Download as pdf or txt
You might also like
- Management of Temporomandibular Disorders: A Rapid Review of Systematic Reviews and GuidelinesDocument15 pagesManagement of Temporomandibular Disorders: A Rapid Review of Systematic Reviews and Guidelinesnabila puspitaNo ratings yet
- Nbde Part 2 El Maestro 1Document209 pagesNbde Part 2 El Maestro 1Ahmed Elsherbini100% (4)
- Dentin As A Bonding SubstrateDocument27 pagesDentin As A Bonding SubstrateAle MonzalvoNo ratings yet
- Cawson S MCQs in Dentistry PDFDocument171 pagesCawson S MCQs in Dentistry PDFOmar Siddig100% (9)
- Drill Less Air AbrasionDocument4 pagesDrill Less Air AbrasionMaria IvanaNo ratings yet
- Accelerated Fatigue Resistance of Thick CAD/CAM Composite Resin Overlays Bonded With Light - and Dual-Polymerizing Luting ResinsDocument8 pagesAccelerated Fatigue Resistance of Thick CAD/CAM Composite Resin Overlays Bonded With Light - and Dual-Polymerizing Luting ResinsTiago SpeziaNo ratings yet
- Influence of Restoration Thickness and Dental Bonding Surface On The Fracture Resistance of Full-Coverage Occlusal Veneers Made From Lithium Disilicate CeramicDocument9 pagesInfluence of Restoration Thickness and Dental Bonding Surface On The Fracture Resistance of Full-Coverage Occlusal Veneers Made From Lithium Disilicate CeramicKennya GarnicaNo ratings yet
- Immediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-AnalysisDocument7 pagesImmediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-Analysismarlene tamayoNo ratings yet
- Treating The Mother of Black Triangles With Bioclear VeneersDocument4 pagesTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicNo ratings yet
- Efficacy of Resin Coating On Strengths of Resin Cement To DentinDocument9 pagesEfficacy of Resin Coating On Strengths of Resin Cement To DentinAli Al-QaysiNo ratings yet
- Color Atlas of EndoDocument203 pagesColor Atlas of Endooana_en100% (23)
- Advanced EndodonticsDocument375 pagesAdvanced EndodonticsSaleh Alsadi100% (1)
- MCQ Review For Saudi Licensing Exam (SLE)Document0 pagesMCQ Review For Saudi Licensing Exam (SLE)Rakesh Kumar83% (6)
- Vital Therapy in Carious ToothDocument9 pagesVital Therapy in Carious ToothAsh PeiNo ratings yet
- Prepared Cavities On The StrenDocument4 pagesPrepared Cavities On The StrenPriyank RaiNo ratings yet
- Longevity and Reasons For Failure of Sandwich and Total-Etch Posterior Composite Resin RestorationsDocument7 pagesLongevity and Reasons For Failure of Sandwich and Total-Etch Posterior Composite Resin RestorationsMAYRA ALEJANDRA BAHAMON TRUJILLONo ratings yet
- Selective Caries ExcavationDocument10 pagesSelective Caries Excavationjorefe12No ratings yet
- Anderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinDocument4 pagesAnderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinОлександр БайдоNo ratings yet
- Orthodontics For Undersized Teeth: The Bioclear MethodDocument7 pagesOrthodontics For Undersized Teeth: The Bioclear MethodThe Bioclear ClinicNo ratings yet
- Silorane CompztDocument5 pagesSilorane CompztNaila AmanNo ratings yet
- Deep Margin ElevationDocument1 pageDeep Margin ElevationJazNo ratings yet
- IJEDe 15 03 Rocca 852 2Document22 pagesIJEDe 15 03 Rocca 852 2hannaly estradaNo ratings yet
- Journal-A Dental Esthetic Checklist For Treatment Planning in Esthetic DentistryDocument8 pagesJournal-A Dental Esthetic Checklist For Treatment Planning in Esthetic Dentistryalmond_pretzelNo ratings yet
- Time To Shift - From Scaling and Root Planing To Root Surface DebridementDocument5 pagesTime To Shift - From Scaling and Root Planing To Root Surface DebridementYing Yi TeoNo ratings yet
- CPR For The Worn DentitionDocument17 pagesCPR For The Worn DentitionGustavo A OrtegonNo ratings yet
- Artigo 4Document14 pagesArtigo 4joao pauloNo ratings yet
- Reconstruction of The Lost Interproximal Papilla - Presentation of Surgical and Nonsurgical Approaches.Document14 pagesReconstruction of The Lost Interproximal Papilla - Presentation of Surgical and Nonsurgical Approaches.EugenioNo ratings yet
- Kurtzman Restoration of Endodontically Treated TeethDocument8 pagesKurtzman Restoration of Endodontically Treated TeethAdelia CaryabudiNo ratings yet
- Linkevisius Ti-BaseDocument6 pagesLinkevisius Ti-Basekatherina rozicNo ratings yet
- Bleaching of Severely Darkened Nonvital Tooth Case - 48 Months Clinical ControlDocument8 pagesBleaching of Severely Darkened Nonvital Tooth Case - 48 Months Clinical ControlPriska talithaNo ratings yet
- The Use of Separating Rings in The Placement of Class II Composite ResinsDocument9 pagesThe Use of Separating Rings in The Placement of Class II Composite ResinsLeslie MorrowNo ratings yet
- Accuracy of Digital Impressions of Multiple Dental Implants An in Vitro StudyDocument6 pagesAccuracy of Digital Impressions of Multiple Dental Implants An in Vitro StudyFellipeCarvalhoNo ratings yet
- Smile Analysis What To MeasureDocument6 pagesSmile Analysis What To MeasureAli RazaNo ratings yet
- Clinical Aids Manipulation of Rubber Dam Septa: An Aid To The Meticulous Isolation of Splinted ProsthesesDocument4 pagesClinical Aids Manipulation of Rubber Dam Septa: An Aid To The Meticulous Isolation of Splinted ProsthesesAlfred Orozco100% (1)
- Layers (2) Direct Composites-14Document30 pagesLayers (2) Direct Composites-14arangoanNo ratings yet
- Inside Outside Bleaching Technique - Poyser NJ, Kelleher MGD PDFDocument8 pagesInside Outside Bleaching Technique - Poyser NJ, Kelleher MGD PDFAndykaYayanSetiawanNo ratings yet
- DelipariJAD2008 RibbondPostDocument8 pagesDelipariJAD2008 RibbondPostDeno MerindaNo ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- Biologic Interfaces in Esthetic Dentistry Part IIDocument27 pagesBiologic Interfaces in Esthetic Dentistry Part IINoelia MadrizNo ratings yet
- Review On Internal BleachingDocument6 pagesReview On Internal Bleachingpiece_of_mindzz1969No ratings yet
- Erosion Guidelines - 2021 - V4 - MJDocument32 pagesErosion Guidelines - 2021 - V4 - MJAARON DIAZ RONQUILLONo ratings yet
- Real-Time In-Depth Imaging of Gap Formation in Bulk-Fill Resin CompositesDocument12 pagesReal-Time In-Depth Imaging of Gap Formation in Bulk-Fill Resin CompositesPaula Francisca MoragaNo ratings yet
- Eur JEsthet Dent 2013 MeyenbergDocument97 pagesEur JEsthet Dent 2013 Meyenbergsoma kiranNo ratings yet
- Crown and Post-Free Adhesive Restorations For Endodontically Treated Posterior Teeth From Direct Composite To Endocrowns-Stappert 2008Document8 pagesCrown and Post-Free Adhesive Restorations For Endodontically Treated Posterior Teeth From Direct Composite To Endocrowns-Stappert 2008Dan MPNo ratings yet
- Pulp Dentin BiologyDocument21 pagesPulp Dentin BiologyCristiane VazNo ratings yet
- The Influence of Resin Cements On The Final Color of Ceramic VeneersDocument6 pagesThe Influence of Resin Cements On The Final Color of Ceramic VeneersBernny DaniloNo ratings yet
- Deliperi S - PPAD - 2005 PDFDocument9 pagesDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance - A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance - A ReviewInside Dentistry educationNo ratings yet
- Practical Advanced Periodontal Surgery 2020Document240 pagesPractical Advanced Periodontal Surgery 2020モハメッド アラーNo ratings yet
- Periodontal-Restorative Interactions: A Review: DentistryDocument7 pagesPeriodontal-Restorative Interactions: A Review: DentistrySahana RangarajanNo ratings yet
- Apical Seal Versus Coronal SealDocument8 pagesApical Seal Versus Coronal SealSalem RawashdahNo ratings yet
- Implants in Esthetic ZoneDocument10 pagesImplants in Esthetic ZoneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ContentServer Asp-84 PDFDocument16 pagesContentServer Asp-84 PDFmutiaNo ratings yet
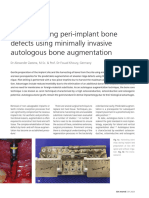
- The Bone Core Technique Reconstructing Peri Implant Bone Defects Using Minimally Invasive Autologous Bone AugmentationDocument6 pagesThe Bone Core Technique Reconstructing Peri Implant Bone Defects Using Minimally Invasive Autologous Bone AugmentationNamratha UmeshNo ratings yet
- 3 PROXIMAL BOX ELEVATIONAND BIOLOGICAL WIDTH CLINICAL R2 TECHNIQUE Frese2013 PDFDocument10 pages3 PROXIMAL BOX ELEVATIONAND BIOLOGICAL WIDTH CLINICAL R2 TECHNIQUE Frese2013 PDFjhon HanselNo ratings yet
- Direct Posterior Composite Restorations. FinalDocument8 pagesDirect Posterior Composite Restorations. FinalJana AliNo ratings yet
- Ultimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationDocument15 pagesUltimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationEvelina HaddadienNo ratings yet
- PRD 22 5 Magne1Document10 pagesPRD 22 5 Magne1sofa83No ratings yet
- Dental Color Matching Instruments and SystemsDocument16 pagesDental Color Matching Instruments and SystemsHandoko DijeNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Digital Smile Design For Computer Assisted Esthetic RehabilitationDocument10 pagesDigital Smile Design For Computer Assisted Esthetic RehabilitationRoberto PucNo ratings yet
- Decoupling With Time - Inside Dentistry - August 2021 - Inside Dentistry - CDEWoDocument7 pagesDecoupling With Time - Inside Dentistry - August 2021 - Inside Dentistry - CDEWoBreno VictorNo ratings yet
- Monoblocks in Root CanalsDocument57 pagesMonoblocks in Root CanalsManva Monish100% (1)
- Remineralization Across The Resin-Dentin Interface: in Vivo Evaiuation Witli Nanoindentation Measurements, EDS, and SEMDocument11 pagesRemineralization Across The Resin-Dentin Interface: in Vivo Evaiuation Witli Nanoindentation Measurements, EDS, and SEMBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- Does Incomplete Caries Removal Reduce Strength of Restored Teeth?Document8 pagesDoes Incomplete Caries Removal Reduce Strength of Restored Teeth?BAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author ManuscriptBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- Dr. Charles H. Tweed: .Jpo/InterviewsDocument9 pagesDr. Charles H. Tweed: .Jpo/InterviewsBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- Charles Tweed: .Jpo/InterviewsDocument9 pagesCharles Tweed: .Jpo/InterviewsBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- Charles H. Tweed, 1895-1970: Pillars in OrthodonticsDocument9 pagesCharles H. Tweed, 1895-1970: Pillars in OrthodonticsBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- ClinicalDocument197 pagesClinicalAlondra BocanegraNo ratings yet
- Pulp Therapy For The Young Permanent Dentition: ApexogenesisDocument15 pagesPulp Therapy For The Young Permanent Dentition: Apexogenesisapi-3855312No ratings yet
- Rekapitulasi Hasil Pelayanan Di BP Gigi Puskesmas Padang Lua TAHUN 2017Document6 pagesRekapitulasi Hasil Pelayanan Di BP Gigi Puskesmas Padang Lua TAHUN 2017taufik hidayatNo ratings yet
- Pediatrics VIVA RevisionDocument9 pagesPediatrics VIVA RevisionJenny WangNo ratings yet
- Endodontic NotesDocument44 pagesEndodontic Noteshunarsandhu100% (1)
- GoldenDocument308 pagesGoldenammarkochiNo ratings yet
- Phoenix AbscessDocument3 pagesPhoenix AbscessOke Soe MoeNo ratings yet
- 2 Treatment of Pulpitis With Biological, Vital Amputational and Extirpation Methods-1Document107 pages2 Treatment of Pulpitis With Biological, Vital Amputational and Extirpation Methods-1Bikku Negi100% (1)
- CH 04Document80 pagesCH 04flock_duxNo ratings yet
- 2023 K2 DenDocument33 pages2023 K2 DenMouhy HalouacheNo ratings yet
- Oral Surgery, Oral Diagnosis and Roentgenology: Cluster VDocument9 pagesOral Surgery, Oral Diagnosis and Roentgenology: Cluster VtsukiyaNo ratings yet
- Chronic Hyperplastic PulpitisDocument30 pagesChronic Hyperplastic PulpitisGlory Pohan67% (3)
- Seminar 1 PulpDocument128 pagesSeminar 1 PulpDarshil100% (2)
- Vitality TestDocument13 pagesVitality TestSwathyNo ratings yet
- Managing Dental EmergenciesDocument46 pagesManaging Dental EmergenciesBoris AbayevNo ratings yet
- Effects of Glass Ionomer Temporary Restorations On Pulpal Diagnosis and TreatmentDocument7 pagesEffects of Glass Ionomer Temporary Restorations On Pulpal Diagnosis and TreatmentKamila BencosmeNo ratings yet
- Classification of Pulpal DiseasesDocument11 pagesClassification of Pulpal DiseasesHassan TantawyNo ratings yet
- 04 Momoi 2012 Clinical Guidelines For Treating Caries in Adults JouDen40 - 95Document31 pages04 Momoi 2012 Clinical Guidelines For Treating Caries in Adults JouDen40 - 95Cherif100% (1)
- A-. The Intimate Association of A-Delta Fibers With The Odontoblastic Cell Layer and DentinDocument12 pagesA-. The Intimate Association of A-Delta Fibers With The Odontoblastic Cell Layer and DentinKaram SarhanNo ratings yet
- Endo - Perio Lesions A Diagnostic DilemmaDocument4 pagesEndo - Perio Lesions A Diagnostic DilemmaPinky TolaniNo ratings yet
- Bds Third Year Test - Docx 2013Document6 pagesBds Third Year Test - Docx 2013Samina TarikNo ratings yet
- Biodentine PulpotomyDocument3 pagesBiodentine PulpotomyDANIELA TOLOZANo ratings yet
- Non Vital Pulp TherapyDocument23 pagesNon Vital Pulp TherapyAmit GaurNo ratings yet
- Grammar in Use: Dentistry. Lecture PART 4Document19 pagesGrammar in Use: Dentistry. Lecture PART 4Ariadne CordeletteNo ratings yet