
Alergic
Alergic
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
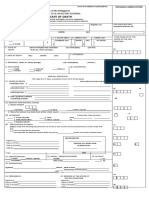
- Certificate of DeathDocument2 pagesCertificate of DeathAngel Urbano67% (3)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Paediatric Advanced Life Support GuidelinesDocument31 pagesPaediatric Advanced Life Support GuidelinesEXODUSGENNo ratings yet
- Anticipatory Medications Guidance Update 24320 1586270784Document3 pagesAnticipatory Medications Guidance Update 24320 1586270784EXODUSGENNo ratings yet
- Gosmanov Etal EPDocument6 pagesGosmanov Etal EPEXODUSGENNo ratings yet
- SDG Guidelines January 2019 PDFDocument71 pagesSDG Guidelines January 2019 PDFEXODUSGENNo ratings yet
- Jurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872Document10 pagesJurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872EXODUSGENNo ratings yet
- MSDS - #820S-NY Opp Packaging Tape PDFDocument3 pagesMSDS - #820S-NY Opp Packaging Tape PDFEXODUSGENNo ratings yet
- MSDS - #820S-NY Opp Packaging Tape PDFDocument3 pagesMSDS - #820S-NY Opp Packaging Tape PDFEXODUSGENNo ratings yet
- Title 25 Chapter 134: Psychiatric HospDocument172 pagesTitle 25 Chapter 134: Psychiatric HosposcartxnNo ratings yet
- Hospital Management SolutionDocument4 pagesHospital Management SolutionsomyaNo ratings yet
- Hildegard PeplauDocument19 pagesHildegard PeplauRosechelle Baggao Siupan-Elarco100% (2)
- Assessment of Disability & CompensationDocument79 pagesAssessment of Disability & CompensationPrasannaKadethotaNo ratings yet
- Self-Management of Mood And/or Anxiety Disorders Through Physical Activity/exerciseDocument11 pagesSelf-Management of Mood And/or Anxiety Disorders Through Physical Activity/exerciseSpj BernardoNo ratings yet
- HIV & AIDS PreventionDocument48 pagesHIV & AIDS PreventionkiookabNo ratings yet
- American Stroke AssociationDocument1 pageAmerican Stroke AssociationritadoloksaribuNo ratings yet
- Combined Use of Antibiotics As A Risk Factor For HDocument15 pagesCombined Use of Antibiotics As A Risk Factor For HGemala AdillawatyNo ratings yet
- Physiological Changes of The PuerperiumDocument6 pagesPhysiological Changes of The PuerperiumBladimir CentenoNo ratings yet
- Annisa Fitriani-19.008-THE TASK OF MAKING SENTENCESDocument2 pagesAnnisa Fitriani-19.008-THE TASK OF MAKING SENTENCESAnnisa FitrianiNo ratings yet
- BariatricDocument7 pagesBariatricNara CavalcantiNo ratings yet
- Mr. Abhijit Bhoyar Lecturer M. Sc. NursingDocument36 pagesMr. Abhijit Bhoyar Lecturer M. Sc. Nursingseeya rayamajhiNo ratings yet
- 1 s2.0 S0255085720315474 MainDocument6 pages1 s2.0 S0255085720315474 MainLidwina ApyakaNo ratings yet
- Doctor Data - DeepikaDocument16 pagesDoctor Data - Deepikainfo.girisanNo ratings yet
- Descoperirea Fiintei-Rollo MayDocument289 pagesDescoperirea Fiintei-Rollo MayAna Sinescu100% (1)
- The Generics ActDocument19 pagesThe Generics ActCJ Halasan100% (1)
- Case StudyDocument3 pagesCase StudySandeepNagarkotiNo ratings yet
- TPN Concept 2 MapDocument3 pagesTPN Concept 2 MapAlvin L. RozierNo ratings yet
- Venture Scape MapDocument4 pagesVenture Scape Mapapi-722297718No ratings yet
- Allied Health Professions That We Presently Have inDocument39 pagesAllied Health Professions That We Presently Have inJayzeel Castor Casaria - FarillonNo ratings yet
- Resume - Afshin AghdasiDocument2 pagesResume - Afshin Aghdasimohammadrezahajian12191No ratings yet
- Class Action Complaint Trial by Jury DemandedDocument58 pagesClass Action Complaint Trial by Jury DemandedXerxes WilsonNo ratings yet
- Osteopathic Manipulative Treatment For Low Back Pain. A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument12 pagesOsteopathic Manipulative Treatment For Low Back Pain. A Systematic Review and Meta-Analysis of Randomized Controlled TrialsPaola GuerraNo ratings yet
- Contemporary Public Health Principles, Practice, and PolicyDocument311 pagesContemporary Public Health Principles, Practice, and PolicyIhor Kuzin100% (1)
- B. Nursing Care PlanDocument3 pagesB. Nursing Care PlanDane YelNo ratings yet
- Basic PrinciplesDocument71 pagesBasic PrinciplesayursrisriharshaNo ratings yet
- Emilio Aguinaldo College Nursing Care PlanDocument1 pageEmilio Aguinaldo College Nursing Care Planamal abdulrahmanNo ratings yet
- Week 2 NURS 2016 Cheat Sheet: by ViaDocument1 pageWeek 2 NURS 2016 Cheat Sheet: by ViaReihann N. EdresNo ratings yet
- Nhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaDocument1 pageNhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaSHWE LINo ratings yet











































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Certificate of DeathDocument2 pagesCertificate of DeathAngel Urbano67% (3)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Paediatric Advanced Life Support GuidelinesDocument31 pagesPaediatric Advanced Life Support GuidelinesEXODUSGENNo ratings yet
- Anticipatory Medications Guidance Update 24320 1586270784Document3 pagesAnticipatory Medications Guidance Update 24320 1586270784EXODUSGENNo ratings yet
- Gosmanov Etal EPDocument6 pagesGosmanov Etal EPEXODUSGENNo ratings yet
- SDG Guidelines January 2019 PDFDocument71 pagesSDG Guidelines January 2019 PDFEXODUSGENNo ratings yet
- Jurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872Document10 pagesJurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872EXODUSGENNo ratings yet
- MSDS - #820S-NY Opp Packaging Tape PDFDocument3 pagesMSDS - #820S-NY Opp Packaging Tape PDFEXODUSGENNo ratings yet
- MSDS - #820S-NY Opp Packaging Tape PDFDocument3 pagesMSDS - #820S-NY Opp Packaging Tape PDFEXODUSGENNo ratings yet
- Title 25 Chapter 134: Psychiatric HospDocument172 pagesTitle 25 Chapter 134: Psychiatric HosposcartxnNo ratings yet
- Hospital Management SolutionDocument4 pagesHospital Management SolutionsomyaNo ratings yet
- Hildegard PeplauDocument19 pagesHildegard PeplauRosechelle Baggao Siupan-Elarco100% (2)
- Assessment of Disability & CompensationDocument79 pagesAssessment of Disability & CompensationPrasannaKadethotaNo ratings yet
- Self-Management of Mood And/or Anxiety Disorders Through Physical Activity/exerciseDocument11 pagesSelf-Management of Mood And/or Anxiety Disorders Through Physical Activity/exerciseSpj BernardoNo ratings yet
- HIV & AIDS PreventionDocument48 pagesHIV & AIDS PreventionkiookabNo ratings yet
- American Stroke AssociationDocument1 pageAmerican Stroke AssociationritadoloksaribuNo ratings yet
- Combined Use of Antibiotics As A Risk Factor For HDocument15 pagesCombined Use of Antibiotics As A Risk Factor For HGemala AdillawatyNo ratings yet
- Physiological Changes of The PuerperiumDocument6 pagesPhysiological Changes of The PuerperiumBladimir CentenoNo ratings yet
- Annisa Fitriani-19.008-THE TASK OF MAKING SENTENCESDocument2 pagesAnnisa Fitriani-19.008-THE TASK OF MAKING SENTENCESAnnisa FitrianiNo ratings yet
- BariatricDocument7 pagesBariatricNara CavalcantiNo ratings yet
- Mr. Abhijit Bhoyar Lecturer M. Sc. NursingDocument36 pagesMr. Abhijit Bhoyar Lecturer M. Sc. Nursingseeya rayamajhiNo ratings yet
- 1 s2.0 S0255085720315474 MainDocument6 pages1 s2.0 S0255085720315474 MainLidwina ApyakaNo ratings yet
- Doctor Data - DeepikaDocument16 pagesDoctor Data - Deepikainfo.girisanNo ratings yet
- Descoperirea Fiintei-Rollo MayDocument289 pagesDescoperirea Fiintei-Rollo MayAna Sinescu100% (1)
- The Generics ActDocument19 pagesThe Generics ActCJ Halasan100% (1)
- Case StudyDocument3 pagesCase StudySandeepNagarkotiNo ratings yet
- TPN Concept 2 MapDocument3 pagesTPN Concept 2 MapAlvin L. RozierNo ratings yet
- Venture Scape MapDocument4 pagesVenture Scape Mapapi-722297718No ratings yet
- Allied Health Professions That We Presently Have inDocument39 pagesAllied Health Professions That We Presently Have inJayzeel Castor Casaria - FarillonNo ratings yet
- Resume - Afshin AghdasiDocument2 pagesResume - Afshin Aghdasimohammadrezahajian12191No ratings yet
- Class Action Complaint Trial by Jury DemandedDocument58 pagesClass Action Complaint Trial by Jury DemandedXerxes WilsonNo ratings yet
- Osteopathic Manipulative Treatment For Low Back Pain. A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument12 pagesOsteopathic Manipulative Treatment For Low Back Pain. A Systematic Review and Meta-Analysis of Randomized Controlled TrialsPaola GuerraNo ratings yet
- Contemporary Public Health Principles, Practice, and PolicyDocument311 pagesContemporary Public Health Principles, Practice, and PolicyIhor Kuzin100% (1)
- B. Nursing Care PlanDocument3 pagesB. Nursing Care PlanDane YelNo ratings yet
- Basic PrinciplesDocument71 pagesBasic PrinciplesayursrisriharshaNo ratings yet
- Emilio Aguinaldo College Nursing Care PlanDocument1 pageEmilio Aguinaldo College Nursing Care Planamal abdulrahmanNo ratings yet
- Week 2 NURS 2016 Cheat Sheet: by ViaDocument1 pageWeek 2 NURS 2016 Cheat Sheet: by ViaReihann N. EdresNo ratings yet
- Nhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaDocument1 pageNhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaSHWE LINo ratings yet