Download as pdf or txt
You might also like
- Hematologic Disorders NCLEXDocument15 pagesHematologic Disorders NCLEXPotchiee PfizerNo ratings yet
- Study Log 1 Objective CheckDocument3 pagesStudy Log 1 Objective CheckWindi Dawn SallevaNo ratings yet
- Sickle Cell CrisisDocument16 pagesSickle Cell Crisismardsz83% (12)
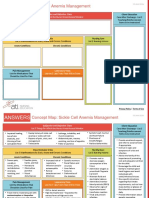
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Axelsson 2012Document11 pagesAxelsson 2012happyNo ratings yet
- Valvular Heart Disease EscDocument96 pagesValvular Heart Disease EscleonelcaolNo ratings yet
- Valvular Esc Book ChapterDocument96 pagesValvular Esc Book ChapterkikiwulandariNo ratings yet
- JCM 10 03239Document42 pagesJCM 10 03239Pamela MusabelliuNo ratings yet
- Declining Case Fatality Rates For Severe Sepsis Good Data Bring Good News With Ambiguous ImplicationsDocument3 pagesDeclining Case Fatality Rates For Severe Sepsis Good Data Bring Good News With Ambiguous ImplicationsRodrigoSachiFreitasNo ratings yet
- Physical Activity and Pain in Youth With Sickle Cell DiseaseDocument9 pagesPhysical Activity and Pain in Youth With Sickle Cell DiseaseTowhid HasanNo ratings yet
- J Deutsche Derma Gesell - 2017 - Santler - Chronic Venous Insufficiency A Review of Pathophysiology Diagnosis andDocument19 pagesJ Deutsche Derma Gesell - 2017 - Santler - Chronic Venous Insufficiency A Review of Pathophysiology Diagnosis andNathan MarquezNo ratings yet
- Determinants of Costs of Care For Patients With Alzheimer's DiseaseDocument11 pagesDeterminants of Costs of Care For Patients With Alzheimer's DiseaseBenny TjanNo ratings yet
- U.S. Department of Veterans AffairsDocument18 pagesU.S. Department of Veterans AffairsemiNo ratings yet
- Identifying Pain and Effects On Quality of Life From Chronic Wounds Secondary To Lower-Extremity Vascular DiseaseDocument7 pagesIdentifying Pain and Effects On Quality of Life From Chronic Wounds Secondary To Lower-Extremity Vascular DiseasecumbredinNo ratings yet
- ACS - Clinical Review 2015Document11 pagesACS - Clinical Review 2015Purwoko SugengNo ratings yet
- 325 FullDocument20 pages325 FullDessyadoeNo ratings yet
- Vascular Abnormalities of SSCDocument9 pagesVascular Abnormalities of SSCCristina ElenaNo ratings yet
- Infecã Ã o e Doenã A CV JACCDocument10 pagesInfecã Ã o e Doenã A CV JACCgpxwdfbqfdNo ratings yet
- Deep Venous Thrombosis 2022. ANNALSDocument20 pagesDeep Venous Thrombosis 2022. ANNALSErnesto LainezNo ratings yet
- Damage Control Surge With.17Document11 pagesDamage Control Surge With.17Mateo Saenz RengifoNo ratings yet
- Cardiovascular Risks Associated With Incident and Prevalent Periodontal DiseaseDocument8 pagesCardiovascular Risks Associated With Incident and Prevalent Periodontal DiseaseAlyaefkageNo ratings yet
- The Impact of Pruritus On Quality of LifeDocument4 pagesThe Impact of Pruritus On Quality of LifeRamona VintilaNo ratings yet
- (Jurnal) Palliative and End-Of-life Care Issues in Chronic Kidney DiseaseDocument10 pages(Jurnal) Palliative and End-Of-life Care Issues in Chronic Kidney DiseaseRizqi DifaNo ratings yet
- Sepsis - Epidemiology Pathophysiology Classification BiomarkersDocument9 pagesSepsis - Epidemiology Pathophysiology Classification BiomarkersFaisal MohammedNo ratings yet
- Acute Coronary Syndromes CompendiumDocument17 pagesAcute Coronary Syndromes CompendiumInasNo ratings yet
- Perioperative Management of Elderly Patients With Hip FractureDocument6 pagesPerioperative Management of Elderly Patients With Hip FractureTinky WinkyNo ratings yet
- Strokeaha 110 610881Document5 pagesStrokeaha 110 610881Damilola AdediniNo ratings yet
- Cellulitis of The Lower Limbs: Incidence, Diagnosis and ManagementDocument4 pagesCellulitis of The Lower Limbs: Incidence, Diagnosis and Managementjenifer paathNo ratings yet
- Cellulitis Incidence in A Defined PopulationDocument7 pagesCellulitis Incidence in A Defined PopulationIsabela MartinsNo ratings yet
- Diare QuebecDocument7 pagesDiare QuebecfadliNo ratings yet
- 61 13 163 1 10 20170731Document6 pages61 13 163 1 10 20170731rundyiramaNo ratings yet
- Berardi Et Al. - Diagnostics - 2021 - A Pound of Flesh What Cachexia Is and What It Is NotDocument19 pagesBerardi Et Al. - Diagnostics - 2021 - A Pound of Flesh What Cachexia Is and What It Is NotLievenNo ratings yet
- GES1 - Dolor - 02Document17 pagesGES1 - Dolor - 02jquer17No ratings yet
- Circulation 2022 146 25 1903-17Document15 pagesCirculation 2022 146 25 1903-17silviaNo ratings yet
- Systemic Sclerosis-Associated Intersititial Lung DiseaseDocument17 pagesSystemic Sclerosis-Associated Intersititial Lung DiseaseAlfi RahmatikaNo ratings yet
- Diverticular Disease: Epidemiology and Management: ReviewDocument5 pagesDiverticular Disease: Epidemiology and Management: ReviewmunazilatulchasanahNo ratings yet
- 2015 Article 367 PDFDocument8 pages2015 Article 367 PDFJesse CusterNo ratings yet
- Pain Mechanisms in Vascular Disease - Dor VascularDocument12 pagesPain Mechanisms in Vascular Disease - Dor VascularAllsNo ratings yet
- Sickle Cell Anemia Students Name Professor's Name Institutional Affiliation Course Unit DateDocument6 pagesSickle Cell Anemia Students Name Professor's Name Institutional Affiliation Course Unit Datejob ominoNo ratings yet
- Chronic Kidney Disease and AnaesthesiaDocument8 pagesChronic Kidney Disease and AnaesthesiaJossiel OlivaresNo ratings yet
- Treatment in The Home Setting With Intermittent Pneumatic Compression For A Woman With Chronic Leg Ulcers: A CaseDocument6 pagesTreatment in The Home Setting With Intermittent Pneumatic Compression For A Woman With Chronic Leg Ulcers: A CaseLinda PermatasariNo ratings yet
- U-Health For Management of Chronic Diseases: - Physical Activity and Therapeutic ExerciseDocument10 pagesU-Health For Management of Chronic Diseases: - Physical Activity and Therapeutic Exercisekang soon cheolNo ratings yet
- Mayoclinproc 84 12 012 PDFDocument17 pagesMayoclinproc 84 12 012 PDFMokaNo ratings yet
- Merolla 2015Document8 pagesMerolla 2015Sandro RolimNo ratings yet
- Samson Et Al - Psychosocial Adaptation To Chronic IllnessDocument13 pagesSamson Et Al - Psychosocial Adaptation To Chronic IllnessRaquel PintoNo ratings yet
- Acute Kidney Injury1Document16 pagesAcute Kidney Injury1Hmn07No ratings yet
- Been Hospitalized For 143 Days. ITP, TreatedDocument78 pagesBeen Hospitalized For 143 Days. ITP, TreatedSutapa PawarNo ratings yet
- Definiciones PreviasDocument7 pagesDefiniciones PreviasJuan RodriguezNo ratings yet
- Management of Lower Extremity Pain From Chronic Venous Insufficiency: A Comprehensive ReviewDocument30 pagesManagement of Lower Extremity Pain From Chronic Venous Insufficiency: A Comprehensive Reviewangeline chandraNo ratings yet
- 12 Ustundag Orignial 9 3Document8 pages12 Ustundag Orignial 9 3Sanjivi GovekarNo ratings yet
- DVT PreventionDocument8 pagesDVT PreventionRonald ThakorNo ratings yet
- Medical Comorbidity in Alzheimer's 2 Disease: A Nested Case-Control StudyDocument9 pagesMedical Comorbidity in Alzheimer's 2 Disease: A Nested Case-Control StudyOncología CdsNo ratings yet
- Good 1 A - Non-Healing - Lesion - On - The - AnDocument4 pagesGood 1 A - Non-Healing - Lesion - On - The - AnAhmad Umar MukhtarNo ratings yet
- JTD 11 01 21Document8 pagesJTD 11 01 21Kornelis AribowoNo ratings yet
- Rheumatoid ArthritisDocument11 pagesRheumatoid Arthritismelinda tannousNo ratings yet
- Angina Pectoris Pharmacological and Acupuncture TherapyDocument5 pagesAngina Pectoris Pharmacological and Acupuncture TherapyEditor IJTSRDNo ratings yet
- Discitis: EviewDocument7 pagesDiscitis: EviewKarina PortilloNo ratings yet
- Geriatric Renal Paliative Care 2012Document10 pagesGeriatric Renal Paliative Care 2012Marcela De La PazNo ratings yet
- Multiple and Mixed Valvular Heart DiseaseDocument13 pagesMultiple and Mixed Valvular Heart DiseaseВенцислав МирчевNo ratings yet
- Ok DeLaCruz2022Document8 pagesOk DeLaCruz2022Lara ReisNo ratings yet
- Evaluation of Crush Syndrome Patients With Extremity Injuries in The 2011 Van Earthquake in TurkeyDocument7 pagesEvaluation of Crush Syndrome Patients With Extremity Injuries in The 2011 Van Earthquake in Turkeysiti fatimahNo ratings yet
- CTS MHDDocument8 pagesCTS MHDTheodoreNo ratings yet
- Fast Facts: Multiple Sclerosis: A new era of disease modification and treatmentFrom EverandFast Facts: Multiple Sclerosis: A new era of disease modification and treatmentNo ratings yet
- Vasculitis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandVasculitis, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Sickle Cell: Kelompok 1 1. Alestya Febrimaharani 2. Iftah Shorayya 3. Lastri Sulastri 4. Siti ShopiaturohmahDocument15 pagesSickle Cell: Kelompok 1 1. Alestya Febrimaharani 2. Iftah Shorayya 3. Lastri Sulastri 4. Siti ShopiaturohmahErnesta Saulina DewiNo ratings yet
- Hemoglobin and Myoglobin Structure and FunctionDocument23 pagesHemoglobin and Myoglobin Structure and FunctionHarun MohamedNo ratings yet
- Thesis - Tracy O. BonsuDocument97 pagesThesis - Tracy O. BonsusnNo ratings yet
- Principles of Biostatistics: Pubh605 (3 Credit Hours)Document17 pagesPrinciples of Biostatistics: Pubh605 (3 Credit Hours)eshet chafNo ratings yet
- Anaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarDocument82 pagesAnaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarReshu ThakuriNo ratings yet
- SUMMATIVE ASSESSMENT Q4 Week 2Document7 pagesSUMMATIVE ASSESSMENT Q4 Week 2Em-Em Alonsagay Dollosa100% (1)
- Sickle Cell AnemiaDocument37 pagesSickle Cell Anemiahazelposis75% (4)
- Internalization of Care: A Qualitative Study With Schoolchildren Living With Sickle Cell DiseaseDocument8 pagesInternalization of Care: A Qualitative Study With Schoolchildren Living With Sickle Cell Diseaseduvan solanoNo ratings yet
- Gene Therapy.Document3 pagesGene Therapy.Louisse Angeli AbucejoNo ratings yet
- Ciulla HemaDocument35 pagesCiulla HemaLancer BlazeNo ratings yet
- Bleeding Disorders During Pregnancy 1.threatened MiscarriageDocument12 pagesBleeding Disorders During Pregnancy 1.threatened MiscarriageKish Gabriel100% (1)
- Alteration in OxygenationDocument8 pagesAlteration in Oxygenationraquel maniegoNo ratings yet
- Hematologic DisordersDocument108 pagesHematologic DisordersEmma IntiaNo ratings yet
- Variation & Selection 3 QP-merged PDFDocument138 pagesVariation & Selection 3 QP-merged PDFrachitNo ratings yet
- Rodaks Hematology Clinical Principles and Application 5th Edition 2 ParteDocument475 pagesRodaks Hematology Clinical Principles and Application 5th Edition 2 Partekrisha padillaNo ratings yet
- Sickle Cell AnaemiaDocument6 pagesSickle Cell AnaemiaJap ReniNo ratings yet
- Splenectomy For Hematologic DisordersDocument8 pagesSplenectomy For Hematologic DisordersShofa NisaNo ratings yet
- CLM PresentationDocument13 pagesCLM PresentationHSC UNITED100% (1)
- Family Origin Questionnaire - DOC-72001 PDFDocument2 pagesFamily Origin Questionnaire - DOC-72001 PDFNathan WatkinsNo ratings yet
- Science Form 4 MutationDocument21 pagesScience Form 4 MutationAsyrafAlvezNo ratings yet
- Children and Their Development Canadian 3rd Edition Kail Test BankDocument57 pagesChildren and Their Development Canadian 3rd Edition Kail Test BankBrianYorktnqsw100% (14)
- The Making of The Fittest: Natural Selection in Humans: Quiz Student HandoutDocument4 pagesThe Making of The Fittest: Natural Selection in Humans: Quiz Student HandoutBeverly Carballo - MoguelNo ratings yet
- IB Biology Notes - 41 Chromosomes, Genes, Alleles and MutationsDocument2 pagesIB Biology Notes - 41 Chromosomes, Genes, Alleles and MutationsJohn Philip D. NapalNo ratings yet
- AnemiaDocument145 pagesAnemiaTegegne WorkNo ratings yet
- A Case-Control Study in Northern Liberia of Plasmodium Falciparum Malaria in Haemoglobin S and - Thalassaemia TraitsDocument9 pagesA Case-Control Study in Northern Liberia of Plasmodium Falciparum Malaria in Haemoglobin S and - Thalassaemia TraitsAnn Irene DomnicNo ratings yet
- Nucleic Acids: Experiment # 12Document4 pagesNucleic Acids: Experiment # 12Princes Viña Dalisay PauloNo ratings yet