Download as pdf or txt
You might also like
- Digital Marketing Strategy Implementation and Prac 220825 185854Document124 pagesDigital Marketing Strategy Implementation and Prac 220825 185854Clarah Kusuta100% (3)
- Abhilasha Visa SopDocument3 pagesAbhilasha Visa Sopjyoti100% (3)
- Risk Management Concept Building Summary Book by CA Shivam PalanDocument125 pagesRisk Management Concept Building Summary Book by CA Shivam PalanShivanand MuleNo ratings yet
- Supply Chain Performance Measurement ApproachesDocument273 pagesSupply Chain Performance Measurement ApproachesErik Van0% (1)
- Med Net CaseDocument3 pagesMed Net CaseVineet Bajaj100% (1)
- 196-1584526128 LeanhospitalDocument8 pages196-1584526128 LeanhospitalDharm Veer RathoreNo ratings yet
- Cost Reduction in Healthcare Via Lean Six SigmaDocument8 pagesCost Reduction in Healthcare Via Lean Six SigmaGloom GomsNo ratings yet
- 2017 Article 563Document11 pages2017 Article 563raphael boechatNo ratings yet
- Lean ManagmentDocument20 pagesLean Managmentفيصل الاعرجNo ratings yet
- Quality ImprovementDocument18 pagesQuality ImprovementSyeda SanaNo ratings yet
- Ic003010 PDFDocument14 pagesIc003010 PDFDiptoNo ratings yet
- Process Improvement in A Radiology Department: Hatice Camgoz-Akdag and Tu Ğçe BeldekDocument12 pagesProcess Improvement in A Radiology Department: Hatice Camgoz-Akdag and Tu Ğçe BeldekAditya ShuklaNo ratings yet
- Six Sigma in Healthcare DeliveryDocument21 pagesSix Sigma in Healthcare Deliverymaribel100% (1)
- Mast Et Al-2011-Quality and Reliability Engineering InternationalDocument12 pagesMast Et Al-2011-Quality and Reliability Engineering InternationalAnonymous 3O0J2YYNo ratings yet
- 018 Quality ManagementDocument17 pages018 Quality Managementfikrumersha47No ratings yet
- FinalDocument27 pagesFinalYasmeen MemonNo ratings yet
- A Study On Total Quality Management and Lean Manufacturing: Through Lean Thinking ApproachDocument12 pagesA Study On Total Quality Management and Lean Manufacturing: Through Lean Thinking ApproachDian AndriliaNo ratings yet
- Improving Emergency Department Through Business PRDocument21 pagesImproving Emergency Department Through Business PRRares VasileNo ratings yet
- The Critical Success Factors For Successful Lean Implementation in HospitalsDocument19 pagesThe Critical Success Factors For Successful Lean Implementation in HospitalsKabib AbdullahNo ratings yet
- A Study On Total Quality Management and Lean Manufacturing: Through Lean Thinking ApproachDocument12 pagesA Study On Total Quality Management and Lean Manufacturing: Through Lean Thinking Approachhusam-h2252No ratings yet
- A Bibliometric View On The Use of Total Quality Management in ServicesDocument29 pagesA Bibliometric View On The Use of Total Quality Management in Servicesyohannes retaNo ratings yet
- Pimentel Major TQMDocument17 pagesPimentel Major TQMpirthisingh53No ratings yet
- Pareto Analysis of Total Quality ManagementDocument18 pagesPareto Analysis of Total Quality ManagementankitatiwarigNo ratings yet
- New ProcessDocument17 pagesNew ProcessLong Live PakistanNo ratings yet
- Critical Success Factors For The Successful Initiation of Lean in Public Hospitals in Kwazulu-Natal: A Factor Analysis and Structural Equation Modelling StudyDocument11 pagesCritical Success Factors For The Successful Initiation of Lean in Public Hospitals in Kwazulu-Natal: A Factor Analysis and Structural Equation Modelling StudySunday Temitope PhillipsNo ratings yet
- Total Quality ImprovementDocument21 pagesTotal Quality ImprovementMar DiyanNo ratings yet
- Quality Management and A Balanced Scorecard As SupportingDocument14 pagesQuality Management and A Balanced Scorecard As SupportingNezo QawasmehNo ratings yet
- Content ServerDocument13 pagesContent Serverwin1234onaNo ratings yet
- Working Paper Series: College of Business Administration University of Rhode IslandDocument25 pagesWorking Paper Series: College of Business Administration University of Rhode IslandDeivid Zharatte Enry QuezNo ratings yet
- Process Analysis For A Hospital Emergency DepartmentDocument8 pagesProcess Analysis For A Hospital Emergency DepartmentEponleeNo ratings yet
- DMAIC For Process Digitalization: A Hospital Case StudyDocument17 pagesDMAIC For Process Digitalization: A Hospital Case StudyGuillermo Luis AcostaNo ratings yet
- Paper 5 Review The Literature of Balanced Scorecard and Performance Measurement 1Document15 pagesPaper 5 Review The Literature of Balanced Scorecard and Performance Measurement 1Kepher OnukoNo ratings yet
- Statistical Process Control: An Essential Ingredient For Improving Service and Manufacuring QualityDocument6 pagesStatistical Process Control: An Essential Ingredient For Improving Service and Manufacuring QualityNilakshi RathnayakeNo ratings yet
- Developments of Traditional Value Stream Mapping To Enhance Personal and Organisational System and Methods CompetenciesDocument15 pagesDevelopments of Traditional Value Stream Mapping To Enhance Personal and Organisational System and Methods CompetenciesDavid OrellanaNo ratings yet
- Lean Healthcare Literature ReviewDocument5 pagesLean Healthcare Literature Reviewea2167ra100% (1)
- Cqi ToolsDocument4 pagesCqi ToolsChilufya MulopaNo ratings yet
- 60 6 Dyas FinalDocument17 pages60 6 Dyas FinallucilleNo ratings yet
- An Evaluation of The Impact of Health Information Technology and Timely Availability of Visit Diagnoses From Ambulatory Visits On Patient Experience and OutcomesDocument16 pagesAn Evaluation of The Impact of Health Information Technology and Timely Availability of Visit Diagnoses From Ambulatory Visits On Patient Experience and OutcomesDick JohnsonNo ratings yet
- Strategi Operasi RUmah SakitDocument4 pagesStrategi Operasi RUmah SakituddindjmNo ratings yet
- Keywords:: International Journal of Applied Strategic Management: Volume 1 Issue 1Document14 pagesKeywords:: International Journal of Applied Strategic Management: Volume 1 Issue 1Sonika Kapoor MehrotraNo ratings yet
- Quality Management in The Healthcare Industry - A Conceptual AnalysisDocument12 pagesQuality Management in The Healthcare Industry - A Conceptual AnalysisEmil CrisanNo ratings yet
- Implementation of The Lean Six Sigma Framework in Non-Profit Organisations A Case StudyDocument18 pagesImplementation of The Lean Six Sigma Framework in Non-Profit Organisations A Case StudyYolandaNo ratings yet
- Application of Jurangçö S TrilogyDocument30 pagesApplication of Jurangçö S TrilogyEr Vbhor ShrmaNo ratings yet
- 015-0788 Organizational Culture by Change Management: DHL Global Forwarding Case StudyDocument27 pages015-0788 Organizational Culture by Change Management: DHL Global Forwarding Case Studynyan hein aungNo ratings yet
- Operations Management Assignment 1Document6 pagesOperations Management Assignment 1Laveda KanishkaNo ratings yet
- TQM in Corporate Hospitals - Using Six SigmaDocument15 pagesTQM in Corporate Hospitals - Using Six SigmaApollo Institute of Hospital Administration100% (3)
- THE EFFECTIVENESS OF SIX SIGMA IN SERVICES SECTORS-libre PDFDocument26 pagesTHE EFFECTIVENESS OF SIX SIGMA IN SERVICES SECTORS-libre PDFsarahNo ratings yet
- Auditing of Explorative ProcessesDocument16 pagesAuditing of Explorative ProcessesSoufiane LabraziNo ratings yet
- SIX SIGMA in EducationDocument17 pagesSIX SIGMA in EducationVadher AmitNo ratings yet
- Improving Quality Services in Banks Using The Six-Sigma DMAIC ModelDocument12 pagesImproving Quality Services in Banks Using The Six-Sigma DMAIC ModelRayanNo ratings yet
- Activity Based CostingDocument18 pagesActivity Based CostingDaniel SaragihNo ratings yet
- Makalah Penerapan Lean Di RSDocument10 pagesMakalah Penerapan Lean Di RSkhrisna02No ratings yet
- Al Araidah2010Document8 pagesAl Araidah2010jf.leungyanNo ratings yet
- A Framework For Analysing Supply Chain Performance Evaluation ModelsDocument12 pagesA Framework For Analysing Supply Chain Performance Evaluation ModelsVivek MohapatraNo ratings yet
- Business Process Reengineering in Emergency Departments (Eds) : Evidence From Two HospitalsDocument15 pagesBusiness Process Reengineering in Emergency Departments (Eds) : Evidence From Two HospitalsNyokabi MuchiriNo ratings yet
- Application of Lean Healthcare in Hospital ServiceDocument14 pagesApplication of Lean Healthcare in Hospital ServiceRon patelNo ratings yet
- Bussiness Excelence)Document20 pagesBussiness Excelence)KelensantNo ratings yet
- Hospital Operations Management: An Exploratory Study From Brazil and PortugalDocument10 pagesHospital Operations Management: An Exploratory Study From Brazil and PortugalQuality SaketNo ratings yet
- Effects of Lean Six Sigma Application inDocument6 pagesEffects of Lean Six Sigma Application inYou YouNo ratings yet
- The Relationship Between Hospital Administration and Quality of Services: Meta-AnalysisDocument9 pagesThe Relationship Between Hospital Administration and Quality of Services: Meta-AnalysisAYESIGA OWENNo ratings yet
- MavsDocument8 pagesMavsfreakgreek34No ratings yet
- The Management of Chronic Diseases: Organizational Innovation and EfficiencyFrom EverandThe Management of Chronic Diseases: Organizational Innovation and EfficiencyNo ratings yet
- Capstone Project Final 2Document52 pagesCapstone Project Final 2priyankaNo ratings yet
- Section 2 PMPDocument69 pagesSection 2 PMPJISHNU SNo ratings yet
- Drug War II Public CitizenDocument51 pagesDrug War II Public CitizenGaby ArguedasNo ratings yet
- Supply Chain Contracting ForecastDocument33 pagesSupply Chain Contracting ForecastKatie Crolley100% (1)
- Lankabangla Project by MinhazDocument40 pagesLankabangla Project by MinhazShafayet JamilNo ratings yet
- 1 P2A PRACT Questions PAPER 1Document28 pages1 P2A PRACT Questions PAPER 1Zoe TanNo ratings yet
- Sas#11 Bam200Document7 pagesSas#11 Bam200Mekuh Rouzenne Balisacan PagapongNo ratings yet
- Yamane v. B.A. Lepanto CondominiumDocument6 pagesYamane v. B.A. Lepanto CondominiumSuzyNo ratings yet
- Mess BillDocument2 pagesMess BillSabari StunnerNo ratings yet
- Program/Project Development and ManagementDocument8 pagesProgram/Project Development and ManagementRhodeny Peregrino IslerNo ratings yet
- SPREE - THE MARKET PLAN (Muhammad Shoaib Assignment)Document10 pagesSPREE - THE MARKET PLAN (Muhammad Shoaib Assignment)shoaibNo ratings yet
- Adrian Raducan CV 1Document3 pagesAdrian Raducan CV 1alinadragos1226No ratings yet
- What Is Iso CertificationDocument4 pagesWhat Is Iso CertificationShailesh GuptaNo ratings yet
- LAS w3Document6 pagesLAS w3Pats MinaoNo ratings yet
- Business Strategy Case Presentation (Case - Cultural Challenges of Integration: Value Creation and Daiichi Sankyo'S Indian Acquisition)Document15 pagesBusiness Strategy Case Presentation (Case - Cultural Challenges of Integration: Value Creation and Daiichi Sankyo'S Indian Acquisition)DivyyaPandeyNo ratings yet
- BBP Profit Center AccountingDocument11 pagesBBP Profit Center AccountingVishal Yadav50% (2)
- Managerial Economics in A Global Economy, 5th Edition by Dominick SalvatoreDocument26 pagesManagerial Economics in A Global Economy, 5th Edition by Dominick SalvatoreFareed khan ZKNo ratings yet
- Câu H i ạ ể: Hoàn thành t i m 1,00 trên 1,00Document4 pagesCâu H i ạ ể: Hoàn thành t i m 1,00 trên 1,00Tram NguyenNo ratings yet
- France - Airbus : A Web Based Case StudyDocument13 pagesFrance - Airbus : A Web Based Case Studyvijaysingh_83No ratings yet
- Placement Opportunity - Rulesiq - Com - B.Tech (Mechanical) - Batch 2023Document2 pagesPlacement Opportunity - Rulesiq - Com - B.Tech (Mechanical) - Batch 2023Aman PatelNo ratings yet
- Palherkar SanjayDocument8 pagesPalherkar SanjayAFTAB AHMADNo ratings yet
- Marketing Performance of Agricultural CooperativesDocument11 pagesMarketing Performance of Agricultural CooperativesRammee AnuwerNo ratings yet
- RFP Digital-Hubs InteriorDocument11 pagesRFP Digital-Hubs InteriorpnkxabaNo ratings yet
- Quality MGTDocument82 pagesQuality MGTEl-azar AssefaNo ratings yet
- Joint Ventures and Learning CapabilitiesDocument22 pagesJoint Ventures and Learning CapabilitiesX NishidaNo ratings yet
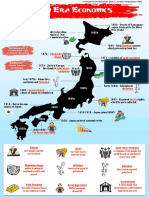
- Meiji Era Economic Copy 2Document1 pageMeiji Era Economic Copy 2api-298392554No ratings yet