Download as pdf or txt
You might also like
- Berges Level 2 Book PDFDocument80 pagesBerges Level 2 Book PDFYulia Larin100% (1)
- Case 29 SolutionDocument7 pagesCase 29 Solutiongators333100% (6)
- Annex C Data Capture Form For Use of CHDs (Municipalities and CCS)Document13 pagesAnnex C Data Capture Form For Use of CHDs (Municipalities and CCS)JRNo ratings yet
- Recent Philippine Budget Reforms: Separating The Chaff From The Grain, The Whimsical From The RealDocument24 pagesRecent Philippine Budget Reforms: Separating The Chaff From The Grain, The Whimsical From The RealJez JanNo ratings yet
- Ao2017 0012Document49 pagesAo2017 0012disasternursinNo ratings yet
- Mukerji Committee Report 1966Document47 pagesMukerji Committee Report 1966lalit823187100% (1)
- Slaying The DragonDocument5 pagesSlaying The DragonMarkus ChNo ratings yet
- Revisiting The Jalong Ambush Site (Hussars)Document41 pagesRevisiting The Jalong Ambush Site (Hussars)stmcipohNo ratings yet
- Mission Statement of BataDocument5 pagesMission Statement of BataArbab Usman Khan0% (1)
- AO 2022 0051 Revised National Policy On Infection Prevention and Control in All Public and Private Health FacilitiesDocument19 pagesAO 2022 0051 Revised National Policy On Infection Prevention and Control in All Public and Private Health FacilitiesBrian VargasNo ratings yet
- dm2021 0327 Surge Response Plan For HFDocument11 pagesdm2021 0327 Surge Response Plan For HFMonica Lowinski100% (1)
- Tanzania Health Sector Strategic Plan V 17 06 2021 Final SignedDocument104 pagesTanzania Health Sector Strategic Plan V 17 06 2021 Final SignedDr mathew MushiNo ratings yet
- Healthcare - Proposal For DG ProjectDocument5 pagesHealthcare - Proposal For DG Projectpawan patelNo ratings yet
- Ao2019 0060Document19 pagesAo2019 0060Charlemagne Sabio GalamgamNo ratings yet
- Concept Note of The Primary Health Care QOC ActivityDocument21 pagesConcept Note of The Primary Health Care QOC ActivityTewodros Worku LiyewNo ratings yet
- Nabh - HicDocument10 pagesNabh - HicArathy A HNo ratings yet
- Assessment of Knowledge, Attitude, and Practice of Telemedicine in IndiaDocument8 pagesAssessment of Knowledge, Attitude, and Practice of Telemedicine in IndiaIJRASETPublicationsNo ratings yet
- DOH AO No - 2020 0022Document17 pagesDOH AO No - 2020 0022MariaChristinaVaronaTemplanzaNo ratings yet
- Policy Analysis Health SectorDocument8 pagesPolicy Analysis Health Sectorerika ocuamanNo ratings yet
- 2021 Budget BrieferDocument24 pages2021 Budget Brieferyg loveNo ratings yet
- FAQs - Local Health Systems Management ToolsDocument2 pagesFAQs - Local Health Systems Management ToolsPhilippe Ceasar C. BascoNo ratings yet
- Private Enterprise For Public Health - Guide 2012Document44 pagesPrivate Enterprise For Public Health - Guide 2012ippfwhrresmobNo ratings yet
- 16 - 41196 - M Alfan Hassan Kamal - LeadershipDocument2 pages16 - 41196 - M Alfan Hassan Kamal - LeadershipDoni SaragihNo ratings yet
- Human Resource Management. An Example in Public SectorDocument12 pagesHuman Resource Management. An Example in Public Sectorcrazy bombNo ratings yet
- 2-Module 2 - Identification - 20181114 WFP Comments - UNICEF v2Document74 pages2-Module 2 - Identification - 20181114 WFP Comments - UNICEF v2MJ ArcillaNo ratings yet
- Ethiopia Health Sector Transformation ProcessDocument184 pagesEthiopia Health Sector Transformation ProcessAbebe TilahunNo ratings yet
- Healthcare in Saudi Arabia PDFDocument16 pagesHealthcare in Saudi Arabia PDFmoh0001No ratings yet
- 1.AMSP StrategiesDocument57 pages1.AMSP StrategiesVeera RaghavanNo ratings yet
- Medical Records Lec 5Document23 pagesMedical Records Lec 5Davis PunjilaNo ratings yet
- MCM Who Academy Guide FinalDocument88 pagesMCM Who Academy Guide FinalHilal Mohamed NorNo ratings yet
- Hospital Scorecard - DepartmentwiseDocument4 pagesHospital Scorecard - DepartmentwiseNatasha BhasinNo ratings yet
- Dead Bodies PDFDocument24 pagesDead Bodies PDFRj Concepcion RrtNo ratings yet
- Doh Mtra PDFDocument8 pagesDoh Mtra PDFElaine DabuNo ratings yet
- Guidelines For Maternal Death Surveillance & ResponseDocument148 pagesGuidelines For Maternal Death Surveillance & ResponseManish Chandra Prabhakar100% (3)
- CHAPTER 6 Epidemiological SurveillanceDocument50 pagesCHAPTER 6 Epidemiological Surveillanceteklay100% (1)
- Ao 2011-0009Document21 pagesAo 2011-0009Joline UrbinaNo ratings yet
- Unit 1Document65 pagesUnit 1shrutiNo ratings yet
- Notification For NABH-Accreditation Program - HCO 5th Edition Guidebook - 30-May-2022Document41 pagesNotification For NABH-Accreditation Program - HCO 5th Edition Guidebook - 30-May-2022Neeraj JoshiNo ratings yet
- Philippines Sta. Ana Hospital HCWM PlanDocument57 pagesPhilippines Sta. Ana Hospital HCWM PlanKimberly BandongNo ratings yet
- EAU Guidelines 2021 FullDocument1,852 pagesEAU Guidelines 2021 FullNugraha GunamantaNo ratings yet
- Comparative Matrix ECQ Vs MECQDocument9 pagesComparative Matrix ECQ Vs MECQTheSummitExpressNo ratings yet
- Implementation Strategies For Health Systems in Low-AcountriesDocument135 pagesImplementation Strategies For Health Systems in Low-AcountriesAlbert Lawrence Kwansa0% (1)
- Research Proposal For Assessing Patient Safety Culture in PublicDocument57 pagesResearch Proposal For Assessing Patient Safety Culture in PublicNikita SinghNo ratings yet
- Draft EO Amending EO No 138 As 4 October 2022 5PMDocument12 pagesDraft EO Amending EO No 138 As 4 October 2022 5PMJeffsonNo ratings yet
- E.2 AO 2020-0037 Implementation of The Local Health Systems Maturity LevelsDocument17 pagesE.2 AO 2020-0037 Implementation of The Local Health Systems Maturity LevelsWinson JayNo ratings yet
- Critical Review of The TransCelerate Template ForDocument10 pagesCritical Review of The TransCelerate Template Forbdvd1007092No ratings yet
- Ipls PDFDocument119 pagesIpls PDFTekle TibebuNo ratings yet
- Olabisi Onabanjo University, Ago - Iwoye, Nigeria.: Format B CDocument9 pagesOlabisi Onabanjo University, Ago - Iwoye, Nigeria.: Format B Cpraisejah moyoNo ratings yet
- Health Care Management in India: Some Issues and Challenges: Mohd Iqbal Khan Amit BanerjiDocument16 pagesHealth Care Management in India: Some Issues and Challenges: Mohd Iqbal Khan Amit BanerjiAnjali sasiNo ratings yet
- Unit 3 Multidisciplinary Team WorkingDocument8 pagesUnit 3 Multidisciplinary Team WorkingMalack ChagwaNo ratings yet
- The Italian Healthcare SystemDocument5 pagesThe Italian Healthcare SystemAnnamaria FrezzaNo ratings yet
- Red Cross, Red Crescent Magazine. No. 1, 2011Document32 pagesRed Cross, Red Crescent Magazine. No. 1, 2011International Committee of the Red Cross100% (1)
- Mercy Corps Report Balochistan PDFDocument388 pagesMercy Corps Report Balochistan PDFwaqas724No ratings yet
- Arba Minch Univerity College of Medicine and Health Sciences Department of Public HealthDocument56 pagesArba Minch Univerity College of Medicine and Health Sciences Department of Public HealthDibora AlemayehuNo ratings yet
- Cavite Readiness Assessment Tools - HC-RHU-BHS - MR SIA 2023Document10 pagesCavite Readiness Assessment Tools - HC-RHU-BHS - MR SIA 2023Christean Val Bayani ValezaNo ratings yet
- Environmental Impact Assessment FOR Development OF BUS Rapid Transit System IN Naya Raipur ChhattisgarhDocument128 pagesEnvironmental Impact Assessment FOR Development OF BUS Rapid Transit System IN Naya Raipur ChhattisgarhAniket BhoskarNo ratings yet
- Tackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettDocument15 pagesTackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettLesley Russell100% (1)
- National Quality Assurance Standars (2018)Document72 pagesNational Quality Assurance Standars (2018)Santhosh KumarNo ratings yet
- At A Glance: The Philippine Health Care System: MedicinesDocument15 pagesAt A Glance: The Philippine Health Care System: MedicinesEdrea Aquino MendezNo ratings yet
- PD 1519-Revised Philippine Medical Care Act Etc..Document15 pagesPD 1519-Revised Philippine Medical Care Act Etc..Rosa GamaroNo ratings yet
- Animal Bite GuildlinesDocument7 pagesAnimal Bite GuildlinesHari Pawan Kishore GarimellaNo ratings yet
- Global DemographyDocument23 pagesGlobal DemographyJhon Albert RobledoNo ratings yet
- Complete Manual MOP - 20150323Document250 pagesComplete Manual MOP - 20150323Angkol TuyorNo ratings yet
- Ao2021-0042 Guidelines On Covid Surge Response of Health FacilitiesDocument13 pagesAo2021-0042 Guidelines On Covid Surge Response of Health FacilitiesMic BNo ratings yet
- dm2020 0123Document47 pagesdm2020 0123Franchise AlienNo ratings yet
- ESR InfographicsDocument1 pageESR InfographicsJoseph RepotenteNo ratings yet
- Nutrition: SectorDocument18 pagesNutrition: SectorJoseph RepotenteNo ratings yet
- SSC and IPSG SignagesDocument2 pagesSSC and IPSG SignagesJoseph RepotenteNo ratings yet
- Office of The SecretaryDocument18 pagesOffice of The SecretaryJoseph RepotenteNo ratings yet
- Office: of The SecretaryDocument16 pagesOffice: of The SecretaryJoseph RepotenteNo ratings yet
- Quality Management System of Dr. Jose N. Rodriguez Memorial Hospital and SanitariumDocument25 pagesQuality Management System of Dr. Jose N. Rodriguez Memorial Hospital and SanitariumJoseph Repotente100% (1)
- Other: RegionDocument4 pagesOther: RegionJoseph RepotenteNo ratings yet
- Office: of The SecretaryDocument4 pagesOffice: of The SecretaryJoseph RepotenteNo ratings yet
- PDCA PrinciplesDocument10 pagesPDCA PrinciplesJoseph RepotenteNo ratings yet
- Request For Document Creation/ Revision/ Deletion Logsheet: Quality Management System OfficeDocument1 pageRequest For Document Creation/ Revision/ Deletion Logsheet: Quality Management System OfficeJoseph RepotenteNo ratings yet
- 9-23-2020-Motion To Post Bail - Voltaire Gebulaguin - Atty. Blancia - Docx (Edited)Document7 pages9-23-2020-Motion To Post Bail - Voltaire Gebulaguin - Atty. Blancia - Docx (Edited)Andrei BlanciaNo ratings yet
- Unit 7 Exercises To StsDocument7 pagesUnit 7 Exercises To StsHưng TrầnNo ratings yet
- Lecture 03 - ECO 209 - W2013 PDFDocument69 pagesLecture 03 - ECO 209 - W2013 PDF123No ratings yet
- Employee Relationship ManagementDocument42 pagesEmployee Relationship Managementsupriyanair80% (5)
- Islam A Case of Mistaken Identity.Document29 pagesIslam A Case of Mistaken Identity.AndrewNo ratings yet
- Dredging and Flood RiskDocument2 pagesDredging and Flood RiskJustin SharpeNo ratings yet
- ForkliftGSF231 1Document1 pageForkliftGSF231 1AbdulHanifNo ratings yet
- Current Trends Issues and Problems in Education SystemDocument49 pagesCurrent Trends Issues and Problems in Education SystemfuellasjericNo ratings yet
- BIR Form 1604EDocument2 pagesBIR Form 1604Ecld_tiger100% (2)
- Job Application Process ModuleDocument8 pagesJob Application Process ModuleacelcastrenceNo ratings yet
- Aircraft LeasingDocument50 pagesAircraft LeasingBenchmarking84100% (2)
- The CPP/NPA/NDF Constitute The Local Communist Movement in The Philippines Beforehand, ItDocument19 pagesThe CPP/NPA/NDF Constitute The Local Communist Movement in The Philippines Beforehand, Itzy_tanNo ratings yet
- Reality TV Shows Effect On PeopleDocument5 pagesReality TV Shows Effect On PeopleNefeli FefeNo ratings yet
- Mobilia Products, Inc. v. Umezawa, 452 SCRA 736Document15 pagesMobilia Products, Inc. v. Umezawa, 452 SCRA 736JNo ratings yet
- Indifference Curve AnalysisDocument91 pagesIndifference Curve AnalysisShweta SinghNo ratings yet
- Week 9 Jose Rizal's Second Travel AbroadDocument6 pagesWeek 9 Jose Rizal's Second Travel AbroadShervee PabalateNo ratings yet
- Laundry and Bourbon AnalysisDocument2 pagesLaundry and Bourbon AnalysisAveryNo ratings yet
- Maimonides 0739 Ebk v6Document525 pagesMaimonides 0739 Ebk v6futurity34No ratings yet
- Nnadili v. Chevron U.s.a., Inc.Document10 pagesNnadili v. Chevron U.s.a., Inc.RavenFoxNo ratings yet
- Psychiatric Nursing NotesDocument13 pagesPsychiatric Nursing NotesCarlo VigoNo ratings yet
- Assignment/ Tugasan - Principles of ManagementDocument11 pagesAssignment/ Tugasan - Principles of ManagementSuriya KumaraNo ratings yet
- Cat Menes - Google SearchDocument1 pageCat Menes - Google SearchShanzeh ZehraNo ratings yet
- Ers. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewDocument10 pagesErs. Co M: JANA Master Fund, Ltd. Performance Update - December 2010 Fourth Quarter and Year in ReviewVolcaneum100% (2)
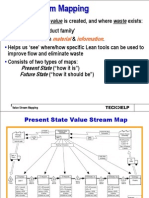
- 4 Slides Value Stream MappingDocument13 pages4 Slides Value Stream MappingRanjan Raj Urs100% (2)