Download as pdf or txt
You might also like
- Uw Step3 NotesDocument34 pagesUw Step3 NotesAakash ShahNo ratings yet
- Carotid Endarterectomy FinalDocument48 pagesCarotid Endarterectomy Finalimad mokalledNo ratings yet
- 99591Document7 pages99591jimejuanfeNo ratings yet
- Strain 3Document7 pagesStrain 3Mustafa Beyazıt AlkanNo ratings yet
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- Circulation 2014 Silvain 918 22Document6 pagesCirculation 2014 Silvain 918 22aninNo ratings yet
- Fifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDocument6 pagesFifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDavid RamirezNo ratings yet
- Jcu 17 127 PDFDocument8 pagesJcu 17 127 PDFRezkyFYNo ratings yet
- Summary and ConclusionDocument4 pagesSummary and Conclusionhamodi222No ratings yet
- Atwater 2020Document6 pagesAtwater 2020Vlada SiricNo ratings yet
- Reverse Tria24 MolDocument12 pagesReverse Tria24 Molbinh doNo ratings yet
- Ortiz2007 PDFDocument3 pagesOrtiz2007 PDFJorge Gomez MarulandaNo ratings yet
- Dialysis After CABG Ejcts 2013ddDocument6 pagesDialysis After CABG Ejcts 2013ddDumitru GrozaNo ratings yet
- Leukoaraiosis Is Associated With Poor Outcomes After Successful Recanalization For Large Vessel Occlusion StrokeDocument7 pagesLeukoaraiosis Is Associated With Poor Outcomes After Successful Recanalization For Large Vessel Occlusion StrokeLaura Valentina Huertas SaavedraNo ratings yet
- Liver Transplantation - 2012 - Plotkin - Coronary Artery Disease and Liver Transplantation The State of The Art PDFDocument4 pagesLiver Transplantation - 2012 - Plotkin - Coronary Artery Disease and Liver Transplantation The State of The Art PDFphonex xoxNo ratings yet
- Application of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationDocument8 pagesApplication of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationSondang JasmineNo ratings yet
- 35 5 854 PDFDocument10 pages35 5 854 PDFRoni ArmandaNo ratings yet
- Doshi 2005Document6 pagesDoshi 2005Luba D'AndreaNo ratings yet
- Bahan Referat Miocardial Stunning Perit Dial Int-2011-Selby-27-33Document7 pagesBahan Referat Miocardial Stunning Perit Dial Int-2011-Selby-27-33viniganorNo ratings yet
- Results With Respect To Intraprocedural Myocardial Contrast EchocardiographyDocument16 pagesResults With Respect To Intraprocedural Myocardial Contrast EchocardiographySavira Tapi-TapiNo ratings yet
- JLM 03 26Document8 pagesJLM 03 26Roberto DianNo ratings yet
- Bibliografia 6Document7 pagesBibliografia 6mrcristian_17892No ratings yet
- CapricornDocument6 pagesCapricornMarkanthony256No ratings yet
- Dr. Faisal Qadir Tachycardia Induced CM - Dr. Faisal Qadir - March 2, 2024Document31 pagesDr. Faisal Qadir Tachycardia Induced CM - Dr. Faisal Qadir - March 2, 2024Hafiz Wajid SadiqNo ratings yet
- Effect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisDocument7 pagesEffect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisMatthew MckenzieNo ratings yet
- By DR - Vasudeva Chetty PakalaDocument97 pagesBy DR - Vasudeva Chetty Pakalaace forumNo ratings yet
- Renal Vascular Diseases FinalDocument43 pagesRenal Vascular Diseases FinalAlina CazanNo ratings yet
- Wellen's Syndrome: Mohan GameshDocument28 pagesWellen's Syndrome: Mohan Gameshmyolie wuNo ratings yet
- Usefulness of Stent Implantation For Treatment ofDocument19 pagesUsefulness of Stent Implantation For Treatment ofAngel YapNo ratings yet
- Surgical Coronary Revascularization Who, What, WhenDocument68 pagesSurgical Coronary Revascularization Who, What, WhenAlaaGaballaNo ratings yet
- 10.1007@s00261 019 02340 5Document25 pages10.1007@s00261 019 02340 5Pablo Henrique Alves TelesNo ratings yet
- Catheter Ablation For Atrial Arrhythmias in Patients With Cardiac AmyloidosisDocument7 pagesCatheter Ablation For Atrial Arrhythmias in Patients With Cardiac AmyloidosisjjsanchezmunozNo ratings yet
- Clinical Characteristics of Fast and Slow Progressors of Infarct Growth in Anterior Circulation Large Vessel Occlusion StrokeDocument6 pagesClinical Characteristics of Fast and Slow Progressors of Infarct Growth in Anterior Circulation Large Vessel Occlusion StrokeItamar MeirelesNo ratings yet
- PIIS1071916411003940Document1 pagePIIS1071916411003940Monica AlbertNo ratings yet
- Rashid 2021Document10 pagesRashid 2021Carmen Cuadros BeigesNo ratings yet
- AKI and CRRT RelationDocument10 pagesAKI and CRRT RelationZainab MotiwalaNo ratings yet
- Device Therapy in Heart Failure Patients With Chronic Kidney DiseaseDocument8 pagesDevice Therapy in Heart Failure Patients With Chronic Kidney DiseaseElizabeth SniderNo ratings yet
- Christersson2022 Article ScreeningForBiomarkersAssociatDocument11 pagesChristersson2022 Article ScreeningForBiomarkersAssociatS FznsNo ratings yet
- Outcome of Unroofing Procedure For Repair of Anomalous Aortic Origin of Left or Right Coronary ArteryDocument8 pagesOutcome of Unroofing Procedure For Repair of Anomalous Aortic Origin of Left or Right Coronary ArteryKrupa KarnikNo ratings yet
- Cardiorenal Syndrome Type 1 (CRS) : BS. Đỗ Tuấn Kiệt BS. Huỳnh Tấn Khảo Khoa Nội tim mạch - Lão học Bệnh viện Lê Văn ThịnhDocument28 pagesCardiorenal Syndrome Type 1 (CRS) : BS. Đỗ Tuấn Kiệt BS. Huỳnh Tấn Khảo Khoa Nội tim mạch - Lão học Bệnh viện Lê Văn ThịnhdovatiNo ratings yet
- Grant2014 PDFDocument10 pagesGrant2014 PDFRalucaNo ratings yet
- Chira Karn Jana Korn 2017Document55 pagesChira Karn Jana Korn 2017JoecoNo ratings yet
- Analysis of The Results of Sanitation Nephrectomies in Polycystic Kidney Disease in Recipients Before Kidney TransplantationDocument12 pagesAnalysis of The Results of Sanitation Nephrectomies in Polycystic Kidney Disease in Recipients Before Kidney TransplantationОлеся МураховськаNo ratings yet
- Department of Urology, Singapore General Hospital: Ganvhl, NGLGDocument2 pagesDepartment of Urology, Singapore General Hospital: Ganvhl, NGLGArmando FigueroaNo ratings yet
- Kvit Noac Bleeding Real LifeDocument6 pagesKvit Noac Bleeding Real LifeLovadi Emese IldikóNo ratings yet
- Mala Goli 2018Document9 pagesMala Goli 2018ErtanNo ratings yet
- The Perindopril in Elderly PeopleDocument8 pagesThe Perindopril in Elderly PeopleluchititaNo ratings yet
- Blah 5 AsdsadsaDocument5 pagesBlah 5 Asdsadsaprern27No ratings yet
- Acute Renal Failure in Critically Ill Surgical Patients PDFDocument7 pagesAcute Renal Failure in Critically Ill Surgical Patients PDFRomán Jiménez LópezNo ratings yet
- Percutaneous Transcatheter Mitral Valve Replacement With AltaValve in Patients With Prior Aortic Valve ReplacementDocument1 pagePercutaneous Transcatheter Mitral Valve Replacement With AltaValve in Patients With Prior Aortic Valve ReplacementliliNo ratings yet
- J Amjcard 2019 01 017Document20 pagesJ Amjcard 2019 01 017NasriNo ratings yet
- Addendum of Newer Anticoagulants To The SIR Consensus GuidelineDocument5 pagesAddendum of Newer Anticoagulants To The SIR Consensus GuidelineCenith De Los ReyesNo ratings yet
- Nej Mo A 1210357Document9 pagesNej Mo A 1210357Tasia DeastutiNo ratings yet
- Outcomes After Listing For Liver Transplant in Patients With Acute-on-Chronic Liver Failure - The Multicenter North American Consortium For The Study of End-Stage Liver Disease ExperienceDocument9 pagesOutcomes After Listing For Liver Transplant in Patients With Acute-on-Chronic Liver Failure - The Multicenter North American Consortium For The Study of End-Stage Liver Disease ExperienceRubia Moresi Vianna De OliveiraNo ratings yet
- Liver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientDocument14 pagesLiver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientSowmya ChitraNo ratings yet
- Carotid JCPSP WaDocument4 pagesCarotid JCPSP Washakil11No ratings yet
- Author's Accepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaDocument47 pagesAuthor's Accepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaОлег ПоздняковNo ratings yet
- 1 s2.0 S0870255121005096 MainDocument3 pages1 s2.0 S0870255121005096 MainangelemanuelarmasNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- Clinical Cases in Heart FailureFrom EverandClinical Cases in Heart FailureRavi V. ShahNo ratings yet
- Best 2009Document2 pagesBest 2009JuanNo ratings yet
- Blast Load Analysis and Simulation of Unreinforced Concrete MasonryDocument13 pagesBlast Load Analysis and Simulation of Unreinforced Concrete MasonryJuanNo ratings yet
- Ring 2000Document5 pagesRing 2000JuanNo ratings yet
- Folding Graphene Film Yields High Areal Energy Storage in Lithium-Ion BatteriesDocument8 pagesFolding Graphene Film Yields High Areal Energy Storage in Lithium-Ion BatteriesJuanNo ratings yet
- Synthesis, Crystal Growth and Studies On Non-Linear Optical Property of New ChalconesDocument6 pagesSynthesis, Crystal Growth and Studies On Non-Linear Optical Property of New ChalconesJuanNo ratings yet
- Boutsioukis 2007Document7 pagesBoutsioukis 2007JuanNo ratings yet
- Anti-Semitism at The Opera: The Portrayal of Jews in The: Singspiels Ofreinhard KeiserDocument28 pagesAnti-Semitism at The Opera: The Portrayal of Jews in The: Singspiels Ofreinhard KeiserJuanNo ratings yet
- Uhf Ask Receiver IC U3741BM: FeaturesDocument33 pagesUhf Ask Receiver IC U3741BM: FeaturesBegu CataNo ratings yet
- CDM833 Parts BookDocument163 pagesCDM833 Parts BookThiago Fredy33% (3)
- Circuits SolnDocument5 pagesCircuits Solndwaytikitan28No ratings yet
- Work Energy Chapter Problems-2009-05-13Document21 pagesWork Energy Chapter Problems-2009-05-13Liam ReillyNo ratings yet
- String HandlingDocument33 pagesString HandlingSushíl kanikeNo ratings yet
- Binder 1Document23 pagesBinder 1Lk Soni100% (1)
- Galileo Galilei: Galileo's Study of Pendulums Assisted in The Development of Pendulum ClocksDocument5 pagesGalileo Galilei: Galileo's Study of Pendulums Assisted in The Development of Pendulum ClockswaeyeoNo ratings yet
- Infomationbook 1699Document4 pagesInfomationbook 1699khanhkhanhvo186No ratings yet
- 1.7 Mathematical Analysis of Non Recursive AlgorithmDocument7 pages1.7 Mathematical Analysis of Non Recursive AlgorithmsaiNo ratings yet
- TIA PRO1 07 ProgBlocksDocument24 pagesTIA PRO1 07 ProgBlocksEmilio MonterichelNo ratings yet
- 03 IPv6 RoutingDocument74 pages03 IPv6 Routingguido.martiniNo ratings yet
- Search Courses: My Courses AWS Certi Ed Solutions Architect Associate Simple Storage Service (S3) - QuizDocument55 pagesSearch Courses: My Courses AWS Certi Ed Solutions Architect Associate Simple Storage Service (S3) - QuizAndres GarciaNo ratings yet
- Dbms Lab File FormatDocument11 pagesDbms Lab File Formatshagunverma039No ratings yet
- The Paper 114 PDFDocument32 pagesThe Paper 114 PDFeu mesmoNo ratings yet
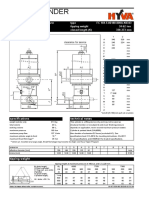
- Hyva CylinderDocument2 pagesHyva CylinderDinifaanNo ratings yet
- Klocke Kroemer ICG15Document11 pagesKlocke Kroemer ICG15ranim najibNo ratings yet
- (2091) Lecture Notes Electrochemistry E.pdf - TMPDocument43 pages(2091) Lecture Notes Electrochemistry E.pdf - TMPRamJiPandeyNo ratings yet
- hp5082 7730 PDFDocument8 pageshp5082 7730 PDFchawkigenieNo ratings yet
- Becoming A Life Coach: Fundamental Life Coaching Tips and TechniquesDocument58 pagesBecoming A Life Coach: Fundamental Life Coaching Tips and Techniquesdiegogrispo6211No ratings yet
- UNIT 3 GRAPHS Class NotesDocument24 pagesUNIT 3 GRAPHS Class NotesSUDHA SNo ratings yet
- FlowCon EVS Tech 08.2013Document7 pagesFlowCon EVS Tech 08.2013Jeff Anderson CollinsNo ratings yet
- Key For Waves Unit II, Worksheet 3: ©modeling Workshop Project 2003 1 W2, Mechanical Waves in 1D, WS 3 Key, v3.0Document3 pagesKey For Waves Unit II, Worksheet 3: ©modeling Workshop Project 2003 1 W2, Mechanical Waves in 1D, WS 3 Key, v3.0cmejdi jNo ratings yet
- CS602 MCQS For Final Term Verified by MastersDocument277 pagesCS602 MCQS For Final Term Verified by MastersjackNo ratings yet
- Physics Blue Print II Puc 2023-24.Document2 pagesPhysics Blue Print II Puc 2023-24.KAUSTUBH RAO KANDULANo ratings yet
- Space and Geometry - DissertationDocument60 pagesSpace and Geometry - DissertationNeha Syal100% (1)
- Electrical Safety: DR N.Vijaya AnandDocument12 pagesElectrical Safety: DR N.Vijaya Anand19501A0455 LOBHISETTI LIKITHANo ratings yet
- UNIT IV 4 DempsterShaferTheoryDocument19 pagesUNIT IV 4 DempsterShaferTheorySravani Srav100% (1)
- ACH550 01 UsermanualDocument474 pagesACH550 01 UsermanualSyed Noman AhmedNo ratings yet
- Topic 14 Bonding HL NotesDocument26 pagesTopic 14 Bonding HL NotesaabbccNo ratings yet
- Two Factors Affecting The Brightness of Led Light Bulb: Sorsogon National High School Sorsogon City S.Y. 2018 - 2019Document4 pagesTwo Factors Affecting The Brightness of Led Light Bulb: Sorsogon National High School Sorsogon City S.Y. 2018 - 2019John KlennNo ratings yet