Download as pdf or txt
You might also like
- Understanding The Health Belief ModelDocument4 pagesUnderstanding The Health Belief ModelBiliNo ratings yet
- Relee CV May 2021Document47 pagesRelee CV May 2021api-566915864No ratings yet
- PASOO Weight ManagementDocument4 pagesPASOO Weight ManagementNestor BalboaNo ratings yet
- CASE 119 ScenarioDocument2 pagesCASE 119 Scenariojhan jhanNo ratings yet
- Community Nutrition Case StudyDocument1 pageCommunity Nutrition Case StudyImmanuel LashleyNo ratings yet
- PnclexDocument3 pagesPnclexPaul Michael BaguhinNo ratings yet
- Sample Menu With JustificationDocument1 pageSample Menu With JustificationAbigail Lonogan100% (1)
- Answer and Rationale Community Health NursingDocument15 pagesAnswer and Rationale Community Health NursingCharles Gerard B. BeluanNo ratings yet
- PHC2. The Philippine Health Care Delivery SystemDocument55 pagesPHC2. The Philippine Health Care Delivery SystemHumilyn NgayawonNo ratings yet
- PHC & Rural Health Hasnat Hussain (Reus-11)Document4 pagesPHC & Rural Health Hasnat Hussain (Reus-11)Hasnat Hussain100% (2)
- Chapter 01 - Introduction To DrugsDocument3 pagesChapter 01 - Introduction To DrugsDaniel BenitezNo ratings yet
- Primary Health Care Hand Outs For StudentsDocument35 pagesPrimary Health Care Hand Outs For StudentsGreggy VenturaNo ratings yet
- Community Health Nursing Lecture Module 4Document10 pagesCommunity Health Nursing Lecture Module 4Meryville JacildoNo ratings yet
- CHN Quiz 1, 2, 3Document2 pagesCHN Quiz 1, 2, 3JkimNo ratings yet
- DT For Diabetes Mellitus and Renal DisordersDocument74 pagesDT For Diabetes Mellitus and Renal DisordersPrecious Diane Sincero BiocoNo ratings yet
- NMC Nursing Curriculum AssessmentDocument22 pagesNMC Nursing Curriculum AssessmentLoren KeithNo ratings yet
- Research and ManagementDocument9 pagesResearch and ManagementMa Charmaine Dawn VillaruelNo ratings yet
- Perineal Care ProcedureDocument12 pagesPerineal Care ProcedureShikarin KitaNo ratings yet
- FHSISDocument31 pagesFHSISNezer SorianoNo ratings yet
- Immunization: Expanded Program On Immunization (EPI)Document4 pagesImmunization: Expanded Program On Immunization (EPI)3amabelle arevaloNo ratings yet
- Maternal and Child NursingDocument13 pagesMaternal and Child NursingCarrel Relojero CarlosNo ratings yet
- Community-Health-Nursing-Review (Revised)Document291 pagesCommunity-Health-Nursing-Review (Revised)Lorelie AsisNo ratings yet
- ProfadDocument53 pagesProfadtetmetrangmail.com tet101486No ratings yet
- Nursing Theory PaperDocument5 pagesNursing Theory Paperapi-268670617No ratings yet
- Fourmula One For Health Goals and Objectives: Notes in Primary Health CareDocument34 pagesFourmula One For Health Goals and Objectives: Notes in Primary Health CarehanedinaNo ratings yet
- Post Test - Prof Ad - Prof. Fuentes (SC)Document2 pagesPost Test - Prof Ad - Prof. Fuentes (SC)Kristen FajilanNo ratings yet
- Quiz 2Document15 pagesQuiz 2Francis Rafael PadillaNo ratings yet
- 1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedDocument65 pages1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedAbdhanie PanontonganNo ratings yet
- Medicine and Medical Nursing Safe Journey Super Mock 2024.answersDocument28 pagesMedicine and Medical Nursing Safe Journey Super Mock 2024.answersSamuel Agyei AmankwaahNo ratings yet
- FHSISDocument14 pagesFHSISSam Raven AndresNo ratings yet
- CHN1Document898 pagesCHN1Mraclne Olaño0% (1)
- NDT Lec Midterm ReviewerDocument50 pagesNDT Lec Midterm ReviewerG05. Del Castillo, Angela Marie D.No ratings yet
- Community NutritionDocument22 pagesCommunity NutritionLilis IndriNo ratings yet
- CHN SyllabusDocument6 pagesCHN SyllabusEdwin Delos Reyes AbuNo ratings yet
- CHN Post Test1Document13 pagesCHN Post Test1Cstive ValenzuelaNo ratings yet
- About Integrated Management of Childhood IllnessDocument5 pagesAbout Integrated Management of Childhood IllnessRouena Santiago VillaramaNo ratings yet
- CHN Module 1Document5 pagesCHN Module 1jaoNo ratings yet
- CHN Notes For MidtermsDocument24 pagesCHN Notes For MidtermsReiner Lopez100% (1)
- CHN ExamDocument2 pagesCHN ExamRaelyn Valenton BenavidesNo ratings yet
- Introduction To NutritionDocument29 pagesIntroduction To NutritionBerhe Gebremichael HailuNo ratings yet
- DOTS Program For TB: Department of HealthDocument11 pagesDOTS Program For TB: Department of HealthCarissa De Luzuriaga-BalariaNo ratings yet
- PHC 1 ModuleDocument136 pagesPHC 1 ModuleRoselyn MadiwoNo ratings yet
- OBDocument9 pagesOBDennis ArevaloNo ratings yet
- Chapter 5: Symptoms and Syndromes: Multiple ChoiceDocument5 pagesChapter 5: Symptoms and Syndromes: Multiple ChoiceJamieNo ratings yet
- Chapter 2: Health Promotion in Middle-Aged AdultsDocument10 pagesChapter 2: Health Promotion in Middle-Aged AdultsTrixie AlvarezNo ratings yet
- Non Communicable DiseaseDocument13 pagesNon Communicable DiseaseClancy Anne Garcia Naval100% (1)
- University of Santo Tomas College of Education: Department of Nutrition and DieteticsDocument11 pagesUniversity of Santo Tomas College of Education: Department of Nutrition and DieteticsChelsea RosalNo ratings yet
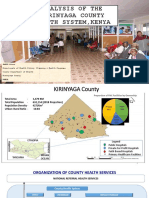
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- PHC & Rural Health Hasnat Hussain (Reus-11)Document4 pagesPHC & Rural Health Hasnat Hussain (Reus-11)Hasnat HussainNo ratings yet
- Nutrition in Life Cycle 2021 PDFDocument18 pagesNutrition in Life Cycle 2021 PDFErvie Marie SN100% (1)
- Determinants of Health and DiseaseDocument5 pagesDeterminants of Health and DiseaseMonesa Christy VillanuevaNo ratings yet
- Pedia Disorders ExamDocument32 pagesPedia Disorders Examjoemer salamatNo ratings yet
- PB 201-Chapter 1-Intro To EntrepreneurshipDocument59 pagesPB 201-Chapter 1-Intro To EntrepreneurshipAdda SyuehadahNo ratings yet
- Chapter 01 - Health Care Delivery and Evidence-Based Nursing PracticeDocument9 pagesChapter 01 - Health Care Delivery and Evidence-Based Nursing PracticePrince K. TaileyNo ratings yet
- Key PRN LM & PD 2021Document6 pagesKey PRN LM & PD 2021Umer IqbalNo ratings yet
- Physio AdapDocument3 pagesPhysio AdapAijem Ryan100% (1)
- Heed AssignmentDocument19 pagesHeed Assignmentapi-287705803100% (1)
- I. Multiple Choice: (Type I, Type II)Document2 pagesI. Multiple Choice: (Type I, Type II)greggy_rebel17No ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Intermittent FastingDocument5 pagesIntermittent FastingIoana IsarieNo ratings yet
- Top 10 Public Health Challenges To Track in 2023Document8 pagesTop 10 Public Health Challenges To Track in 2023Anne LauretaNo ratings yet
- Let's Change Our Lifestyle: Activity 2: Healthy Food Habits Lead inDocument5 pagesLet's Change Our Lifestyle: Activity 2: Healthy Food Habits Lead inmaria elisa felix cuyaNo ratings yet
- GSK Sotrovimab Fact Sheet For HCP 12222021Document34 pagesGSK Sotrovimab Fact Sheet For HCP 12222021Jillian SmithNo ratings yet
- Obesity Obesity OverviewDocument6 pagesObesity Obesity OverviewLorena IbarrolaNo ratings yet
- Guide To Promoting Health and Wellbeing in The WorkplaceDocument64 pagesGuide To Promoting Health and Wellbeing in The WorkplaceRoxana Stefanescu75% (4)
- Problem SolutionDocument3 pagesProblem SolutionCleo Abegail Palomado100% (1)
- Greg Nuckols Strength Potential Master CalculatorDocument4 pagesGreg Nuckols Strength Potential Master CalculatorKönczölDávidNo ratings yet
- EXTENDED ESSAY ASSINGMENT (PS102) S11195702 Romanu SavitaDocument10 pagesEXTENDED ESSAY ASSINGMENT (PS102) S11195702 Romanu SavitaSavita RomanuNo ratings yet
- Coronary Heart DiseaseDocument18 pagesCoronary Heart DiseasesamjaisheelNo ratings yet
- Psychological Interventions in Youth SportsDocument26 pagesPsychological Interventions in Youth SportsGuille monsterNo ratings yet
- Years of Democracy: Growing South Africa Together For Women's EmancipationDocument26 pagesYears of Democracy: Growing South Africa Together For Women's EmancipationAli AbbasNo ratings yet
- Literature Review On Physical ActivityDocument6 pagesLiterature Review On Physical Activityafmzxhvgfvprhm100% (1)
- Prevalence of Diabetes, Associated Symptoms and Risk Factors Among University StudentsDocument8 pagesPrevalence of Diabetes, Associated Symptoms and Risk Factors Among University Studentsijmb333No ratings yet
- Pregnancy Induced Hypertension Nursing Diagnosis NANDADocument9 pagesPregnancy Induced Hypertension Nursing Diagnosis NANDASanal S SalimNo ratings yet
- Life SciencesDocument12 pagesLife SciencesMJ SapiterNo ratings yet
- 2000-11 & 2012 Hkcee + Al LQDocument180 pages2000-11 & 2012 Hkcee + Al LQArthur ChoiNo ratings yet
- Fictional Narrative Essay ExamplesDocument7 pagesFictional Narrative Essay Examplesafhbhgbmy100% (2)
- Iehp 104Document8 pagesIehp 104imanuelcNo ratings yet
- Overweight Among Adolescents and Nutritional Status of Their Parents: A Systematic ReviewDocument10 pagesOverweight Among Adolescents and Nutritional Status of Their Parents: A Systematic Reviewonurb90No ratings yet
- ApexDocument18 pagesApexbaronggamingNo ratings yet
- SITHKOP004 Student PackDocument42 pagesSITHKOP004 Student PackAhmad TararNo ratings yet
- Fast Food Consumption (Paper)Document6 pagesFast Food Consumption (Paper)Shafiul Islam ArnobNo ratings yet
- Artikel 3Document23 pagesArtikel 3Hadian UwuoNo ratings yet
- Listening: The Biggest Loser Is A RealityDocument18 pagesListening: The Biggest Loser Is A RealityMaria Adelaide Maia TorresNo ratings yet
- Cardiologist Prof Rishi Sethi' Presentation On World Heart DayDocument36 pagesCardiologist Prof Rishi Sethi' Presentation On World Heart DaybobbyramakantNo ratings yet
- Blossom Pătė Borsenio Cura Vergara Fesib Study 1Document28 pagesBlossom Pătė Borsenio Cura Vergara Fesib Study 1FRANKLYN TRONCONo ratings yet
- Updated Pe 104 Course Design 2ND Sem 2022-2023-1Document53 pagesUpdated Pe 104 Course Design 2ND Sem 2022-2023-1Gadez JeanpelNo ratings yet
- Guidelines On Physical Activity-EngDocument36 pagesGuidelines On Physical Activity-EngsofiabloemNo ratings yet
- Euromonitor 10 Global Consumer TrendsDocument94 pagesEuromonitor 10 Global Consumer Trendsrave-n100% (2)