Download as pdf or txt
You might also like
- Community Health Nursing Astig NurseDocument4 pagesCommunity Health Nursing Astig NurseKristine Singson100% (1)
- P U P M S S D M: Olytechnic Niversity of The HilippinesDocument5 pagesP U P M S S D M: Olytechnic Niversity of The HilippinesAnthony Japhz EmuelNo ratings yet
- Toronto Public Health Absenteeism Notification LetterDocument2 pagesToronto Public Health Absenteeism Notification LetterToronto StarNo ratings yet
- COVID ChildCareProgram Flowchart HDocument1 pageCOVID ChildCareProgram Flowchart HAli Ben HusseinNo ratings yet
- Sample Contingency Plan For Limited F2F ClassesDocument12 pagesSample Contingency Plan For Limited F2F Classeschristian capunongNo ratings yet
- Word ForDocument2 pagesWord ForAnthony Japhz EmuelNo ratings yet
- COVID 19 Health Declaration and Liability Waiver For New Normal CampingDocument2 pagesCOVID 19 Health Declaration and Liability Waiver For New Normal CampingTelapatio Elementary School (R III - Bulacan)No ratings yet
- Back To School During COVID-19 FAQ: ContentsDocument7 pagesBack To School During COVID-19 FAQ: ContentsTaylor MoffittNo ratings yet
- Health Declaration Form F2FDocument1 pageHealth Declaration Form F2FLizette Janiya SumantingNo ratings yet
- Name: Age: Sex: Address: Contact No: Occupation: Body TemperatureDocument2 pagesName: Age: Sex: Address: Contact No: Occupation: Body TemperatureJoshua Christian TeopengcoNo ratings yet
- Best Practices in School in Handling Covid 19 CaseDocument6 pagesBest Practices in School in Handling Covid 19 CaseJayson WongNo ratings yet
- DepEd School Contingency Plan ManualDocument23 pagesDepEd School Contingency Plan ManualJohn Christopher OsorioNo ratings yet
- MDH Guidance For Schools Response To COVID 19 7.21.2020Document4 pagesMDH Guidance For Schools Response To COVID 19 7.21.2020David M. Higgins IINo ratings yet
- WaitingDocument1 pageWaitingdaam naamNo ratings yet
- HDF Entrance Oct 2022Document2 pagesHDF Entrance Oct 2022Lovly YeshyyNo ratings yet
- Chaparral 2nd Notification Letter - 2020 - 10 - 12 PDFDocument1 pageChaparral 2nd Notification Letter - 2020 - 10 - 12 PDFNicole GutierrezNo ratings yet
- To: Parents/Guardians Re: Probable COVID-19 Variant of Concern in School SettingDocument2 pagesTo: Parents/Guardians Re: Probable COVID-19 Variant of Concern in School SettingXian CaesarNo ratings yet
- School Contingency PlanDocument19 pagesSchool Contingency PlanReymond E. Delos ReyesNo ratings yet
- HCSD Student Process Map For COVID - 19Document1 pageHCSD Student Process Map For COVID - 19pearl015No ratings yet
- Reopening Parent Document 3-19-21 English 1Document10 pagesReopening Parent Document 3-19-21 English 1api-237662624No ratings yet
- Dr. Charles R. Drew Science Magnet, PS#59 Will Remain OPEN During This TimeDocument1 pageDr. Charles R. Drew Science Magnet, PS#59 Will Remain OPEN During This Timenilufarrahman26No ratings yet
- HW Health Office Update 12-16-22Document1 pageHW Health Office Update 12-16-22etracyhwhsNo ratings yet
- Return, Recover, Reimagine:: Boston Public SchoolsDocument34 pagesReturn, Recover, Reimagine:: Boston Public SchoolsChristopher GavinNo ratings yet
- School Communication PlanDocument5 pagesSchool Communication PlanReymond E. Delos ReyesNo ratings yet
- CDC COVID QuestionnaireDocument2 pagesCDC COVID QuestionnaireKenneth A. Prado M.No ratings yet
- The Melting Pot DesktoppcDocument4 pagesThe Melting Pot DesktoppcKheiNo ratings yet
- Contingency Plan For Limited Expanded FTF ClassesDocument20 pagesContingency Plan For Limited Expanded FTF ClassesHanne UyNo ratings yet
- 2020-07 Health and Safety Handbook (SY 2020-21) Version 1Document28 pages2020-07 Health and Safety Handbook (SY 2020-21) Version 1HNNNo ratings yet
- COVID Medical FAQ Sheet For ParentsDocument4 pagesCOVID Medical FAQ Sheet For ParentsVinay StokesNo ratings yet
- Hudson COVID Letter August 3 2021Document2 pagesHudson COVID Letter August 3 2021KTARNo ratings yet
- KumonLipaLearningCenter WaiverDocument2 pagesKumonLipaLearningCenter WaiverRyzel Lianna M. IsabedraNo ratings yet
- DepEd School Contingency Plan Manual For The Implementation of Limited Face To Face ClassesDocument27 pagesDepEd School Contingency Plan Manual For The Implementation of Limited Face To Face ClassesMMC BSEDNo ratings yet
- EGSES - Contingency PlanDocument15 pagesEGSES - Contingency PlanEsperanza Quiambao CrisostomoNo ratings yet
- Pup HDFDocument1 pagePup HDFAnthony Japhz EmuelNo ratings yet
- Httpscovid-19.ontario - Caschool-Screeningapproved 2Document1 pageHttpscovid-19.ontario - Caschool-Screeningapproved 2SZNo ratings yet
- Genesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools With Universal Mask MandatesDocument26 pagesGenesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools With Universal Mask MandatesCourtney BennettNo ratings yet
- Student Health Card and Physical Examination Record - 04.03.2017 - FINALDocument4 pagesStudent Health Card and Physical Examination Record - 04.03.2017 - FINALYOONNo ratings yet
- COVID 19 Protocol For Marian Academy: Tel: 592-226-9045 Carifesta Avenue Fax: 592-226-9044 Georgetown Guyana, S.ADocument2 pagesCOVID 19 Protocol For Marian Academy: Tel: 592-226-9045 Carifesta Avenue Fax: 592-226-9044 Georgetown Guyana, S.Aanthony ToddNo ratings yet
- Limited F2F Learning Contingency PlanDocument33 pagesLimited F2F Learning Contingency PlanDaniel MingoyNo ratings yet
- Contingency-Plan-for-COVID-19 - Face-To-Face RequirementsDocument31 pagesContingency-Plan-for-COVID-19 - Face-To-Face Requirementsanier joy sejatnomNo ratings yet
- Sta. Ines Es School Contingency Plan 2021-2022Document28 pagesSta. Ines Es School Contingency Plan 2021-2022Darwin Ignacio DI ChannelNo ratings yet
- Ctes Contingency Plan f2f Sy2022 2023Document8 pagesCtes Contingency Plan f2f Sy2022 2023Angelo Aniag UnayNo ratings yet
- Health Sign Off-March 18-01Document2 pagesHealth Sign Off-March 18-01Jackson SilvaNo ratings yet
- COVID-19 School Screening 2Document1 pageCOVID-19 School Screening 2milamoo425No ratings yet
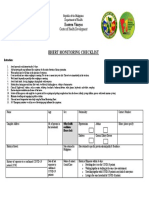
- Bhert Monitoring Checklist: Eastern VisayasDocument1 pageBhert Monitoring Checklist: Eastern VisayasBLGU Lake DanaoNo ratings yet
- Covid-19 Health and Safety GuidanceDocument20 pagesCovid-19 Health and Safety Guidanceapi-494337591No ratings yet
- Schools Modified QuarantineDocument1 pageSchools Modified QuarantineAYOMIDE SILEOLA OLADOSUNo ratings yet
- COVID19 Update - Gulf County: Weekly Update: 8/7-8/13 Totals Since The BeginningDocument8 pagesCOVID19 Update - Gulf County: Weekly Update: 8/7-8/13 Totals Since The Beginningmanager2738No ratings yet
- Moraza ES - Contingency Plan FinalDocument17 pagesMoraza ES - Contingency Plan FinalericaNo ratings yet
- Sta. Ines Es School Contingency Plan 2021-2022Document28 pagesSta. Ines Es School Contingency Plan 2021-2022Darwin Ignacio DI ChannelNo ratings yet
- Blanchard Back To School Plan 2020-2021Document11 pagesBlanchard Back To School Plan 2020-2021KFORNo ratings yet
- 2021-09-05 - Markville SS - General Notification LetterDocument3 pages2021-09-05 - Markville SS - General Notification Letter2044542559lNo ratings yet
- Contingency Plan For Face-to-Face Classes S.Y. 2022-2023Document21 pagesContingency Plan For Face-to-Face Classes S.Y. 2022-2023Mark Jayson Gonzaga100% (2)
- Protocols For Responding To COVID-19 ScenariosDocument19 pagesProtocols For Responding To COVID-19 ScenariosMike CarraggiNo ratings yet
- HCS School Handout SetDocument9 pagesHCS School Handout SetGenevieve GrippoNo ratings yet
- COVID-19 School ScreeningDocument1 pageCOVID-19 School Screeningmilamoo425No ratings yet
- Planco DR ArticleDocument2 pagesPlanco DR ArticleShaira Dawn D. PLANCONo ratings yet
- Care For Vulnerable Populations During COVID-19 PandemicFrom EverandCare For Vulnerable Populations During COVID-19 PandemicNo ratings yet
- Care For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19From EverandCare For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19No ratings yet
- How To Prepare GOLD COMFORT v2Document1 pageHow To Prepare GOLD COMFORT v2RJ DAWATONNo ratings yet
- Tax FinalDocument5 pagesTax FinalRJ DAWATONNo ratings yet
- CivilDocument1 pageCivilRJ DAWATONNo ratings yet
- Riminal Law Final Examination Dean Gemy Lito LDocument8 pagesRiminal Law Final Examination Dean Gemy Lito LRJ DAWATONNo ratings yet
- Important Notes in The Bar ExamsDocument17 pagesImportant Notes in The Bar ExamsRJ DAWATONNo ratings yet
- ConstiDocument1 pageConstiRJ DAWATONNo ratings yet
- SlowDocument2 pagesSlowRJ DAWATONNo ratings yet
- Criminal Law Tanglaw Notes Dean FestinDocument44 pagesCriminal Law Tanglaw Notes Dean FestinRJ DAWATONNo ratings yet
- PUP Health Declaration Form ADocument1 pagePUP Health Declaration Form ARJ DAWATONNo ratings yet
- Barier NursingDocument23 pagesBarier NursingNIVEDITA KOCHARNo ratings yet
- Argument Article Elc 231Document1 pageArgument Article Elc 231izzahNo ratings yet
- Adult Reproductive Health - Keith Nester LavinDocument25 pagesAdult Reproductive Health - Keith Nester LavinKeith LavinNo ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Faq Coliforms Drinking WaterDocument2 pagesFaq Coliforms Drinking WaterTaehyung's WifeNo ratings yet
- MODULE 2: Types of Vaccine and Adverse ReactionsDocument29 pagesMODULE 2: Types of Vaccine and Adverse ReactionsnandaNo ratings yet
- COVID 19 NewsDocument65 pagesCOVID 19 NewsBryce BihagNo ratings yet
- Ivyx Z Fvbivm I Ivyx Z JVBF F VKWMB ..Document2 pagesIvyx Z Fvbivm I Ivyx Z JVBF F VKWMB ..Arafat RinkyNo ratings yet
- Doggy StyleDocument13 pagesDoggy StyleOppaGangnamNo ratings yet
- Epidemiological Literature ReviewDocument8 pagesEpidemiological Literature Reviewafmzbzdvuzfhlh100% (1)
- Infertility: How Does Body Weight Affect The Production of Ova/Sperm?Document3 pagesInfertility: How Does Body Weight Affect The Production of Ova/Sperm?Robin jake SorianoNo ratings yet
- CHCECE002 - Ensure The Health and Safety of ChildrenDocument8 pagesCHCECE002 - Ensure The Health and Safety of ChildrenGisele SilvestreNo ratings yet
- Barangay Officials, SKS, Barangay Workers & Barangay TanodsDocument2 pagesBarangay Officials, SKS, Barangay Workers & Barangay TanodsCristina MelloriaNo ratings yet
- ScriptDocument4 pagesScriptJasper AriapNo ratings yet
- 5 Hiv Aids in PregnancyDocument26 pages5 Hiv Aids in PregnancyBethelAberaHaydamoNo ratings yet
- Lione of WarDocument41 pagesLione of WarLeonard PiusNo ratings yet
- All You Need To Know About: COVID Vaccine SafetyDocument199 pagesAll You Need To Know About: COVID Vaccine SafetyaijazNo ratings yet
- Street Food PolicyDocument78 pagesStreet Food PolicyAnthony AlesnaNo ratings yet
- Regresi Logistik - BahanDocument89 pagesRegresi Logistik - BahanDevi YuliaNo ratings yet
- Topic 9 Infection Prevention and Control: Patient Safety Curriculum GuideDocument17 pagesTopic 9 Infection Prevention and Control: Patient Safety Curriculum GuideIndahEkaPutriNo ratings yet
- Project:: Augmentation of Water Supply & Construction of 37Mld Capacity Water Treatment Plant at AizawlDocument5 pagesProject:: Augmentation of Water Supply & Construction of 37Mld Capacity Water Treatment Plant at Aizawlepe civil1No ratings yet
- A Study To Assess The Knowledge Regarding Cervical Cancer Among Women in Selected Community Setting, ChennaiDocument3 pagesA Study To Assess The Knowledge Regarding Cervical Cancer Among Women in Selected Community Setting, ChennaiEditor IJTSRDNo ratings yet
- DCF Internal Report of Chance Walsh DeathDocument6 pagesDCF Internal Report of Chance Walsh DeathNews-PressNo ratings yet
- Infant Mortality Rate in IndiaDocument22 pagesInfant Mortality Rate in Indiaboogeyman1990No ratings yet
- Medical Care After Cat Bites A Typical Case and Re Alo1661346855153Document4 pagesMedical Care After Cat Bites A Typical Case and Re Alo1661346855153laksonoNo ratings yet
- History of PlumbingDocument45 pagesHistory of PlumbingWinnieBlancoAlabanJr.No ratings yet
- Perinatal & Neonatal Mortality RateDocument20 pagesPerinatal & Neonatal Mortality RateRida GillNo ratings yet
- Final Key 12-2010 PDFDocument14 pagesFinal Key 12-2010 PDFAbubakar AbdhooNo ratings yet
- Tugas Individu Bahasa Inggris-EliskaDocument4 pagesTugas Individu Bahasa Inggris-Eliskaambaria hasib100% (1)
- Emergency ContraceptionDocument24 pagesEmergency Contraceptionfarmasi_hm100% (1)