Download as pdf or txt
You might also like
- Laboratory Manual For Anatomy and Physiology 6th Edition Marieb Solutions ManualDocument7 pagesLaboratory Manual For Anatomy and Physiology 6th Edition Marieb Solutions Manualhanhgiaoghhr100% (37)
- Viteri2018 Prevalensi 5Document17 pagesViteri2018 Prevalensi 5adrian revoNo ratings yet
- Plant FDocument5 pagesPlant Fny neNo ratings yet
- Patho 2 Important QuestionsDocument54 pagesPatho 2 Important QuestionsSadanand DubeyNo ratings yet
- Benigno: T.locoliaoeat - EsDocument8 pagesBenigno: T.locoliaoeat - EsTeonaNo ratings yet
- Anatomy NotesDocument12 pagesAnatomy Notesm.nicoaraNo ratings yet
- CH 28 - AlgaeDocument3 pagesCH 28 - AlgaeElle QuizonNo ratings yet
- Lab Kingdom Animalia PDFDocument8 pagesLab Kingdom Animalia PDFJamesea MilesNo ratings yet
- EmbryologyDocument15 pagesEmbryologyKoushal Sharma, JammuNo ratings yet
- Climatic: SomesDocument8 pagesClimatic: SomesDaliNo ratings yet
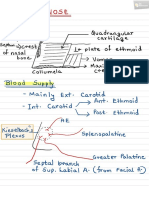
- Nose PDFDocument6 pagesNose PDFNiranjanPandeyNo ratings yet
- Final DermatologyDocument6 pagesFinal DermatologyrahulNo ratings yet
- HNF BDocument8 pagesHNF Bjb0647564No ratings yet
- Anatomy 2Document1 pageAnatomy 2Casey Rae YanoNo ratings yet
- SF2 - Lecture-03 - Cell The Unit of Life - NotesDocument11 pagesSF2 - Lecture-03 - Cell The Unit of Life - Notesdisha shuklaNo ratings yet
- MycoBacteria, Gram Positive - Summary For Med StudentsDocument3 pagesMycoBacteria, Gram Positive - Summary For Med StudentsrefuapalackyNo ratings yet
- Urethra and PenisDocument17 pagesUrethra and PenisSakshi RamtekeNo ratings yet
- Mepioti Tistowgicaratnotioypipeete: QP - Info#Mtuystaoswpivd2I-D23Document23 pagesMepioti Tistowgicaratnotioypipeete: QP - Info#Mtuystaoswpivd2I-D23Nikita VermaNo ratings yet
- Cerebrum Dan CerebellumDocument24 pagesCerebrum Dan CerebellumGek NissaNo ratings yet
- EmbryologyDocument8 pagesEmbryologyjb0647564No ratings yet
- NeuropediatriDocument1 pageNeuropediatriDigital Study 101No ratings yet
- Muestras Histologia MorfoDocument15 pagesMuestras Histologia MorfoluisavaleriaccNo ratings yet
- NematodesDocument4 pagesNematodeshazelloraenne.conarcoNo ratings yet
- Cell CycleDocument1 pageCell CycleAvinashNo ratings yet
- 9-2+EWS+Cnidarians. Valentina TamayoDocument1 page9-2+EWS+Cnidarians. Valentina TamayoValentina Tamayo ArangoNo ratings yet
- Guide Gi CancerDocument1 pageGuide Gi Cancerapi-446887131No ratings yet
- PathologyDocument64 pagesPathology2021004207.garimaNo ratings yet
- Reproduction at The Cellular LevelDocument7 pagesReproduction at The Cellular LevelDaniel JungNo ratings yet
- Gram Negative Bacilli - RespiratoryDocument4 pagesGram Negative Bacilli - RespiratoryrefuapalackyNo ratings yet
- Blood PhysiologyDocument1 pageBlood PhysiologyAnshu SharmaNo ratings yet
- Osce (Tourniquet Dan Besresdka)Document1 pageOsce (Tourniquet Dan Besresdka)LILIANA DEWINo ratings yet
- EndocrineDocument19 pagesEndocrineIsabel Bibat DavidNo ratings yet
- PleuraDocument3 pagesPleuraAmrinder MaanNo ratings yet
- T2 Histology of Epithelial, Connective, and Muscle TissueDocument86 pagesT2 Histology of Epithelial, Connective, and Muscle TissueretterateNo ratings yet
- GastroDocument9 pagesGastroJoshua AtienzaNo ratings yet
- Adobe Scan 07-Mar-2023Document1 pageAdobe Scan 07-Mar-2023Vriddhi AhujaNo ratings yet
- 11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - NotesDocument16 pages11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - Notesdisha shuklaNo ratings yet
- EmbryologyDocument1 pageEmbryologyprasannaipad324No ratings yet
- Do Not Delete (Chick-God)Document6 pagesDo Not Delete (Chick-God)Ricky Justin NgoNo ratings yet
- 01 Bio 3Document1 page01 Bio 3LovialNo ratings yet
- Laboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFDocument28 pagesLaboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFJohnathanFitzgeraldnwoa100% (13)
- Important Questions - Answers 2Document9 pagesImportant Questions - Answers 2singhshreya.0214No ratings yet
- Unit 5Document7 pagesUnit 5Leen Al-FouzanNo ratings yet
- Biology O Level Summary NotesDocument5 pagesBiology O Level Summary NotesAdriana MuzfirahNo ratings yet
- Bedah 2 Dr. UswaDocument36 pagesBedah 2 Dr. UswaSiq Febri SmnjtkNo ratings yet
- Bedah-1 RetakerDocument28 pagesBedah-1 Retakersuci gustiNo ratings yet
- DevBio Lec Intro Part 4Document1 pageDevBio Lec Intro Part 4amydumpling9No ratings yet
- Filogenia de Briofitos SensulatoDocument1 pageFilogenia de Briofitos SensulatoYuyitoS2714No ratings yet
- IB Cell Division NoteDocument1 pageIB Cell Division Note다윤No ratings yet
- OrtopedieDocument40 pagesOrtopedieNaomi CurcanuNo ratings yet
- Notebook PDFDocument1 pageNotebook PDFJong PetchinNo ratings yet
- Digestion - 2Document4 pagesDigestion - 2aaravrshah14No ratings yet
- Biology 10.1 MeiosisDocument1 pageBiology 10.1 MeiosisAleksandra LukanovskaNo ratings yet
- Kidneys - FactRecallDocument2 pagesKidneys - FactRecallsabinaNo ratings yet
- Mitosis &meiosis I and II QuestionDocument3 pagesMitosis &meiosis I and II Questionغدي بنت بن قاعدNo ratings yet
- Magee 6th Edition - OPA - 4 Temporomandibular JointDocument30 pagesMagee 6th Edition - OPA - 4 Temporomandibular JointRonny Araya AbarcaNo ratings yet
- Animalia File 2023-1Document12 pagesAnimalia File 2023-1Syed Zee Waqar GillaniNo ratings yet
- Maxdmiaanmetieraneemingigmei - Ec/'s :.nia::nanieai: Inferior LungDocument1 pageMaxdmiaanmetieraneemingigmei - Ec/'s :.nia::nanieai: Inferior LungElaineNo ratings yet
- Chapter 7 Protista and Fungi-1Document5 pagesChapter 7 Protista and Fungi-1muhammad shoaibNo ratings yet
- Adobe Scan 02 Jan 2023Document1 pageAdobe Scan 02 Jan 2023KRITTIKAA PARAMANICKNo ratings yet
- Comprehensive Pediatric NephrologyDocument3 pagesComprehensive Pediatric NephrologyFadel BilondatuNo ratings yet
- Urinary Pics ADocument22 pagesUrinary Pics A46bwilsonNo ratings yet
- Paediatric Nephrology Syllabus FinalDocument13 pagesPaediatric Nephrology Syllabus FinalClever BarbieNo ratings yet
- CASESTUDY PyelonephritisDocument37 pagesCASESTUDY Pyelonephritisyasira100% (1)
- 62-Article Text-58-1-10-20190528 PDFDocument5 pages62-Article Text-58-1-10-20190528 PDFputri vinia /ilove cuteNo ratings yet
- Management of Pregnant Patient in DentistryDocument10 pagesManagement of Pregnant Patient in DentistryVíctor Orduña LópezNo ratings yet
- Crisis Trauma: WWW - Eastzonemedico.co M WWW - Eastzonemedico.inDocument14 pagesCrisis Trauma: WWW - Eastzonemedico.co M WWW - Eastzonemedico.inswipetoplay32No ratings yet
- Slide Urine RetentionDocument25 pagesSlide Urine RetentionResky Alfiansyah ANo ratings yet
- 2 - Renal PhysiologyDocument8 pages2 - Renal PhysiologyKunware TropaNo ratings yet
- Icd 10 Excell NewDocument491 pagesIcd 10 Excell Newlilik fitriatulNo ratings yet
- 2023 - 01 - 23 1 - 17 PM Office LensDocument6 pages2023 - 01 - 23 1 - 17 PM Office LensKUMAR SUMITNo ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- Mcqs On Excretory SystemDocument3 pagesMcqs On Excretory SystemIshfaq Lone100% (1)
- Excretion & Osmoregulation: 16. Highlights of This TopicDocument41 pagesExcretion & Osmoregulation: 16. Highlights of This TopicSAGAR PADALKARNo ratings yet
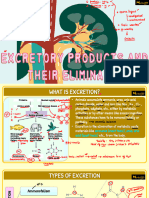
- Vipin Sir Biology 19. Excretory Products and Their EliminationDocument55 pagesVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisNo ratings yet
- Agrimony Agrimonia Eupatoria KeelDocument12 pagesAgrimony Agrimonia Eupatoria KeelAlejandra Guerrero100% (2)
- GlomerulonephritisDocument1 pageGlomerulonephritismaleskunNo ratings yet
- A Case Study On A Pediatric Patient Diagnosed With Urinary Tract InfectionDocument55 pagesA Case Study On A Pediatric Patient Diagnosed With Urinary Tract InfectionADOLF FRUELAN HIDALGO100% (1)
- PREECLAMPSIADocument93 pagesPREECLAMPSIADaly L. Nacional100% (1)
- Chemical PathologyDocument8 pagesChemical PathologyBobskinnyNo ratings yet
- 211102-113535529 Muntazir 21Y 02-Nov-2021 IMG-1115332275 MaleDocument1 page211102-113535529 Muntazir 21Y 02-Nov-2021 IMG-1115332275 MaleMuntazir MehdiNo ratings yet
- DR Shirin Surani Resident Year 1Document29 pagesDR Shirin Surani Resident Year 1arjumandNo ratings yet
- Zinner's Syndrome: A New Asymptomatic Case ReportDocument3 pagesZinner's Syndrome: A New Asymptomatic Case ReportasclepiuspdfsNo ratings yet
- Anatomy N Physiology of UtiDocument6 pagesAnatomy N Physiology of UtiMarjorie PalaganasNo ratings yet
- The Organ System of The Human BodyDocument45 pagesThe Organ System of The Human Bodymonch1998100% (3)
- Physiological Changes During Pregnancy 2010Document42 pagesPhysiological Changes During Pregnancy 2010Asyhok Renault100% (1)
- Diagnostic Imaging of Lower Urinary Tract DiseaseDocument25 pagesDiagnostic Imaging of Lower Urinary Tract DiseaseSoyKlicheRodriguezNo ratings yet
- J Jcpa 2020 09 008Document6 pagesJ Jcpa 2020 09 008Valentina UribeNo ratings yet
- KB 10Document5 pagesKB 10Reband AzadNo ratings yet