Download as pdf or txt
You might also like
- AtenololDocument4 pagesAtenololimaginarna_88No ratings yet
- Shiela's DE COCO'S DE TURONDocument27 pagesShiela's DE COCO'S DE TURONMary Grace Jerna Artazo Nozal-CuadraNo ratings yet
- Infection Control Power Point PresentationDocument45 pagesInfection Control Power Point PresentationPayal Thakker100% (1)
- TurbulencetrainingDocument59 pagesTurbulencetrainingappeal123No ratings yet
- Risk Factors of Chronic Venous Disease Inception: Received After Revision May 2008Document12 pagesRisk Factors of Chronic Venous Disease Inception: Received After Revision May 2008Pelipeschi ClaudiaNo ratings yet
- Diabetes and Fracture RiskDocument5 pagesDiabetes and Fracture RiskRifky F NaratamaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 15: MusculoskeletalFrom EverandComplementary and Alternative Medical Lab Testing Part 15: MusculoskeletalNo ratings yet
- Epidemiology Pelvic FloorDocument13 pagesEpidemiology Pelvic FloorBudi Iman SantosoNo ratings yet
- Overactive BladderDocument9 pagesOveractive BladderestalinxNo ratings yet
- Aliment Pharmacol Ther - 2004 - ChangDocument9 pagesAliment Pharmacol Ther - 2004 - ChangCynthia SuarezNo ratings yet
- PIIS0015028212002592Document11 pagesPIIS0015028212002592Carolina SidabutarNo ratings yet
- Arch Dis Child 2005 Jones 312 6Document6 pagesArch Dis Child 2005 Jones 312 6Indra GunawanNo ratings yet
- Cheung2013 Article AssociationOfHandgripStrengthWDocument13 pagesCheung2013 Article AssociationOfHandgripStrengthWAahna GuptaNo ratings yet
- EU Rccm.200611-1717ocDocument6 pagesEU Rccm.200611-1717ocDumitru BiniucNo ratings yet
- Sono Chest Estado Arta 2023Document17 pagesSono Chest Estado Arta 2023analisador analsiadorNo ratings yet
- Hsci 451 TermpaperDocument9 pagesHsci 451 Termpaperapi-241136824No ratings yet
- Obesity and DepressionDocument5 pagesObesity and DepressionTunde WilliamsNo ratings yet
- E.P.C.M.S.: Complete Pelvic Organ Prolapse in A Young Woman With Recent-Onset AscitesDocument2 pagesE.P.C.M.S.: Complete Pelvic Organ Prolapse in A Young Woman With Recent-Onset AscitesLim RidaNo ratings yet
- Epidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangDocument19 pagesEpidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangIkmal ShahromNo ratings yet
- Risk factors for preeclampsia عبدالسلامDocument5 pagesRisk factors for preeclampsia عبدالسلامmqbljbr529No ratings yet
- Pathophysiology of IBDDocument11 pagesPathophysiology of IBDOktarina Heni SunandarNo ratings yet
- Jurnal Etiologi (EBM)Document9 pagesJurnal Etiologi (EBM)Dewi LarasatiNo ratings yet
- Aipm 15 82Document6 pagesAipm 15 82Isini sehansa amarathungaNo ratings yet
- Body Mass Index, Mortality, and Gender Difference in Advanced Chronic Kidney DiseaseDocument13 pagesBody Mass Index, Mortality, and Gender Difference in Advanced Chronic Kidney DiseaseCleo AlvesNo ratings yet
- Joernal 3Document13 pagesJoernal 3Dyra DizhwarNo ratings yet
- AbstractDocument5 pagesAbstractputriprihatiningrumNo ratings yet
- Population-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenDocument14 pagesPopulation-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenSagar SononeNo ratings yet
- EthiopiaSTEPSPaper PDFDocument10 pagesEthiopiaSTEPSPaper PDFNovia LarasatiNo ratings yet
- Ard 2009 116053Document6 pagesArd 2009 116053tahirahaniyaNo ratings yet
- The Association Between Insomnia and Cardiovascular DiseasesDocument8 pagesThe Association Between Insomnia and Cardiovascular Diseasesnouval_iqbalNo ratings yet
- Association Between Low Back Pain and Various Everyday PerformancesDocument9 pagesAssociation Between Low Back Pain and Various Everyday Performancesshaik chandiniNo ratings yet
- Fcaa 185Document14 pagesFcaa 185Fhia TemansforNo ratings yet
- Longitudinal Predictors of Dieting and Disordered Eating Among Young Adults in The U.SDocument12 pagesLongitudinal Predictors of Dieting and Disordered Eating Among Young Adults in The U.SKira BeamesderferNo ratings yet
- Be Cher 2014Document9 pagesBe Cher 2014Puji Adi KharismaNo ratings yet
- Lower Back PainDocument4 pagesLower Back PainAizaz ul HaqNo ratings yet
- 66703b ImpactodelsuelopelvicoyelpartoDocument2 pages66703b Impactodelsuelopelvicoyelpartojavieralorenzo1No ratings yet
- Venous UlcersDocument11 pagesVenous UlcersAndrea Gómez SchulzNo ratings yet
- A Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomsDocument13 pagesA Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomssusanaNo ratings yet
- The Open Orthopaedics Journal: Etiological Theories of Adolescent Idiopathic Scoliosis: Past and PresentDocument24 pagesThe Open Orthopaedics Journal: Etiological Theories of Adolescent Idiopathic Scoliosis: Past and Presentrobervania leite marinho vaniaNo ratings yet
- Obesity & Osteoarthritis PDFDocument9 pagesObesity & Osteoarthritis PDFTaufik Ramadhan BiyaNo ratings yet
- Depression Is Inversely Associated With Sexual Satisfaction and Physical Function in Men Living With HIV/AIDSDocument7 pagesDepression Is Inversely Associated With Sexual Satisfaction and Physical Function in Men Living With HIV/AIDSWillNo ratings yet
- Physical Activity, Abdominal Obesity and The Risk of Coronary Heart Disease: A Korean National Sample StudyDocument7 pagesPhysical Activity, Abdominal Obesity and The Risk of Coronary Heart Disease: A Korean National Sample StudyFrankis De Jesus Vanegas RomeroNo ratings yet
- R245 FullDocument11 pagesR245 FullYuliana WiralestariNo ratings yet
- Peyronie's Disease: A Literature Review On Epidemiology, Genetics, Pathophysiology, Diagnosis and Work-UpDocument10 pagesPeyronie's Disease: A Literature Review On Epidemiology, Genetics, Pathophysiology, Diagnosis and Work-UpAdil BarutNo ratings yet
- Is There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyDocument6 pagesIs There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyYaarit IustainNo ratings yet
- Recent Advances in Cardiovascular Aspects of Polycystic Ovary SyndromeDocument9 pagesRecent Advances in Cardiovascular Aspects of Polycystic Ovary SyndromeRuth BritoNo ratings yet
- 035 ZoologyDocument7 pages035 ZoologyMuhammad SibtainNo ratings yet
- ArticuloDocument7 pagesArticuloDulceEspinozaLNo ratings yet
- Assessing The Influence of Benign Prostatic Hyperplasia (BPH) On Erectile Dysfunction (Ed) Among Patients in PolandDocument4 pagesAssessing The Influence of Benign Prostatic Hyperplasia (BPH) On Erectile Dysfunction (Ed) Among Patients in PolandAdly SungkarNo ratings yet
- Frissora - Practical GastroHORMONESDocument9 pagesFrissora - Practical GastroHORMONESMihaela AndreiNo ratings yet
- Localized Aggressive PeriodontitisDocument2 pagesLocalized Aggressive PeriodontitisKejora HanadinantiNo ratings yet
- The Importance of Gender in Health ProblemsDocument6 pagesThe Importance of Gender in Health Problemsmohdisram26No ratings yet
- Erectile Dysfunction and Comorbid Diseases, Androgen Deficiency, and Diminished Libido in MenDocument7 pagesErectile Dysfunction and Comorbid Diseases, Androgen Deficiency, and Diminished Libido in MenAfif Al FatihNo ratings yet
- Ulnocarpal Impactionealwe PDFDocument1 pageUlnocarpal Impactionealwe PDFunitbetty3No ratings yet
- 10 1016@j Esxm 2019 09 003Document12 pages10 1016@j Esxm 2019 09 003Bandac AlexandraNo ratings yet
- Urologic Complications of DiabetesDocument9 pagesUrologic Complications of DiabetesMaria Marcella RusliNo ratings yet
- Arumugam Et Al-Clinical Anatomy 2Document10 pagesArumugam Et Al-Clinical Anatomy 2Kavitha RajaNo ratings yet
- Chapter 1: IntroductionDocument10 pagesChapter 1: IntroductionSereneBaderNo ratings yet
- Medical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660Document6 pagesMedical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660David WheelerNo ratings yet
- Cardiovascular Risk in PCOSDocument2 pagesCardiovascular Risk in PCOSBill HarmanNo ratings yet
- Theburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingDocument12 pagesTheburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingabdulfatahalhemeryNo ratings yet
- Associations of Body Mass Index and Body Height With Low Back Pain in 829,791 AdolescentsDocument7 pagesAssociations of Body Mass Index and Body Height With Low Back Pain in 829,791 AdolescentsLeona NgadiahNo ratings yet
- Johne's Disease and Crohn's Disease, Report in BriefDocument2 pagesJohne's Disease and Crohn's Disease, Report in BriefNational Academies of Science, Engineering, and MedicineNo ratings yet
- The Vein Book 2ed Copia-43Document1 pageThe Vein Book 2ed Copia-43Miguel MendozaNo ratings yet
- Epidemiology of Chronic Peripheral Venous DiseaseDocument1 pageEpidemiology of Chronic Peripheral Venous DiseaseMiguel MendozaNo ratings yet
- The Vein Book 2ed Copia-41Document1 pageThe Vein Book 2ed Copia-41Miguel MendozaNo ratings yet
- The Vein Book 2ed Copia-46Document1 pageThe Vein Book 2ed Copia-46Miguel MendozaNo ratings yet
- The Vein Book 2ed Copia-42Document1 pageThe Vein Book 2ed Copia-42Miguel MendozaNo ratings yet
- Mudra: Analogy How It WorksDocument19 pagesMudra: Analogy How It WorksMariana DragomirNo ratings yet
- Guideline Mood Australia New Zeland PDFDocument120 pagesGuideline Mood Australia New Zeland PDFFábio C NetoNo ratings yet
- Upsc Csat Question Paper 2023 Set ADocument21 pagesUpsc Csat Question Paper 2023 Set Amahendra tadiparthiNo ratings yet
- EXSA - Gold Award Recipients 2006Document15 pagesEXSA - Gold Award Recipients 2006applebarrel100% (1)
- 5 - Farmakoterapi Pediatri - Dr. Nanang MunifDocument45 pages5 - Farmakoterapi Pediatri - Dr. Nanang MunifEdzhar Hasiholan100% (1)
- Homeopathic Clinical TipsDocument2 pagesHomeopathic Clinical Tipskaravi schiniasNo ratings yet
- Three Components of Hospice Care PrintableDocument4 pagesThree Components of Hospice Care PrintableVette Angelikka Dela CruzNo ratings yet
- GAD Proposal Client FocusedDocument6 pagesGAD Proposal Client FocusedIMELDA GUARINNo ratings yet
- Case Study (BIO320)Document12 pagesCase Study (BIO320)Ilham Amni AmaninaNo ratings yet
- Professional Development PlanDocument5 pagesProfessional Development Planapi-520853476No ratings yet
- The Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersDocument3 pagesThe Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PneumoniaDocument3 pagesPneumoniaJAGNo ratings yet
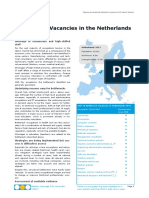
- Country Fiche NL - Final - RevisedDocument5 pagesCountry Fiche NL - Final - RevisedPranav DubeyNo ratings yet
- Complaint Handling SOPDocument9 pagesComplaint Handling SOPVidhya GGNo ratings yet
- 02 Kanto Region (Kaigofukushishi) 12000017Document4 pages02 Kanto Region (Kaigofukushishi) 12000017bnp2tkidotgodotidNo ratings yet
- Jurnal Food and Covid-19: DR - Badrut Tamam, SPT, M.BiotechDocument10 pagesJurnal Food and Covid-19: DR - Badrut Tamam, SPT, M.Biotechindah kahaNo ratings yet
- The Leeds Assessment of Neuropathic Symptoms and SignsDocument2 pagesThe Leeds Assessment of Neuropathic Symptoms and SignsPutu Gede SudiraNo ratings yet
- Cues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IDocument3 pagesCues/Data Family Nursing Problems: Unsanitary Food Handling and Preparation IAlbert GamasNo ratings yet
- The Relationships Among Uncertainty, Social Support, and Psychological Distress in Adolescents Recently Diagnosed With CancerDocument10 pagesThe Relationships Among Uncertainty, Social Support, and Psychological Distress in Adolescents Recently Diagnosed With CancerAhmed NuruNo ratings yet
- SKINVIVE by JUVÉDERM - P110033 - S059 - FDADocument3 pagesSKINVIVE by JUVÉDERM - P110033 - S059 - FDAfatmamohamed3338No ratings yet
- Should Shouldn'tDocument17 pagesShould Shouldn'tAvlandeNo ratings yet
- CIWM 2006 - Salim Vohra - Waste and HIA Paper - FINAL With Panel AmendmentsDocument14 pagesCIWM 2006 - Salim Vohra - Waste and HIA Paper - FINAL With Panel AmendmentsSalim VohraNo ratings yet
- FIGO Accreta Prenantal DiagnosisDocument7 pagesFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi Salan100% (1)
- Core Competency 2:: Participates in Nursing Audits and RoundsDocument8 pagesCore Competency 2:: Participates in Nursing Audits and RoundsMary Grace MasNo ratings yet
- A Beautiful MindDocument5 pagesA Beautiful MindKirby Contaoi100% (3)
- Advanced English For Nursing English DialogueDocument4 pagesAdvanced English For Nursing English Dialogueirfani28No ratings yet