Spontaneous
Stereotactic radiosurgery for intramedullary
spinal epidural hematoma: findings at MR
spinal arteriovenous malformations. J Clin
imaging and clinical correlation. Radiology 1996;
Neurosci 2016;29:162-167. doi:10.1016/
199(2):409-413. doi:10.1148/radiology.199.
j.jocn.2015.12.005
2.8668786
103 Constantini S, Ashkenazi E, Shoshan Y, et al.
116 Mélé N, Boulouis G, Bozier E, et al. Thoracic
Thoracic hematomyelia secondary to coumadin
outlet syndrome causing epidural hematoma:
anticoagulant therapy: a case report. Eur Neurol
case illustration. J Neurosurg 2020:1-2. doi:
1992;32(2):109-111. doi:10.1159/000116804
10.3171/2019.12.JNS192397
104 Zeidman SM, Olivi A. Cervical intramedullary
117 Yu JX, Hong T, Ma YJ, et al. A new type of spinal
hemorrhage as a result of anticoagulant therapy.
epidural arteriovenous fistulas causes spinal
J Spinal Disord 1993;6(5):456-457; discussion
epidural hemorrhage: an analysis of five cases
457-458.
and natural history consideration. World
105 Sedzimir CB, Roberts JR, Occleshaw JV, Buxton Neurosurg 2017;103:371-379. doi:10.1016/
PH. Gowers' syringal haemorrhage. J Neurol j.wneu.2017.04.036
Neurosurg Psychiatry 1974;37(3):312-315.
118 Rispoli R, Mastrostefano R, Passalacqua G, et al.
doi:10.1136/jnnp.37.3.312
Epidural hematoma caused by a spinal osseous
106 Wu CY, Riangwiwat T, Nakamoto BK. epidural arteriovenous fistula in a 14-year-old
Hemorrhagic longitudinally extensive transverse patient. A case report. Neuroradiol J 2009;22(4):
myelitis. Case Rep Neurol Med 2016;2016: 452-457. doi:10.1177/197140090902200416
1596864. doi:10.1155/2016/1596864
119 Lawton MT, Porter RW, Heiserman JE, et al.
107 Chang CC, McLean C, Vujovic O, et al. Fatal Surgical management of spinal epidural
acute varicella-zoster virus hemorrhagic hematoma: relationship between surgical timing
meningomyelitis with necrotizing vasculitis in an and neurological outcome. J Neurosurg 1995;
HIV-infected patient. Clin Infect Dis 2009;48(3): 83(1):1-7. doi:10.3171/jns.1995.83.1.0001
372-373. doi:10.1086/595894
120 Bakker NA, Veeger NJ, Vergeer RA, Groen RJ.
108 Wang Y, Yu CY, Huang L, et al. Acute longitudinal Prognosis after spinal cord and cauda
and hemorrhagic myelitis caused by compression in spontaneous spinal epidural
varicella-zoster virus in an immunocompetent hematomas. Neurology 2015;84(18):1894-1903.
adolescent. Neurologist 2015;19(4):93-95. doi:10.1212/WNL.0000000000001545
doi:10.1097/NRL.0000000000000016
121 Akiyama Y, Koyanagi I, Mikuni N. Chronic spinal
109 Nakajima H, Furutama D, Kimura F, et al. Herpes subdural hematoma associated with antiplatelet
simplex virus myelitis: clinical manifestations therapy. World Neurosurg 2017;105:1032.
and diagnosis by the polymerase chain reaction e1031-1032.e1035. doi:10.1016/j.wneu.2016.11.128
method. Eur Neurol 1998;39(3):163-167.
122 Ma H, Kim I. Idiopathic lumbosacral spinal
doi:10.1159/000007927
chronic subdural hematoma. Korean J Spine
2012;9(1):41-43. doi:10.14245/kjs.2012.9.1.41
60 FEBRUARY 2021
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
123 Nagamoto Y, Takenaka S, Aono H. Postoperative 126 Yost MD, Rabinstein AA. Spontaneous spinal
spinal subdural lesions following lumbar spine subarachnoid hemorrhage: presentation and
surgery: prevalence and risk factors. Asian Spine outcome. J Stroke Cerebrovasc Dis 2018;27(10):
J 2017;11(5):793-803. doi:10.4184/asj.2017.11.5.793 2792-2796. doi:10.1016/j.jstrokecerebrovasdis.
2018.06.005
124 Rinkel GJ, van Gijn J, Wijdicks EF. Subarachnoid
hemorrhage without detectable aneurysm. A 127 Subbiah MM, Velayudhan BV. Spinal
review of the causes. Stroke 1993;24(9): subarachnoid hemorrhage in type B aortic
1403-1409. doi:10.1161/01.str.24.9.1403 dissection: a rare presentation. Asian
Cardiovasc Thorac Ann 2020;28(3):175-178.
125 Alexander EL, Craft C, Dorsch C, et al.
doi:10.1177/0218492320901935
Necrotizing arteritis and spinal subarachnoid
hemorrhage in Sjögren syndrome. Ann Neurol
1982;11(6):632-635. doi:10.1002/ana.410110614
CONTINUUMJOURNAL.COM 61
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Graphic Guide Diseases PDFDocument382 pagesGraphic Guide Diseases PDFRafael100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Comptia Security Sy0 601 Exam Objectives (2 0)Document24 pagesComptia Security Sy0 601 Exam Objectives (2 0)tha_flameNo ratings yet
- Cefaleia - ContinuumDocument195 pagesCefaleia - ContinuumRafaelNo ratings yet
- Vol 27.5 - Neurocritical Care.2021Document363 pagesVol 27.5 - Neurocritical Care.2021RafaelNo ratings yet
- GiovaniDocument9 pagesGiovaniRafaelNo ratings yet
- Otorrino ContinuumDocument220 pagesOtorrino ContinuumRafaelNo ratings yet
- Periferico - ContinuumDocument239 pagesPeriferico - ContinuumRafaelNo ratings yet
- Febre No Pos OperatorioDocument4 pagesFebre No Pos OperatorioRafaelNo ratings yet
- Cerebrovasc - ContinuumDocument239 pagesCerebrovasc - ContinuumRafael100% (1)
- Febre Na UTIDocument8 pagesFebre Na UTIRafaelNo ratings yet
- Distúrbios de SodioDocument19 pagesDistúrbios de SodioRafaelNo ratings yet
- Candida Score 2006Document9 pagesCandida Score 2006RafaelNo ratings yet
- CVC Infecção Corr SangDocument8 pagesCVC Infecção Corr SangRafaelNo ratings yet
- Candida Col IndexDocument20 pagesCandida Col IndexRafaelNo ratings yet
- Major Article Influence of Exposure and Vertical Transmission of HIV-1 On The Neuropsychomotor Development in ChildrenDocument7 pagesMajor Article Influence of Exposure and Vertical Transmission of HIV-1 On The Neuropsychomotor Development in ChildrenRafaelNo ratings yet
- Ensuring Children and Adolescents Are Not Left BehindDocument2 pagesEnsuring Children and Adolescents Are Not Left BehindRafaelNo ratings yet
- Cardiohepatic Interactions in Heart Failure: An Overview and Clinical ImplicationsDocument9 pagesCardiohepatic Interactions in Heart Failure: An Overview and Clinical ImplicationsRafaelNo ratings yet
- Paul CooksDocument4 pagesPaul CooksMicNo ratings yet
- Maximo Training Material Day 2Document41 pagesMaximo Training Material Day 2ckombo9912100% (2)
- Full Chapter Embracing Modern C Safely 1St Edition Lakos PDFDocument53 pagesFull Chapter Embracing Modern C Safely 1St Edition Lakos PDFjeffery.rosseau147No ratings yet
- Unit Iv Secondary and Auxilary Motions 12Document3 pagesUnit Iv Secondary and Auxilary Motions 129043785763No ratings yet
- Conceptual FrameworkDocument4 pagesConceptual FrameworkEustass KiddNo ratings yet
- Springer Nature Latex TemplateDocument13 pagesSpringer Nature Latex TemplateAndres FloresNo ratings yet
- OceanofPDF - Com Strictly Research - Terry TowersDocument284 pagesOceanofPDF - Com Strictly Research - Terry TowersKenny SimNo ratings yet
- AfPS&CS Ch-01Document10 pagesAfPS&CS Ch-01Amelwork AlchoNo ratings yet
- JF 2 14 PDFDocument32 pagesJF 2 14 PDFIoannis GaridasNo ratings yet
- Bus Bar SolutionsDocument3 pagesBus Bar SolutionsSanjay MehtaNo ratings yet
- Akira - GA - Intro-To-Coding-Html-CssDocument46 pagesAkira - GA - Intro-To-Coding-Html-CssVinoth JayaprakasamNo ratings yet
- LPPDocument35 pagesLPPommprakashpanda15scribdNo ratings yet
- Tic EbookDocument215 pagesTic EbookTaju Deen100% (1)
- Plastic and Paper PDFDocument12 pagesPlastic and Paper PDFBhanu Pratap SolankiNo ratings yet
- Astm A 1011 2005Document8 pagesAstm A 1011 2005gao yanminNo ratings yet
- Anesthetic Consideration in Thyroid SurgeryDocument36 pagesAnesthetic Consideration in Thyroid Surgerymaulina13No ratings yet
- FACTORY IO-Sorting of Boxes (1) / PLC - 1 (CPU 1212C AC/DC/Rly) / Pro Gram BlocksDocument3 pagesFACTORY IO-Sorting of Boxes (1) / PLC - 1 (CPU 1212C AC/DC/Rly) / Pro Gram BlocksHasaan HussainNo ratings yet
- Bullz Audio Catalog 2013Document20 pagesBullz Audio Catalog 2013Jhonne TJ (TJ)No ratings yet
- SAP Idoc Steps by Step ConfigDocument7 pagesSAP Idoc Steps by Step Configgirish85No ratings yet
- Microsoft Project TOCDocument5 pagesMicrosoft Project TOCali_zulfikarNo ratings yet
- BitBox CarList 2022 10 28Document97 pagesBitBox CarList 2022 10 28marcos hernandezNo ratings yet
- PLC - HMI Lab #4 22W1Document2 pagesPLC - HMI Lab #4 22W1crazyjmprNo ratings yet
- (Shuangzhu Jia Et Al 2020) Study On The Preparing and Mechanism of Chitosan-Based Nanomesoporous Carbons by Hydrothermal MethodDocument21 pages(Shuangzhu Jia Et Al 2020) Study On The Preparing and Mechanism of Chitosan-Based Nanomesoporous Carbons by Hydrothermal MethodSilvia Devi Eka PutriNo ratings yet
- Admission LetterDocument7 pagesAdmission Letterduke cyberNo ratings yet
- General Revision For Treasury Management (Please See That You Can Answer The Following 32 Questions and The MCQS)Document14 pagesGeneral Revision For Treasury Management (Please See That You Can Answer The Following 32 Questions and The MCQS)RoelienNo ratings yet
- 6068TF250 Engine Performance CurveDocument2 pages6068TF250 Engine Performance CurveJulioNo ratings yet
- MTCNA Lab Guide INTRA 1st Edition - Id.en PDFDocument87 pagesMTCNA Lab Guide INTRA 1st Edition - Id.en PDFreyandyNo ratings yet
- SkillsDocument7 pagesSkillsRufus RajNo ratings yet
- English For ITDocument276 pagesEnglish For ITBao Tram100% (1)