Download as docx, pdf, or txt
You might also like
- On Balanced DietDocument55 pagesOn Balanced Dietshitalsawant100% (2)
- MalnutritionDocument26 pagesMalnutritionudaybujji100% (1)
- Lecture 10 Protein Energy Malnutrition (PEM)Document26 pagesLecture 10 Protein Energy Malnutrition (PEM)jaish8904100% (1)
- Growth and DevelopmentDocument64 pagesGrowth and DevelopmentRahul Dhaker100% (2)
- Nutritional AssessmentDocument16 pagesNutritional AssessmentGelo Libelo100% (1)
- 0347burst AbdomenDocument24 pages0347burst AbdomenSathishKumar100% (1)
- Nutrition ProblemsDocument11 pagesNutrition Problemsvikas tak100% (2)
- Nutritional Problems: Presenter Priyanka Gehlot M. Sc. (Prev.)Document38 pagesNutritional Problems: Presenter Priyanka Gehlot M. Sc. (Prev.)vikas takNo ratings yet
- Disease PEMDocument16 pagesDisease PEMMeena KoushalNo ratings yet
- Recommended Dietary AllowanceDocument24 pagesRecommended Dietary Allowanceuttkarsh100% (4)
- Protein Energy MalnutritionDocument38 pagesProtein Energy Malnutritionjeshema100% (2)
- WEANINGDocument9 pagesWEANINGSREEDEVI T SURESHNo ratings yet
- Prolactin Reflex (Milk Secretion Reflex)Document16 pagesProlactin Reflex (Milk Secretion Reflex)Juhi Johnson JadhavNo ratings yet
- MalnutritionDocument27 pagesMalnutritionRIYA MARIYATNo ratings yet
- Nutritional ProgrammesDocument15 pagesNutritional ProgrammesRaman SamraoNo ratings yet
- Nutritional Requirements in ChildrenDocument30 pagesNutritional Requirements in ChildrenArchana100% (2)
- By, Dr. Swapna, PG Final Year, Community MedicineDocument67 pagesBy, Dr. Swapna, PG Final Year, Community Medicinesreedhar muthyalaNo ratings yet
- Diet & Disease PPT 2021 - Final EditedDocument156 pagesDiet & Disease PPT 2021 - Final Editedbonsa JalataNo ratings yet
- Nutritional Needs of AdolescentsDocument9 pagesNutritional Needs of AdolescentsLstr B PrltaNo ratings yet
- Nutrition Nursing: ProteinsDocument38 pagesNutrition Nursing: ProteinsAngelyka Nicole Bengco David100% (1)
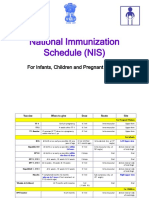
- National Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenDocument13 pagesNational Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenPrabir Kumar Chatterjee100% (1)
- Nutrients and Nutrional Requirements For ChildrenDocument11 pagesNutrients and Nutrional Requirements For ChildrenSANANo ratings yet
- Midday Meal SchemeDocument16 pagesMidday Meal Schemeaswathy100% (1)
- Embryo Development (Embryogenesis)Document31 pagesEmbryo Development (Embryogenesis)SHEMAR STEWARTNo ratings yet
- Breast FeedingDocument43 pagesBreast FeedingsindhujojoNo ratings yet
- Mid Day Meal ProgramDocument20 pagesMid Day Meal Programayushi rainaNo ratings yet
- Food and Nutrition Requirements For School Going Children-Selection PBDocument27 pagesFood and Nutrition Requirements For School Going Children-Selection PBSELVI ANo ratings yet
- Assisting in Insertion of Intrauterine Contraceptive Device (Copper-T)Document4 pagesAssisting in Insertion of Intrauterine Contraceptive Device (Copper-T)manju100% (1)
- Nursing Foundation Harinderjeet GoyalDocument31 pagesNursing Foundation Harinderjeet Goyalmanrajghumman5550% (1)
- IGNOU Block 2 Unit 4 Nutritional Deficiency DisordersDocument22 pagesIGNOU Block 2 Unit 4 Nutritional Deficiency Disorderserice.research100% (3)
- Rama College of Nursing: Health Education OnDocument24 pagesRama College of Nursing: Health Education OnBrijesh Yadav100% (1)
- Nutritional Needs/ B.Sc. Nursing/ Fundamental of Nursing/ Nutrition/ Sameeksha PatialDocument138 pagesNutritional Needs/ B.Sc. Nursing/ Fundamental of Nursing/ Nutrition/ Sameeksha PatialSameekshaNo ratings yet
- Seminar ON Artificial Feeding: Satya Nursing College RohtakDocument8 pagesSeminar ON Artificial Feeding: Satya Nursing College RohtakVikas NehraNo ratings yet
- Introduction To Pediatric NursingDocument36 pagesIntroduction To Pediatric Nursingcharan poonia100% (2)
- Lesson Plan On Unit III Balanced DietDocument20 pagesLesson Plan On Unit III Balanced DietMs.Prachi ChaudhariNo ratings yet
- PemDocument37 pagesPemJOSLINNo ratings yet
- Universal Immunization ProgrammeDocument3 pagesUniversal Immunization ProgrammeAmy Lalringhluani ChhakchhuakNo ratings yet
- Unit 7 - Food-Born Diseases (Poisoning)Document28 pagesUnit 7 - Food-Born Diseases (Poisoning)Abdulmajid Abdella100% (1)
- JG College of Nursing, AhmedabadDocument13 pagesJG College of Nursing, AhmedabadVinayak Srivastava100% (1)
- Weaning FoodsDocument9 pagesWeaning FoodsraisNo ratings yet
- 5.1. Nutritional Requirements in ChildrenDocument63 pages5.1. Nutritional Requirements in ChildrenArchanaNo ratings yet
- 3 1 Rol of Regulatory BodiesDocument29 pages3 1 Rol of Regulatory BodiesBisakha Dey0% (1)
- KMCDocument13 pagesKMCJOSLINNo ratings yet
- Introduction About SelfDocument27 pagesIntroduction About SelfsimonjosanNo ratings yet
- Preventive Pediatric Seminar 2Document82 pagesPreventive Pediatric Seminar 2Yashoda Satpute100% (1)
- 1 Applied Nutrition and Dietetics - 020222Document6 pages1 Applied Nutrition and Dietetics - 020222Akshata Bansode50% (2)
- Ors Solution: Object: TheoryDocument2 pagesOrs Solution: Object: TheoryFaiz Ur RehmanNo ratings yet
- Artificalfeedingprocedure 180425131100Document11 pagesArtificalfeedingprocedure 180425131100Manisa ParidaNo ratings yet
- Extended and Expanded Role of NursesDocument20 pagesExtended and Expanded Role of NursesSandeep choudharyNo ratings yet
- Baby Friendly Hospital InitiativeDocument2 pagesBaby Friendly Hospital InitiativeChandu Raj100% (2)
- Introduction To Nutrition Unit IDocument118 pagesIntroduction To Nutrition Unit IAnuchithra RadhakrishnanNo ratings yet
- IGNOU Block 2 Unit 2 Nutrition During Pregnancy & LactationDocument25 pagesIGNOU Block 2 Unit 2 Nutrition During Pregnancy & Lactationerice.researchNo ratings yet
- BreastfeedingDocument36 pagesBreastfeedingArchana100% (1)
- Pharmacology, Pathology, Genetics: QP Code: BNN203Document1 pagePharmacology, Pathology, Genetics: QP Code: BNN203Mamta KumariNo ratings yet
- c14 p51 Nutritional Programmes in IndiaDocument13 pagesc14 p51 Nutritional Programmes in IndiaSrinivas Kasi0% (1)
- Effects of Maternal Drugs On The FetusDocument9 pagesEffects of Maternal Drugs On The FetusJennifer DixonNo ratings yet
- Pre & Post Operative Care of ChildrensDocument22 pagesPre & Post Operative Care of Childrenscharan poonia100% (2)
- Vit ADocument9 pagesVit AmalathiNo ratings yet
- Subjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionDocument26 pagesSubjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionHemant SharmaNo ratings yet
- 1 NCM 116Document378 pages1 NCM 116Alkiana SalardaNo ratings yet
- NCM 116Document78 pagesNCM 1166pk4c7kw4kNo ratings yet
- CATARACTDocument9 pagesCATARACTHemant SharmaNo ratings yet
- By Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainDocument8 pagesBy Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainHemant SharmaNo ratings yet
- GASTRITISDocument11 pagesGASTRITISHemant SharmaNo ratings yet
- Charbohydrate: Unit - IiDocument8 pagesCharbohydrate: Unit - IiHemant SharmaNo ratings yet
- Subjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionDocument26 pagesSubjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionHemant SharmaNo ratings yet
- Why People Use Herbal Medicine: Insights From A Focus-Group Study in GermanyDocument9 pagesWhy People Use Herbal Medicine: Insights From A Focus-Group Study in GermanyMichael LopezNo ratings yet
- Drug Study - Carvedilol: Vijandre, Sheryl G. BSN Iii-IDocument2 pagesDrug Study - Carvedilol: Vijandre, Sheryl G. BSN Iii-IJan Emmanuel DC SerranoNo ratings yet
- Role of Hijama Cupping Therapy in The Management of Niqras Goutyarthritis 2167 7921 1000256Document8 pagesRole of Hijama Cupping Therapy in The Management of Niqras Goutyarthritis 2167 7921 1000256Rafa CalamiNo ratings yet
- History TakingDocument28 pagesHistory TakingguldonNo ratings yet
- Diseases of Hard Tissues of Teeth PDFDocument152 pagesDiseases of Hard Tissues of Teeth PDFAPARNA AARATHI SREEKUMARNo ratings yet
- Medicinal Uses For Herbal Teas: Evidence, Dosing, and Preparation MethodsDocument7 pagesMedicinal Uses For Herbal Teas: Evidence, Dosing, and Preparation MethodsJose Ph YuNo ratings yet
- Ophthalmic Manifestation of Systimic DiseaseDocument45 pagesOphthalmic Manifestation of Systimic DiseaseSarahNo ratings yet
- Q - A Random 14Document6 pagesQ - A Random 14Yuuki Chitose (tai-kun)No ratings yet
- Approach To Short Stature: Guest Editor: Bhim S. PandhiDocument9 pagesApproach To Short Stature: Guest Editor: Bhim S. PandhiAldy WaveNo ratings yet
- Trimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleDocument1 pageTrimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleRenmico Aquino0% (1)
- Facial Nerve ParalysisDocument73 pagesFacial Nerve ParalysisAys Ghaysa100% (2)
- Pathogenesis of PcosDocument14 pagesPathogenesis of PcosMitali Narurkar100% (1)
- What Causes Food Spoilage?: Melissa H. Pecundo IAS-BiologyDocument12 pagesWhat Causes Food Spoilage?: Melissa H. Pecundo IAS-BiologyAbie Jewel Joy RoqueNo ratings yet
- Different Types StressDocument2 pagesDifferent Types StressSmail BenidirNo ratings yet
- Lec10 CV PathologyDocument75 pagesLec10 CV PathologymanuelNo ratings yet
- OsteoarthritisDocument29 pagesOsteoarthritisniekoNo ratings yet
- Annotated Bibliography FinalDocument13 pagesAnnotated Bibliography Finalapi-252551056No ratings yet
- Violencia y Comportamiento Agresivo Ped in ReviewDocument14 pagesViolencia y Comportamiento Agresivo Ped in ReviewFederico AlzugarayNo ratings yet
- 129 SAQsDocument13 pages129 SAQsSuryanarayana Murthy Kaivaram100% (3)
- Modul Perdarahan Saluran CernaDocument21 pagesModul Perdarahan Saluran CernaErica SkinnerNo ratings yet
- Rheumatological Disorders in PregnancyDocument61 pagesRheumatological Disorders in Pregnancydrsyan hamzahNo ratings yet
- Angiotensin Converting Enzyme Inhibitors: Properties and Side EffectsDocument6 pagesAngiotensin Converting Enzyme Inhibitors: Properties and Side EffectselvishmicroNo ratings yet
- Soal Un Bhs Inggris Tipe BDocument8 pagesSoal Un Bhs Inggris Tipe BgirinitaNo ratings yet
- 3rd Q Prelim Gr.8Document2 pages3rd Q Prelim Gr.8Arianne B. CabañezNo ratings yet
- Obesity in PregnancyDocument9 pagesObesity in PregnancydarkkryNo ratings yet
- GDS K-6 - Newborn Physical ExaminationDocument44 pagesGDS K-6 - Newborn Physical ExaminationJosephine IrenaNo ratings yet
- How To Know That Your Digestion System Is Working +Document30 pagesHow To Know That Your Digestion System Is Working +Sahal ShaikhNo ratings yet
- Anatomy PDFDocument32 pagesAnatomy PDFSoroush100% (1)
- South African Medicinal Plants ManualDocument33 pagesSouth African Medicinal Plants ManualSello SelowaNo ratings yet