Download as docx, pdf, or txt
You might also like
- Secret Magic Spells of The Romany GypsiesDocument28 pagesSecret Magic Spells of The Romany Gypsiesakenaton4089% (66)
- Nursing Care Plan Dysfunctional Uterine Bleeding (DUB)Document2 pagesNursing Care Plan Dysfunctional Uterine Bleeding (DUB)deric90% (10)
- NCP Anxiety Related To Unconscious Conflict About Essential Goals and Values of Life Into Financial Instability Causing DistressDocument2 pagesNCP Anxiety Related To Unconscious Conflict About Essential Goals and Values of Life Into Financial Instability Causing DistressMa. Elaine Carla Tating33% (3)
- The Case of The Missing TimeDocument14 pagesThe Case of The Missing TimeSharingan MangekyouNo ratings yet
- NCP Dysfunctional Uterine BleedingDocument2 pagesNCP Dysfunctional Uterine BleedingDayan CabrigaNo ratings yet
- Santos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument1 pageSantos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveIvan SantosNo ratings yet
- Fear Related To Threat of DystociaDocument2 pagesFear Related To Threat of DystociaMark FernandezNo ratings yet
- Cancer Care NCPDocument2 pagesCancer Care NCPMaverick LimNo ratings yet
- NCP Fear PDF Relaxation (Psychology) Positive Psychology 2Document1 pageNCP Fear PDF Relaxation (Psychology) Positive Psychology 2BERSAMERA JOVEN 1CNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Objectives Interventions Rationale Evaluation Subjective CuesDocument2 pagesNursing Care Plan: Cues Nursing Diagnosis Objectives Interventions Rationale Evaluation Subjective CuesAkira A. AtomarNo ratings yet
- Abnormal Uterine Bleeding - Fear NCPDocument2 pagesAbnormal Uterine Bleeding - Fear NCPJasmine100% (1)
- CP NCPDocument4 pagesCP NCPalamillodemarkbsn3No ratings yet
- Panic Attack Nursing Care PlanDocument4 pagesPanic Attack Nursing Care PlanSamVelasco100% (2)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationPam RomeroNo ratings yet
- Revised. NCP. Jam 1Document3 pagesRevised. NCP. Jam 1ACOB, Jamil C.No ratings yet
- Cholecystitis NCPDocument5 pagesCholecystitis NCPtsukino143No ratings yet
- NCP FearDocument3 pagesNCP Fearエド パジャロン100% (1)
- Nursing Care Plan For Client With AnxietyDocument2 pagesNursing Care Plan For Client With AnxietyThe Right WayNo ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Situational Low Self-Esteem - NCPDocument3 pagesSituational Low Self-Esteem - NCPLizzey YuNo ratings yet
- NCP-and-Drug-study For MENDocument8 pagesNCP-and-Drug-study For MENVillie SumandeNo ratings yet
- NCP TemplateDocument3 pagesNCP TemplateYvesNo ratings yet
- Ncp-Post OpDocument3 pagesNcp-Post OpFran LanNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanCarl Andre ReyesNo ratings yet
- NCP Colon CancerDocument8 pagesNCP Colon CancerSkyla FiestaNo ratings yet
- NCPDocument1 pageNCPnictan 140% (1)
- Nlah BlahDocument2 pagesNlah BlahACOB, Jamil C.No ratings yet
- NCPDocument1 pageNCPVictor MurilloNo ratings yet
- NCPDocument1 pageNCPVictor MurilloNo ratings yet
- Care Plan On Trigeminal NeuralgiaDocument3 pagesCare Plan On Trigeminal Neuralgiaanimesh pandaNo ratings yet
- NCP For CSDocument2 pagesNCP For CSIris Coronel AdamosNo ratings yet
- NCPDocument3 pagesNCPCharles Mallari Valdez100% (1)
- NCPDocument4 pagesNCPyasayayasay yasayNo ratings yet
- NCP, 3 Case StudyDocument9 pagesNCP, 3 Case StudyKrishelle Kate PannigNo ratings yet
- NCP FearsDocument1 pageNCP FearsFrances MercadoNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMonteroso, Kae Rhenzel A.No ratings yet
- Tuano, Salma M. Bsn4-1 Fear/AnxietyDocument3 pagesTuano, Salma M. Bsn4-1 Fear/AnxietySALMA M. TUANO100% (1)
- Cues/ Evidence Nursing Diagnosis Objectives Interventions Rationale Evaluation Subjective CuesDocument2 pagesCues/ Evidence Nursing Diagnosis Objectives Interventions Rationale Evaluation Subjective CuesFelmerPolancoRodaNo ratings yet
- Ncm112a Allncpforcancers BalangueDocument11 pagesNcm112a Allncpforcancers BalangueNurse NotesNo ratings yet
- Subjective: Long Term Goal: Long Term GoalDocument1 pageSubjective: Long Term Goal: Long Term GoalRAFNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument15 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveWhoo CaresNo ratings yet
- NCP Anxiety DRDocument3 pagesNCP Anxiety DRyuri dominxNo ratings yet
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- Nursing Care PlansDocument8 pagesNursing Care PlansCindy MariscotesNo ratings yet
- NURSING CARE PLAN EndoDocument7 pagesNURSING CARE PLAN EndoFrancise Elyn OcubilloNo ratings yet
- NCP AnxietyDocument3 pagesNCP AnxietyPaolo EspinosaNo ratings yet
- NCP 66Document1 pageNCP 66Dheng EsquijoNo ratings yet
- Anxiety R:T Death ThreatDocument8 pagesAnxiety R:T Death ThreatAlfredo BaulaNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Fluoroscopy NCPDocument1 pageFluoroscopy NCPFillanie Dominique LetadaNo ratings yet
- Defining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions RationaleDocument3 pagesDefining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions Rationalesbo100% (1)
- Anxiety NCPDocument2 pagesAnxiety NCPAnaleah MalayaoNo ratings yet
- ANXIETYDocument2 pagesANXIETYChombe JcNo ratings yet
- Nursing Care Plan 1Document3 pagesNursing Care Plan 1Kuro HanabusaNo ratings yet
- NCP Anxiety 1Document3 pagesNCP Anxiety 1goodemonz15No ratings yet
- Lucie Fink NCPsss - BUAYA PIA N32Document7 pagesLucie Fink NCPsss - BUAYA PIA N32Pia Mae BuayaNo ratings yet
- NCP of Endometrical CancerDocument2 pagesNCP of Endometrical CancerFrando kennethNo ratings yet
- Cues Nursing Diagnosis Outcome Nursingintervention Rationale Evaluation Discharge PlanningDocument5 pagesCues Nursing Diagnosis Outcome Nursingintervention Rationale Evaluation Discharge PlanningBSN 3B-Bulatao,Goergie Ann L. CPUSNNo ratings yet
- CCN NCPDocument5 pagesCCN NCPFRAULINE CLAIRE ELEURIN. GAGARACRUZNo ratings yet
- Workbook & Summary - The Gift Of Fear - Based On The Book By Gavin De BeckerFrom EverandWorkbook & Summary - The Gift Of Fear - Based On The Book By Gavin De BeckerNo ratings yet
- Overcome Anxiety: Break Free From Fear, Worry, Trauma, and Negative ThinkingFrom EverandOvercome Anxiety: Break Free From Fear, Worry, Trauma, and Negative ThinkingNo ratings yet
- The use of therapeutic relaxation methods: Employed by nurses at the hospital against anxietyFrom EverandThe use of therapeutic relaxation methods: Employed by nurses at the hospital against anxietyNo ratings yet
- Mental Status Examination: Your Own Words and ObservationsDocument8 pagesMental Status Examination: Your Own Words and ObservationsLadybelle GototosNo ratings yet
- Applying Restraints PDFDocument6 pagesApplying Restraints PDFLadybelle GototosNo ratings yet
- Mse Asssessment GototosDocument6 pagesMse Asssessment GototosLadybelle GototosNo ratings yet
- Mse 1Document27 pagesMse 1Ladybelle GototosNo ratings yet
- Week 7 en ModuleDocument27 pagesWeek 7 en ModuleLadybelle GototosNo ratings yet
- Sunday Reflection - GototosDocument1 pageSunday Reflection - GototosLadybelle GototosNo ratings yet
- Journal - Writing #2 - GOTOTOSDocument3 pagesJournal - Writing #2 - GOTOTOSLadybelle GototosNo ratings yet
- Journal Writing #1 GOTOTOSDocument3 pagesJournal Writing #1 GOTOTOSLadybelle GototosNo ratings yet
- Age Drug StudyDocument20 pagesAge Drug StudyLadybelle GototosNo ratings yet
- Drug Study LadyDocument8 pagesDrug Study LadyLadybelle GototosNo ratings yet
- Ladybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPDocument2 pagesLadybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPLadybelle GototosNo ratings yet
- AGE Pedia CaseDocument83 pagesAGE Pedia CaseLadybelle GototosNo ratings yet
- Gordon'S 11 Functional Health Patterns Functional Health Pattern Before Hospitalization During Hospitalization Health Perception-Health ManagementDocument6 pagesGordon'S 11 Functional Health Patterns Functional Health Pattern Before Hospitalization During Hospitalization Health Perception-Health ManagementLadybelle GototosNo ratings yet
- Evaluation Guide For USL Students: E-Form4 S-SLDocument3 pagesEvaluation Guide For USL Students: E-Form4 S-SLLadybelle GototosNo ratings yet
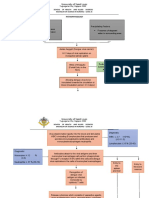
- Pathophysiology: Tuguegarao City, Cagayan 3500Document2 pagesPathophysiology: Tuguegarao City, Cagayan 3500Ladybelle GototosNo ratings yet
- Area Assessed Technique Used Normal Findings Actual Findings RemarksDocument11 pagesArea Assessed Technique Used Normal Findings Actual Findings RemarksLadybelle GototosNo ratings yet
- Pathophysiology: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiDocument4 pagesPathophysiology: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiLadybelle GototosNo ratings yet
- Week 3-4 Lessons: Week 3 - 4 Learning Resources & AssessmentDocument15 pagesWeek 3-4 Lessons: Week 3 - 4 Learning Resources & AssessmentLadybelle GototosNo ratings yet
- Dengue Drug Study and NCPDocument22 pagesDengue Drug Study and NCPLadybelle GototosNo ratings yet
- University of Saint LouisDocument10 pagesUniversity of Saint LouisLadybelle GototosNo ratings yet
- University of Saint Louis Tuguegarao City School of Health and Allied SciencesDocument2 pagesUniversity of Saint Louis Tuguegarao City School of Health and Allied SciencesLadybelle GototosNo ratings yet
- Transcultural Perspectives in Mental Health Nursing: Prepared By: Alfrey J. Corpuz, RN, MSNDocument22 pagesTranscultural Perspectives in Mental Health Nursing: Prepared By: Alfrey J. Corpuz, RN, MSNLadybelle GototosNo ratings yet
- Time Table:: Week 1 and 2 LessonsDocument11 pagesTime Table:: Week 1 and 2 LessonsLadybelle GototosNo ratings yet
- LFD PediaDocument1 pageLFD PediaLadybelle GototosNo ratings yet
- Weeks 5 and 6 Lessons: Weeks 5-6 Learning Resources & AssessmentsDocument5 pagesWeeks 5 and 6 Lessons: Weeks 5-6 Learning Resources & AssessmentsLadybelle GototosNo ratings yet
- Midterm Psych Module 8Document10 pagesMidterm Psych Module 8Ladybelle GototosNo ratings yet
- Souls-That's Culture. Delivering Culturally Competent Care Is The Real Measure."Document2 pagesSouls-That's Culture. Delivering Culturally Competent Care Is The Real Measure."Ladybelle GototosNo ratings yet
- Midterm Psych Module 9Document6 pagesMidterm Psych Module 9Ladybelle GototosNo ratings yet
- Learning Content: Final Term Week 15Document6 pagesLearning Content: Final Term Week 15Ladybelle GototosNo ratings yet
- Prelim Adtech Week4 BDocument5 pagesPrelim Adtech Week4 BLadybelle GototosNo ratings yet
- CRV Led Spec SheetDocument3 pagesCRV Led Spec SheetGabrielGrecoNo ratings yet
- What Is The Endocrine System?Document4 pagesWhat Is The Endocrine System?ROXANNE V. LOPEZNo ratings yet
- MC-WHY DO PEOPLE SNORE - PFC In-Class Language Practice MaterialDocument1 pageMC-WHY DO PEOPLE SNORE - PFC In-Class Language Practice MaterialKutay KılıçtekNo ratings yet
- A High Proportion of Beta-Tocopherol In. 2019Document5 pagesA High Proportion of Beta-Tocopherol In. 2019Miguel Antonio CaicedoNo ratings yet
- WorkShop Supervisor Management NotesDocument10 pagesWorkShop Supervisor Management NotesWeyih ReganNo ratings yet
- ProjectDocument32 pagesProjectFavour NwachukwuNo ratings yet
- Fighter Archetypes & Fighting StylesDocument17 pagesFighter Archetypes & Fighting StylesKristopher GarrettNo ratings yet
- Triber Accessories - BrochureDocument10 pagesTriber Accessories - Brochurecrm testNo ratings yet
- Physics For Scientists and Engineers 9th Edition Serway Test BankDocument23 pagesPhysics For Scientists and Engineers 9th Edition Serway Test Bankninhletitiaqt3100% (33)
- Castrol 0w-30 German CastrolDocument2 pagesCastrol 0w-30 German CastrolTudor RatiuNo ratings yet
- Crit DRDocument5 pagesCrit DRAnonymous 8AVGWWCDfNo ratings yet
- Idioms For IELTS SpeakingDocument21 pagesIdioms For IELTS SpeakingРоза АсановаNo ratings yet
- Cosmology of The SelfDocument39 pagesCosmology of The SelfAgnostikaNo ratings yet
- Test Bank For Entrepreneurship Theory Process and Practice 10th Edition by KuratkoDocument36 pagesTest Bank For Entrepreneurship Theory Process and Practice 10th Edition by Kuratkosanityenhanceqould1100% (54)
- BTCDocument30 pagesBTCshajib_sustNo ratings yet
- Mark Scheme (Results) : January 2017Document21 pagesMark Scheme (Results) : January 2017Mohammad AliNo ratings yet
- Cardomom in Guatemala June 11 2022Document9 pagesCardomom in Guatemala June 11 2022Luis MijaresNo ratings yet
- Tiruvannamalai and RajinikanthDocument2 pagesTiruvannamalai and RajinikanthashokhaNo ratings yet
- Fdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetDocument12 pagesFdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetRDNo ratings yet
- Science FictionDocument26 pagesScience Fictionmilkaddict100% (3)
- 79-Article Text-140-3-10-20170810Document5 pages79-Article Text-140-3-10-20170810Raihanah Fadhillah YulianiNo ratings yet
- 2frm Rexroth Re28389Document16 pages2frm Rexroth Re28389Anurag JainNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument9 pagesSafety Data Sheet: 1. IdentificationVictorNo ratings yet
- Company Analysis Report On M/s Vimal Oil & Foods LTDDocument32 pagesCompany Analysis Report On M/s Vimal Oil & Foods LTDbalaji bysani100% (1)
- SanDiegoZoo GuideMap 1.2016 REFERNCEDocument1 pageSanDiegoZoo GuideMap 1.2016 REFERNCETerry Tmac McElwainNo ratings yet
- Crochet Pattern: Little FrogDocument7 pagesCrochet Pattern: Little Froglina.dmitrenckoNo ratings yet
- Test-Retest Reliability of The Speech-Evoked Auditory Brainstem ResponseDocument10 pagesTest-Retest Reliability of The Speech-Evoked Auditory Brainstem ResponseCabinet VeterinarNo ratings yet
- Cu ZN 10Document2 pagesCu ZN 10wjjt6chgtmNo ratings yet